
Abstract
The goal of this study was to determine whether high-resolution magnetic resonance imaging (MRI) microscopy coil imaging can improve the depiction parotid masses. A total of 14 parotid masses, including 7 salivary neoplasms, 2 abnormal lymph nodes, and 5 benign cystic lesions were imaged with T2-weighted and fat-suppressed postcontrast T1-weighted sequences using a 47-mm diameter microscopy coil in addition to conventional MRI sequences acquired with a conventional head and neck neurovascular coil. Compared to conventional parotid MRI sequences, microscopy coil images provided better definition of the margins of neoplasms, provide more detailed definition of lymph node morphology, and better depict certain cyst contents in the superficial portions of the parotid gland. The microscopy coil images provided significantly better definition of lesions and surrounding tissues within the superficial parotid gland with resptect to the deep parotid gland structures due to loss of signal. Furthermore, the fat-suppressed postcontrast T1-weighted microscopy coil images were significantly better than the corresponding T2-weighted images for delineating the superficial parotid gland. Ultimately, the microscopy coil sequences added over 10 minutes to the examination time.
Introduction
Magnetic resonance (MR) microscopy imaging consists of using small surface coils that are less than 100 mm in diameter in order to acquire images with higher spatial resolution than what is achieved through the use of usual coils. 1 Through the use of microscopy coils, T1- and T2-weighted sequences can be implemented to yield detailed imaging of various head and neck structures. For example, microscopy coil magnetic resonance imaging (MRI) can accurately delineate the deep margins of skin tumors for surgical planning, facilitate diagnosis and preoperative planning of orbital lesions, and can help differentiate between benign and malignant lymph nodes. 1 -3 Furthermore, MR microscopy imaging can help differentiate the parotid glands in patients with xerostomia who have Sjogren syndrome from those without the syndrome, can help assess radiation-induced effects on the internal architecture of the parotid gland, and to better delineate the intraparotid facial nerve and its branches via 3-dimensional-reverse fast imaging with steady state precession diffusion-weighted imaging. 4 -7
Preoperative MRI plays an important role in the differential diagnosis and surgical planning of parotid tumors. The goal of this study was to explore the potential utility and limitations of high-resolution MRI microscopy coil imaging for the initial evaluation of parotid tumors.
Methods and Materials
This study was conducted under an approved institutional review board (IRB) protocol. Patients with parotid tumors underwent a parotid protocol MRI using a 3 T MRI (Ingenia dStream; Philips Healthcare, Best, The Netherlands) and head and neck neurovascular coil, which included axial fat-suppressed T2-weighted (TR: 3839, TE: 80, NEX: 2) and postcontrast fat-suppressed T1-weighted (TR: 684, TE: 10, NEX: 2) sequences with the following parameters: 3-mm slice thickness with 1-mm gap, matrix size: 256 × 256 to 312 × 312, field of view (FOV): 18 to 20 cm. Magnetic resonance microscopy was performed using a 47-mm inner diameter microscopy coil (Philips Healthcare). The coil was positioned over the parotid gland with a palpable lesion. Axial fat-suppressed T2-weighted (TR: 4946, TE: 90, NEX: 1) and fat-suppressed postcontrast T1-weighted (TR: 700, TE: 10, NEX: 1) images were acquired using the following parameters: 1.5-mm section thickness with no gap, matrix size: 200 × 200 to 240 × 240, FOV: 4 to 6 cm. The in-plane resolution in terms of pixel size is calculated as FOV/matrix size. The acquisition time for each sequence was approximately 4 minutes. The lesions included in this study subsequently underwent fine needle aspiration (FNA) or surgical resection. The microscopy coil images were semiquantitatively compared to the conventional MR images by 2 board-certified radiologists with certificate of added qualification in neuroradiology. In particular, the overall detail, including the conspicuity the internal contents, tumor margins, and surrounding structures on both T2-weighted and postcontrast T1-weighted sequences for the microscopy versus conventional coils, was rated as follows: 1-much worse/not visible, 2-slightly worse, 3-about the same, 4-slightly better, 5-much better. This was carried out for both the superficial and deep portions of the parotid glands. The scores of the 2 reviewers were averaged together and differences between the scores among the different sequences and superficial versus deep portions of the parotids gland were evaluated using 2-tailed paired t test. A P value of less than .05 was considered statistically significant.
Results
Among a total of 14 patients with parotid gland tumors and available MRI examinations that included MR microscopy coil images, there were 7 salivary neoplasms (3 pleomorphic adenomas, 2 basaloid neoplasms, 1 oncocytoma, and 1 adenoid cystic carcinoma), 1 mucosa-associated lymphoid tissue (MALT) lymphoma with intraparotid lymphadenopathy, 1 benign lymph node, and 5 benign cysts.
The average image detail score in the superficial portions of the parotid glands for the fat-suppressed postcontrast T1-weighted and the T2-weighted microscopy coil images was 4.2 and 3.8, respectively, with a statistically significant difference between the 2 sequences (P value = .04). On the other hand, the average image detail score in the deep portions of the parotid glands for the fat-suppressed postcontrast T1-weighted and the T2-weighted microscopy coil images was 2.2 and 2.1, respectively, which were both significantly lower than the corresponding scores for the superficial portion of the parotid gland (P values <.001) due to considerably reduced signal-to-noise.
The microscopy coil images provided approximately 2.5 to 3.5 times greater in-plane resolution than the corresponding conventional images. Notably, the fat-suppressed postcontrast T1-weighted MR microscopy images better depicted the subtle ill-defined margins of an adenoid cystic carcinoma that arose at the site of what was reported to have been a benign parotid tumor resected over 20 years earlier, thereby raising the possibility of malignancy rather than a recurrent benign tumor (Figure 1). Similarly, the MR microscopy images adequately depicted the bosselated contours associated with a small superficial parotid pleomorphic adenoma, which were otherwise not evident on the conventional images (Figure 2). In addition, the MR microscopy images more clearly defined the smooth contours and nodal morphology associated with MALT lymphoma (Figure 3). However, the conventional images depicted additional cervical lymphadenopathy beyond the FOV of the microscopy images. Based on the combination of these findings, a lymphoproliferative disorder rather than a clinically suspected salivary neoplasm was suggested prospectively in the MRI report. Finally, the microscopy coil images were useful for defining the walls and internal contents of superficial benign cysts (Figure 4).
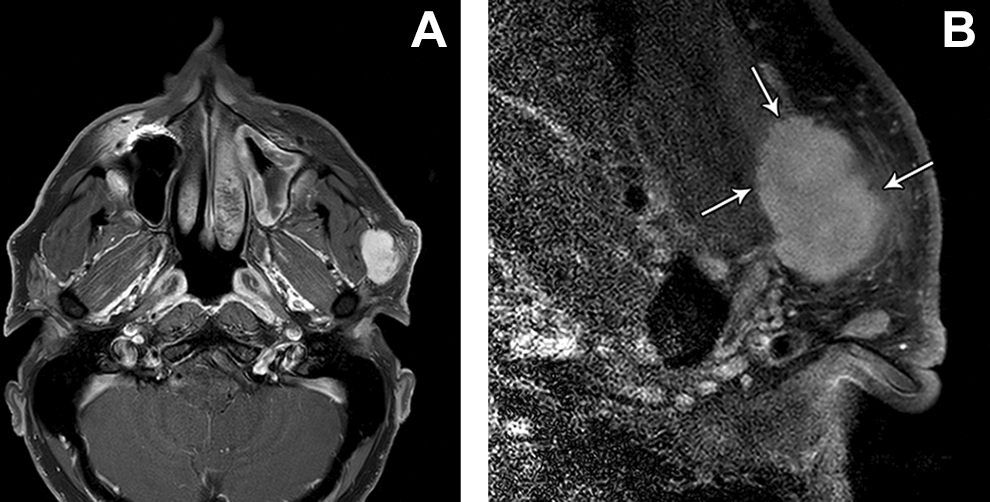
Axial fat-suppressed postcontrast T1-weighted conventional MRI (A) shows an enhancing left parotid space mass in a patient with a remote history of benign left parotid tumor resection. The corresponding axial fat-suppressed postcontrast T1-weighted microscopy coil MRI (B) reveals subtle infiltrative margins suggestive of a malignant neoplasm to a better advantage (arrows). The tumor proved to be an adenoid cystic carcinoma. MRI indicates magnetic resonance imaging.
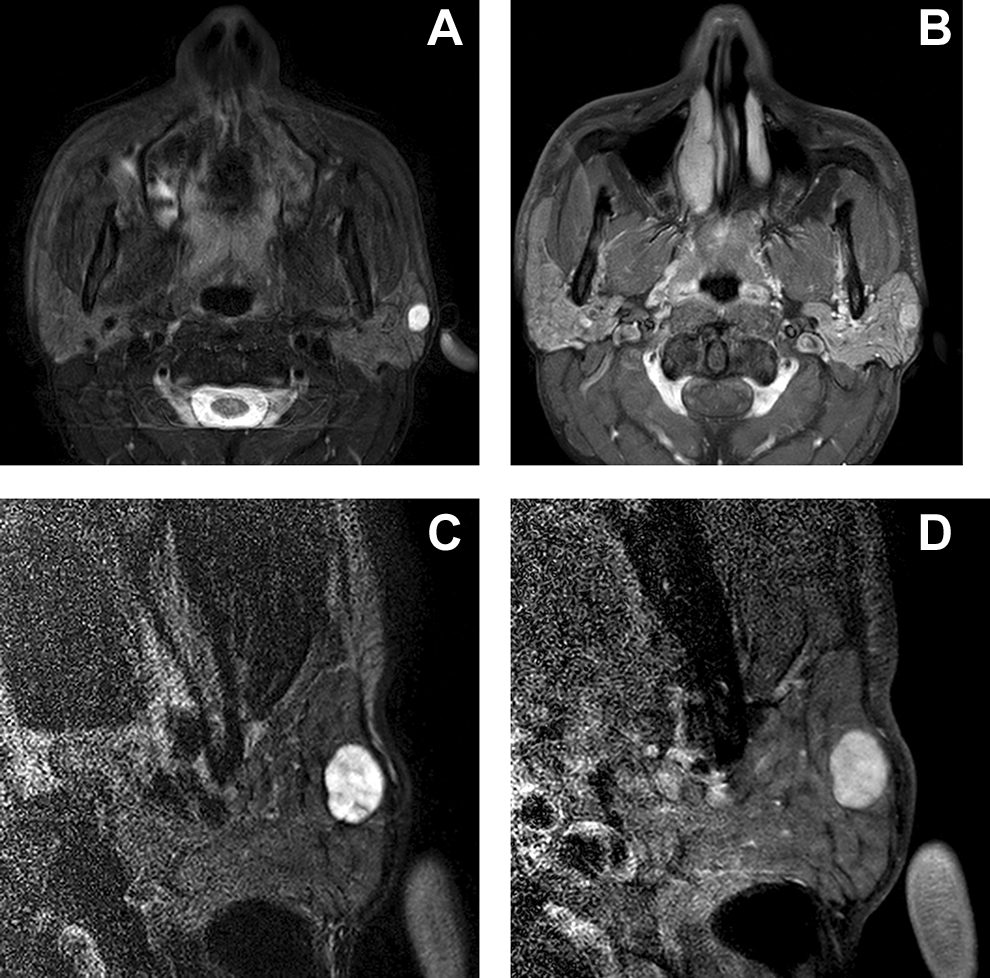
Axial T2-weighted (A) and fat-suppressed postcontrast T1-weighted conventional MRI (B) show a small enhancing nodule in the superficial left parotid gland. The corresponding axial T2-weighted (C) and fat-suppressed postcontrast T1-weighted microscopy coil MRI (D) better depict the mildly bosselated contours of the tumor, which proved to be a pleomorphic adenoma. MRI indicates magnetic resonance imaging.
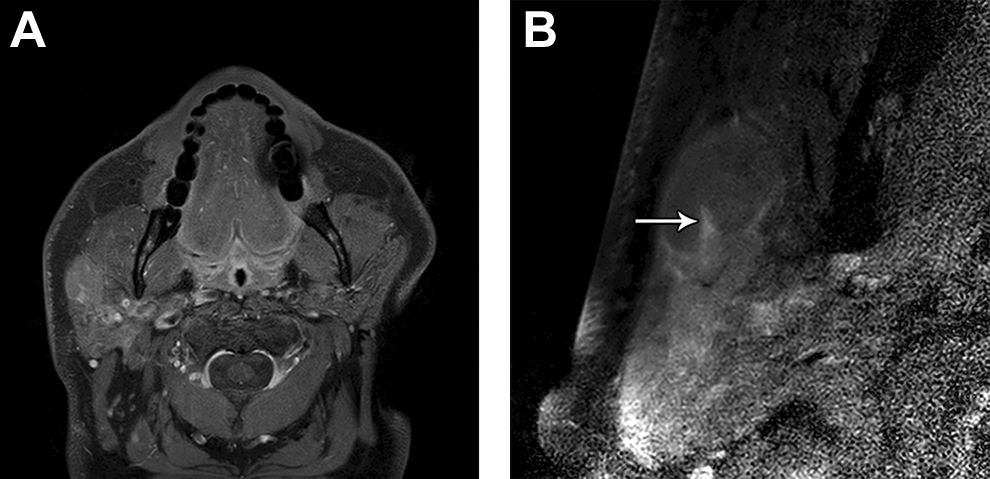
Axial fat-suppressed postcontrast T1-weighted conventional MRI (A) shows a homogeneously enhancing nodule in the superficial right parotid gland. The corresponding axial fat-suppressed postcontrast T1-weighted microscopy coil MRI (B) better depicts the lymph node contours and morphology with a narrow hilum (arrow). The lesion subsequently proved to be MALT lymphoma. MRI indicates magnetic resonance imaging.
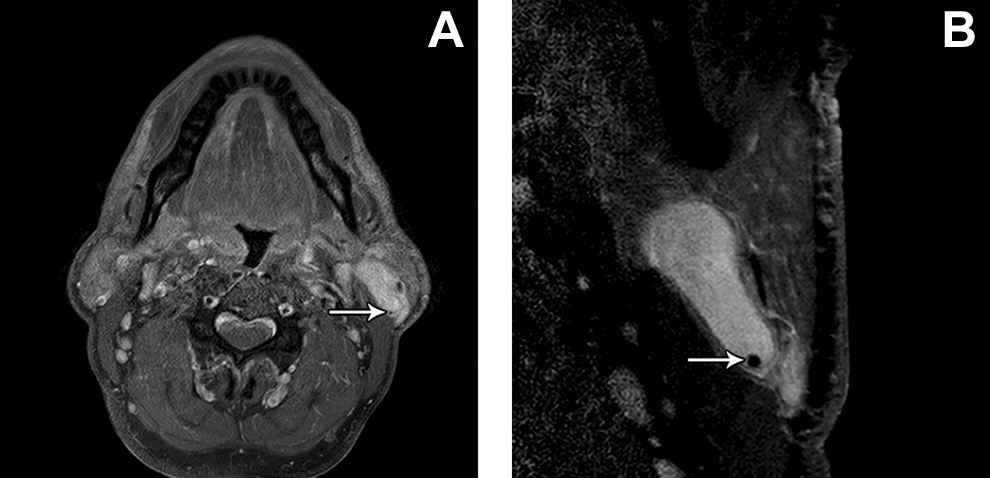
Axial fat-suppressed postcontrast T1-weighted MRI (A) shows an intrinsically hyperintense cystic lesion with a punctate hypointense focus (arrow) dependently in the left parotid gland. The corresponding axial fat-suppressed postcontrast T1-weighted microscopy coil MRI (B) better defines the contours of the cyst and the hypointense nodule (arrow), suggestive of a calculus. Aspiration of the cyst revealed needle-shaped crystals, which have been reported in non-neoplastic disease, such as sialadenitis. MRI indicates magnetic resonance imaging.
Each of the 2 microscopy coil sequences lasted up to approximately 4 minutes. Furthermore, at least 2 minutes would be spent by technologists to remove the head and neck neurovascular coil, apply the microscopy coil, and run a new survey scan. Thus, the dedicated parotid gland microscopy coil images added over 10 minutes to the MRI examination time. Furthermore, the pressure applied by affixing the microscopy coil to the face can distort the underlying anatomy and thereby limit the comparison of images obtained using the 2 different types of coils.
Discussion
This preliminary study of microscopy coil imaging as a supplement to a conventional MRI parotid protocol for the assessment of parotid gland masses highlights some of the strengths and weaknesses of the technique. The main advantage of high-resolution MR microscopy coil imaging is the improved delineation of tumor margins. This is relevant to the management of parotid tumors since ill-defined margins are highly suggestive of malignancy, 8 as exemplified by the case of adenoid cystic carcinoma in this series. Similarly, discerning the presence of bosselated margins on microscopy coil imaging can aid in the differential diagnosis of parotid tumors since this finding is rather suggestive of pleomorphic adenoma, as shown in this series. Furthermore, the presence of irregular borders increases the likelihood of positive margins and tumor recurrence even with pleomorphic adenomas. 9
In general, the internal architecture of the lymph nodes are not depicted in sufficient detail on conventional MRI sequences, such that the lymph node signal characteristics do not significantly improve the diagnostic ability of the size criteria for metastatic nodes. 2 On the other hand, the depiction of lymph node architecture on MR microscopy coil imaging may provide useful information in distinguishing benign from malignant lymph nodes in the neck. 2 For example, lymphomas may be associated with a narrow hilum, diffuse homogeneous enhancement, and smooth contours, as demonstrated in this series.
Cystic lesions of the parotid gland can be divided into the following categories: non-neoplastic cysts, benign tumors with macrocystic change, and malignant tumors with macrocystic change. It is important to distinguish these types of lesions from one another since management differs. 10 In terms of radiologic differential diagnosis, cystic lesions with well-defined margins and no solid components on MRI are likely non-neoplastic cysts. 11 Although neoplasms with extensive cystic degeneration have been reported on MRI, these nevertheless typically contain small mural nodules. 10 Thus, high-resolution MR microscopy imaging can potentially be more sensitive for identifying these nodules than via the conventional sequences. Furthermore, the higher in-plane resolution provided by microscopy coil imaging can aid in characterizing the internal contents of a cyst, such as the presence of calculi, which are suggestive of a benign entity, as exemplified in this series.
The main disadvantage of MR microscopy coil imaging is that it prolongs the examination time and at least in some cases lengthens the image interpretation time. In order to mitigate the scan time prolongation, perhaps only including the postcontrast T1-weighted microscopy coil sequence in the scan protocol is sufficient since this sequence was found to be significantly better than the corresponding T2-weighted images for the superficial parotid gland. Otherwise, it is not advisable to substitute the microscopy coil images for the conventional sequences since the larger FOV is useful for identifying other related abnormalities, such as lymphadenopathy in the rest of the neck. In addition, the small FOV and image quality degradation due to relatively lower signal-to-noise undermine the advantages of the microscopy coil for imaging lesions in the deep parotid gland.
Conclusion
Compared to conventional parotid MRI sequences, microscopy coil images can better define the margins of neoplasms, provide more detailed definition of lymph node morphology, and better depict certain cyst contents in the superficial portions of the parotid gland. However, the microscopy coil sequences lengthen the overall examination time and are not as well-suited for imaging deep parotid gland lesions. Thus, microscopy coil imaging for parotid tumors should be reserved for specific situations in which the technique may provide additional insights, such as those highlighted in this series. Ultimately, further evaluation of the impact of high-resolution parotid gland microscopy coil MRI upon patient management is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.