
Abstract
Background:
A lymph node yield (LNY) over 20 is considered a quality metric for lateral neck dissection to ensure an oncologic representative sample. Anecdotally, however, LNY in patients undergoing neck dissection after radiation therapy (RT) is lower due to atrophy and fibrosis.
Objective:
To determine whether preoperative RT decreases LNY in patients with laryngeal cancers undergoing surgery.
Methods:
Medical record database was queried for patients presenting between 2006 and 2015 with laryngeal cancer. Tabulation was made for location (glottic/supraglottic), stage, and side for the total number of lymph nodes between primary surgery and RT (salvage surgery) groups. Descriptive analysis and a paired Student t test were used for statistical analysis.
Results:
Fifty-nine patients were included in the study for a total of 98 neck dissections. Twenty-six (44%) patients had primary surgery, and 33 (56%) patients had salvage surgery. The mean left and right total LNY in the salvage surgery group was 27.6 and 29.5, respectively, and 32.2 and 33.7 for the primary surgery group. A difference of 4.5 (left) and 4.3 (right) in LNY between the salvage surgery and primary surgery group was found. A Student t test showed no statistically significant difference in LNY between both groups when analyzed per site (glottic and supraglottic), side, and stage (III-IV).
Conclusion:
Although patients with prior RT had a lower mean of LNY, our results did not demonstrate a statistically significant difference. Further studies with a larger number of patients are recommended.
Introduction
Lymph node (LN) metastasis is the single most important prognostic factor for patients with squamous cell carcinoma (SCC) of the head and neck. Primary surgical treatment versus primary radiation therapy (RT) can be affected by multiple factors such as disease stage, patient surgical eligibility, and patient and surgeon preferences. The extent of LN dissection has been an independent prognostic factor in several cancers, 1,2 with an association between higher lymph node yield (LNY) and improved survival for patients with oral cavity SCC. 3 The probability to histologically detect an LN+ neck increases with LNY, this way, having a direct impact on survival and outcome. Some have considered an LNY >20 to be adequate in increasing the probability of detecting LN metastasis, while others have reported a mean of 27.5 3 ; nevertheless, this number is not constant and is dependent on the type of neck dissection (radical, modified radical, supraomohyoid, selective, or lateral neck dissection). The role of RT on LNY in head and neck cancer has been studied in the past with different outcomes. 4 –7 The purpose of this study is to specifically evaluate the effect that RT has on LNY in patients with laryngeal SCC.
Methods
The institution review board of Augusta University approved this project. Medical record database was queried for patients presenting between 2006 and 2016 with laryngeal cancer. Tabulation was made for location (glottic/supraglottic), pretreatment radiologic Tumor-Node-Metastasis staging, and side (right/left) for LNY between primary chemoradiation therapy (salvage surgery) and non-RT queries using Microsoft Excel. Descriptive analysis and paired Student t test were used for statistical analysis; significance level was predicted with a P < .05. Inclusion criteria were patients with laryngeal SCC (glottic and supraglottic) who underwent selective neck dissection from levels 2 to 4, completed RT, and had a complete pathological report. Patients were divided in 2 groups: one group with primary surgery as treatment modality and the other group as salvage surgery (patients who underwent primary chemoradiation and then surgery).
Results
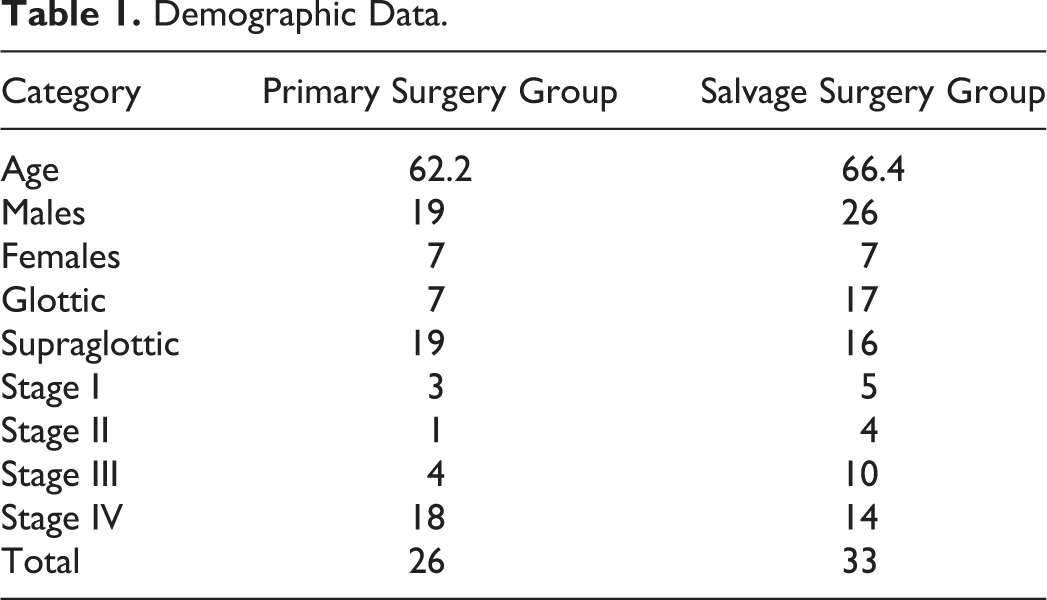
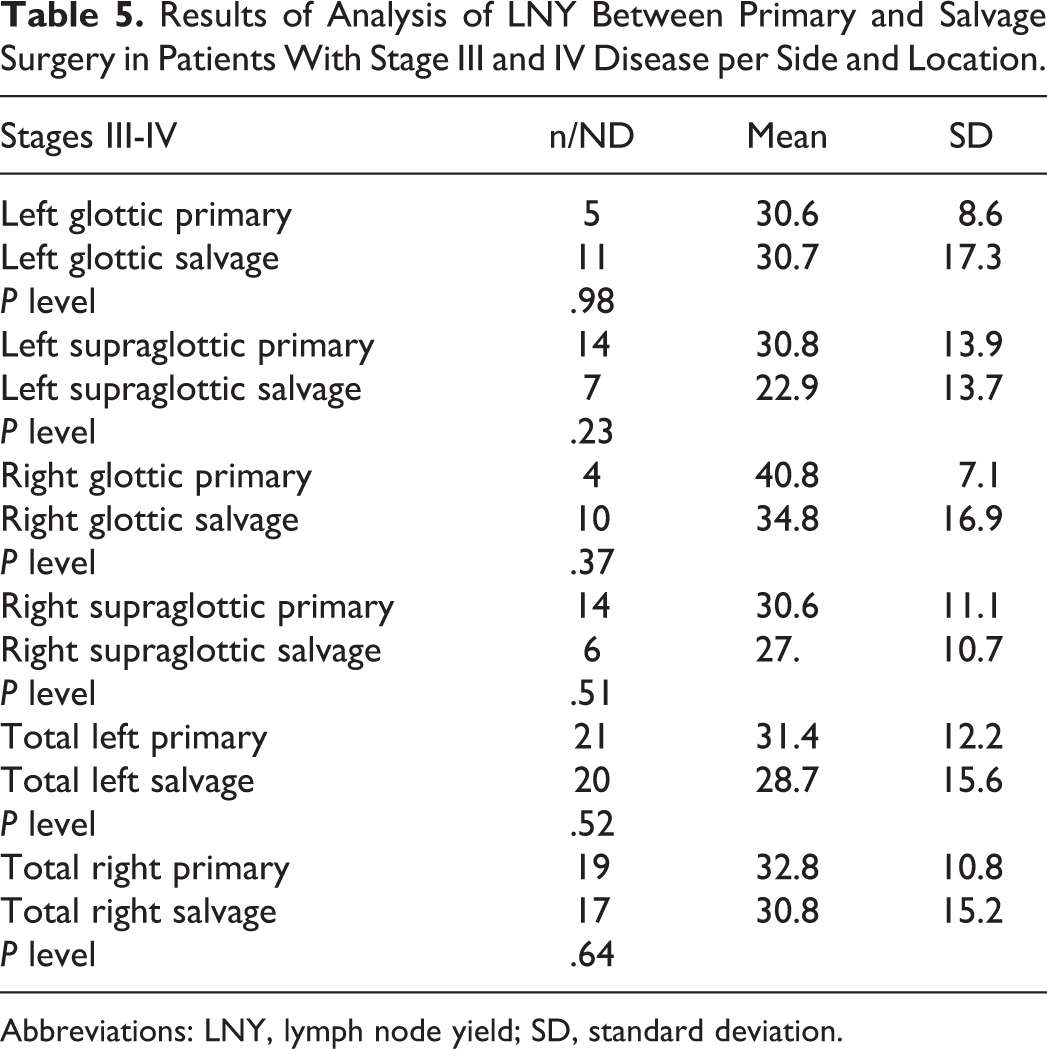
Sixty-five patients were included in the study for a total of 98 neck dissections (ND). A total of 26 (40%) patients had primary surgery and 39 (60%) patients had primary chemoradiation therapy or RT with subsequent salvage surgery. Demographic data are presented in Tables 1 to 3. Patients with stage I and stage II disease were excluded because these patients were treated with narrow field radiation to the primary site. All NDs were performed at an academic tertiary care institution. The average time from RT to ND (salvage surgery time) was 38.4 months (3.2 years). Therapeutic RT with or without chemotherapy was administered with a total dose ranging from 66 to 72 Gy to the primary site and neck. The mean left and right total LNY in the salvage surgery group was 27.6 and 29.5, respectively, and for the primary surgery group was 32.2 and 33.7, respectively. A difference of 4.5 (left) and 4.3 (right) in LNY between the salvage surgery and primary surgery group was found. A Student t test showed no statistically significant difference in LNY between both groups when analyzed per site (glottic and supraglottic), side, and stage (III-IV; Tables 4 and 5).
Demographic Data.
Distribution of Disease Stage in Relation to Tumor Location.
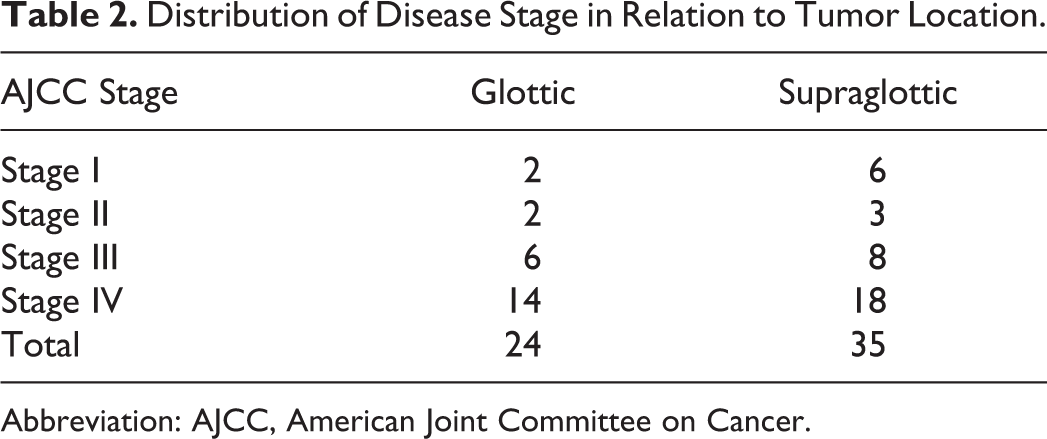
Abbreviation: AJCC, American Joint Committee on Cancer.
Salvage Surgery Group—Patients Who Received RT or CRT.
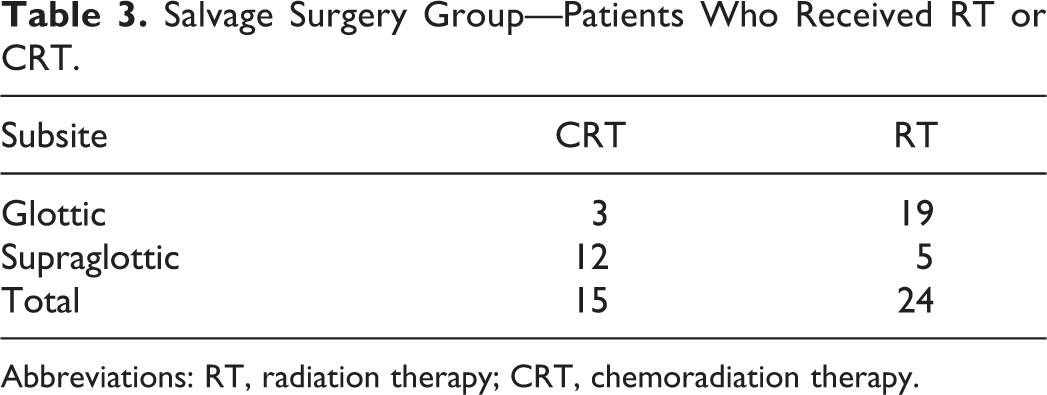
Abbreviations: RT, radiation therapy; CRT, chemoradiation therapy.
Results of Analysis of LNY Between Primary Versus Salvage Surgery.
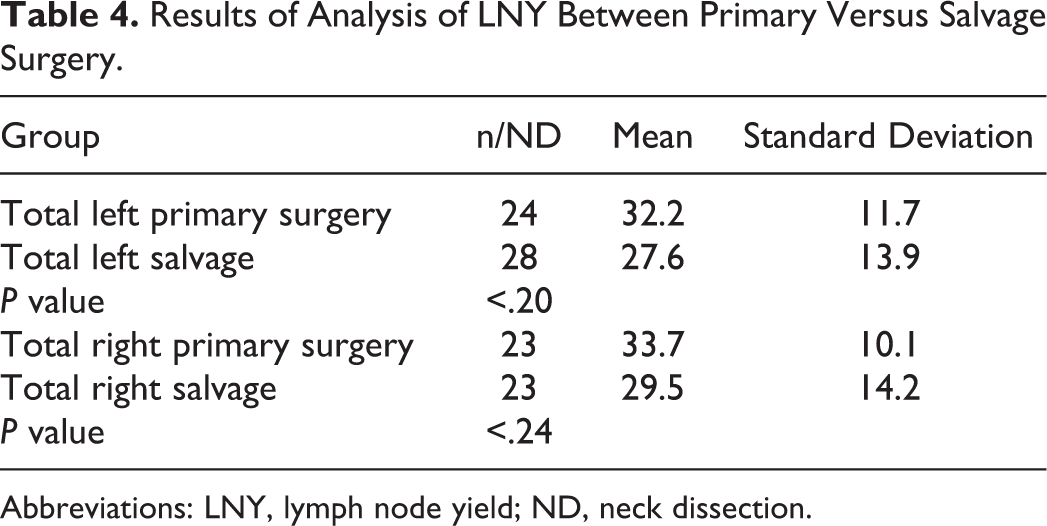
Abbreviations: LNY, lymph node yield; ND, neck dissection.
Results of Analysis of LNY Between Primary and Salvage Surgery in Patients With Stage III and IV Disease per Side and Location.
Abbreviations: LNY, lymph node yield; SD, standard deviation.
Discussion
Tumor ablation and neck dissection is considered the standard of care for the treatment of most head and neck cancers, especially SCC. In some scenarios, such as advanced stage III and IV SCC, combined chemoradiation therapy has been used as primary treatment modality. The importance of LNY in patients with SCC of the head and neck has been well-documented. 3,8,9 In clinically N0 patients, increased LNY has improved survival outcomes and lower regional recurrence for oral cavity, 3 lip, floor of mouth, tongue, and gum 9 SCC by removing micrometastatic disease in addition to more accurate staging.
A paucity of data has been published about the effects of preoperative radiation on LNY; only 5 publications to our knowledge have approached this subject. Carter et al 4 briefly mentioned observing a decrease in LNY after radiotherapy in patients with nasopharyngeal, esophageal, oropharynx, larynx, and hypopharynx cancer but ran no formal statistical analysis. Moore and Bhattacharyya 6 assessed LNY between irradiated (LNY = 23.5) and nonirradiated (LNY = 23) matched neck-level dissection in patients with oropharyngeal, laryngeal, and hypopharyngeal SCC and found no statistically significant difference (P = .77) on the effects of preoperative radiation on LNY, although they included all primary site as one category. Johnstone et al 7 analyzed the effects of RT on LNY in patients with cancer from the oropharynx, tonsil, hypopharynx, or larynx and found a statistically significant decrease in LNY with preoperative radiotherapy; however, their data came from the Surveillance, Epidemiology, and End Results (SEER) database, they did not described the histologic type of cancer, and they did not define which neck levels were used in their analysis.
Moore and Bhattacharyya 6 analyzed the effects of different neck dissection techniques, such as selective neck dissection (SND), radical neck dissection (RND), or modified radical neck dissection (MRND) on LNY in patients with thyroid, cutaneous, orohypopharyngeal, and laryngeal cancer. They concluded that there was a statistically significant decrease in LNY in radiated patients versus nonirradiated patients (17 vs 22; P < .02) looking at all neck dissection techniques together. However, when analyzed independently, only the MRND group was found to have a statistically significant decrease in LNY, while all other types of neck dissections had no statistically significant difference in LNY. It is logical to conclude that a radical neck dissection or an MRND has an increased LNY when compared to a selective or supraomohyoid neck dissection due to more dissected levels. Therefore, we specifically included only patients with laryngeal SCC who had neck dissection from levels II to IV and matched them by side and stage in order to attempt to remove the confounding effect of differing neck levels on LNY.
Harvesting a significant LNY in previously irradiated patients is more difficult, this way compromising the LNY due to the fact that RT to the neck results in fibrosis and fatty replacement of the cervical LN, particularly for patients who had radiation 6 years prior to surgery. 10 This means that the timing between RT and neck dissection is important, as a fibrotic specimen will entail more difficulty in identifying LN in a sample by the pathologist, and patients with longer intervals between RT and neck dissection may have a lower LNY. Our cohort had a mean time between RT and ND of 3.2 years. About a fifth of our patients analyzed had an over 6 years’ time elapse between radiation and neck dissection; however, the number of patients was too low to significantly affect our results.
Discordant results of the effects of preoperative radiotherapy on LNY may also be explained by a lack of congruity in each paper selection of primary cancers by histologic type. Because radiation sensitivity is dependent on the prolific activity of the tumor, different histological types of cancer respond differently to radiation. 11 A discrepancy exists not only between the histologic type of head and neck cancer of our results and the literature but also among the published papers themselves. Our data were only taken from histologically proven SCC of the larynx, while other authors included papillary thyroid, melanoma, adenocarcinoma, and undifferentiated cancer in their statistical analysis. In addition to this, we included only LNs from levels II to IV in order to attempt to remove the effect of differing neck levels on LNY. The small number of patients and our sole focus on primary laryngeal SCC leads to a lack of generalizability of our results. It is difficult to discern whether the enhanced effects of radiation when simultaneously administered with chemotherapy could have had any effect on LNY; although it wasn’t the objective of this study, we did not find a statistically significant difference in LNY between patients who had chemoradiation (CRT) versus those who had RT only (21.7 vs 26.3, respectively; difference = 4.6, P = .23). Our results show that for laryngeal SCC, previous RT has no impact on LNY, however, due to the conflicting conclusions drawn by previous authors, future studies with a focused approach by primary disease location, use of CRT versus RT, tumor histology, and neck dissection levels done may be required to define the overall effects of RT on specific head and neck cancers.
Conclusions
Radiotherapy does not significantly reduce LNY in patients with glottic and supraglottic SCC. After radiotherapy, a significant number of LNs will remain in the neck similar to a nonradiated neck. A surgeon should therefore do his or her best to harvest an adequate sample for proper metastatic disease identification.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.