
Abstract

It is safe to argue that Markus Hajek was the most influential rhinologist of the early 20th century. While he credits the work of giants, especially Zuckerkandl, Weichselbaum, and Schäffer in anatomy and pathology, and Killian, Hartmann, Luc, Mikulicz, Halle, and Grünwald in surgery, Hajek’s own descriptions of anatomic variants and pathological anatomy are without equal. At least as important as his contribution to rhinology was his desire to communicate surgical knowledge to otolaryngologists around the world. Scores of students visited his clinic in Vienna to study and hone their skills. More were influenced by his popular textbook, which, through 5 German editions 1 and an English translation 2 (Pathology and Therapy of Inflammatory Diseases of the Sinuses and Nose), became the standard text of sinus disease and surgery.
Markus Hajek (Hájek pronounced in Czech is HAY-yek) was born the son of a peddler in 1861, in a town on the Austro-Hungarian and Romanian borders. He arrived in Vienna in the 1880s, penniless and unable to speak German. 1 By dint of will and intelligence, he was accepted to university, and in 1885, he received his doctorate in medicine. He chose post-graduate study in rhinology—a poorly-respected specialty and thus available to the medical underclass. Hajek received specialty training at the Rudolfstiftung Hospital under Leopold Schrötter von Kristelli and at the General Polyclinic under Johann Schnitzler. Hajek was a brilliant researcher and a popular teacher. He quickly rose through the academic ranks, and by 1919, he had become professor at the University of Vienna and Director of the Rhinolaryngological Hospital.
Hajek explored both open approaches to the sinuses and endonasal surgery. He became convinced that for most primary cases, approaching disease through the nose provided superior results with acceptable morbidity. His years of dissecting autopsy specimens enhanced his knowledge of the many variations in sinus anatomy. Thus, he could anticipate and understand the anomalies he encountered when working through the small nasal opening with only a head mirror for illumination. While sinus radiographs were available in the latter half of his career, he operated with only mental images of the sinuses early on. Hajek argued strongly that the endonasal approach had its limits. When extensive pneumatization or bleeding limited visualization, or when faced with orbital or intracranial complications, open approaches were preferred.
Hajek held that rhinoscopy, rather than transillumination or radiography, led to correct diagnosis in sinus disease. When reading Hajek’s description of intranasal ethmoidectomy, one hears the mantras of FESS as expounded much later by Messerklinger, Stammberger, and Kennedy. He firmly believed that adequate sinus drainage and ventilation allowed diseased mucosa to recover.
During both ethmoidectomy and frontal sinus surgery, Hajek took down the uncinate process with a strong hook or blade and resected the anterior portion of the middle turbinate for access to the hiatus semilunaris. He resected the ethmoid air cells from anterior to posterior with a combination of his hook, curettes, and Harmann’s through-biting forceps (Figures 1 and 2). Polyps were removed, but mildly-diseased mucosa was left in place to heal. Cells free of disease were left unopened.
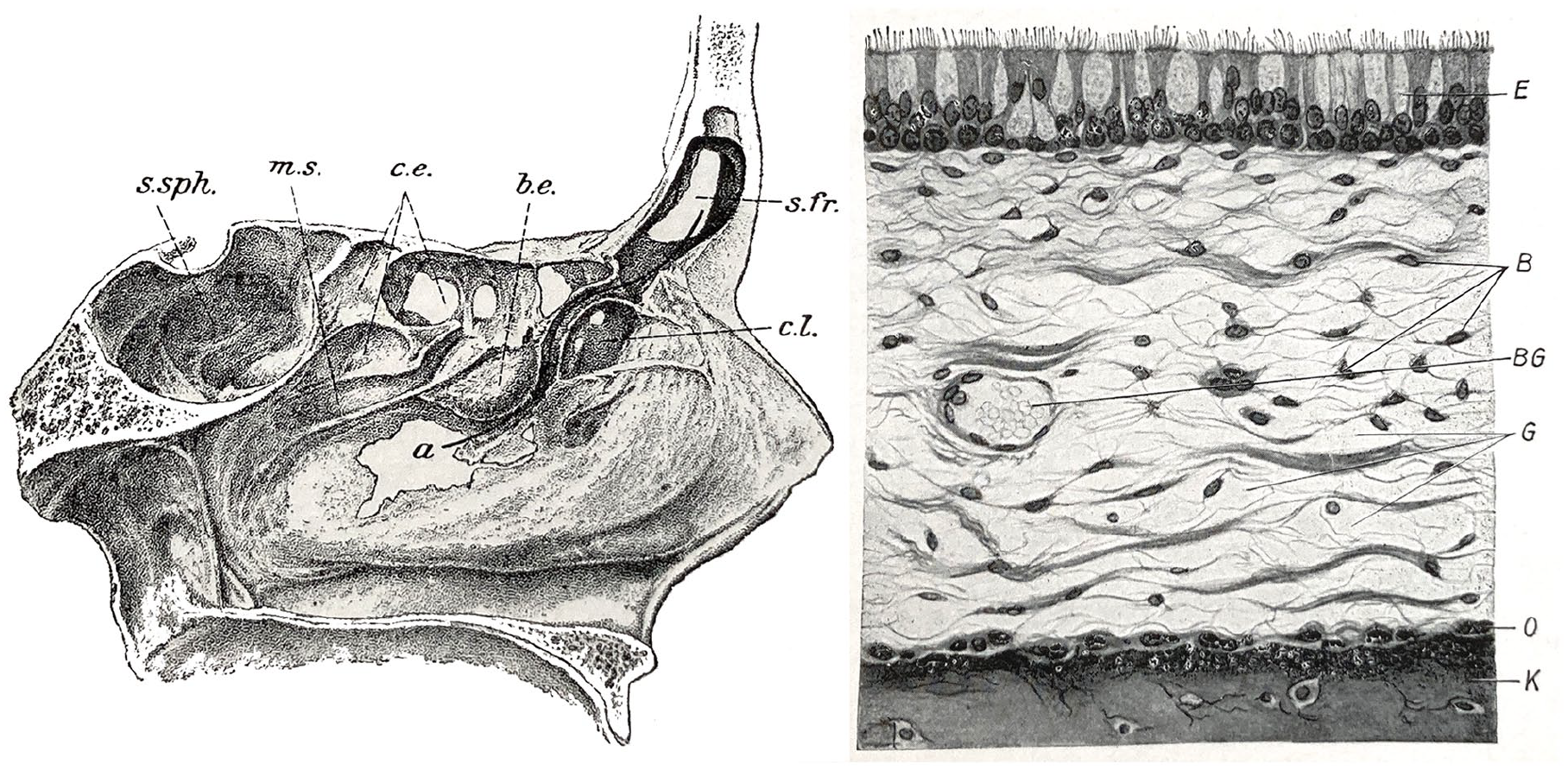
(Left) Hajek’s dissection of the lateral nasal wall with a probe in the frontal recess. (Right) Histology of the nasal sinus mucosa. Note: ciliated epithelium. 2
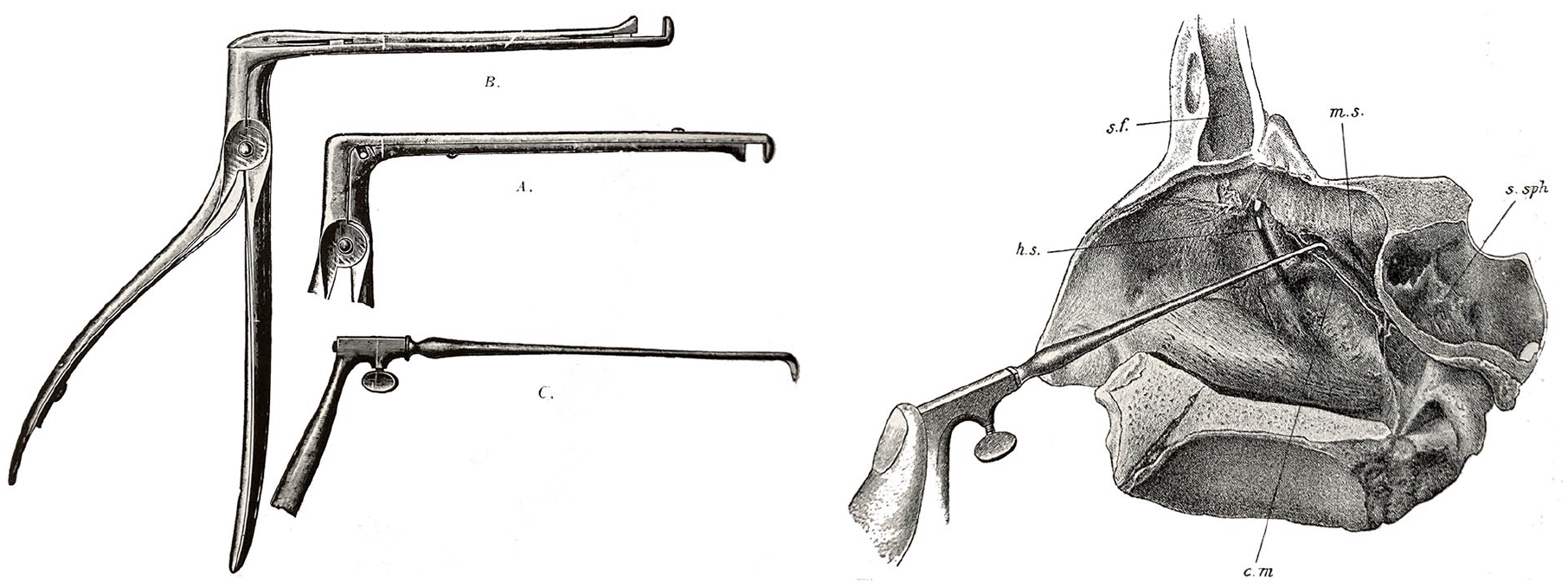
(Left) Hajek’s instruments for intranasal sphenoidotomy. (Right) Illustration of Hajek’s technique for removing the posterior ethmoid cells to approach the sphenoid sinus. 2
In 1904, Hajek detailed the endonasal approach to the sphenoid sinuses. 3 He emphasized that the anterior wall of the sphenoid could not be adequately opened without resecting portions of the posterior ethmoid labyrinth—a concept that laid the groundwork for transsphenoidal hypophysectomy. 4
Hajek appreciated the dangers of intranasal surgery before computed tomography showed individual anatomy and endoscopes allowed continuous visualization during surgery. His textbook includes the sections, “Unpleasant Accidents from Antrum Puncture,” and “Accidents in Probing the Frontal Sinus.” During ethmoidectomy, he describes orbital emphysema and blindness from breeching the lamina papyracea, and meningitis and death from violation of the ethmoid roof.
I have seen only one case (of death) . . . one of my assistants could not complete the operation. Before the labyrinth was sufficiently opened, the patient had a hystero-epileptic attack. . . Meningitis followed 3 days later.
Sadly, major complications by surgeons less skilled than Hayek doomed endonasal sinus surgery for decades. It was not until the 1980s that endoscopes made the technique safe for most otolaryngologists.
Hajek’s prominence in Viennese medicine could not shield him from the horrors of history. As a Jewish academic, he was swept up in the Nazi purges following the 1938 Anschluss. 5 In letters to his former student Karl Moriz Menzel—who had already fled to Brussels—Hajek revealed his growing fear of persecution and the urgency to escape. He would eventually find refuge in London, where he died in 1941, far from the surgical theaters of Vienna where he had once revolutionized sinus surgery.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.