
Abstract
We sought to establish the effect of introducing a multidisciplinary tracheotomy management team (MDT). Tracheotomies are high-cost interventions with potentially devastating complications. Multidisciplinary teams have been introduced in many hospitals with the aim of reducing complications, however, data supporting them are lacking. There is currently insufficient evidence to conclude MDTs reduce length of hospital or intensive care unit (ICU) stay, and there is little information on cost analysis. A chart review identified patients who had a tracheotomy inserted at a major metropolitan teaching hospital with an acute spinal medicine service 2 years before and after the MDT was implemented. The primary outcome was time to decannulation. Other outcomes included tracheotomy complications, the proportion of patients decannulated, length of ICU and hospital stay, and admission cost. Our search identified 174 (78 prior and 96 post-MDT) patients. Baseline demographics were similar between groups. There was no difference in time to decannulation, the decannulation rate, or the length of hospital or ICU stay. Complication rates were low in both groups. There was an increase in the proportion of patients who received speaking valves and a reduction in cost of admission in a subgroup of patients who did not undergo head and neck surgery. There is insufficient evidence to support the widespread introduction of tracheotomy MDTs. Institutions considering introducing a tracheotomy team should carefully consider their case-mix, volume, and available resources as well as the structure and responsibilities of the team, and the timing of its activities within the working week. The potential benefits of MDTs including teaching of staff, and collaboration of teams should be acknowledged. Given the potentially significant implications for cost to the health system, a randomized trial is needed to guide policy in this area.
Introduction
Tracheostomies are high-cost interventions with potentially devastating complications and require specialist expertise to manage. Tracheotomy care was traditionally the responsibility of the surgical team that performed the procedure. However, with the advent of the percutaneous technique, the responsibility now often falls to the treating team which may have limited experience in tracheotomy management. Hence, multidisciplinary teams (MDTs) have been introduced in many hospitals with the hope of improving outcomes. 1 However, the data supporting MDTs are limited and it has been observed in other areas of health care that MDTs have failed to deliver expected benefits. 2
The available literature consists only of observational studies. There is low-quality evidence that MDTs reduce tracheotomy time and increase speaking valve use. 1 Reductions in hospital length of stay (LOS) and intensive care unit (ICU) LOS have been reported, though not consistently, and only a few studies have reported cost data. 3 -5
If found to be effective, and with more supporting data, tracheotomy teams might prove to be an effective safety measure with additional cost benefits that could be implemented on a large scale. We sought to establish the effect of introducing a unique MDT consisting of an ICU consultant, ENT registrar, speech pathologist, and clinical nurse consultants from ENT, ICU, and spinal medicine. The team reviewed all inpatients with a tracheotomy every Thursday.
Patients and Methods
A before–after observational study was performed at a major adult metropolitan teaching hospital with an acute spinal medicine service. Ethics approval was granted by the hospital’s research ethics committee.
A power calculation guided by a systematic review and meta-analysis by Speed et al (2013) was performed based on a mean time to decannulation of 33 days, standard deviation of 14 days, and an effect size of 8 days. To achieve a power of 80%, the required sample size was 52 patients in each group. A post hoc power calculation was also performed.
A medical record database search identified all patients who underwent tracheotomy in the 2 years before and after implementation of the tracheotomy MDT excluding a 3-month “run-in” period to exclude teething problems. The study period was July 2011 to October 2015. The primary outcome was time to decannulation (the total time the tracheotomy was in situ). Secondary outcomes included length of hospital stay (LOS), length of ICU stay (LOS-ICU), decannulation rate, tracheotomy-specific complications, speaking valve use, and cost of admission episode.
The cost of patient admissions was calculated using the Clinical Costing method and standards of the New South Wales Health Cost Data Collection. This is a bottom-up method where the cost per patient is built up from recorded utilization of services and their associated costs (eg, radiology and pathology actual charges, theater minutes used, prosthetics costs, drug costs, allied health minutes used, transport costs). Medical costs are usually first estimated for their relative inpatient versus outpatient uses and then allocated to the patient episode. Nursing costs are allocated on the bed days used by a patient. Costs are calculated in Australian Dollars and are inflation adjusted to 2017 Australian dollar values. The cost of implementing the tracheotomy team was not included in this analysis.
Post hoc subgroup analyses were performed on patients who did not undergo head and neck surgery (ie, those patients who would not otherwise have regular reviews by ICU or ENT physicians once transferred to the ward) as it was hypothesized that this is where the MDT might make the greatest difference.
Only patients who underwent tracheotomy at our center within the study period were included. Hence, patients who had preexisting tracheotomies or were transferred to our center with a tracheotomy in situ were excluded, as were laryngectomy patients. Decannulation rate was defined as the proportion of patients whose tracheotomies were decannulated within the same admission. Only patients whose tracheostomies were inserted with the intention to decannulate were included in this analysis.
Data are presented as median (interquartile range, IQR) unless otherwise stated. Analyses were performed using Stata 14.2 software. Where significant, P values were adjusted for multiple measures by Holm step-down Bonferroni procedure.
Results
Our search identified 176 patients who received tracheotomies. Two patients were excluded from the post-MDT group: one due to a medicolegal dispute that significantly affected their hospital stay, the other underwent an emergency tracheotomy but was immediately transferred to another hospital. The remaining 174 patients were included in the analysis (78 pre-MDT implementation, 96 post-MDT implementation).
Baseline demographics, indications for tracheotomy, urgency, and the proportion of percutaneous and surgical tracheotomies were similar between groups (Table 1). Results are presented in Table 2. There was no difference in time to decannulation between the pre-MDT and post-MDT groups; 16 (IQR: 10-39) versus 19 (IQR: 10-35) days (P = .41). A post hoc calculation showed a power of 85% to detect a median difference in time to decannulation of 8 days. All patients had their tracheotomies inserted with the intention to decannulate, and the decannulation rate was similar 79% versus 88% (P = .21). The length of hospital stay and the length of ICU stay were not significantly different. The cost of patient admission was also not significantly different.
Patient Characteristics.
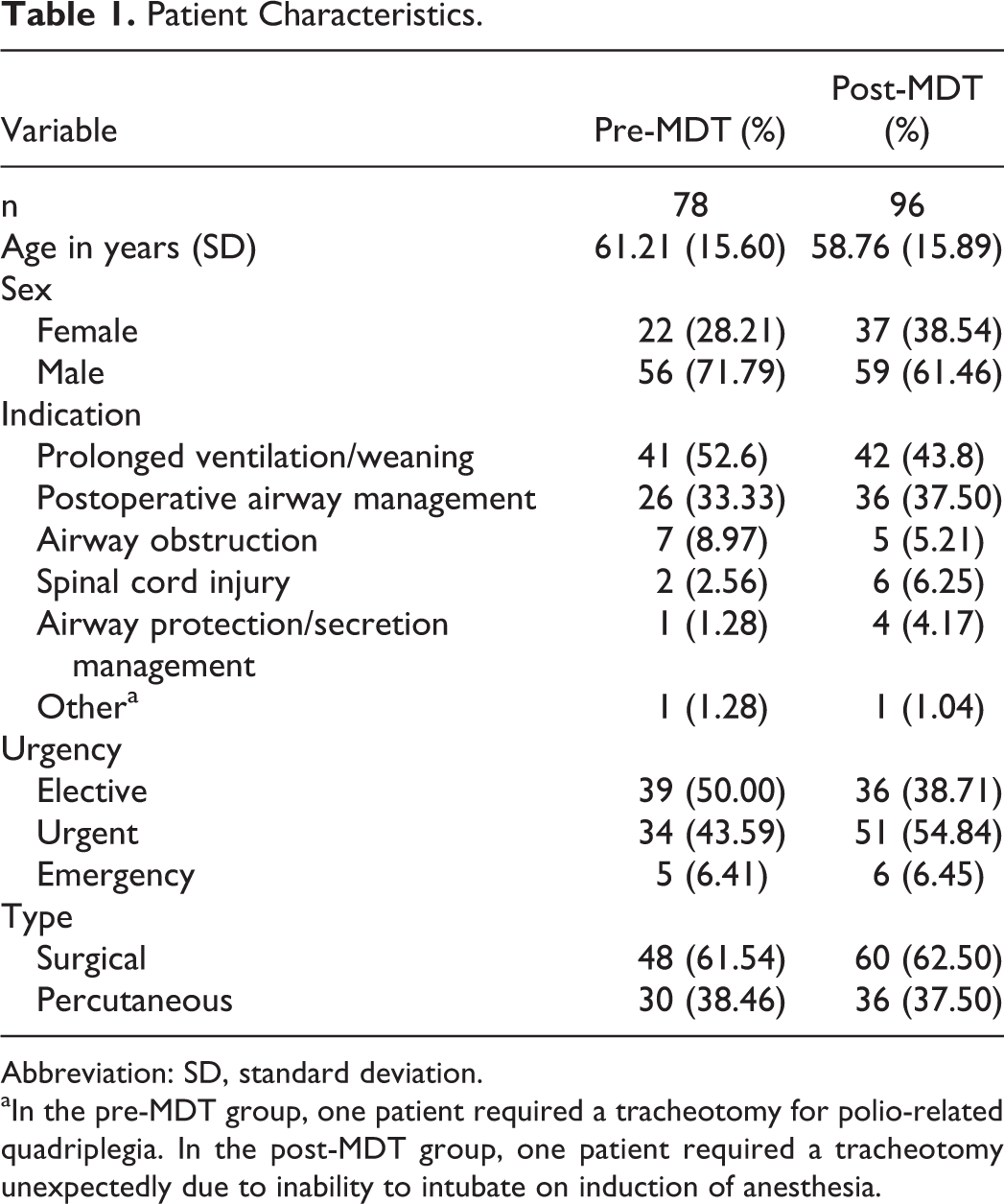
Abbreviation: SD, standard deviation.
aIn the pre-MDT group, one patient required a tracheotomy for polio-related quadriplegia. In the post-MDT group, one patient required a tracheotomy unexpectedly due to inability to intubate on induction of anesthesia.
Results.
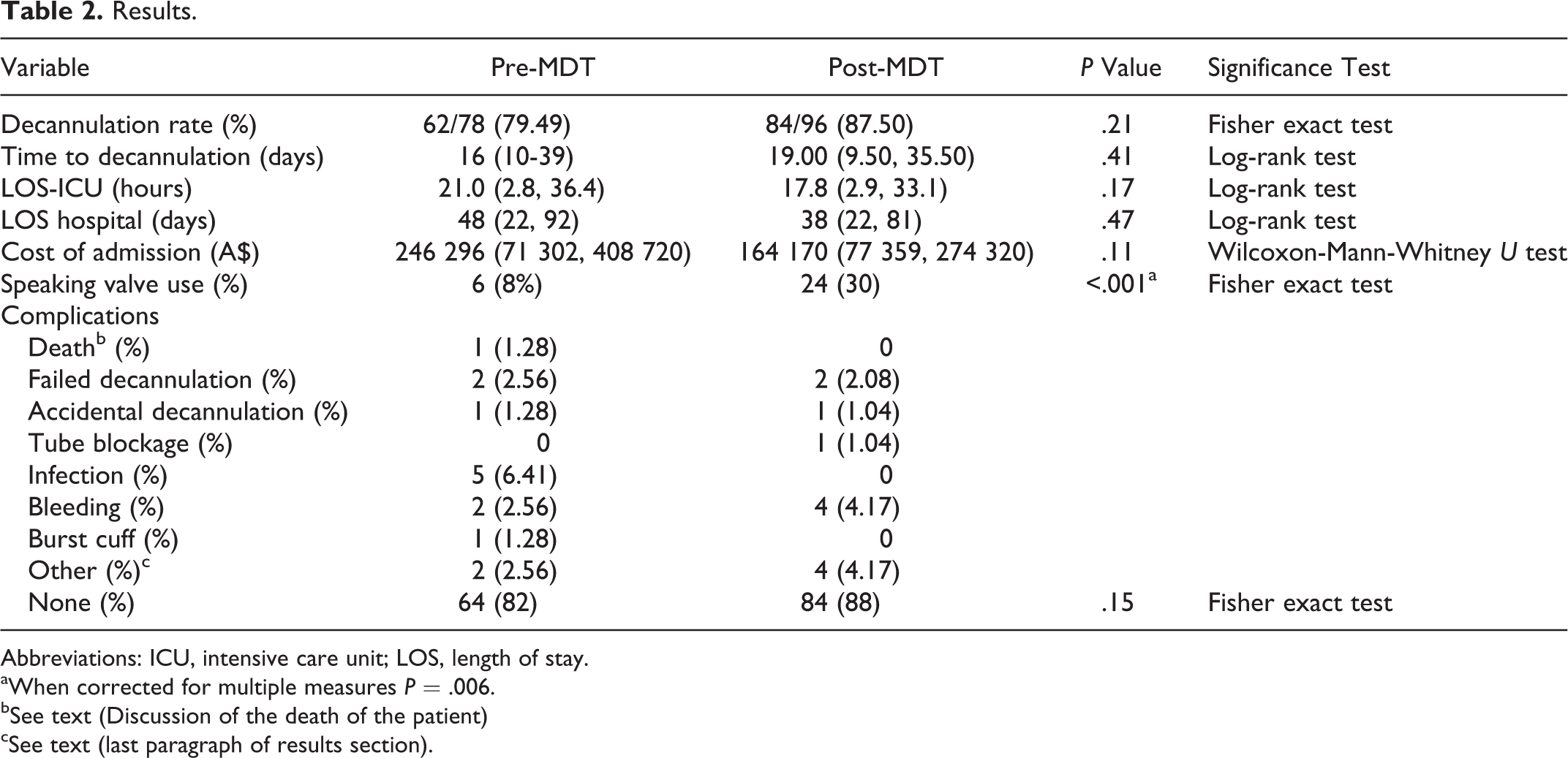
Abbreviations: ICU, intensive care unit; LOS, length of stay.
aWhen corrected for multiple measures P = .006.
bSee text (Discussion of the death of the patient)
cSee text (last paragraph of results section).
Complications were uncommon in both groups with no statistically significant difference between the groups (Table 2). There was one death in the pre-MDT group and none in the post-MDT group. There was 1 accidental decannulation, and 2 failed decannulations in both groups. There were no tube blockages in the pre-MDT group and 1 in the post-MDT group. The death in the pre-MDT group resulted from sudden catastrophic airway hemorrhage in a patient who had multiple prior tracheotomies for subglottic stenosis. A recent attempt at an emergency tracheotomy was abandoned due to grossly distorted anatomy. A tracheotomy was performed in the resuscitation attempt, but the bleeding was not possible to arrest despite prompt care and appropriate expertise.
Other complications included one patient in the pre-MDT group who required a redo-tracheotomy due to a take back to theater for positive margins and a compromised flap. Another patient had a minitracheotomy placed for pulmonary toileting but failed to improve so this was converted to a formal tracheotomy. In the post-MDT group, one patient’s tracheotomy tube was displaced into the pretracheal plane. He had no respiratory distress and was decannulated. One patient developed excessive granulation tissue and 2 patients had breakdown of their tracheotomy wound sites that were all treated conservatively.
Subgroup Analysis
In the subgroup of patients who did not undergo head and neck surgery, there were 52 patients in the Pre-MDT group and 60 in the post-MDT group. Demographics are presented in Table 3. The majority of patients were male in both groups though the proportion was higher in the pre-MDT group.
Demographic Data of Patients Not Undergoing Head and Neck Surgery.
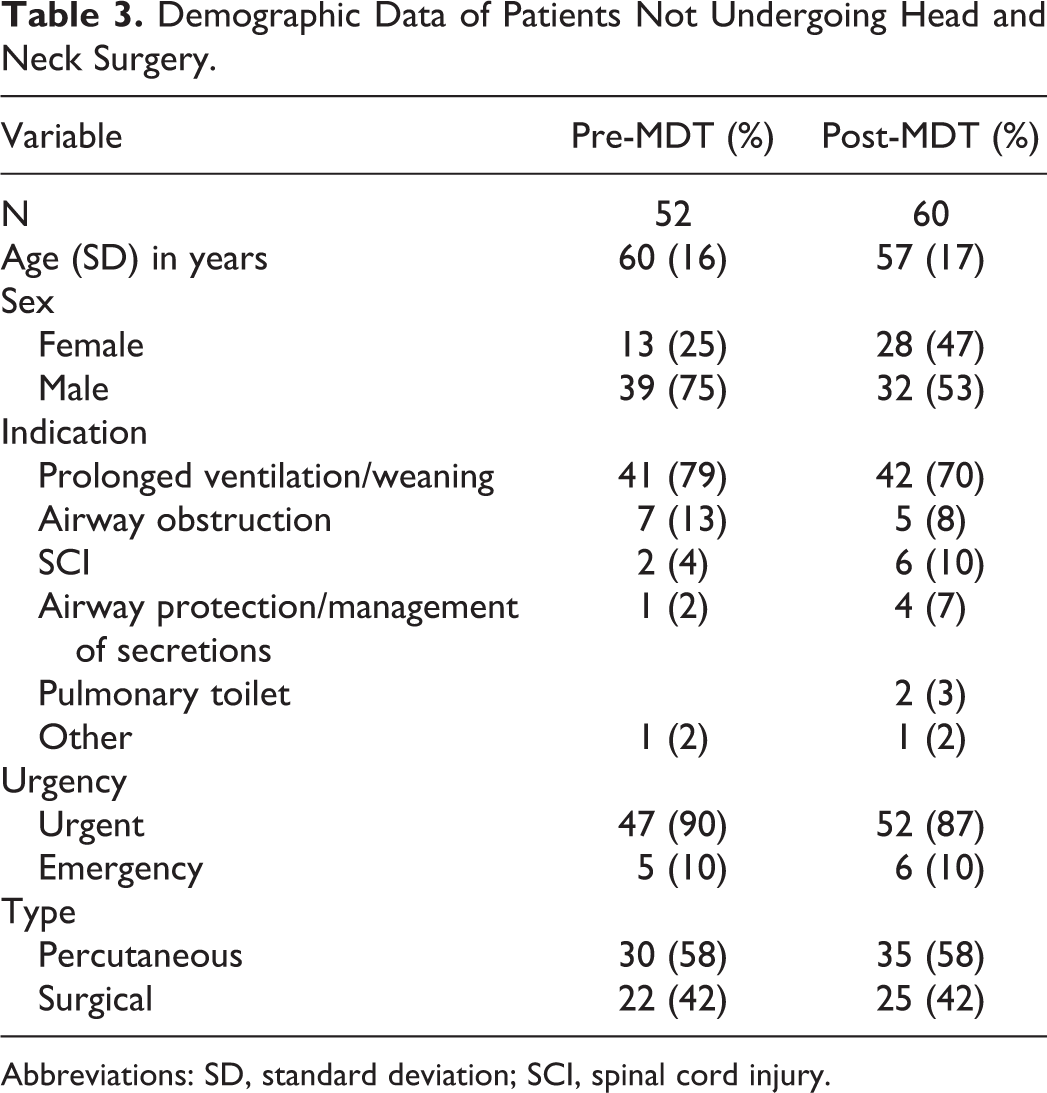
Abbreviations: SD, standard deviation; SCI, spinal cord injury.
There was a significant reduction in cost of admission associated with the introduction of the MDT in this subgroup: 328 377 (IQR: 231 152-535 687) versus 246 945 (IQR: 152 620-353 930) dollars (P = .004). When corrected for multiple measures, P value equals .04. No statistically significant difference was observed in the other variables (Table 4). Length of hospital and ICU stay were not significantly different. Complications were uncommon in both groups.
Results for Patients Not Undergoing Head and Neck Surgery.
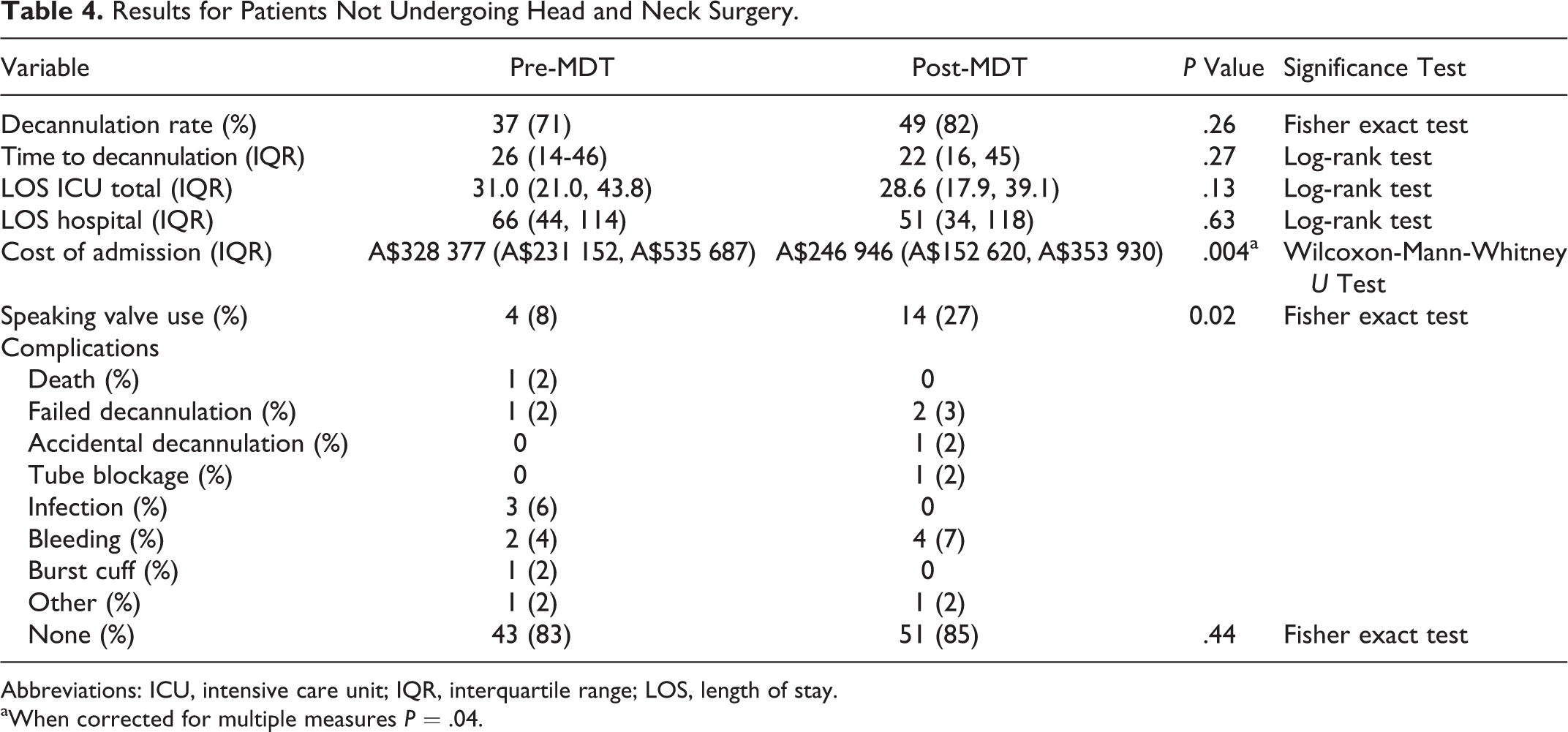
Abbreviations: ICU, intensive care unit; IQR, interquartile range; LOS, length of stay.
aWhen corrected for multiple measures P = .04.
Discussion
This study is the largest to date and was adequately powered. This contrasts with previous studies which are mostly underpowered and most have not shown a significant difference in outcomes. 1 Additionally, the study populations are heterogeneous; one includes only traumatic brain injury patients, 6 another one includes only spinal cord injury patients and excluded those patients who required permanent tracheotomy, and those who died of non-tracheotomy-related causes. 3
Time to Decannulation
It was hypothesized that an MDT would help form structured and consistent plan for the progression of tracheotomy care, which may result in a reduced time to decannulation. 7 However, this study, along with others, does not support this assumption. 5 In a systematic review, Speed and Harding reported a reduction in time to decannulation of 8 days associated with the introduction of MDTs however only 4 of 6 studies that reported on time to decannulation were meta-analysed. 3,6,8,9 Of the 2 studies that were excluded, because they did not report a measure of spread, one reported very similar results, 10 and the other reported a longer tracheotomy time in the post-MDT group. 11 Our study did not demonstrate a significant difference despite adequate power, though the median time to decannulation was longer in the post-MDT group.
This finding was unexpected as we had hypothesized that regular input from clinicians experienced in tracheotomy management would progress tracheotomy care more rapidly. The increase may relate to many factors, though may be partly accounted for by a tendency for treating teams to wait for the weekly review to address concerns, rather than seeking prompt consultation. Another possibly contributory factor is that the MDT rounds on a Thursday, and there may be reluctance (or policy against) implementation of significant changes such as decannulation prior to the weekend.
Length of Hospital Stay
A statistically significant reduction in the LOS has been observed in 2 studies, 3,6 and a trend was observed in another. 11 A meta-analysis of the available data from 3 of 4 studies that reported on LOS, suggested a trend toward a reduction in LOS but was not statistically significant. 1 Similarly, our study did not demonstrate a significant reduction in LOS.
Length of ICU Stay
A reduction in LOS-ICU was expected stemming from the expertise available to manage these patients on the ward, enabling earlier discharge from the unit. Trends have been identified in previous studies supporting this, but in keeping with 5 other studies that have reported on LOS-ICU, a statistically significant difference was not identified. 3 -5,8,12
Cost
Our data did not show a significant reduction in cost of admission among the whole cohort. However, there was a statistically significant reduction in the cost of admission for patients who did not undergo head and neck surgery, and this remained significant when adjusted for multiple measures. It was hypothesized this group was most likely to benefit from MDT input as they would otherwise have no regular input from clinicians experienced in tracheotomy management. It is difficult to account for the cost reduction in the absence of a significant reduction in LOS, or LOS-ICU, though the medians observed for both these variables were lower in the post-MDT group.
The few other studies that have reported on cost data have consistently observed cost reductions. Mirski et al calculated a net benefit of US$1 308 949 in their 2008 study of 253 patients, which strongly related to decreased length of ICU stay. 4 Likewise, Pandian et al estimated a cost saving of US$235 506 comparing 2004 data with that from 2008. Cameron et al studied 53 spinal cord injury patients and calculated a significant cost saving of A$1 240 933 over 3 years attributed mostly to a reduction in length of hospital stay. 3 Other authors have speculated that reductions in LOS will result in cost savings but did not include data. 8,11,12
Speaking Valve Use
There was increased use of speaking valves in the post-MDT group which remained significant when tested for multiple measures. This is in keeping with other studies and may improve quality of life, cough, and decrease secretions. 1
Complications
The reporting of specific outcomes and complications relevant to tracheotomy patients have been variable and were not reported in several studies. 3,12,13 We observed that complications were uncommon in both groups, and there was no significant difference shown in our study. This is comparable with what has been reported in some studies, 3,8,10 though others have observed significant decreases in adverse outcomes including deaths due to tube blockages and respiratory distress. 9,10
Limitations
This study is limited by its retrospective observational design. To date, all the data on this topic are observational, and most come from retrospective before–after trials, 3,6,9 -11 with 2 studies collecting some data prospectively. 8,12 Some have suggested that ethical concerns might prevent experimental trials on this subject. 14 However, there are now several retrospective studies which have shown no significant difference in most outcomes despite a very plausible hypothesis. The potential implications for cost to the health system are substantial; hence, a randomized trial is needed.
We did not assess the effect of the MDT on institutional factors such as teaching and staff satisfaction and on the patient’s experience and confidence, which have all been raised as potential benefits of MDTs. 15 With the exception of tracheotomy-specific complications, the other outcomes including LOS and decannulation rates are confounded by the comorbidities of our patient population including acute spinal injuries and multi-organ failure.
Conclusion
This study did not identify a statistically significant difference in patient-related outcomes following the introduction of a tracheotomy MDT. It did not find a reduction in the time to decannulation or length of hospital or ICU stay. There was no significant difference in tracheotomy-related complications. A cost saving was identified in a subgroup of patients who did not have head and neck surgery.
Based on these findings, the widespread adoption of tracheotomy MDTs cannot be given a strong recommendation. A randomized trial is needed to guide policy in this area. It remains important to acknowledge potential benefits of MDTs including teaching of staff and improved collaboration of specialist teams involved in the patient’s care. In institutions where implementation of a tracheotomy team is being considered, careful consideration of the structure and responsibilities of the team and timing of reviews within the working week are recommended.
Footnotes
Authors’ Note
The study was conducted at the Prince of Wales Hospital, Sydney, New South Wales, Australia.
Acknowledgments
The authors would like to thank the medical, nursing, and allied health staff who have served on the tracheotomy MDT for their contribution. The authors also acknowledge the assistance provided by the hospital finance department for providing cost data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.