
Abstract
We assessed the prevalence and predictors of malnutrition in patients with nasopharyngeal carcinoma. Sixty cases and 123 controls matched for age and gender were included. Bio-data, dietary history, height, weight, body mass index (BMI), ideal body weight, and serum albumin levels were recorded. Pretreatment weight loss of >5% was present in 35% of subjects (P < 0.0001). A BMI of < 18.5 kg/m2 was present in 13.3% (P < 0.001), percent ideal body weight of <90% was present in 30% (P < 0.001), and serum albumin levels < 30 g/dL was present in 23.3% (P < 0.001) of cases. Nasopharyngeal carcinoma increased the likelihood of having a BMI < 18.5 kg/m2 (odds ratio, 9.3 (3.4–25.3) P ≤ 0.001). Logistic regression shows that stage IV disease was associated with a decrease in all parameters except protein-calorie intake. Stage IV nasopharyngeal carcinoma is a predictive marker for weight loss and low serum albumin levels. Nutritional management is important for ensuring the patients’ ability to withstand chemoradiation and thus improve survival and quality of life.
Introduction
Nutrition is a significant aspect of cancer management. It determines a patient's functional status, tolerance to therapeutic interventions, and overall prognosis. There is no consensus on the definition of malnutrition, which results from a state where food intake does not meet the energy requirements. This could be due to increased metabolic demands, malabsorption, or inadequate food intake. 1 Malignant transformation of cells alters their metabolism to support the tumor's metabolic needs. This involves the shift from mitochondrial oxidative phosphorylation to aerobic glycolysis, an inefficient process. This results in rapid depletion of glucose stores and a shift towards gluconeogenesis from fat and protein stores in muscle. The body's metabolic and immunologic response to cancer also encourages malnutrition through anorexia.
Malnutrition and wasting in cancer is a prevalent condition and the incidence ranges from 30 to 80%.2–4 In patients with head and neck cancers, malnutrition is further worsened by dysphagia, odynophagia, pain, and depressed mood. 5 Malnutrition increases the risk of infections, treatment toxicity, and health-care costs. It also adversely affects the quality of life and prognosis.6–8 The prevalence of malnutrition in the adult Kenyan population is between 9 and 12%.9,10
Nasopharyngeal carcinoma (NPC) is the most prevalent cancer in the East and South East Asian populations. 11 In Kenya, NPC is the second-most common carcinoma of the head and neck after oral tumors. 12 The prevalence of malnutrition in patients with head and neck squamous cell carcinoma has been thoroughly studied. Because NPC is prevalent in Kenya, this study examined the nutritional status of patients with NPC, the parameters most useful in evaluating this, and predictors of malnutrition in this population.
Methods
Subjects
This research was approved by the Kenyatta National Hospital Ethics and Research Committee in March 2012. The study was conducted in accordance with the principles of the Declaration of Helsinki, at the Kenyatta National Hospital in Nairobi, Kenya. This is the only public facility in the country with a cancer treatment center. Patients with histological diagnosis of NPC were enrolled into the study. Written consent was obtained from all study participants. Controls were recruited from the dental outpatient clinic. They were matched for age and gender. All patients gave a negative history of co-morbid conditions associated with weight change in the preceding six months.
Data collection
Demographic characteristics (age and gender), his topathological grade based on World Health Organization (WHO) guidelines, and stage (American Joint committee on Cancer 7th edition) were recorded. Stage of the disease was determined using clinical, endoscopic, and computed tomography (CT) scan findings in all cases. All subjects were required to undergo HIV testing.
Dietary intake was entered into the Nutrition Assessment Form that contains a comprehensive list of local foods. Daily intake was then calculated by the nutritionist. Protein intake was recorded in grams and the energy intake in kilocalories using the Kenyatta National Hospital Food Exchange Index. The intake list was recorded based on average weekly intake and confirmed three days later to reduce discrepancies. Factors affecting food intake lasting for more than two weeks were recorded as anorexia, dysphagia, pain, vomiting, diarrhea, and others.
Weight (kg) was measured using a conventional mechanical weighing scale and recorded to one decimal point. Height was measured in the standing position using a height meter with bare feet and recorded in centimeters. Body mass index (BMI) and the ideal body weight (IBW) were then derived.
Two millilitres of blood was drawn from each patient and processed at the Kenyatta National Hospital Biochemistry lab. The samples were analyzedusing the AU640 Chemistry Analyzer Automated System (Olympus, Tokyo, Japan). The lab normal values for serum albumin were 30–54 g/dL.
Confidentiality was maintained throughout the study.
Criteria for nutritional classification
Nutritional status was assessed by (1) calculating the percentage weight loss by comparing with the usual weight; (2) the body mass index using WHO cutoff points; (3) percent of ideal body weight; (4) protein intake, and (5) caloric intake. Indicators of under nutrition were weight loss of >5% in the preceding month; BMI < 18.5 kg/m2; percent of ideal body weight (%IBW) <90%; protein intake <1.5 g/kg body weight per day and caloric intake of less than 35 kcal/kg body weight per day.13,14
Statistical analyses
The subjects’ characteristics were analyzedusing descriptive statistics. The subjects’ disease stage, nutritional status, and dietary intake were expressed as percentages, means, and standard deviation values. Cases and controls weight loss, dietary intake, anthropometric parameters, and serum albumin levels were compared using chi-square tests for categorical variables and Student's t-tests for continuous variables. Percentages of patients who were considered malnourished were calculated based on the results achieved on the first and third day.
To identify predictors for malnutrition weight loss, protein-calorie intake, BMI, percent ideal body weight, and serum albumin levels were considered dependent variables and multivariate logistic regression analysis was conducted. A P-value of <0.05 was considered to be statistically significant. Data was analyzedusing SPSS version 17.0 (SPSS Inc, Chicago, IL, USA).
Results
The summary of patients’ characteristics is shown in Table 1.
Significant weight loss was present in 35% of the patients. Severe weight loss requiring hospitalization was reported in 6.7% of the patients. The BMI was found to be <18.5 kg/m2 in 13% of the patients. Of note is that 6.7% of the cases were overweight as compared to 1.6% of the controls. The %IBW was <90% in 30% of the patients. There was hypoalbuminemia (<30 g/dL) in 23.3% of the patients. Severe weight loss of > 10% of the usual body weight in the preceding month was reported in 6.7% of patients.
Patient characteristics.
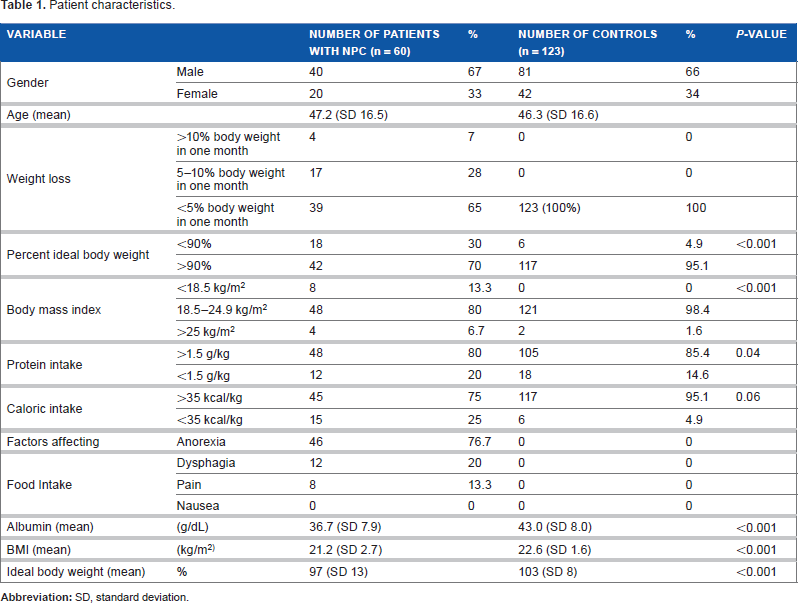
There were 14 cases with serum albumin levels < 30 g/dL compared to a single control (P ≤ 0.001). Fisher's exact test (two-tailed) was used to compare the association between the anthropometric indices and the serum albumin levels. Cases with BMI <18.5 kg/m2 were 8 times more likely to have low albumin levels (<30 g/L) (OR 8.0 (1.6–39.5) 95% CI P = 0.013). Cases with %IBW <90% were associated with low serum albumin when compared to patients with normal weight (OR 20 (4.5–92) 95% CI P = 0.0001). Patients with NPC had a higher likelihood of being underweight as compared to the controls (OR 9.3 (3.4–25.3) 95% CI P < 0.001).
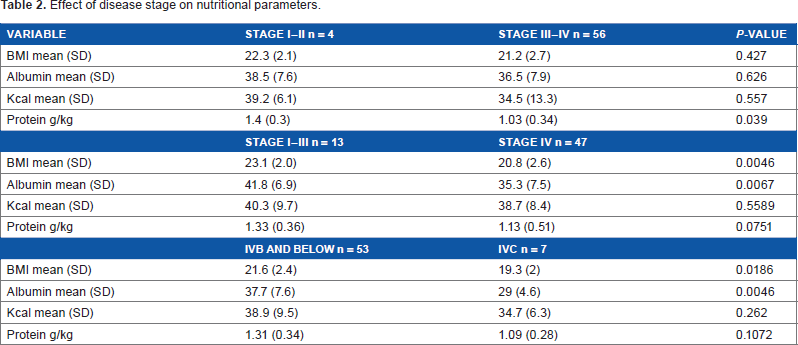
Logistic regression was used to determine the effect of disease stage on the parameters used to analyze nutritional status. When divided patients into early disease stage I/II and advanced disease stage III/IV and observed no significant differences in the parameters. However, when stage IV disease was compared to earlier stages it was found to be associated with a decrease in all the parameters except the protein-caloric intake. Metastatic disease was associated with a significant decrease in serum albumin levels. There was no significant correlation between any of the indices and the his topathological grade of the tumor.
The stage of the disease was found to be a predictive marker for weight loss, BMI, and low serum albumin (P < 0.001).
Discussion
Nasopharyngeal carcinoma was found to adversely affect the nutritional status of the patient, with pretreatment weight loss a significant factor in determining weight loss during treatment and the likelihood of hospitalization. 15 Nourissat et al conducted a study on 907 patients and found a strong correlation between the quality of life of patients and pretreatment weight loss. This not only impacted their disease status but also increased their hospital stay. 16
Patients reporting anorexia, dysphagia, pain or who are on semi-solid or liquid diets are less likely to achieve their protein and caloric requirements. Kubrak et al followed up cancer patients prospectively using the Patient-Generated Subjective Global Assessment Tool. 17 Anorexia, dysphagia, pain, and mouth sores were found to be significant predictors of reduced dietary intake and weight loss.
There was no difference in the protein-caloric intake between the cases and controls and no correlation was found between the patient food intake and nutritional status. This indicates that other factors also come into play with regards to malnutrition other than the intake. However, Jager-Witenaar et al found that patients with sufficient intake (>35 kcal and >1.5 g protein/kg body weight) lost less body weight and lean mass and gained body weight and lean mass after treatment. 7 This shows that even though other factors play a role, dietary intake is very important for managing malnutrition in these patients.
Furhman et al concluded that a decrease in protein intake is not consistently correlated with decrease in serum protein levels. 20 Prealbumin is also measured as a marker of protein levels. It has the advantage of having a shorter half-life of 2–3 days over the 14–21 days of albumin. It thus serves as a more sensitive indicator of recent changes and patients at risk of malnutrition. Systemic factors such as inflammation and hepatic insufficiency affect serum protein levels.
Serum albumin levels have been shown to correlate with the morbidity and mortality of patients. A systematic search of the literature studying the relationship between serum albumin levels and cancer survival show that pretreatment serum albumin levels are a useful prognostic factor in cancer. 21 Proinflammatory cytokines, including tumor necrosis factor-a, interleukin-6, interleukin-1b, Interferon-gamma, and a proteolysis-inducing factor, have been shown to cause anorexia and induce a hypermetabolic state in patients with malignancy resulting in cachexia. 22
Ravasco and colleagues found that patients with advanced disease (stage III and IV) reported weight loss >10%. 19 Advanced staging showed a significant association with decreased energy and protein intake and nutritional depletion in his study. The ability to detect mild to extreme nutritional changes was better using the percentage weight loss compared to other clinical variables.
In Kenya >90% of patients present in Kenya present in stage IV nasopharyngeal carcinoma. 18 Thus, active screening of these patients is essential as chemoradiation is the treatment of choice and is associated with anorexia, mucositis, nausea, and other symptoms that further worsen the nutritional status of the patient. Histology had no significant correlation with the nutritional status of the patients.
Low serum albumin has been found to serve as an independent prognostic indicater in patients with advanced head and neck cancers on treatment with chemoradiation. 23
Conclusions
Significant weight loss was observed in 35% of the patients at presentation with 6.7% having severe malnutrition. Nasopharyngeal carcinoma was found to significantly increase the probability of weight loss and malnutrition. Stage IV disease was the most significant factor affecting the nutritional status of the patients. The percent ideal body weight was a more sensitive measure of the nutritional status than the BMI. Additionally, metastatic disease was associated with hypoalbuminemia. This study shows that a higher disease stage is associated with pretreatment weight loss, lower percent ideal body weight, and lower serum albumin levels. Pretreatment weight loss and malnutrition are worsened during treatment of nasopharyngeal carcinoma. Thus, active assessment and management of the nutritional status of patients at presentation ensures optimum quality of, improves their ability to withstand chemoradiation improving survival. 23
Effect of disease stage on nutritional parameters.
Author Contributions
Conceived and designed the experiments: CWI, HOO. Analyzed the data: CWI. Wrote the first draft of the manuscript: CWI. Contributed to the writing of the manuscript: CWI, HOO, BO. Agree with manuscript results and conclusions: CWI, HOO, BO. Jointly developed the structure and arguments for the paper: CWI, HOO. Made critical revisions and approved final version: CWI, HOO, BO. All authors reviewed and approved of the final manuscript.