
Abstract
Background:
The Tinnitus Questionnaire is commonly used to evaluate the psychological impact of tinnitus and has been translated into Mandarin. The original English version of the Tinnitus Questionnaire was translated into Mandarin (Mandarin Tinnitus Questionnaire [MTQ]). The MTQ included not the same items compared with original version. Thus, MTQ should have its own severity categorization.
Aims/Objectives:
The objective of this research was to develop a method to categorize tinnitus patients by clinical severity using scores from the MTQ.
Material and Methods:
A total of 192 participants with primary complaint of tinnitus were enrolled. Cross-tabulation was used to compare 2 categorization approaches of tinnitus severity. With the first approach, categories were assigned based purely on quartiles of MTQ scores. In the second approach, severity was determined based on ordinal logistic regression. The 2 approaches were verified by comparing the consistency with clinical judgment.
Results:
Categorization based on quartiles showed low consistency with clinical assessment (κ = 0.33), while categorization based on ordinal logistic regression showed good consistency with clinical assessment (κ = 0.86). Regression-based MTQ score cutoffs were <21 for no problem with tinnitus, 21 to 36 for mild tinnitus, 37 to 47 for moderate tinnitus, and >47 for severe tinnitus.
Conclusions and Significance:
Tinnitus severity can be categorized accurately using ordinal logistic regression analysis of MTQ scores.
Introduction
Tinnitus is the perception of sound, commonly described as a buzzing, humming, or ringing noise, in the absence of an external source. 1 It occurs in 10% to 15% of adults. 2 Although it is one of the most common symptoms of hearing disorders, relatively few people who experience tinnitus seek medical help at ear, nose, and throat or audiology clinics. According to a study by Davies et al, 3 only 7.1% of adults with tinnitus consult a doctor and only 2.5% seek specialist advice. This is likely due to variation in the severity of tinnitus: most people experience tinnitus only occasionally and consider that it does not affect them substantially. However, some people suffer persistent tinnitus, which may be severely annoying and very troublesome. 4 In fact, apart from the tinnitus itself, some patients suffer from tinnitus-related anxiety, depression, and insomnia. Evidence shows that just over one quarter (26.1%) of adults with tinnitus report problems with anxiety, 5 48% to 60% report depression, 6 and 76% experience insomnia. 7 Perceived tinnitus severity does not appear to be influenced by age, gender, or hearing status but is related to anxiety–depressive symptoms. 8
Tinnitus severity has been assessed using psychoacoustic measurements, structured questionnaires, and open-ended approaches. Self-report measures are becoming increasingly common in managing tinnitus patients and in tinnitus research. 9 One example is the visual analog scale, in which patients report the severity of their tinnitus by choosing a position along a continuous line between 2 end points, where the line is divided into 5 to 10 equal intervals. Such scales can be useful for self-rating tinnitus loudness and the annoyance it causes. 10 However, visual analog scales are not reliable and cannot be used to judge tinnitus severity independently.
An alternative to these scales is questionnaires. A recent review identified 24 tinnitus-related questionnaires. 11 The ones most often used in clinical trials are the Tinnitus Handicap Inventory (THI), the Tinnitus Questionnaire, the Tinnitus Reaction Questionnaire, and the Tinnitus Handicap Questionnaire. 11 These questionnaires assess different aspects of tinnitus severity. For example, the THI quantifies the functional, emotional, and catastrophic impacts of tinnitus. 12 The Tinnitus Reaction Questionnaire assesses tinnitus-associated psychological distress, including general distress, interference, severity, and avoidance, 13 while the Tinnitus Handicap Questionnaire focuses on the patient’s hearing ability and the social consequences of tinnitus. 14
The Tinnitus Questionnaire was one of the first to be developed and is one of the most commonly used. It is used mainly to evaluate the psychological impact of tinnitus, such as depression, anxiety, insomnia, negative attitudes toward tinnitus, and interference with social activities. 15 The Tinnitus Questionnaire has been translated into German, Spanish, French, Dutch, Cantonese, and Mandarin. 15 The full questionnaire consists of 52 items, of which 41 are used in the English version to calculate subscale and total scores. The English version has 5 subscales: (1) emotional distress (including cognitive distress, 19 items), (2) auditory perceptual difficulties (APDs, 7 items), (3) intrusiveness (7items), (4) sleep disturbance (4 items), and (5) somatic complaints (4 items).The responses to each item are given a score of 0, 1, or 2, where higher scores indicate stronger tinnitus complaints.
The numbers of items in the subscales of different language versions of the questionnaire differ, reflecting different factor analyses. For example, the German version of the Tinnitus Questionnaire has 40 items, 15 while the Dutch version has 38 items. 15 The Tinnitus Questionnaire is used mainly to evaluate the psychological impact of tinnitus effects, such as depression, anxiety, insomnia, negative attitudes toward tinnitus, and interference with social activities. 15 The original English version of the questionnaire was translated into Mandarin by Meng et al, 16 who validated it among Chinese adults and showed that there was high consistency between retests (Spearman correlation coefficients = 0.87-1.00) as well as good internal consistency and reliability (overall Cronbach α = .93, subscale α values = .71-.86). The Mandarin version of the Tinnitus Questionnaire (MTQ) has 37 items, where the highest possible score is 74. The 5 subscales are emotional distress (11 items), APDs (8 items), cognitive distress (6 items), sleep disturbance (6 items), and intrusiveness (6 items). Comparing with Tinnitus Questionnaire, items of somatic complaints were not extracted in MTQ.
While the score on the Tinnitus Questionnaire provides insight into the severity of the psychological impacts of tinnitus, it only roughly reflects the clinical severity of the disorder. This is important because clinicians must determine whether patients have bothersome or nonbothersome tinnitus, 1 and this classification affects subsequent intervention. Developing a scale of tinnitus severity with more than these 2 categories may help clinicians to design effective intervention plans for each patient, as well as assess whether the intervention has reduced tinnitus severity.
Although using a questionnaire may be one of the most straightforward ways to assess tinnitus severity, 1 no categorization of tinnitus severity has been developed for the original Tinnitus Questionnaire or for the MTQ. Only the German version of the Tinnitus Questionnaire, which includes a total of 42 items covering 5 subscales (emotional and cognitive distress, intrusiveness, APDs, sleep disturbances, and associated somatic complaints), has an indication for distress level based on the total score (0-30 = mild, 31-46 = moderate, 47-59 = severe, 60-84 = very severe). 17
It has been proposed that this categorization system could also be used for other tinnitus-related questionnaires. The original English version of the THI also categorizes the severity of tinnitus into 4 levels based on score (0-16 = no handicap, 18-36 = mild handicap, 36-56 = moderate handicap, 58-100 = severe handicap). 12 A revised version of this categorization has 5 levels (0-16 = slight, 18-36 = mild, 38-56 = moderate, 58-76 = severe, 78-100 = catastrophic). 5 A Tinnitus Functional Index (TFI) has been developed to assess severity, where a score of <25 is mild and requires no intervention, 25 to 50 is significant and indicates a possible need for professional attention, and >50 is severe and requires more aggressive efforts. 18 In China, 2 versions of the THI categorization have been used in the clinic. A 5-step TFI for assessing severity has also been developed based on US respondents 19 (0-17 = not a problem, 18-31 = small problem, 32-53 = moderate problem, 54-72 = big problem, 73-100 = very big problem), while a slightly different index has been developed based on UK respondents 20 (0-7 = no problem, 7-28 = small problem, 29-47 = moderate problem, 48-65 = big problem, 66-100 = very big problem).
Therefore, as indicated above, Tinnitus Questionnaire is useful to evaluate the psychological impact of tinnitus effects. As different language versions of the tinnitus questionnaire contain different numbers of items, different versions should have their own severity categorizations. The purpose of the current study was to develop a categorization method for tinnitus severity based on MTQ score. Accurate classification of patients may help provide new criteria for designing intervention protocols and assessing treatment efficacy.
Materials and Methods
Participants
Participants at least 18 years old were recruited from patients who sought treatment for primary tinnitus at the Department of Otorhinolaryngology in the Hearing Center of West China Hospital, Sichuan University. Patients with psychiatric disorders, auditory hallucination, or difficulty in expressing themselves were excluded. Subjects were enrolled after they provided written informed consent. Each patient underwent routine audiological examination, which consisted of pure-tone audiometry followed by completion of the MTQ. This research was approved by the ethics committee of West China Hospital, Sichuan University.
Mandarin Tinnitus Questionnaire
Participants filled out all 52 items on the full MTQ, but only 37 were analyzed in the present study. 16 The following items from each subscale were analyzed: emotional distress, 11, 16, 19, 45, 35, 37, 39, 48, 43, 46, 47; APDs, 26, 15, 38, 50, 33, 2, 9, 14; cognitive distress, 41, 23, 42, 18, 32, 17; sleep disturbance, 20, 36, 5, 12, 52, 4; and intrusiveness, 27, 21, 3, 13, 28, 29. 16 Three responses were possible for each item: “true” (2 points), “partly true” (1 point), or “not true” (0 point), such that the maximum possible score was 74. A higher score indicated more severe tinnitus.
Categorization of Tinnitus Severity From MTQ Data
We tested 2 statistical approaches to classifying the clinical severity of tinnitus based on MTQ data. The first approach MTQ scores were divided into quartiles, and individuals in the first quartile were classified as having no problem with tinnitus, the second quartile as having mild tinnitus, the third as having moderate tinnitus, and the fourth as having severe tinnitus. 12 Quartile is a ranked set of data. The first quartile is the middle number between the smallest number and the median of the data set. The second quartile is the median of the data. The third quartile is in the middle between the median and the highest value of the data set. This is the method used, for example, on the THI. As an existing categories way used for identifying categories in other categorizing tinnitus severity, quartile analysis was used as a starting point in this analysis. In the second approach, tinnitus severity was determined based on ordinal logistic regression. Patients were divided into 4 groups based on cutoffs determined by ordinal logistic regression.
The validity of creating tinnitus distress severity categories for MTQ based on statistic method was verified by comparing the method with a clinical categories based on a clinician judgment. The clinician who specialized in tinnitus, judged the tinnitus severity based on clinical assessment and the patient's history (including emotional and cognitive distress, APDs, sleep disturbance, and intrusiveness). Patients with more complaints in these categories or more severe psychological impacts associated with tinnitus were categorized as having more severe tinnitus. The categories (mild, moderate and severity) for clinical categorization were not a problem. Consistency between the 2 categorization approaches was assessed.
Data Analysis
Statistical analysis was performed using SPSS 20.0 (IBM, Chicago, Illinois). Receiver Operating Characteristic Curve (ROC) is often used as a recognized method when there is a golden standard with a cutoff point in order to explore the sensitivity and specificity of an individual test. In the present study, logistic regression was chosen because there was no golden standard for categorizing tinnitus severity in Tinnitus Questionnaire. Ordinal logistic regression was performed to examine the correlation between clinical assessment of tinnitus severity and the MTQ score. Ordinal rather than binary logistic regression was chosen because we wanted to classify tinnitus severity on a 4-degree scheme (not a problem, mild, moderate, severity). The dependent variable in the regression was severity defined by clinical assessment, and total MTQ score was the independent variable. Cohen κ coefficient, which was introduced in 1960, serves as the most widely employed coefficient to assess interobserver agreement for categorical outcomes. Because the assessment of tinnitus severity category was ranked data, consistency between the clinical assessment and regression-based severity was evaluated using the κ co-efficient.
Results
A total of 192 participants with a primary complaint of tinnitus were enrolled. The average age was 45 years (standard deviation [SD] = 15.52 years; range = 18-83 years), and participants had tinnitus for periods ranging from 3 days to 25 years (mean = 26.37 months, SD = 41.36 months).
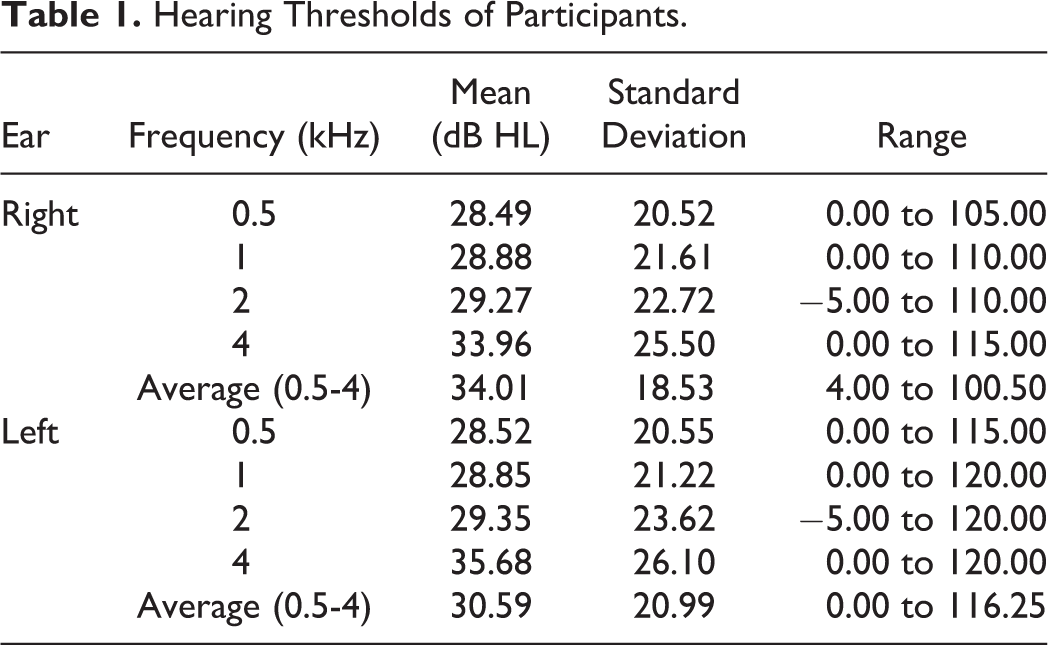
Hearing assessments were performed in all 192 participants (Table 1). For the right ear, 78 patients had normal hearing; 57, mild hearing loss; 38, moderate loss; 15, severe loss; and 4, profound loss. This assessment was based on the grades of hearing loss defined by the World Health Organization in 2006. For the left ear, 99 participants had normal hearing; 37, mild loss; 37, moderate loss; 16, severe loss; and 3, profound loss. Nearly all participants (181, 94.27%) had continuous tinnitus, while the remaining 11 (5.73%) had intermittent tinnitus.
Hearing Thresholds of Participants.
Mandarin Tinnitus Questionnaire Scores and 2 Categorization Analysis of Tinnitus Severity
The mean total score was 26.63 (SD = 16.26), with a median of 23.00. The 25th percentile was 14.00 and the 75th percentile was 38.75. Respondents were categorized by tinnitus severity based on quartiles, and further statistical analysis was performed using the mean (Table 2). All 4 quartiles were nearly equal in size, with each accounting for 22.92% to 28.13% of respondents.
Categorization of Tinnitus Severity Based on Quartile Analysis of MTQ Scores (n = 192).
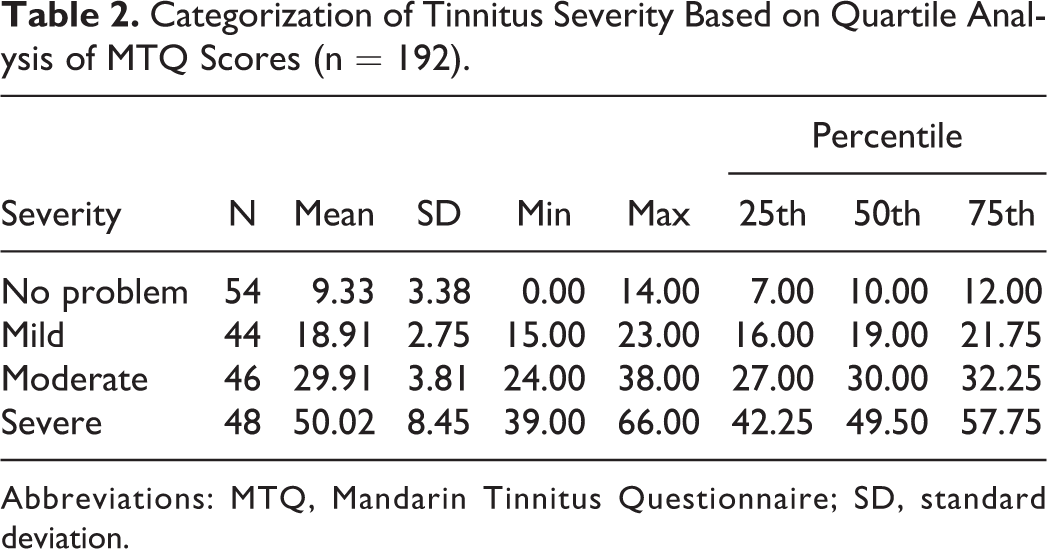
Abbreviations: MTQ, Mandarin Tinnitus Questionnaire; SD, standard deviation.
We compared the number of patients in each category as determined by quartile-based classification with the number of patients in each category as determined by clinical classification (Table 3). For clinical classification, there were fewer patients with moderate and severe tinnitus than with mild tinnitus or no problem with tinnitus. When patients were categorized by clinical classification, MTQ scores ranged from 11.00 to 23.00 in patients with mild tinnitus, 35.00 to 49.00 in patients with moderate tinnitus, and >49.00 for all patients with severe tinnitus. The highest MTQ score in patients with no problem with tinnitus was 26.00. Some overlap was observed between patients with mild tinnitus or no problem with tinnitus and between patients with mild or moderate tinnitus. This likely reflects the subjective nature of clinical assessment.
MTQ Scores in Patients Categorized by Clinical Assessment (n = 192).
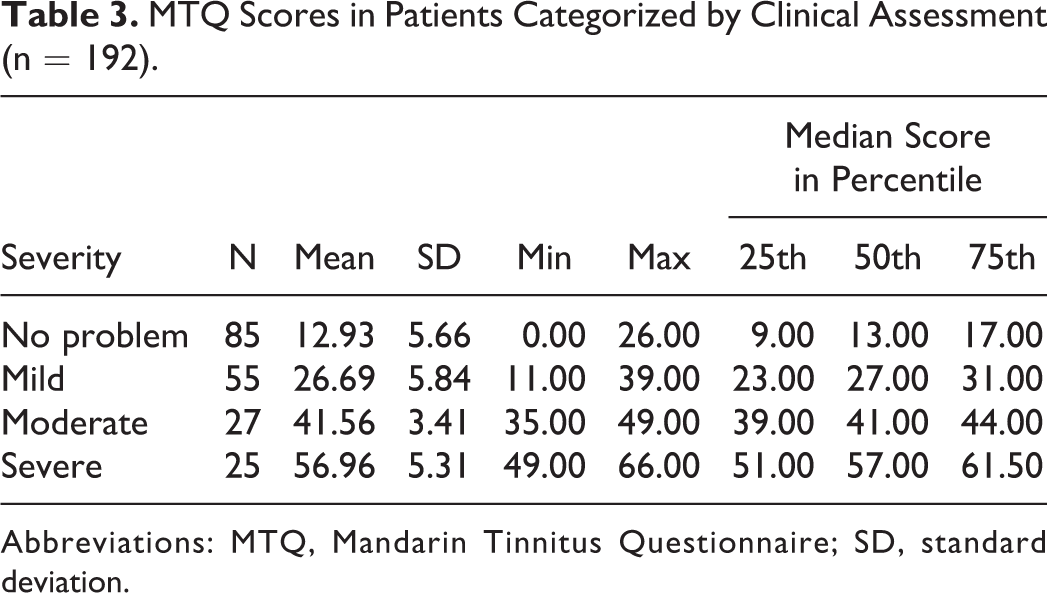
Abbreviations: MTQ, Mandarin Tinnitus Questionnaire; SD, standard deviation.
Severity categorization agreed significantly between quartile analysis and clinical assessment (P < .01), but consistency was low (κ = 0.33; Table 4). There was excellent agreement between the 2 types of classification for patients with no problem with tinnitus (52/54, 96.30%). However, 30 participants categorized as having mild tinnitus based on quartile analysis were categorized as having no problem with tinnitus by clinical assessment. In addition, 38 participants categorized as having moderate tinnitus based on quartile analysis were categorized as having severe tinnitus based on clinical assessment. Twenty-five patients were categorized as having severe tinnitus using both classification methods (25/48, 52.08%); however, 22 patients categorized as having severe tinnitus based on quartile analysis were categorized as having moderate tinnitus based on clinical assessment.
Consistency Between Quartile-Based or Clinical Assessment-Based Categorization of Tinnitus Severity.a
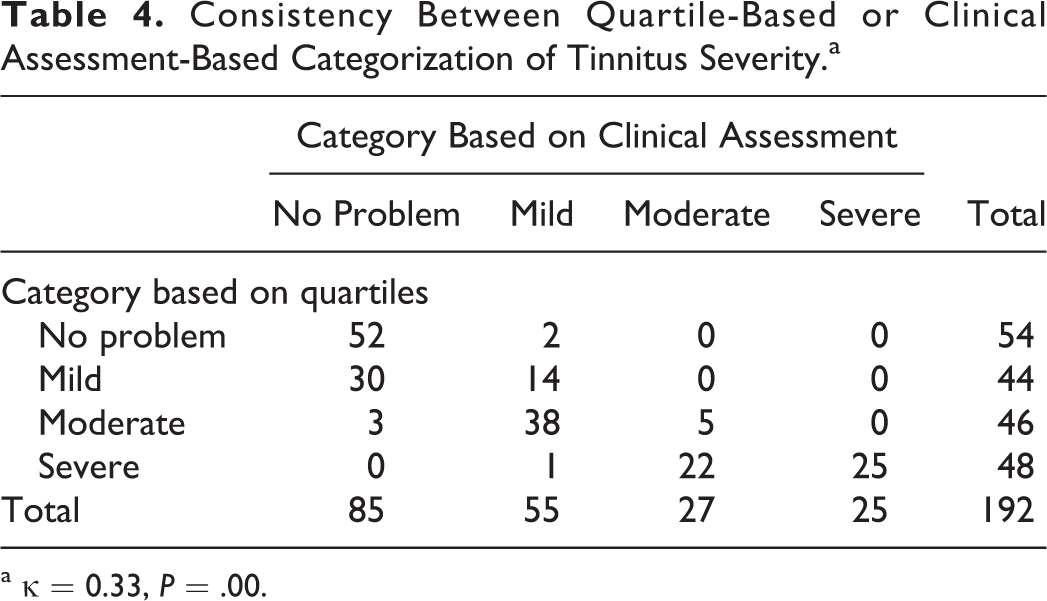
a κ = 0.33, P = .00.
Regression-Based Prediction of Tinnitus Severity
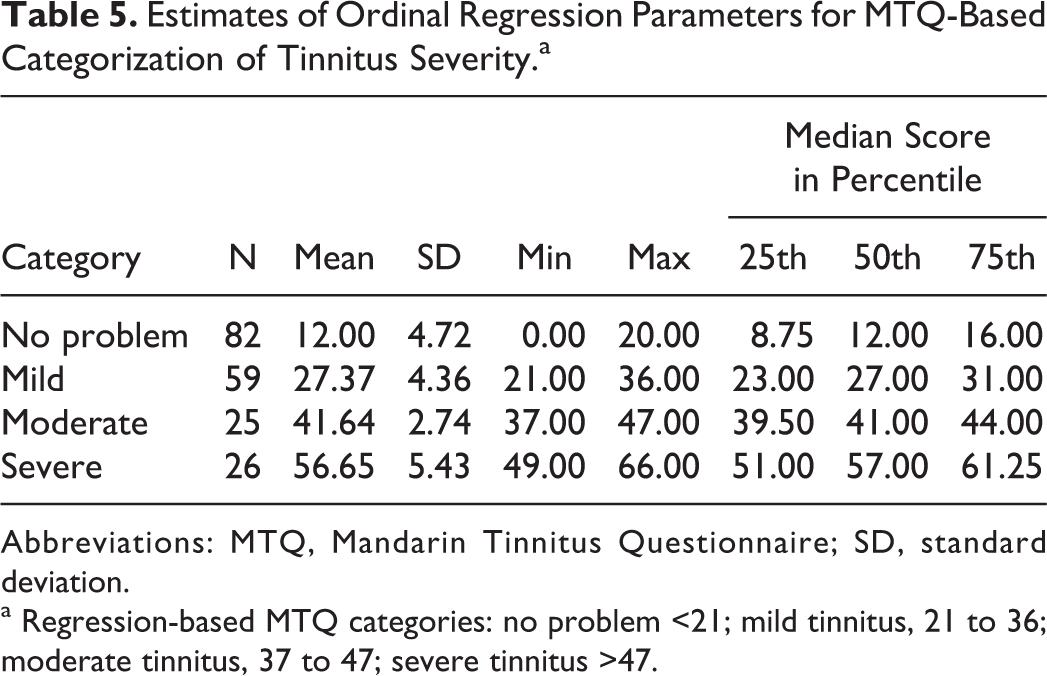
In the second method, we used ordinal logistic regression to determine MTQ score cutoffs for categorizing patients with different levels of tinnitus severity. Mandarin Tinnitus Questionnaire scores ranged from 0 to 20 for patients with no problem with tinnitus, 21 to 36 for patients with mild tinnitus, 37 to 47 for patients with moderate tinnitus, and 49 to 66 for patients with severe tinnitus, as categorized by clinical assessment (Table 5).We used these values to define cutoff scores for each category (no problem with tinnitus = less than 21; mild tinnitus = 21-36; moderate tinnitus = 37-47; severe tinnitus = greater than 47).
Estimates of Ordinal Regression Parameters for MTQ-Based Categorization of Tinnitus Severity.a
Abbreviations: MTQ, Mandarin Tinnitus Questionnaire; SD, standard deviation.
a Regression-based MTQ categories: no problem <21; mild tinnitus, 21 to 36; moderate tinnitus, 37 to 47; severe tinnitus >47.
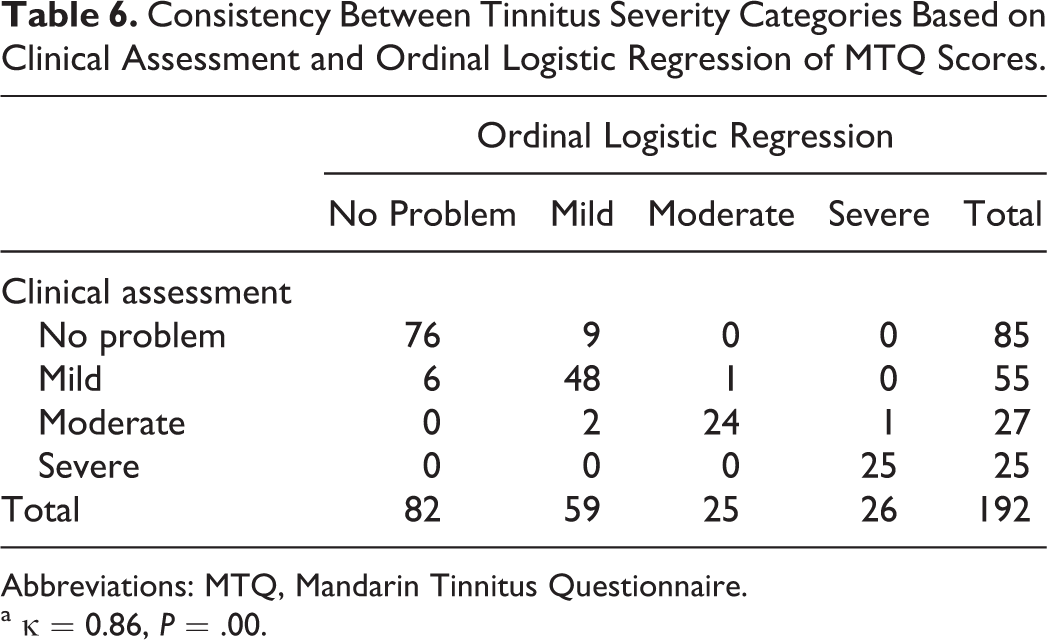
We then compared the results of the above classification method with classifications by clinical assessment. There was a strong correlation between the 2 classification methods (P < .01) and a high κ value (0.86; Table 6). There were disagreements in categorizing 3 patients with no problem with tinnitus, 4 patients with mild tinnitus, and 1 patient with moderate tinnitus. The clinical and regression-based methods agreed on categorizing 25 patients with severe tinnitus, with a disagreement for only 1 patient who was classified as having moderate tinnitus based on clinical assessment but severe tinnitus based on regression.
Consistency Between Tinnitus Severity Categories Based on Clinical Assessment and Ordinal Logistic Regression of MTQ Scores.
Abbreviations: MTQ, Mandarin Tinnitus Questionnaire.
a κ = 0.86, P = .00.
Discussion
The biggest obstacle in grading tinnitus severity is the lack of any objective measure. Psychometrically validated questionnaires are the most effective way of assessing tinnitus. 4 Unfortunately, there is no uniform questionnaire to be accepted. The questionnaire used to judge tinnitus severity should minimize some of the inaccuracy and bias inherent in subjective assessment. 4 The Tinnitus Questionnaire and THI are widely used for subjectively measuring tinnitus severity. 4 The lack of a single standard can lead to inaccuracy and bias in subjective clinical assessments. 4
Considering most of tinnitus is primary and subjective in nature, besides questionnaire measurements, clinical judgment by clinicians is also an essential element before making clinical decision to provide safe and effective interventions for patients with tinnitus. To grade tinnitus severity by only using MTQ or statistical analysis may be misleading. It is evidenced that the grade of tinnitus severity is likely not to being accepted when the statistical categorizing analysis of tinnitus severity is inconsistent with clinical judgment. Similarly, clinical judgment is also a subjective concept, depending on individual’s knowledge, clinical experience, and sometimes preference. Without regulation and standardization of structures and processes, it could be biased and unreliable to grade tinnitus severity only relying on individual’s clinical judgment. Therefore, it seems better to combine the statistical analysis and clinical judgment in terms of validity and efficacy when categorizing the tinnitus severity in clinic.
We used 2 statistical approaches to grade tinnitus severity and found large discrepancies between the results of categorizing participants based purely on MTQ score quartiles and the results of clinical assessment based on medical records. The quartile approach assigned nearly the same number of participants to each of the 4 categories (Table 2), while there were more patients with mild tinnitus or with no problem with tinnitus using the clinical approach (Table 3). This uneven distribution more closely matches what would be expected in the clinic. Ordinal logistic regression assigned 26 (13.54%) participants to the group with severe tinnitus and 25 (13.02%) to the group with moderate tinnitus, which is consistent with a previous study showing that approximately 20% of adults who experience tinnitus require clinical intervention. 5 Our results indicate that quartile-based classification does not accurately reflect clinical reality. In contrast, regression-based categorization was more consistent with clinical assessment.
Regression-based classification may be useful for identifying individuals who require clinical intervention and determining whether a given intervention has been effective or not. An effective treatment should, for example, reduce tinnitus severity according to the MTQ score. Further work should examine how much the MTQ score needs to decrease in order to achieve clinically significant improvement. The ultimate test of any categorization method is whether it is sensitive enough to detect differences in therapeutic efficacy between interventions.
One limitation of our study is that clinical assessment of all study participants was carried out by a single individual. To minimize any bias or subjectivity, we provided our clinician with clear, predefined criteria as specified in Methods. However, our results may not be reflective of assessment outcomes by other clinicians. Further work should be performed to verify and extend this work using clinical assessments by multiple physicians. Future studies could also compare the outcomes of different clinicians’ assessments and patients’ self-assessment on the same 4-point scale.
The MTQ categorization strategy in this study should be used, in principle, only for Chinese patients because different language versions have different numbers of items. Therefore, categorization methods for Tinnitus Questionnaires in other languages are still needed. The total scores, items, and categories in the MTQ and German Tinnitus Questionnaire are different: 42 items are included in the German version and 37are included in the MTQ. Therefore, although both versions feature 4 distress levels, they do not mean the same thing. The German version classifies patients as having mild, moderate, severe, or very severe tinnitus, while the MTQ classifies patients as having no problem with tinnitus or as having mild, moderate, or severe tinnitus. Only 7.1% of adults with tinnitus consult a doctor and only 2.5% seek specialist advice, 3 even though 94% of normal individuals report some form of tinnitus-like perception; therefore, we think that the category of “no problem with tinnitus” on the MTQ may be more appropriate than “mild tinnitus” on the German version.
The 4-level categorization on the MTQ is similar to that on the THI, 12 although he revised version of the THI contains 5 levels. 5 Future study should explore whether a 5-level categorization on the MTQ is needed. It is noteworthy that no one questionnaire can assess all aspects of tinnitus-related severity. Although the MTQ can capture the psychological severity of emotional distress, APDs, cognitive distress, sleep disturbance, and intrusiveness, other questionnaires are still needed to capture the psychological severity caused by problems or interference with work, family life, social activities, or mental concentration.
Conclusions
Ordinal logistic regression provides a reliable categorization of tinnitus severity based on the MTQ score. Scores were <21 for those with no problem with tinnitus, 21 to 36 for those with mild tinnitus, 37 to 47 for those with moderate tinnitus, and>47 for those with severe tinnitus. Our findings should be verified and extended in studies based on clinical assessments with multiple physicians.
Footnotes
Acknowledgments
The authors gratefully acknowledge Prof. Guanjian Liu at the Chinese Evidence-Based Medicine/Cochrane Center for excellent support with research design and statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Sichuan Province Health Department (130100).