
Abstract
The main aims of tympanoplasty are eradication of chronic middle ear disease, repair of the tympanic membrane, and restoration of hearing. Nitrous oxide (N2O) is not a commonly preferred anesthetic agent for tympanoplasty because this agent may increase middle ear pressure and displace the graft. In this study, we researched the surgical outcomes of the underlay tympanoplasty performed with N2O anesthesia. Patients who underwent tympanoplasty were included in this prospective study. A type 1 tympanoplasty was performed in all patients using the underlay technique. Patients were randomized to groups that did and did not receive N2O. Preoperative and postoperative hearing thresholds were evaluated, postoperative pain scores were recorded, and the differences between the groups were statistically evaluated. There were 44 patients who received N2O and 44 who did not. The graft success rate was 93.2% in the N2O-receiving group and 84.1% in the nonreceiving group (P > .05). Hearing levels improved significantly after surgery in each group (P < .05), but the difference between the groups was not significant (P > .05). The postoperative pain score was 3.72 ± 1.3 in the N2O-receiving group and 4.45 ± 2.3 in the nonreceiving group (P > .05). Nitrous oxide is a cheap, safe, and readily available anesthetic agent that provides acceptable success rates in patients undergoing tympanoplasty.
Introduction
Chronic otitis media, a disease commonly encountered in otorhinolaryngology practice, is characterized by conductive hearing loss and perforation of the tympanic membrane. Tympanoplasty is a surgical procedure to eradicate middle ear disease, reconstruct an intact tympanic membrane, and restore hearing physiology. Different techniques and graft materials have been used with high success rates. 1 –3 A successful operation is shown by the presence of an intact tympanic membrane and closure of the air-bone gap (ABG). The pre-, post-, and intraoperative condition can affect the surgical outcome. The presence of an active middle ear infection, edema of the middle ear mucosa, or dysfunction of the Eustachian tube can affect middle ear pressure. Factors affecting middle ear pressure are crucial when integrating a graft with the tympanic membrane.
Nitrous oxide is a cheap and widely used inhalation anesthetic for general anesthesia. Nitrous oxide has less of a depressive effect on the cardiovascular system compared to other inhalation agents. 4 In addition, an analgesic effect of N2O has been reported. 4 It is known that N2O is a highly soluble agent that accumulates in the body cavity due to its dissolution properties. Accumulation of this agent in closed spaces of the body increases the pressure in these areas. Gas expansion in the tympanic cavity in cases of Eustachian tube dysfunction raises middle ear pressure. An increase in middle ear pressure is not a desirable condition during a tympanoplasty. Karabiyik et al reported that N2O was not a useful agent for general anesthesia during tympanoplasty, 5 as changes in middle ear pressure can displace the graft. Graft lateralization has been observed as a postoperative complication when N2O is used for tympanoplasty. 6
The underlay tympanoplasty technique involves placing the graft material on the medial side of the manubrium mallei and remnant tympanic membrane. In this technique, filling the middle ear with sponge gel is very important to provide medial support to the graft and ensure contiguity between the graft and the tympanic membrane. We observed that the increased middle ear pressure due to N2O allowed the graft material to move toward the remnant membrane, providing sufficient contact with the graft. In this study, we investigated the efficacy of N2O as an anesthetic agent during underlay tympanoplasty.
Patients and Methods
This prospective study was performed with approval of our local ethics committee (YYUKAEK-31.01.2018/2). Patients who were scheduled to undergo tympanoplasty for treatment of chronic otitis media were included in the study as were those who had a dry central tympanic membrane perforation. However, patients who had cholesteatoma, adhesive otitis media, attic perforation, ossicular chain erosion, or a history of tympanoplasty were excluded. All patients had inactive mucosal chronic otitis media. The patients were informed about the study, and informed consent was obtained from all participants. Patients were randomized to tympanoplasty with and without N2O anesthesia groups. Sevoflurane was used to provide general anesthesia for all patients in the N2O nonreceiving group. Type 1 tympanoplasties were performed in all patients.
All surgeries were performed by the same surgeon (U.D.). Maintenance of general anesthesia was achieved with or without N2O. A postauricular approach was used for the surgery. After the tympanomeatal flap was elevated, the middle ear was reached under the annulus. The status of the ossicles was checked, and patients with ossicular problems were excluded from the study. The tragal cartilage perichondrium was harvested as graft material. The middle ear was filled with a sponge gel, and the perichondrium was placed under the remnant tympanic membrane and the malleus. The lateral side of the tympanic membrane was supported with sponge gel. Nitrous oxide was terminated after placing the graft. The tympanomeatal flap was reposed, and the skin was sutured. The patients were followed up on day 14, and at 1, 2, and 3 months postoperatively. The presence of reperforation was checked by microscopic evaluation. Silver nitrate was used to close small perforations. The presence of any perforation was recorded at the 3-month visit and was accepted as graft failure. The patients rated their postoperative pain level from 1 (the least pain) to 10 (the most pain) using a visual analog scale.
Air conduction (AC) and bone conduction (BC) hearing thresholds were investigated at 500, 1000, 2000, and 4000 Hz preoperatively and at 3 months postoperatively. The gap between the AC and the BC thresholds was considered as the ABG.
The normality of the distribution of variables was evaluated with the Shapiro-Wilk test. Independent nonparametric variables were compared to the Wilcoxon rank test, and independent parametric variables were compared with an independent t test. Differences between preoperative and postoperative hearing thresholds were evaluated with the paired t test. Fisher exact test was used to compare the success rate between the 2 study groups. The difference in pain scores between the study groups was evaluated by the Mann-Whitney U test. The statistical analysis was performed using SPSS 16.0 software (IBM Corp, Armonk, New York). A P value < .05 was considered significant. A power analysis was performed to determine the required sample size.
Results
There were 44 patients in the N2O group and 44 in the non-N2O group. The demographic information of both groups is shown in Table 1.
Demographic Data of the Patients.
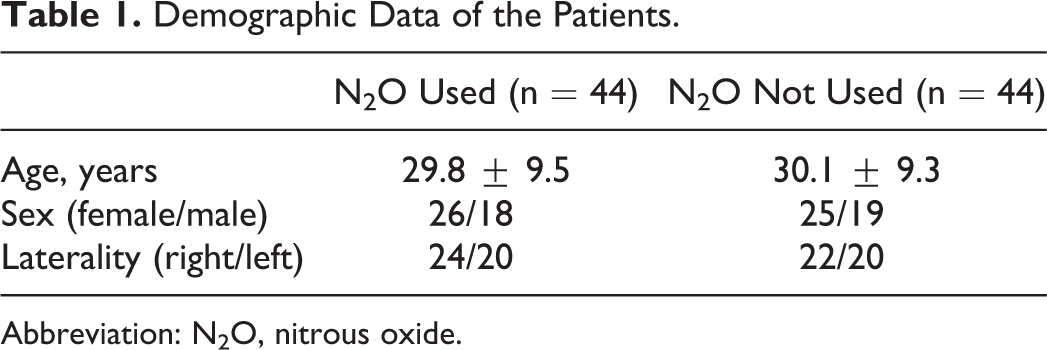
Abbreviation: N2O, nitrous oxide.
Reperforations were detected in 3 patients in the N2O group and in 7 patients in the non-N2O group; the success rates of the groups were 93.2% and 84.1%, respectively (Table 2). The success rate of the N2O group tended to be higher than that of the non-N2O group, but the difference was not significant (P > .05). All reperforations were detected in the anterior superior part of the tympanic membrane. No graft lateralization was observed during follow-up. The postoperative pain score was 3.72 ± 1.3 in the N2O group and 4.45 ± 2.3 in the non-N2O group (P > .05; Table 2). No complications related to the anesthetic agent were observed. Preoperative and postoperative BC and AC thresholds were similar between the 2 groups (P > .05; Table 3).
Postoperative Findings of the Patients.
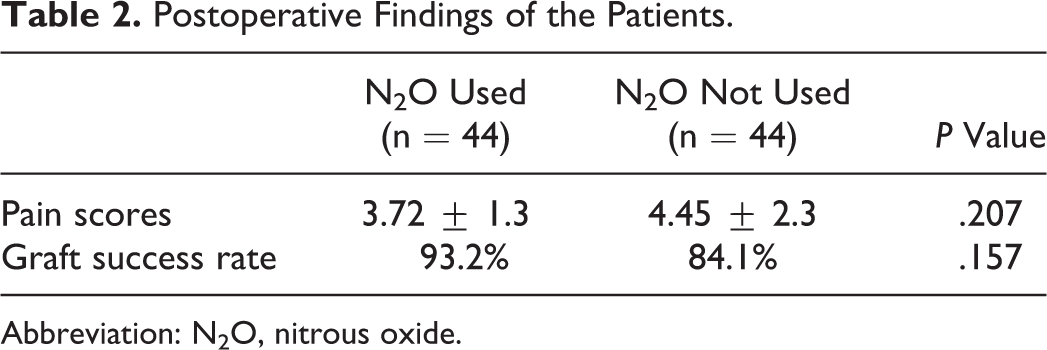
Abbreviation: N2O, nitrous oxide.
Preoperative and Postoperative Audiologic Findings.
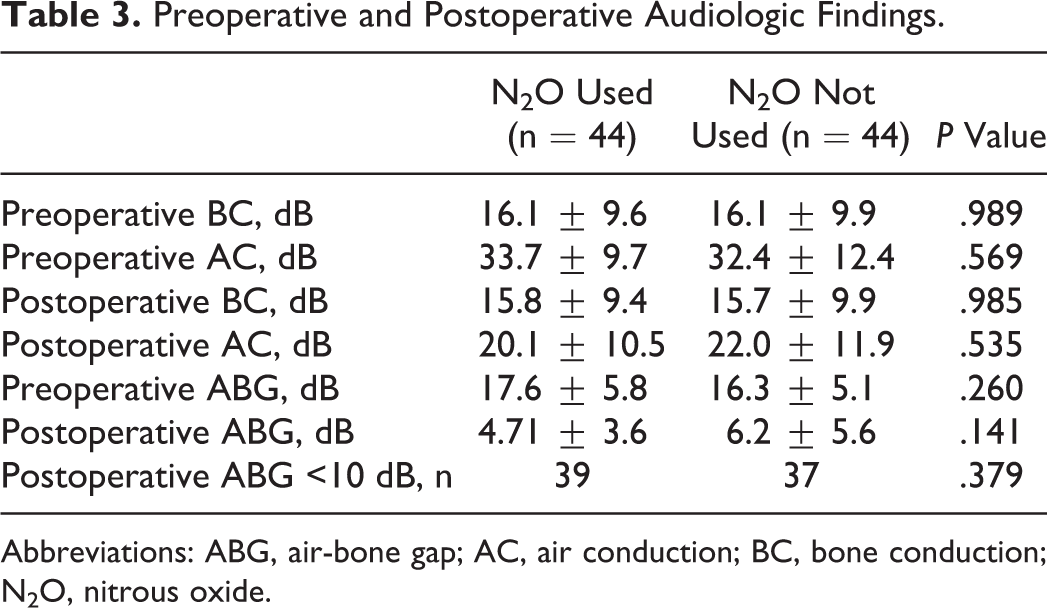
Abbreviations: ABG, air-bone gap; AC, air conduction; BC, bone conduction; N2O, nitrous oxide.
Discussion
Chronic otitis media is a very common disease characterized by conductive hearing loss and tympanic membrane perforation. Tympanoplasty is used in the treatment of this disease and involves placement of a graft to close a tympanic membrane defect. The main goal of this surgery is to reconstruct an intact membrane and obtain normal hearing thresholds. Different tympanoplasty techniques have been shown successful outcomes. 7 –9 Underlay tympanoplasty involves placing the graft under the remnant tympanic membrane and manubrium mallei. 10 In a meta-analysis, Tan et al reported that similar outcomes were observed between the underlay and the overlay techniques, but graft lateralization was observed mostly after the overlay technique. 11
Nitrous oxide is a cheap and readily available anesthetic agent with less of a depressive effect on the cardiovascular system than certain other anesthetics. However, N2O can increase pressure in closed cavities, such as the middle ear. 12 Increased pressure in the middle ear during tympanoplasty is considered responsible for displacement of the graft. 13 In contrast, we observed that increased middle ear pressure during underlay tympanoplasty with N2O anesthesia led to elevation of the perichondrium graft. Thus, contact of the graft with the tympanic membrane and the malleus increased due to the increased middle ear pressure. Accordingly, we hypothesized that using N2O for an under–under tympanoplasty may increase the success rate of this surgery.
In this study, the intact graft rate tended to be higher in the N2O group, but the difference was not significant. Closure of the ABG is an important factor for a successful outcome. We observed a significant decrease in the ABG after surgery in both groups. The postoperative pain score in the N2O group tended to be lower than that in the non-N2O group, but the difference was not significant. Becker and Rosenberg reported that N2O provides an analgesic effect, unlike other anesthetics. 4 Additionally, no graft lateralization and no complications related to the anesthetic agent were observed in that study. Kouhi et al reported 10.3% graft lateralization after over–under tympanoplasty in their N2O group. 6 We placed the graft under the manubrium mallei, which may have been responsible for the absence of graft lateralization with N2O anesthesia in our study.
Previous studies have reported that use of N2O might lead to graft failure after tympanoplasty. 5,13 Ramirez-Camacho and Jimenez demonstrated that using N2O during overlay tympanoplasty did not affect long-term hearing outcomes. 14 They also suggested stopping the N2O 30 minutes before graft placement. In the present study, we stopped the N2O after placing the graft under the malleus to ensure sufficient elevation of the graft. Kouhi et al presented similar hearing and graft success rates in N2O-receiving and nonreceiving groups. 6 They hypothesized that increased middle ear pressure may have increased graft and membrane contact. Cartilage and perichondrium as graft materials have different elasticities and middle ear pressure does not affect them equally. Graft–membrane contact occurs with increased pressure, and adhesive forces between the graft and the membrane may be helpful. On the other hand, the malleus is a stronger structure than the tympanic membrane, with respect to preventing lateralization of the graft material.
In this study, we speculated that N2O might be a useful anesthetic agent for underlay tympanoplasty. The number of patients in this study was relatively low and we presented only short-term outcomes of the tympanoplasties. However, the power of the study was high, at more than 0.80. Future studies that include larger groups will provide more information about the utility of N2O in tympanoplasty.
Conclusion
Hearing outcomes and postoperative pain scores were similar between patients who did and did not receive N2O as an anesthetic during tympanoplasty. No significant difference in graft success rates were observed between the groups. Taken together, N2O did not affect the success rates of the surgery or the postoperative hearing outcomes. Nitrous oxide can be considered as a cheap, safe, and effective anesthetic agent for tympanoplasty.
Footnotes
Authors’ Note
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 2000 Helsinki declaration and its later amendments or comparable ethical standards. The local ethical committee approval for prospective clinical research was obtained (YYUKAEK-31.01.2018/2). Informed consents were obtained from all individuals.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.