
Abstract
The following report is of a 36-year-old male who presented with a growing mass in the region of the parotid gland. Initial fine needle aspiration biopsy suggested a primary neoplasm of the parotid gland, but subsequent frozen section analysis intraoperatively demonstrated a schwannoma of the facial nerve. An intracapsular enucleation of the schwannoma was performed in order to preserve the fibers of the motor nerve.
Introduction
A mass in the region of the parotid gland typically suggests a neoplasm of the gland itself, such as a pleomorphic adenoma, Warthin tumor, mucoepidermoid carcinoma, or other salivary gland neoplasm. However, consideration should also be given to the possibility of a mass emanating from other structures located within the region, such as the facial nerve. Imaging, fine needle aspiration (FNA), core needle biopsy, as well as intraoperative frozen section can help distinguish between various potential etiologies and point to the most appropriate plan of management. In the current report, we present a case of a male who was initially thought to suffer from a tumor arising from the parotid gland but was subsequently proven to have a facial nerve schwannoma.
Case
A 36-year-old male presents with a large, painless right parotid mass that had been growing progressively for 3 years. The patient was otherwise healthy with no significant past medical or social history but had no health insurance.
The physical exam was notable for an 8 cm hypomobile, firm parotid mass with no overlying skin changes. The patient had intact function of the facial nerve and no trismus. The tumor extended from the preauricular region down to the neck. Fine needle aspiration biopsy was interpreted as “vascular salivary gland neoplasm of uncertain malignant potential.”
An axial computed tomography (CT) scan showed a large mass of the right parotid gland with a hypodense interior consistent with necrosis and an enhancing rim, extending into the deep lobe of the parotid gland and displacing most of the superficial gland superiorly and laterally (Figure 1). The patient’s lack of insurance delayed operative intervention, and he was lost to follow-up. Seven months later, however, the patient returned and was insured. The physical examination was largely unchanged and facial nerve function was still intact. On magnetic resonance imaging (MRI), T1 fat-suppressed contrast-enhanced axial imaging showed similar findings to that of the CT: A cystic peripherally enhancing mass of the parotid gland (Figure 2).
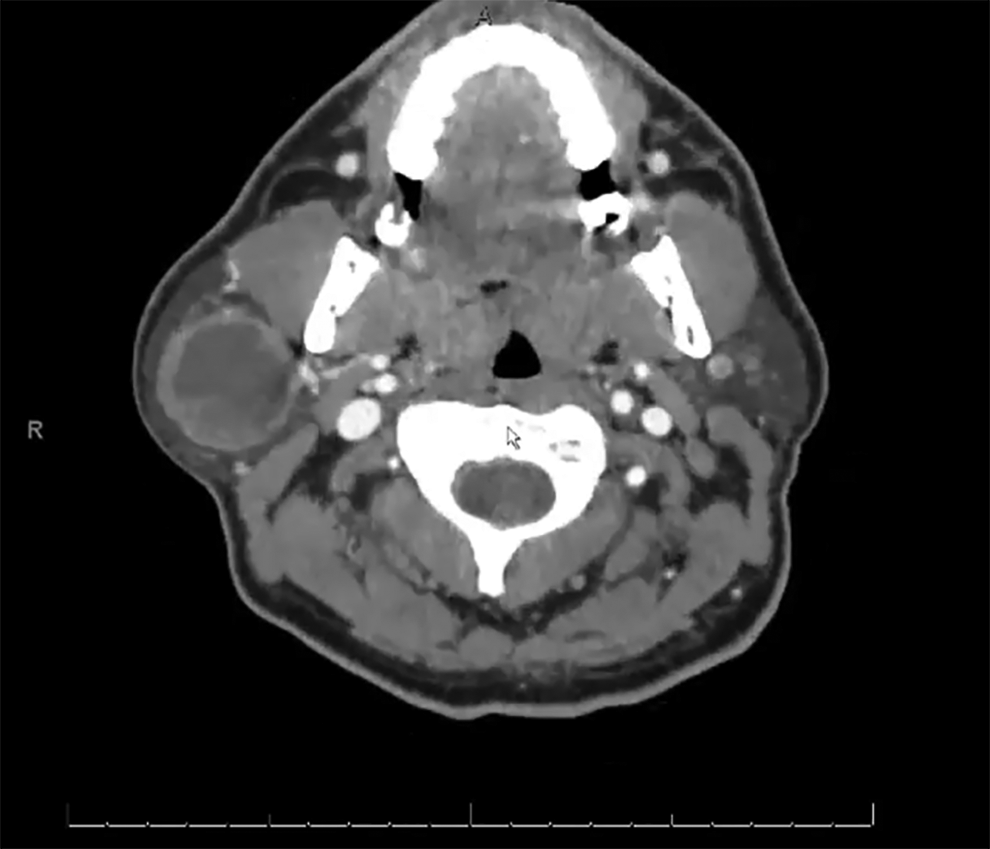
Axial computed tomography (CT) scan showing a large mass of the right parotid gland with a hypodense interior consistent with necrosis and an enhancing rim.
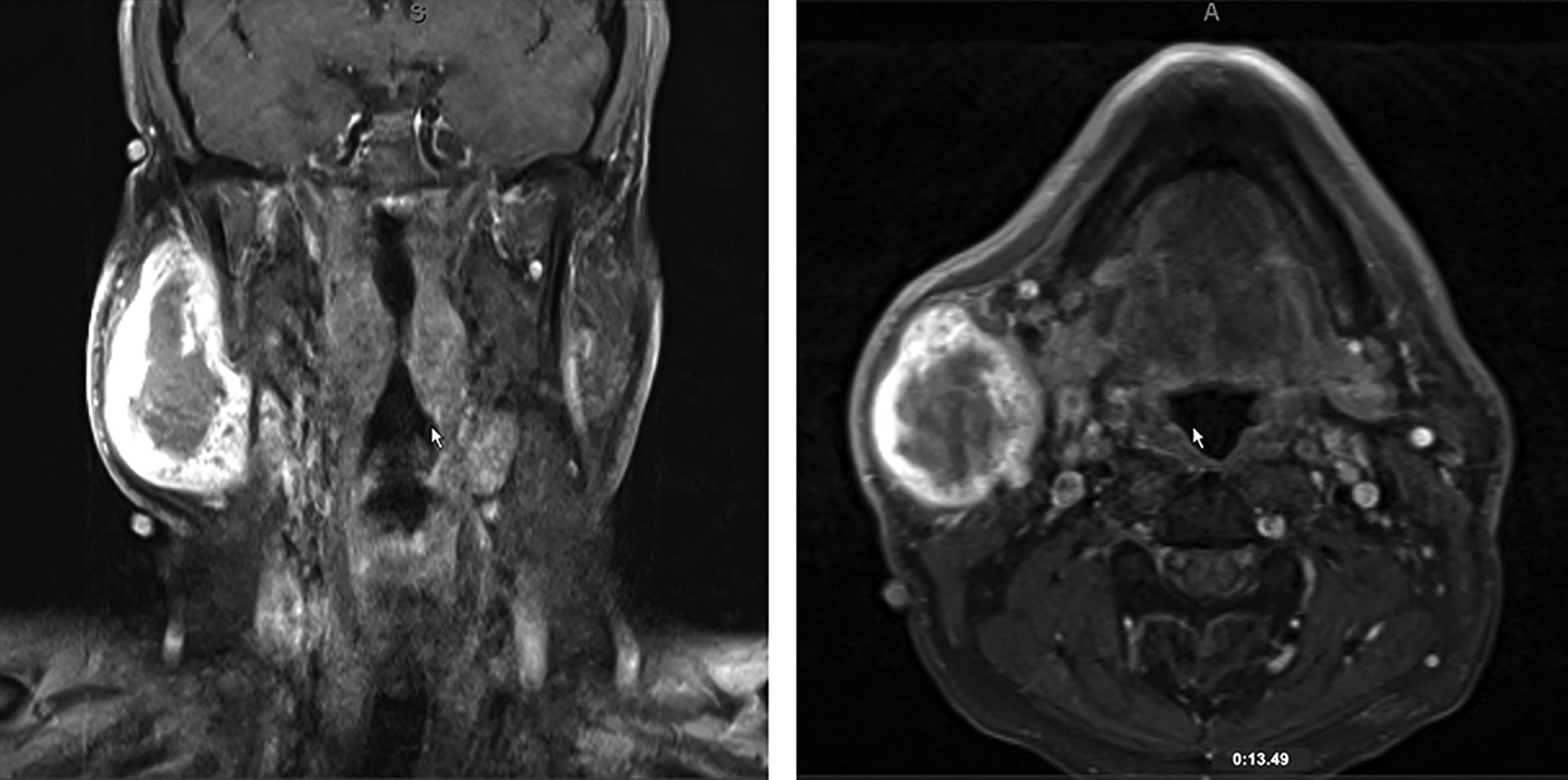
Coronal and axial T1 fat-suppressed, contrast-enhanced MRI showing a rim-enhancing large mass of the right parotid gland. MRI indicates magnetic resonance imaging.
Management discussed with the patient, and surgery was recommended. Given the size and involvement of the deep lobe of the gland and anticipating the possibility of a well-differentiated malignancy, the patient was consented for a total parotidectomy, possible neck dissection, possible facial nerve sacrifice, and possible anterolateral thigh fascial free flap with vastus nerve graft.
In the operating room, the mass was measured to be about 8 cm craniocaudal with a very firm leathery capsule surrounding it. The superficial lobe of the parotid was reflected upward, revealing the tumor residing in the deep lobe (Figure 3). The main trunk of the facial nerve proximally near the auricle could not be found due to obstruction of the view by the mass of the tumor but the buccal, zygomatic, and the marginal mandibular branches were identified more distally. Those branches were fused with the capsule of the mass. Given that these gross intraoperative findings were not consistent with a primary parotid neoplasm, a piece of the tumor was taken from between the identified nerve branches and sent for frozen section.
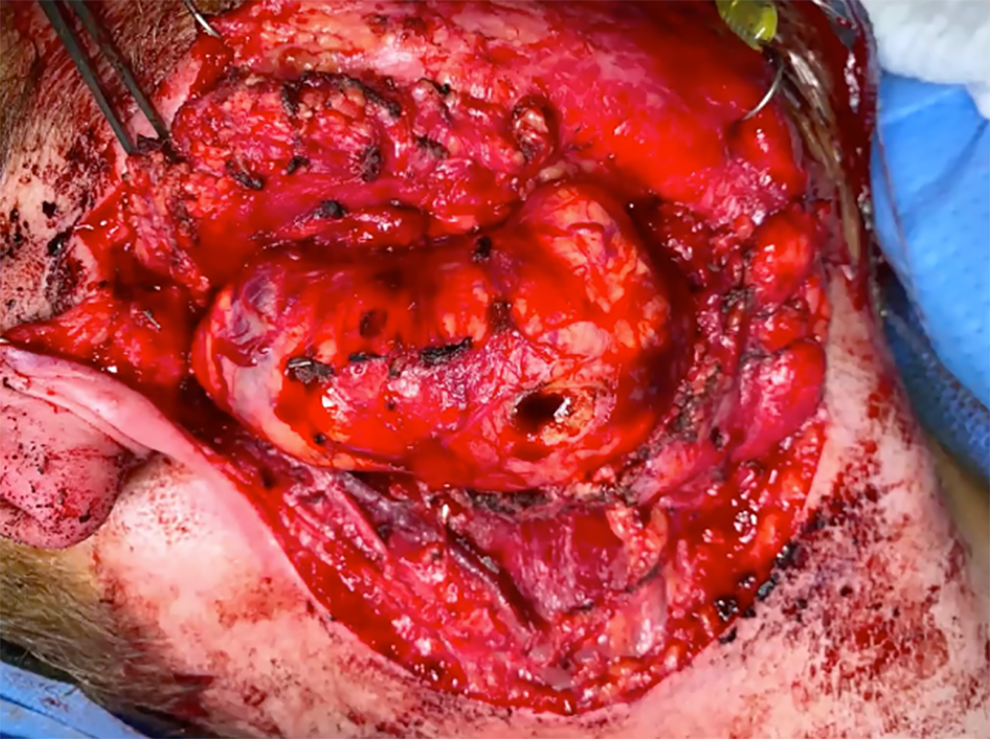
Encapsulated mass occupying the deep lobe of the parotid following superficial parotidectomy.
The frozen section revealed a benign spindle cell tumor. Contrary to what the FNA suggested (primary neoplasm of the parotid gland), this was likely a schwannoma of the facial nerve. Using a technique described in the literature, an incision was made into the fibrotic capsule of the schwannoma, followed by an intracapsular enucleation of the schwannoma, preserving the fibers of the motor nerve (Figure 4). The final diagnosis was a right parotid gland schwannoma (3.5 cm excision), and a right parotid gland benign parotid with 2 lymph nodes (superficial parotidectomy).
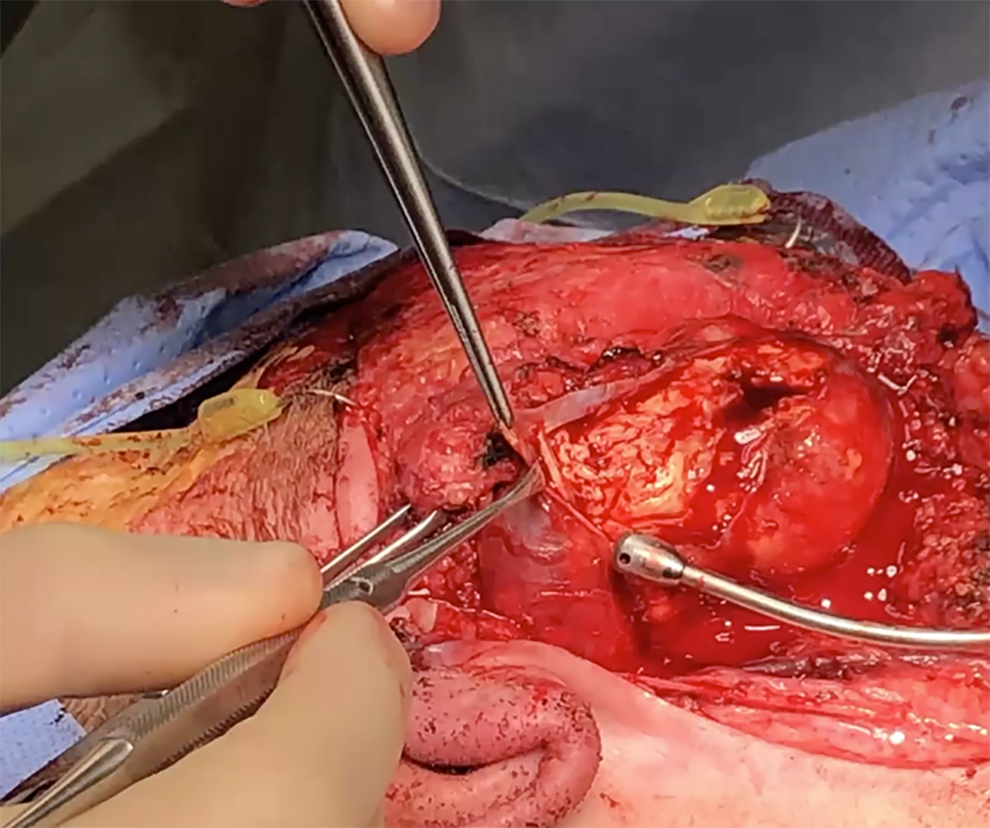
Intracapsular enucleation of the schwannoma, preserving the fibers of the facial nerve.
Immediately postoperatively, the patient maintained tone in the lower division of the facial nerve and demonstrated a slight twitch with volitional movement of the mouth (House-Brackmann [HB] IV) and had a complete paralysis of the upper division (HB VI). At 6-months postoperative, the patient had mild weakness of the lower division (HB II) and moderate weakness of the upper division (HB III).
Discussion
Facial nerve schwannomas are rare with most (83.6%) arising within the temporal bone. 1 They represent only a tiny fraction of intraparotid neoplasms, however, are an important consideration whenever considering surgery for a parotid gland mass. Imaging features that should prompt consideration of a facial nerve schwannoma include well circumscribed margins, displacement of local structures, internal cystic spaces, and heterogeneous high signal intensity specifically on T2-weighted MR images, all of which were present in our patient at time of presentation. 2
While FNA should be considered in the evaluation of almost all new parotid mass, the results are often not definitive. Parotid FNA has a wide range of described diagnostic accuracy ranging from 79% to 97%. 3 Fine needle aspiration is also particularly unreliable in differentiating benign from malignant parotid tumors. 3 In a recent case review of patients with facial nerve schwannomas, only 31.6% who underwent FNA had the correct diagnosis made prior to treatment, 1 consistent with our described experience.
Whenever performing parotidectomy for a parotid neoplasm, surgeons should maintain a low threshold to perform frozen section, particularly when gross intraoperative findings do not correlate with the presumed diagnosis. Studies have shown that this second line of inquiry can further confirm or even overturn prior diagnoses following FNA cytology. 4
Intracapsular enucleation of schwannomas was initially describes by Dr Netterville and Dr Groom at Vanderbilt University as a method of achieving gross total resection of cervical schwannomas while preserving nerve function. 5 Subsequent series have described this technique specifically for facial nerve schwannomas with all patients maintaining HB I or II function postoperatively 6 and this technique is now a well-accepted method of treating these tumors. This was successfully employed in our case with immediate preservation of some lower division function and subsequent partial recovery of the upper division.
Footnotes
Authors’ Note
This manuscript is original and has not been submitted elsewhere in part or in whole.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.