
Abstract
The purpose of this study is to categorize anomalous tympanic facial nerve (FN) on high-resolution computed tomography (HRCT) and to determinate the significance of associated temporal bone anomalies and congenital syndromes without microtia in patients with hearing loss. A retrospective analysis of HRCT findings in 30 temporal bones in 18 patients with anomalous FN was performed. Abnormalities of the tympanic FN were categorized as follows: category 1: FN medially positioned, but above the oval window; category 2: FN in the oval window niche; and category 3: FN below the oval window. Potential associated findings that were assessed included stapes abnormalities, oval window atresia, and inner ear anomalies, as well as the presence of a known congenital syndrome with hearing loss. The most common type of anomalous tympanic FN was category 1 (67%, n = 20), following by group 2 (20%, n = 6) and group 3 (13%, n = 4). Stapes anomalies were detected in 77% of temporal bones (n = 23), oval window atresia was detected in 43% of temporal bones (n = 13), and inner ear anomalies were detected in 70% of temporal bones (n = 21). Anomalous tympanic facial nerves in temporal bone with conductive hearing loss were often (60%) not associated with oval window atresia. The combination of aberrant tympanic FN and inner ear anomalies was significantly (P = .038) associated with a known congenital syndrome (6 patients), including CHARGE syndrome, oculo-auriculo-vertebral spectrum, Pierre-Robin sequences, and Down syndrome. Therefore, an anomalous tympanic FN in conjunction with inner ear anomalies appears to be a biomarker for certain congenital syndromes with hearing loss in the absence of microtia.
Introduction
An anomalous tympanic facial nerve (FN) is a rare embryologic anomaly characterized by dehiscence and an abnormal course. 1 Formation of FN begins during the fourth week of gestation. At about the 6th week, the FN bends caudally and the tympanic segment then passes through a deep sulcus in the otic capsule during the 10th week. 1 The facial canal begins to ossify during the fourth and fifth months and the ossification is completed at the end of the first postnatal year. 1 The formation of the FN is intimately related to the development of the stapes, the annular ligament, the oval window, and the vestibular component of the otic capsule. Since the FN develops earlier than those structures, abnormal timing of the anterior migration of FN prevents the developing stapes from attaining the otic capsule, which results in stapes and oval window abnormalities. 1,2
There are a few reports that describe the abnormal developmental relationships between tympanic FN, stapes, and oval window on temporal bone computed tomography, 3 -9 although a standardized approach to evaluating such cases is lacking in the literature. Yet, it is important to be aware of the clinical and surgical implications of the anomalous tympanic FN. Thus, the purpose of this study was to characterize anomalous tympanic FN on temporal bone HRCT in patients with hearing loss and to assess the presence and significance of associated temporal bone anomalies, including any congenital syndromes without microtia.
Materials and Methods
Patient Population
Our institutional review board approved this study and waived the need for informed consent. The study complied with the Health Insurance Portability and Accountability Act. A database of 7487 HRCT temporal bone studies performed at our institution between January 1, 2007, and December 31, 2017, was searched for relevant cases. In particular, cases were identified based on the radiology reports containing the following keywords: abnormal FN, aberrant FN, dehiscent facial canal, FN malposition, oval window atresia/abnormality, or stapes malformation/impingement/fixation. Up to 27 patients with hearing loss were identified, but 8 patients with associated microtia and 1 patient with previous surgery were excluded, leaving a total of 18 patients. Hospital electronic medical records were reviewed in order to obtain the following information: age, gender, audiological studies including tympanometry, pure tone audiometry, free field audiometry and otoacoustic emission, and clinical diagnosis. The type of hearing loss was classified as conductive hearing loss (CHL), sensorineural hearing loss (SNHL), and mixed hearing loss (MHL) according to the results of audiological studies and clinical evaluations.
Image Acquisition
All temporal bone HRCTs were obtained in axial planes in 0.6-mm slice thickness with 0.55 pitch, 512 x 512 matrix, 200-mm field of view, 120 kVp, and 250 mAs parallel to the hard palate, corresponding to an angulation to the canthomeatal baseline and providing optimal visualization of the stapes superstructure and oval window. Subsequently, the images were reconstructed with a 0.6-mm slice thickness by using a small field of view (8-10 cm diameter) centered on the cochlear promontory and processed with a bone or sharp imaging algorithm, as well as 0.3-mm reformatted images in the coronal plane.
Image Interpretation
High-resolution computed tomography studies of temporal bone were reviewed on a picture archiving and communication workstation (IntelliSpace PACS Enterprise; Philips, Amsterdam, The Netherlands). A neuroradiology fellow reviewed the axial and coronal images in consensus with an attending neuroradiologist with certificate of added qualification and over 5 years of experience in the head and neck imaging.
Malpositioning of the tympanic FN was categorized as follows (Figure 1):
Category 1: Aberrant FN positioned above the oval window. Category 2: Aberrant FN in the oval window niche. Category 3: Aberrant FN below the oval window niche.
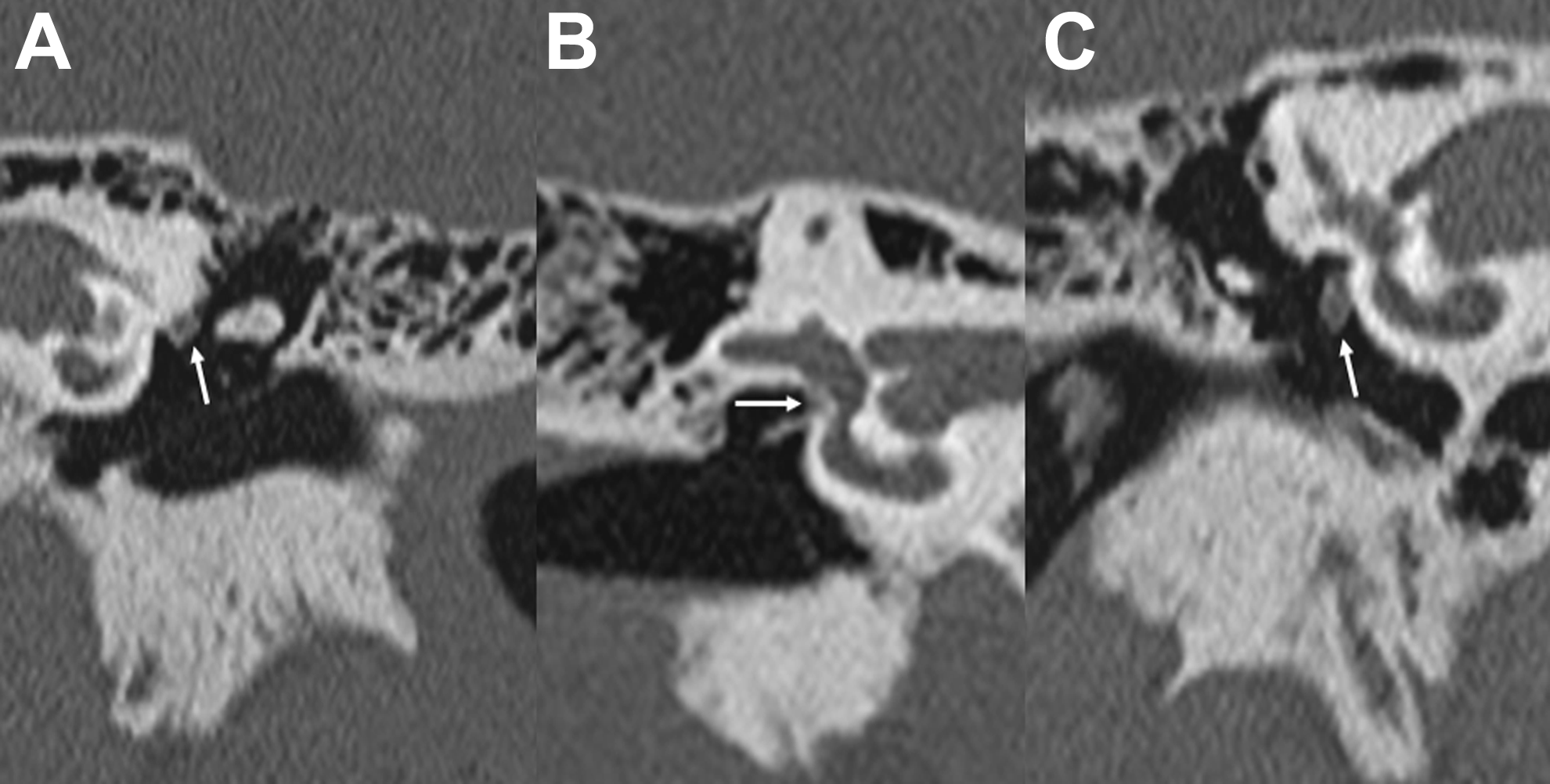
The categories of aberrant FN (arrows) is demonstrated on the picture, with category 1, superior to the oval window; category 2, FN in the oval window niche; category 3, FN below oval window niche. FN indicates facial nerve.
Potential associated temporal bone findings were categorized as follows (Figure 2):
Stapes anomalies, including abnormal position or morphology, such as deficiency or deformity of any part of the ossicle. Oval window atresia defined as the absence of the structure with the presence of a bony plate superimposed between the vestibule and middle ear.
10
Inner ear anomalies, including malformed cochlea such as abnormal shape, abnormal modiolus, abnormal interscalar septum, stenotic fossette, malformed vestibule, enlarged vestibular aqueduct, absence or malformed semicircular canals, and abnormal internal auditory canal.
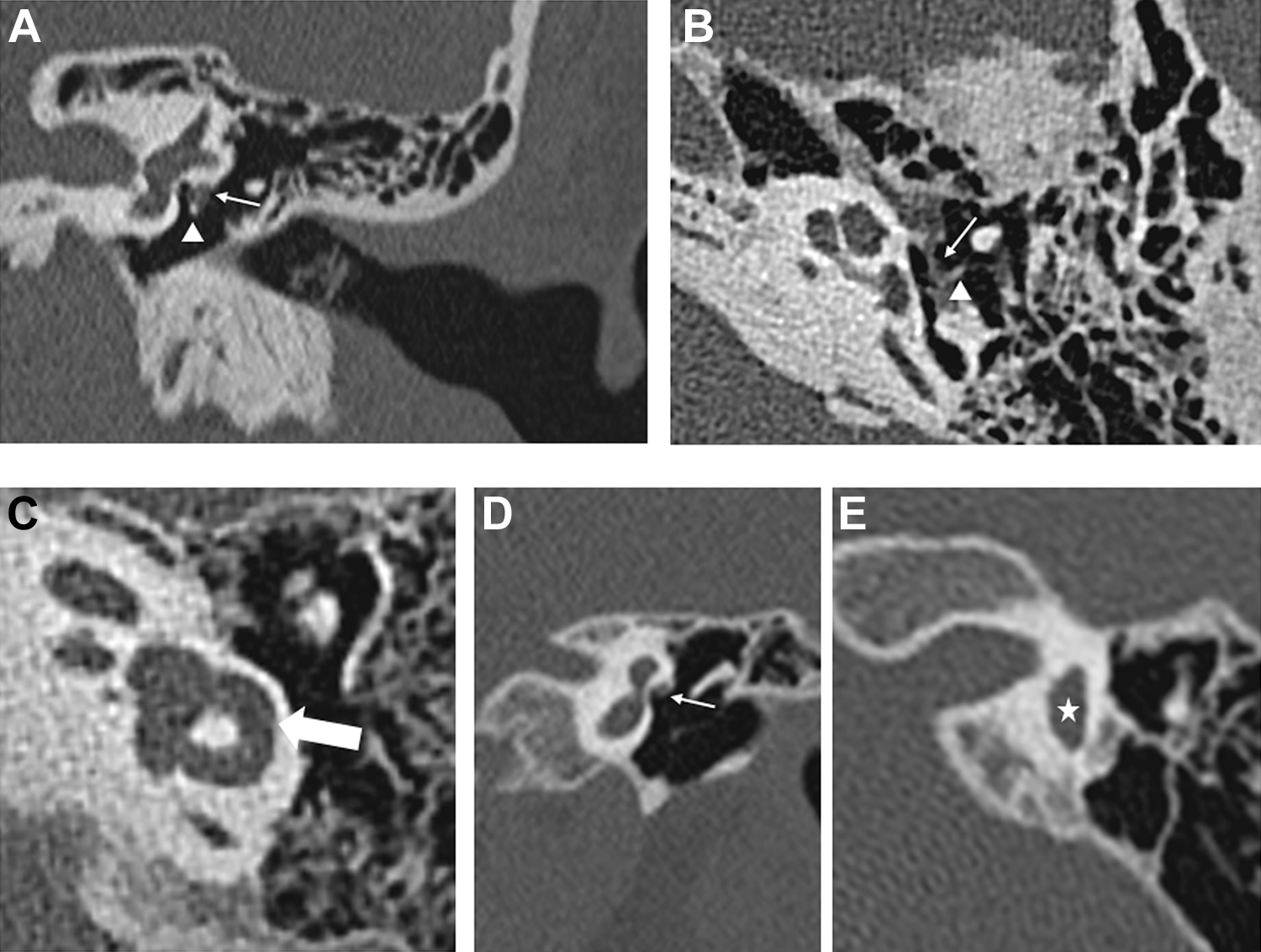
Case 1 with a history of bilateral CHL: left temporal bone HRCT (A, coronal plane and B, axial plane) demonstrates category 1 FN (arrow) associated with stapes impingement (arrowhead) and oval window atresia. Case 8 with CHARGE syndrome: left axial temporal bone HRCT (C) demonstrates an enlarged lateral semicircular canal (thick arrow). There are also numerous inner ear malformations including dysplastic vestibule, enlarged vestibular aqueducts, deficiency of modiolus and cochlear turn, severely narrowed internal acoustic canal, and oval window atresia associated with aberrant FN in this case (not shown). Case 9 with CHARGE syndrome: left temporal bone HRCT (D, coronal plane and E, axial plane) demonstrates category 1 anomalous FN (arrow) and dysplastic vestibule (star) as one of the examples of multiple inner ear abnormalities (not shown). CHL indicates conductive hearing loss; FN, facial nerve; HRCT, high-resolution computed tomography.
Statistics
All statistical analyses were performed by using Stata version 15 (StataCorp, College Station, Texas). Categorical variables were analyzed by χ2 test or 2-tailed Fisher exact test to determine the statistical significance of associations between abnormal FN and other variables of interest. A P value of less than .05 was considered statistically significant.
Results
A total of 18 patients were identified (12 females and 6 males; mean age: 10.3 years; range: 9 months to 59 years) with 30 temporal bones that demonstrated anomalous tympanic FN, in which 80% (n = 24) were bilateral and 20% (n =6) of which were unilateral. Among the 30 anomalous tympanic FN, 67% (n = 20) were classified as category 1, 20% (n = 6) as category 2, and 13% (n = 4) as category 3. There were 10 temporal bones with CHL, 14 temporal bones with SNHL, and 7 temporal bones with MHL. The results are further summarized in Table 1 and in the following text.
Summary of Clinical Data and Imaging Findings.
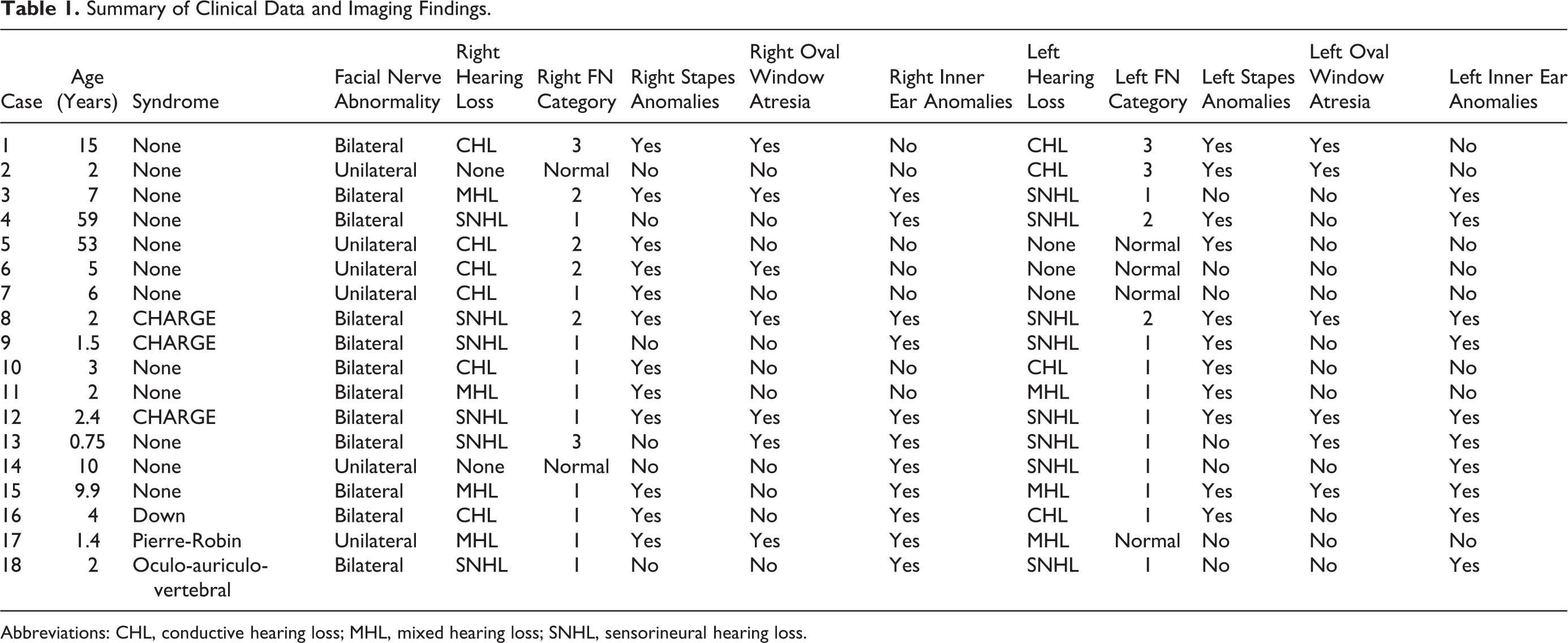
Abbreviations: CHL, conductive hearing loss; MHL, mixed hearing loss; SNHL, sensorineural hearing loss.
Stapes anomalies were detected in 77% of temporal bones (n = 23), oval window atresia was detected in 43% of temporal bones (n = 13), and inner ear anomalies were detected in 70% of temporal bones (n = 21). Among 7 patients with CHL, 3 had bilateral involvement, including 5 with FN in category 1, 2 in category 2, and 3 in category 3. All were associated with stapes anomalies, while inner ear anomalies were not apparent in any of them except for 1 patient diagnosed with Down syndrome, in which the inner ear anomalies were mild and did not result in SNHL. Among the 10 temporal bones with CHL, 6 (60%) did not have associated oval window atresia.
There were 6 (33%) patients with known congenital syndromes, including 1 diagnosed with Down syndrome, 1 diagnosed Pierre-Robin sequence, 3 diagnosed with CHARGE syndrome, and 1 diagnosed with oculo-auriculo-vertebral syndrome. There was a statistically significant association between the combination of abnormal FN, inner ear abnormalities, and underlying congenital syndromes (P = .038). However, this combination was only present in 28% (n = 5) of cases without a known congenital syndrome. Otherwise, there was no statistically significant correlation between the categories of anomalous FN and the presence of inner ear abnormalities. Furthermore, the presence of bilateral as opposed to unilateral aberrant FN involvement did not significantly predict the presence of other temporal bone abnormalities.
Discussion
The status of the FN should be routinely assessed on temporal bone HRCT performed for hearing loss. Although a quantitative approach toward characterizing the FN location on HRCT with respect to various landmarks has been described, including the cochlear promontory, oval window, round window, and mastoid antrum, 10 this approach can be cumbersome. Rather, we propose that a qualitative categorization approach to delineating the anomalous FN with respect to the oval window, such as the one introduced in this study, may be more practical for conveying the salient findings in routine practice than implementing various measurements in order to define the localization of FN.
As demonstrated in this study, CHL can be associated with any category of anomalous tympanic FN when there is an accompanying stapes abnormality, such as fixation to the nerve or deficiency of the ossicles, and oval window atresia, and not just when the FN obliterates the oval window niche. Since category 1 and 3 anomalous FN with stapes fixation do not appear to be associated with oval window atresia, such cases may be amenable to ossicular reconstruction. 11 The presence of some form of FN anomaly has been reported in up to 8% of stapedectomy procedures and requires special management. 12 Given the variability of anomalous tympanic FN demonstrated in this study, it is important to obtain HRCT of the temporal bone prior to middle ear surgery and to effectively communicate the type of FN anomaly to the otologist in order to avoid iatrogenic FN injury. 13 Although not encountered in this series of patients, FN duplication is another rare anomaly that can be a hazard for middle ear surgery. 14
The presence of the FN in the oval window niche confers a particularly increased risk of FN injury during middle ear surgery and can be a contraindication to stapes reconstruction. 9,15 Nevertheless, categories 1 and 3 of anomalous FN are also of clinical relevance, since those cases are associated with other anomalies that can lead to hearing loss and can be associated with an increased risk of injury during middle ear surgery. Indeed, even isolated FN dehiscence in an orthotopic location is prone to iatrogenic injury. 16,17 Furthermore, it is important to be aware that there can be an anomalous FN in patients with SNHL due to the presence of associated inner ear malformations and that this can pose a hazard during cochlear implantation. 18 Therefore, HRCT of the temporal bone should also be considered in the preoperative evaluation of patients with SNHL loss.
Microtia and external auditory canal atresia are classic external markers of second branchial arch derivative malformations, including an abnormal course of the FN, as part of various syndromes. 5,19,20 . However, an anomalous tympanic FN can be a manifestation of several congenital syndromes with temporal bone malformations without appreciable microtia. 21 For example, anomalous FN has been reported in 29% to 88% of patients with CHARGE syndrome, along with other temporal bone anomalies, such as dysplastic cochlea and vestibule, absent semicircular canals, ossicular anomalies, and small internal auditory canals. 22 Yet, up to 20% of patients with CHARGE syndrome do not have noticeable microtia. 21 Likewise, similar circumstances can be encountered in patients with Pierre-Robin sequence, oculo-auriculo-vertebral sequence, and Down syndrome. 23 -26
This study has certain limitations. For example, the database search may not have identified all relevant cases if the findings of interest were not mentioned in the radiology reports. In addition, there was no histopathological or surgical correlation of the imaging findings, which may underestimate subtle abnormalities.
Conclusion
High-resolution computed tomography reveals that anomalous tympanic FNs are associated with CHL even without oval window atresia. Furthermore, an anomalous tympanic FN in conjunction with inner ear anomalies appears to be a biomarker for certain congenital temporal bone syndromes with hearing loss in the absence of external auditory canal atresia. Therefore, HRCT of the temporal bone should be considered in the evaluation of hearing loss particularly before surgery in order to avoid from potential iatrogenic FN injury and to diagnose inner and middle ear abnormalities in the presence of normal external auditory canal or pinna.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.