
Abstract
Auditory and verbal abilities of children with early cochlear implant (CI) surgery usually take some time to develop, and a reference index of early development for horizontal comparisons is urgently needed to guide the mapping process and adjust rehabilitation programs. Therefore, the aim of this study was to establish a reference value for early auditory preverbal skills development in children with CI and investigate the developmental curve and influencing factors for these children. The LittlEARS® Auditory Questionnaire (LEAQ) scores of 287 eligible Chinese participants were obtained at 1, 2, 3, 6, 9, 12, 18, 24, 28, and 36 months interval after CI activation. The median and standard deviation of the LEAQ score of each hearing stage for these children with different activation ages were calculated to establish the reference values. Quadratic regression was conducted to fit the expected developmental curve of the LEAQ score (
Introduction
Over the past two decades, the age at which children receive cochlear implants (CIs) in China has decreased, while the number of CIs has increased because of the implementation of both the universal newborn hearing screening program and the deafness-gene screening program. In the Chinese Cochlear Implantation Work Guide (2013), children who were 12 months to 6 years old with severe to profound sensorineural hearing loss were recommended to have cochlear implantation (The Editorial Committee of the Chinese Journal of Otorhinolaryngology Head and Neck Surgery, the Otolaryngology Head and Neck Surgery Branch of the Chinese Medical Association, & Persons, 2014). In the expert consensus (2019) of reflections on the guideline, it was suggested to redefine the minimum age (12 months) in order to achieve early intervention (Gao Zhiqiang & Shiming, 2019). However, the auditory and verbal abilities of children with early CI implantation usually take some time to develop, and no standard reference index of early development for horizontal comparisons in children with CIs is available.
The LittlEARS® Auditory Questionnaire (LEAQ) is a validated, language-independent questionnaire reflecting children’s initial auditory behaviors (Ching & Hill, 2007; Tsiakpini, Esser, & D'Haese, 2004; Zimmerman-Phillips, Robbins, & Osberger, 2000). The following advantages made it feasible for monitoring early auditory preverbal development in children with hearing loss. Firstly, the LEAQ is sensitive to young children with impaired auditory development. Secondly, multiple dimensions of auditory and language skills are addressed by the LEAQ, with the 35 questions divided into the three domains of receptive auditory behavior, semantic auditory behavior, and expressive language skills (Coninx et al., 2009; Weichbold, Tsiakpini, Coninx, & D'Haese, 2005). Thirdly, they are all yes or no questions, which can be completed by caregivers. Compared to other questionnaires that need professionals” evaluation (the Infant-Toddler Meaningful Auditory Integration Scale, for example), answers from a parent-administered questionnaire may better reflect the actual situation of children in their daily life.
Previously, LEAQ scores of children with CIs have typically been compared to those of children with normal hearing development at the same hearing age to understand their auditory development progress (Coninx et al., 2009; L. Wang, Sun, Liang, Chen, & Zheng, 2013). However, children with CIs might show different developmental trajectories in auditory reception and expression. In the existing literature, studies have focused on auditory abilities, speech intelligibility, and language skills to explore the development of auditory and speech perception in children with CI (Geers, Nicholas, & Sedey, 2003; Guo et al., 2020; Kronenberger, Xu, & Pisoni, 2020; Schramm, Bohnert, & Keilmann, 2010; Zhang, Li, Yu, & Liu, 2021). However, these abilities could take time to accumulate, and before that, auditory preverbal skills have started to develop. This study was devoted to identifying early auditory preverbal skills during development to recognize any delays as early as possible.
In our preliminary work, we described the developmental trends of auditory preverbal skills of 33 children with hearing loss and confirmed the effectiveness of early implantation (Liu et al., 2015). The present study is based on a larger sample of pediatric CI recipients and includes a longer follow-up time. The primary purpose of this study was to establish reference values of LEAQ for pediatric CI recipients with different ages at the time of CI activation. An additional goal was to investigate the progress trajectory of early auditory preverbal behaviors of young children post CI implantation.
Materials and Methods
Participants
All candidates received CIs and were followed up at Beijing Children’s Hospital between 2012 and 2020. The inclusion criteria were as follows: (1) children with congenital hearing impairment who met the criteria for CI according to the guidelines in China and received a CI in the first three years of their life; (2) Mandarin language environment; (3) oral communication mode, and (4) no other comorbid disabilities.
Materials
We utilized the Mandarin version of the LEAQ to monitor the early auditory preverbal performance of these participants. The questionnaire consists of 35 yes-or-no questions which are designed to measure the observed receptive, semantic, and early expressive language skills of young children.
Procedures
Before the cochlear implantation, a series of audiological tests, including auditory brain stem response (ABR), auditory steady-state response (ASSR), acoustic immittance, distortion-product otoacoustic emission (DPOAE), cochlear microphonics (CM), pediatric behavioral audiometry, and aided hearing threshold, were conducted to evaluate the auditory status of the children. For children who did not have experience wearing hearing aids, aided thresholds were measured using hearing aids that were fitted by their objective auditory test results. In addition, a radiology examination and psychosocial testing were also conducted on the participants. Parents who accepted this protocol were invited for the study. Informed consent was signed by parents at the first clinical appointment. Ethics approval for this study was obtained from the Institutional Review Board of Beijing Children’s Hospital. The LEAQ assessments were assigned and completed at the time of each clinical appointment. During the CI activation, those parents of CI recipients were informed that CI mapping sessions and performance assessments were required in the following three years and the time intervals were 1, 2, 3, 6, 9, 12, 18, 24, 28, and 36 months following activation.
Statistical Analysis
For demographic information and clinical characteristics, continuous variables were described with mean and standard deviation, and categorical variables were described with numbers and percentages. In order to establish the reference values of LEAQ score for children at different hearing age (defined as “duration of CI usage”), we divided the participants into groups according to their age at CI activation. We then calculated the median and standard deviation of the LEAQ scores for each group at each stage of hearing age. Furthermore, to fit the expected developmental curve of the LEAQ score with hearing age, a quadratic regression was fitted with “hearing age” as the independent variable and “total score” as the dependent variable. The least square fit method was applied to estimate these parameters.
To explore influencing factors of the development of the LEAQ scores with the longitudinal measurement data, we constructed a linear mixed-effects model with participants as a random effect and set the hearing age (quadratic form) and the status of the inner ear and auditory nerve, pre-implantation residual hearing, and development quotient as fixed effects. Among the independent variables, the status of inner ear and auditory nerve was set as a categorical variable, which was including typical development, large vestibular aqueduct syndrome (LVAS), auditory neuropathy spectrum disorder (ANSD), Mondini, and other types of malformations. The hearing age, pre-implantation residual hearing threshold (dB nHL), and development quotient (DQ) were included as continuous variables. Hearing aid usage prior to implantation is an important factor that could affect post-implantation development. In the present study, children with profound hearing loss accounted for a large proportion, and few participants had hearing aid usage. In addition, the correlation coefficient between pre-implantation aided threshold and pre-implantation residual hearing threshold was high. For these reasons, hearing aid usage and pre-implantation aided threshold were not included in the linear mixed-effects model analysis. The significance level was set at 0.05. All statistical analyses and figures were conducted by using JMP Pro 15.
Results
Demographics
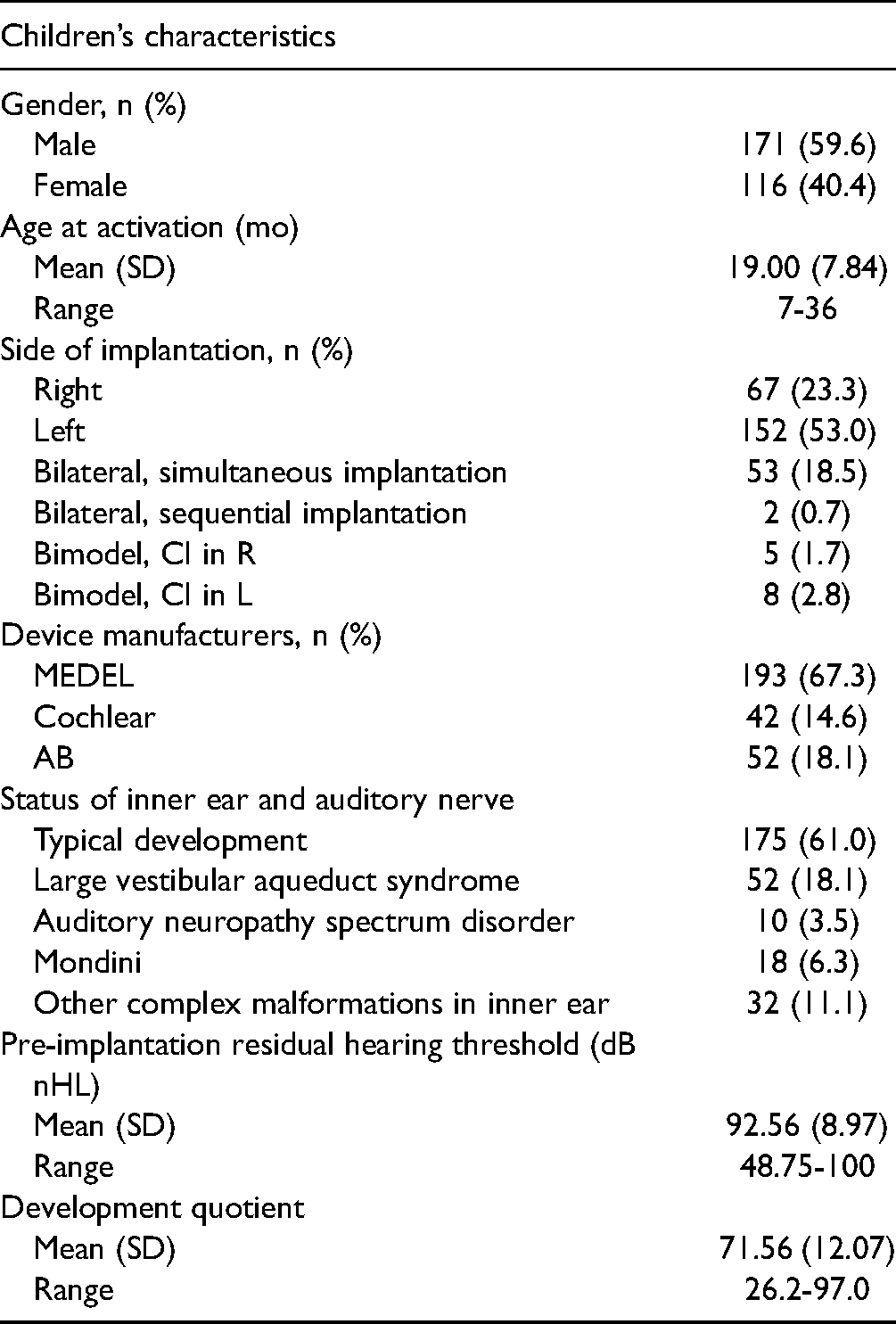
Based on the inclusion criteria of this study, a total of 287 participants were included, of which 171 were boys and 116 were girls. All participants received CIs between November 2012 and September 2020. The mean age of CI activation was 19.00 months (SD = 7.84), with a range from 7 to 36 months. In the Chinese Cochlear Implantation Work Guide (2013), children with profound sensorineural hearing loss were recommended to consider cochlear implant; children with severe hearing loss should wear hearing aids for 3–6 months first, and cochlear implantation could be performed if the progress is not ideal. In the present study, 41 participants were with severe hearing loss, 32 of them wore hearing aids for more than 3 months before the surgery. Other characteristics, including gender distribution, side of implantation, manufacturer of device, the status of inner ear and auditory nerve, pre-implantation residual hearing, and development quotient, are shown in Table 1.
Demographic Characteristics.
Reference Values of LEAQ for Children with CI
A total of 1057 questionnaires were collected, with which we established the reference values of LEAQ for children with CI with different activation ages at each hearing period (Table 2). The result showed that general trends of different activation age groups were essentially the same, with subtle differences.
Reference Values of LEAQ Score Along with Hearing age for Children with CI with Different Activation Ages.

The clinical information of children in each activation age group is shown in Table 3. In this study, children whose CIs were activated at 13–18 months accounted for the largest proportion, followed by children whose CIs were activated before 12 months, who also had the largest number of bilateral implantations. The longest activation age group (31–36 months) had the largest amount (57.14%) of the inner ear and auditory nerve anomalies, including ANSD and Mondini each accounting for 10.71%. Only 42.86% of children in this group had normal cochlear structure and auditory nerve, which is lower than the other four groups. The largest proportion of children with LVAS was in the group of 25–30 months, accounting for 33.33%, followed by the group of 31–36 months, accounting for 21.43%.
Clinical Characteristics of Children with CI with Different Activation Ages.

LVAS: Large vestibular aqueduct syndrome
ANSD: Auditory neuropathy spectrum disorder
The Developmental Trajectory of Early Auditory Preverbal Behaviors Post CI
In order to investigate differences between the children with CI and their hearing-age-matched normal-hearing peers, we further established an expected curve of the Mandarin version of the LEAQ for pediatric CI recipients and compared the curve with the published norm data (Figure 1). The fitted developmental curve of CI recipients can be expressed as a function of LEAQ score (

The expected curve of LEAQ score by duration of CI use for infants and toddlers with hearing loss (N = 287, red lines), compared with data on normal-hearing infants by chronological age (green lines) (adapted from Wang et al. 2013).
In addition, in order to clarify the influence of each parameter on the score, we calculated the formula considering multiple variables.
The development trend of receptive, semantic, and early expressive language skills of children with CIs are shown in Figure 2. The score of receptive auditory behavior increased rapidly in the first 5 months post CI activation and began to level off after 9 months. The progress rate of semantic auditory behavior was slower than receptive auditory behavior and gradually reached the plateau after 17 months of CI use. The score of expressive language skills was close to 0 at the beginning of CI use, then increased at a steady and slow rate, and gradually became stable after 20 months of CI use.

The expected curves for receptive auditory behavior score, semantic auditory behavior score, and expressive language skills score for Children with CIs.
In order to explain the difference in scores of early auditory preverbal skills reasonably, a linear mixed-effects model was constructed (Table 4). These results showed that early auditory preverbal performance was significantly related to the duration of CI use. Specifically, the longer the hearing age was, the higher score they received. For the status of inner ear and auditory nerve, children with LVAS had significantly higher scores and children with ANSD had significantly lower scores than children without any anomalies. The malformation of Mondini showed no obvious effect on LEAQ scores. Besides, children with higher DQ and longer activation ages had better performance after CI activation. Parameter estimation indicated that the association of pre-implantation residual hearing was not statistically significant post-CI.
Discussion
Based on the longitudinal data from National Center for Children’s Health of China, the present study established reference values of LEAQ for pediatric CI recipients with different CI activation age. To investigate the progress trajectory of early auditory preverbal behaviors post CI, we fitted the expected curve of the LEAQ for children with CIs and explored influencing factors of LEAQ scores. These results can effectively assist clinicians and parents to have a rational reference for postoperative rehabilitation.
In previous studies, researchers have found that the post-CI performance of infants with hearing loss was as good as or even better than their hearing-age-matched normal-hearing peers, although they exhibited very limited auditory skills before CI surgery (Kishon-Rabin, Taitelbaum-Swead, Ezrati-Vinacour, & Hildesheimer, 2005). However, the development pattern of CI recipients might be different from normal-hearing children. The progress of auditory preverbal skills could not be entirely attributed to the benefits of CI; instead, the accumulation of auditory experience and maturation of cognitive abilities may also play a role. In their studies, Kishon-Rabin et al. proposed that the duration of CI use and age of implantation were both important factors to be considered in the evaluation of early auditory development, while quantifying the contribution of each factor separately could be difficult (Kishon-Rabin et al., 2005). Therefore, in the present study, we described the value of LEAQ for children with different CI activation ages at different hearing ages, instead of only taking hearing age into account.
The benefits of early cochlear implantation have been widely documented (Leigh, Dettman, Dowell, & Briggs, 2013). In the present study, it was indicated that the children who had early implantation exhibited lower initial LEAQ scores but progressed faster and achieved higher scores in the later stage. By contrast, children with delayed implantation progressed at a slower rate and reached a lower plateau along with the duration of CI use. Data from both animal models and deaf children have provided evidence that the maturation of auditory cortex has a sensitive period during the first 2–4 years of life. During this period, auditory stimulation can affect the development of cortical function to the greatest extent, and it is also the period during which auditory and speech ability grows most rapidly (Kral, Dorman, & Wilson, 2019). Therefore, hearing intervention before this period would help children with hearing loss obtain better rehabilitation. All participants in this study received their CI before this period, but there were still unexplained individual differences in developmental outcomes. In recent years, studies have used EEG, fMRI, fNIRS, and other technologies to explore the development of the auditory cortex, and have demonstrated that the duration of auditory deprivation also affects the post-implantation rehabilitation significantly, especially for young infants/toddlers (Glick & Sharma, 2017). The duration of auditory deprivation here refers to the duration of severe to profound hearing loss. If the auditory ability of the participant were improved after intervention, such as hearing aid or CI, it would be considered that the participant has the ability to acquire external sound stimulation and has less negative effects from hearing deprivation. There were 32 children who had a hearing aid fitted before the surgery. This had shortened the duration of deprivation, accumulated auditory experience, and could affect post-implant development. The maturity of the auditory cortex depends on the input of auditory stimulation, which promotes the formation of stable synapses in the cortex. Long duration of auditory deprivation degenerates the function of the auditory pathway, and cross-modal reorganization could happen to the cerebral cortex, that is, the auditory cortex may be replaced by the visual cortex or other functional cortex. Coez et al. (2021) observed the evolution of perfusion with age in deaf and normal-hearing children. Brain areas that showed abnormal rest-cerebral blood flow were associated with deafness. They found that the temporal perfusion evolution of deaf children was significantly different from that of normal-hearing children (Coez et al., 2021). Their study confirmed the effect of early auditory deprivation on cortical function. The changes of cortical function occurred earlier than previously stated, with the study showing significant differences in cortical connections between children with hearing loss and with normal hearing in infancy (S. Wang et al., 2019; Wu et al., 2016), which is much earlier than three years of age for auditory intervention. The group who had a CI implanted between 25–30 months of age had a rapid improvement, which was not consistent with the previous evidence. The reason could be that a higher proportion of children in this group were with LVAS, and children with LVAS might have auditory experience prior to CIs which could lead to a better performance. The outcome of children with LVAS has also been confirmed in the following analysis of influencing factors. Participants with malformation were not excluded when establishing the reference values as it could truly reflect the current situation of cochlear implantation in Chinese children, that bilateral implantation accounted for a higher proportion in early intervened children and children with inner ear malformation or ANSD accounted for a higher proportion in older candidates.
Post-implantation therapy and rehabilitation could also be an important factor influencing development. Factors such as auditory and speech rehabilitation training, daily usage of devices, parents” educational level, annual household income, living environment, and so on, have been identified as potentially affecting the auditory development of children with CIs (Park et al., 2013; Wiseman, Warner-Czyz, Kwon, Fiorentino, & Sweeney, 2021; Zhao et al., 2019). In the present study, 91.30% of participants were involved in at least one year of auditory and speech rehabilitation after implantation; 32.77% of caregivers systematically learned about how to interact with their children to enhance auditory development; 55.17% of families have full-time guardians; other children did not receive professional rehabilitation due to economic and geographical reasons, which could affect the outcomes.
To tentatively explore the pattern of early auditory preverbal behavior development post CI, we established the expected curve of LEAQ score for children with hearing loss who received CIs younger than 20 months of age, and described the developmental trajectory of 3 domains of LEAQ evaluation contents separately. We found that the score of receptive auditory behavior had the fastest growth rate and was also the first measure to reach a plateau post CI, immediately followed by the trajectory of skills of semantic auditory behavior. It took time to develop expressive language skills after cochlear implantation, so the trajectory of that measure had steady and continuous progress after auditory rehabilitation, without a rapidly growing period. However, the basic function of LEAQ is not for evaluating the development of receptive, semantic, and expressive domains separately. As a result, the current interpretation must be regarded as exploratory, and requires further confirmation..
There have been studies demonstrating that preverbal auditory skills could predict spoken word perception and production outcomes in young hearing-impaired children (Tait, Nikolopoulos, & Lutman, 2007). In the present study, we explored factors affecting auditory preverbal development. Children with LVAS developed better preverbal auditory skills than typically developing children after cochlear implantation. Children with LVAS might have experienced some hearing in early life and may thus have experienced some early learning, resulting in greater progress after implantation (Demir et al., 2019).
Spiral ganglion neurons were diminished in individuals with Mondini dysplasia (Kaya et al., 2017), so it could be difficult for those children to obtain similar benefits from CI compared to typically developing children. However, data from the present study revealed no significant effects of Mondini on early auditory and preverbal skills. Qi et al. (2019) compared the meaningful speech and speech intelligibility post CI between 108 children with Mondini dysplasia and 592 children with radiologically normal inner ears. Their results showed that compared to age-matched children with normal inner ears, children with Mondini dysplasia were able to achieve similar speech skills over the long term. These studies have demonstrated that cochlear implantation was an effective intervention for children with Mondini dysplasia and provided them the opportunity to acquire similar outcomes.
The present study revealed a negative impact for children with ANSD on the development of early auditory and preverbal skills compared with typically developing ones. Nevertheless, we still suggest that prelingual children with ANSD, who failed to show expected oral and auditory progress after extensive rehabilitation with conventional hearing aids, should be considered for cochlear implantation, because long-term outcomes of children with ANSD post CI are promising (Attias et al., 2017; Ehrmann-Muller, Back, Kuhn, Hagen, & Shehata-Dieler, 2020).
Pre-implantation residual hearing threshold was not one of the significant influencing factors in the present study. However, a mounting body of evidence has suggested that there is a better-developed tendency in children with better preimplantation residual hearing post CI. Niparko et al. conducted a prospective, longitudinal, and multi-center study on the spoken language development involving 188 children and concluded that outcomes were positively associated with the amount of residual hearing prior to CI (Niparko et al., 2010). A study of early auditory skills development in aided infants and toddlers with varying degrees of hearing loss showed that pediatric hearing aid users with better residual hearing achieved more auditory skills 2 months after initial hearing aids fitting than those with less residual hearing (Ben-Itzhak, Greenstein, & Kishon-Rabin, 2014). Based on the aforementioned observations, it can be hypothesized that preoperative residual hearing was valuable in predicting speech perception and production outcomes. In addition, some research has suggested that residual hearing could affect the rate of development for post implantation (Schaefer, Sahwan, Metryka, Kluk, & Bruce, 2021). The parameter was not measured in this study, which made it one of the limitations of this study.
The major advantage of this study was that it focused on auditory preverbal behaviors, which reflect auditory and speech development issues of young children with CIs at an early stage. Also, based on the data from the National Center for Children’s Health of China, we utilized a large number of participants who all undertook the same measures at multiple post-CI intervals, which could better represent the actual situation of children with CIs in China and ensure the generalization of the study. Furthermore, we established reference values for children with different activation age, which were very specific and could play an important role in the clinical management for pediatric CI recipients during the early stage of activation.
However, there were still some limitations. First, the rate of attrition was an issue that cannot be ignored. Although efforts were made to complete all assessments in a timely manner, it still proved difficult to accomplish all measures at each test interval. Second, we did not include factors such as non-implanted ear intervention, parents” involvement, post-implant therapy or rehabilitation methods, or residual hearing pre- and post-implantation, all of which could also influence the auditory preverbal performance of pediatric CI recipients.
Conclusions
In the present study, reference values of LEAQ scores for children with CIs with different activation age were established, from which audiologists and parents may obtain a reliable reference to make further decisions regarding management plans. The expected curve of the LEAQ in Mandarin-speaking children demonstrated that early preverbal auditory skills development was approximately the same between CI recipients and normal-hearing children, and even better performance could be observed among CI recipients. Those influencing factors for preverbal auditory skills were investigated and these findings could provide scientific evidence for the selection of clinical interventions.
Effect estimates of influencing factors on auditory preverbal skills.

**p < 0.01.
*p < 0.05.
Footnotes
Acknowledgments
The authors thank all participants in this study. This research was supported by Beijing Talents Project (2019), and the Natural Science Foundation of Beijing, China (H2018316006), and the Special Fund of the Pediatric Medical Coordinated Development Center of Beijing Hospitals Authority (XTYB201826), and the Capital's Funds for Health Improvement and Research (No. 2022–1–2023), and the Beijing Health Technologies Promotion Program (BHTPP202045). In addition, we would like to thank Guo Ying for his help to improve the wording and flow of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Beijing, China, Special Fund of the Pediatric Medical Coordinated Development Center of Beijing Hospitals Authority, Beijing Health Technologies Promotion Program, Capital's Funds for Health Improvement and Research, Beijing Talents Project, (grant number H2018316006, XTYB201826, BHTPP202045, No. 2022-1-2023, 2019 A34).