
Abstract
Orbital apex syndrome (OAS) is a rare condition that usually occurs due to damage to surrounding inner and surrounding bone tissue. Orbital apex syndrome may result from a variety of conditions that cause damage to the superior orbital fissure and to the optic canal leading to optic nerve (II) dysfunction. We recently experienced a rare case of sphenoidal Aspergillosis, which damaged the adjacent cavernous sinus structures and led to the definite symptom of bilateral OAS in a 77-year-old male. We present this rare case with a brief review of these disease’s entities.
Introduction
Orbital apex syndrome (OAS) is characterized by the signs and symptoms which were developed by the involvement of various structures around orbital apex by a disease process. 1 The orbital apex disorders include 3 groups: superior orbital fissure syndrome, OAS, and cavernous sinus syndrome. All 3 groups have similar clinical findings and various etiologies. Superior orbital fissure syndrome involves the cranial nerves (CNs) III, IV, VI and the ophthalmic division of CN V. Cavernous sinus syndrome affects the maxillary divisions of CN5 and the sympathetic nerve without involving the optic nerve. 2 The clinical presentation of OSA is visual loss and ophthalmoplegia, periorbital pain, proptosis, diplopia, and optic neuropathy which involving CNs II, III, IV, V1, and VI. 1
Orbital apex syndrome is a rare condition that usually occurs due to damage to surrounding inner and surrounding bone tissue. Orbital apex syndrome may result from a variety of inflammatory, infectious, neoplastic, and vascular conditions that cause damage to the superior orbital fissure and to the optic canal leading to optic nerve(II) dysfunction. 1,3 Individuals with immunocompromised disease such as uncontrolled diabetes and immunosuppressive agents are susceptible to the fungal infections. 1 Orbital apex syndrome due to mixed bacterial sphenoid sinusitis can be life-threatening if there is disease invasion through ophthalmic vessels or bone fissures, leading to intracranial involvement. 4 Orbital apex syndrome due to Aspergillus sphenoid sinusitis is a rare condition.
In this study, we have introduced the recent bilateral OAS case by the progression of sphenoid sinus Aspergillus. The retrospective study was approved by the institutional review board (GAIRB2020-176).
Case Report
A 77-year-old male patient has visited the hospital with headache, bilateral eye pain, diplopia, and visual disturbance for 1 month. There was no history of trauma, surgery, or dental treatment, with a diabetes that was poorly controlled.
Ophthalmologic examination have found that ptosis and visual disturbance was in the both eyes. Due to visual loss in both eyes, visual activity test cannot be performed. Also, direct and indirect light reflex was performed but there were no responses. Eye movement was significantly reduced in all directions, such as up, down, left, and right with impairment of CNs II, II, IV, V1, and VI. No specific findings were observed in the nasal endoscopy examination (Figure 1). Computed tomography examination revealed unevenly enhanced soft tissue density with calcification density in both sphenoid sinus. The soft tissue mass that destroyed the septum and cribriform plate, invaded the orbital apex and optic nerve, and invaded to the brain (Figure 2). magnetic resonance imaging has shown that the dura matter was intact.

Extraocular movements in 9 cardinal positions of gaze showed total ophthalmoplegia of both eye.
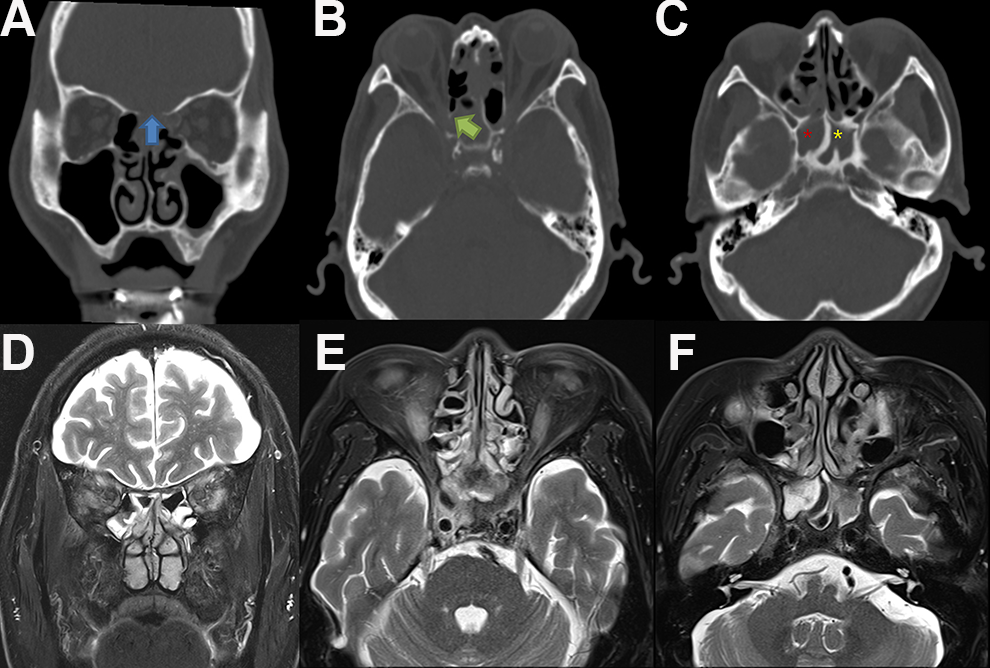
Computed tomography (CT) and magnetic resonance imaging (MRI) findings. (A-C) Coronal and axial noncontrast-enhanced orbital CT scan revealed soft tissue density at frontal, ethmoid, and sphenoid sinus with bony erosion on ethmoid roof, lamina papyracia, crista gali, and perpendicular erosion. (Blue and Green arrow) Both sphenoid sinusitis was seen (red and yellow star). (D-F) Axial and coronal T2-weighted MRI scan showing hyperintense lesion in both ethmoid and sphenoid sinus and compression of both orbital apex with bony erosion but dura mater was intact.
Endoscopic surgical removal was performed in the sphenoid sinus using navigation system (Medigator). Purulent secretions with dark brown mud-like lesions were observed in the sphenoid sinus (Figure 3). Abscess was found in the septum and the necrotic granulation tissue with thick purulent discharge was attached to dura matter of the cribriform plate area. After aggressive endoscopic removal of the necrotic tissue, cerebrospinal fluid (CSF) leakage was leaked from the dura matter and then the CSF leakage site was closed with the septal mucosa (Figure 3). Histopathology finding has shown Aspergillus fumigatus (Figure 4).
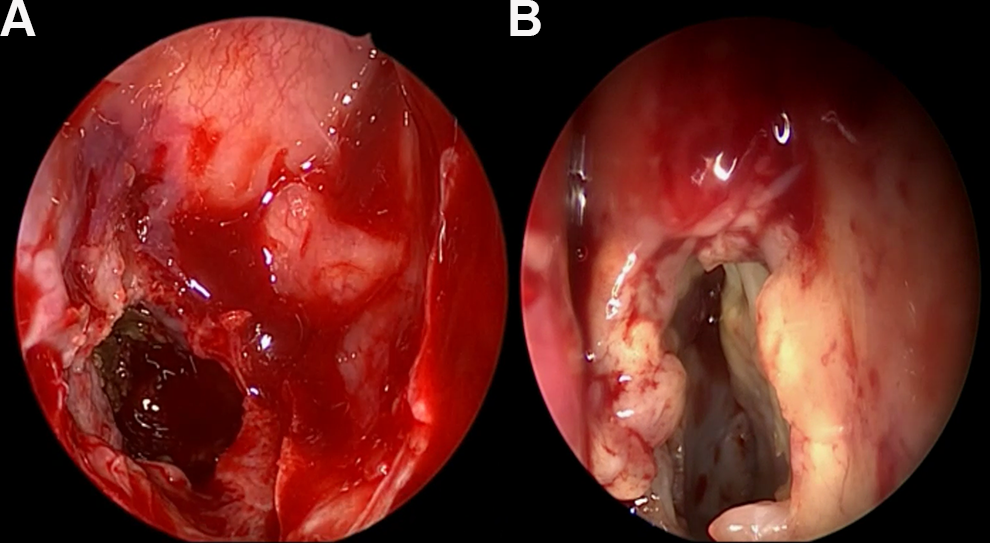
(A) Endoscopic findings of fungal balls filled up with right sphenoid sinus and (B) Mucosal thickening in sphenoid sinus.
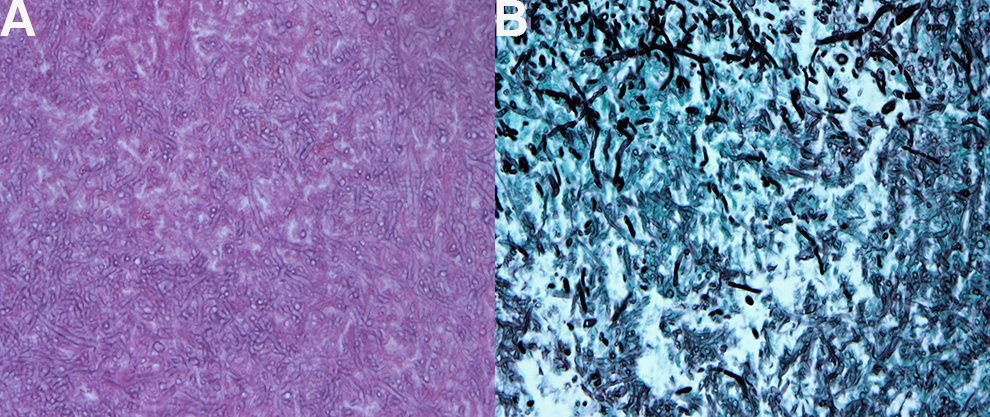
(A) Hematoxylin and eosin (H&E) stain, 400×; (B) Grocott-Gomori methenamine silver (GMS) stain, 400×. A narrow, septate hyphae with an acute angle of less than 45°, which can be thought of Aspergillus is observed.
Amphotericin B was administered as an intravenous infusion at 12.5 mg on the day of administration, 25 mg from the second day of administration, and 37.5 mg from the seventh day of administration to 2 months postoperatively. On the 20th postoperative day, ptosis was observed, but the range of motion and visual acuity was not recovered. Direct and indirect large light reflexes were observed, but visual acuity was not improved compared to before surgery, no additional visual acuity test was performed.
Discussion
Invasive fungal sinusitis is a rare condition that usually occurs in immunocompromised patients and often presents as an OAS. 5 Mucormycosis is the most common pathogens as a cause of invasive fungal sinusitis. A patient with rhino-orbito-cerebral Mucormycosis has been treated with extensive surgical and medical treatment to maximize outcomes. 6 In retrospective study with 50 patients with OAS, 42 cases were unilateral and 8 were bilateral. The most common initial symptoms were blurred vision, proptosis, periorbital pain, and headache in order. The most common etiology of the OAS was neoplasia, of which lymphoma was the most common, inflammation, infection, trauma, and others. 2
Our case of bilateral OAS case by sphenoid sinus Aspergillus has not been reported until now. The patient with diabetes mellitus was emergently treated with the diagnosis was chronic Aspergillus sinusitis and right-sided OAS. 7 Orbital apex syndrome caused by Aspergillus infection has been reported in patient during chemotherapy for metastatic colorectal cancer 8 and immune compromised patients with a long history of methylprednisolone. 9 In the review with OAS caused by Aspergillus species in 73 patients, 33 (45%) patients did not experience any improvement or continued to deteriorate, and 23 (32%) died in the course of their reported follow-up. 10
The possible pathogenic mechanisms of OAS due to herpes zoster ophthalmicus are direct cytopathic effect of the virus, immune-mediated tissue damage, and inflammatory edema causing compression and ischemia. Direct pressure by the fungal lesion of the inoculation appears to have caused visual impairment and paralysis of the eye muscles. 11
Infections can spread from sphenoid sinus to the orbital apex and invade to the cerebral cortex. Our case has also shown that Aspergillus infection has spread to the dura matter of the cribriform plate area. Orbital apex syndrome should be diagnosed and treated immediately. The majority of invasive rhino-orbito-cerebral infection are originated from Mucormycosis infection. Eleven cases of invasive rhino-orbito-cerebral Mucormycosis are presented with OAS initially. 12
Orbital apex syndrome is an uncommon manifestation of a wide range of disease entities, with management ranging from antibiotic therapy to immunosuppression and surgery. 5 Early empiric antifungal treatment and debridement can potentially reduce morbidity and mortality. 10 Since it is very difficult to predict the prognosis after treatment, and despite surgery and 6 weeks of antifungal treatment, it is often necessary to reoccurring with computerized tomography once every 3 to 4 months after treatment and endoscopy every 2 to 3 months to check whether there is a local recurrence or recurrence of eye or brain to adjacent organs. 13
Conclusion
This case is a very rare case of by Aspergillus sphenoid sinusitis which has extended to the skull base and septum, resulted in bilateral OAS in uncontrolled diabetic patient. We report with the literature.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Technology Innovation Program(#10063389) funded By the Ministry of Trade, Industry & Energy(MOTIE, Korea), This work was supported by the Korea Medical Device Development Fund grant funded by the Korea government (the Ministry of Science and ICT, the Ministry of Trade, Industry and Energy, the Ministry of Health & Welfare, the Ministry of Food and Drug Safety) (KMDF-PR-20200901-0147).