
Abstract
Loneliness and isolation are recognized as distinct phenomena, however, each can have a profound negative effect on anyone experiencing them long-term (Yang, 2019). Loneliness is defined as a subjective, painful feeling, experienced when an individual recognizes their relationships are not as they would wish them to be (Perlman & Peplau, 1981). Isolation, however, is defined as an objective state of limited or absent social interaction or relationships (Fakoya et al., 2020). Chronic loneliness is associated with severe physical and mental health outcomes, including stroke, high blood pressure, suppressed immune system, depression, sleep disturbance, and even early mortality (Cacioppo & Capitanio, 2014).
UK governmental data indicates that people with a disability are more likely to report feeling lonely than the general population. However, these figures do not report levels of loneliness among people with specific conditions, such as visual impairments (Qualter et al., 2023). A 2013 review of evidence about the prevalence of loneliness and isolation among people with visual impairments found some modest evidence of an increased risk for these conditions, while noting findings across studies were inconsistent (Hodge & Eccles, 2013). More recent studies have found significantly higher levels of loneliness among participants with visual impairments (Brunes et al., 2019; Mick et al., 2018), while others have not established any association (Harithasan et al., 2019). A small number of studies have found lower levels of loneliness among people who are visually impaired compared to people without visual impairments (Rokach et al., 2021; Stanimirović et al., 2017). Over 2 million people in the United Kingdom live with some degree of visual impairment. Of this number, 340,000 individuals are registered as “severely sight impaired” (i.e. blind) or “sight impaired” (partial sight or low vision). Since visual impairment is more prevalent among older people, these figures are projected to rise because of the aging population in the United Kingdom (Royal National Institute of Blind People, 2023).
Methodology
Participants
Interview participants were recruited by disseminating information about the study to a range of voluntary sector organizations for people with visual impairments. People who expressed interest in being interviewed were given detailed information about the study before they confirmed their participation. The average length of interviews was around one hour. Eighteen interviews were conducted in line with the recommended sample sizes in grounded theory (Corbin & Strauss, 2015).
The age range of participants was 18 to 73 years (mean = 51.89). Eight males and nine females took part, along with one participant who is gender fluid. Fourteen participants lived in England, and two apiece lived in Scotland and Wales. Sixteen of the participants were citizens of the United Kingdom, one was Irish, and one was from the United States. Seventeen participants described their ethnic group as white, while one person identified as Black British. Seven interviewees were employed full-time, and six had retired or given up work due to their visual impairment. Two were unemployed, two had retired for reasons unrelated to their visual impairment, and one was in full-time education. Nine interviewees lived alone, six lived with their spouse or partner, two lived with their family of origin, and one lived with their adult daughter. Six members of the sample were married or cohabiting with a partner, and three were in a relationship and lived apart from their partner. Four were single and had never been married, three were divorced, and a further two were widowed. Fifteen participants described their sexual orientation as being heterosexual or straight. One person was gay, one was bisexual, and one was pansexual. Sixteen of the participants were registered as “severely sight impaired,” and one was registered as “sight impaired.”
An online survey was created from themes identified in the interview data. Overall, 162 responses to the survey were recorded. However, respondents were free to omit any questions they did not want to complete, resulting in variation in the number of responses provided to specific questions.
Participation was completely anonymous and no identifying information was collected. However, some demographic information was collected including the age, current gender, and ethnic group of participants which are presented in Tables 1 to 3, respectively. Of the respondents who chose to disclose their level of visual impairment, 75% (84 individuals) described this as severely sight impaired or blind, while 25% (28 individuals) chose the term sight impaired or partially sighted.
Age Distribution of Survey Respondents.
Current Gender of Survey Respondents.
Ethnic Group of Survey Respondents.
Data Collection
During each interview, participants were asked about the background to their eye condition and level of visual impairment; their past and present experiences of loneliness and isolation, and how these had been affected by their visual impairment; factors in their life that mitigated against their feelings lonely or being isolated; and their experiences of loneliness and isolation during the COVID-19 pandemic. Although discussion on these topics was consistent across interviews, the range of experiences described by participants led to significant variation between interviews. This variation was facilitated and encouraged by the interviewer adopting an open curiosity to whatever participants brought to the discussion. All interviews were conducted by the first named author.
All interviews took place either over the telephone or on Microsoft Teams video conferencing software. Interviews were recorded and transcribed verbatim. Anonymization took place during the transcription process.
The survey was distributed by major UK sight loss charities who invited the participation of all people who use their services. Qualtrics software was used to create the survey due to it reputedly having good accessibility features for use by people with visual impairments. The survey's accessibility was checked by the three authors of this paper, who have severe sight impairments.
The survey sought to measure the prevalence of feelings of loneliness among respondents. Participants were also given the opportunity to validate the themes identified through the interview analysis as well as provide free-text answers about their own experiences of loneliness and isolation.
Measurement of Loneliness
Participants in both the interviews and the survey completed the UCLA-3 Loneliness Scale and were directly asked how often they felt lonely. The UCLA-3 Scale is a validated measure of loneliness, widely used in academic studies about loneliness (Daniel et al., 2023). This scale is also used by the UK government in national studies of loneliness and allows comparison with data for the UK population (UK Office for National Statistics, 2018).
Data Analysis
Reflexive Statement
Two authors are registered counselors, who have an interest in visual impairment and mental health. Two authors work for a leading sight loss charity. Three authors are severely sight impaired.
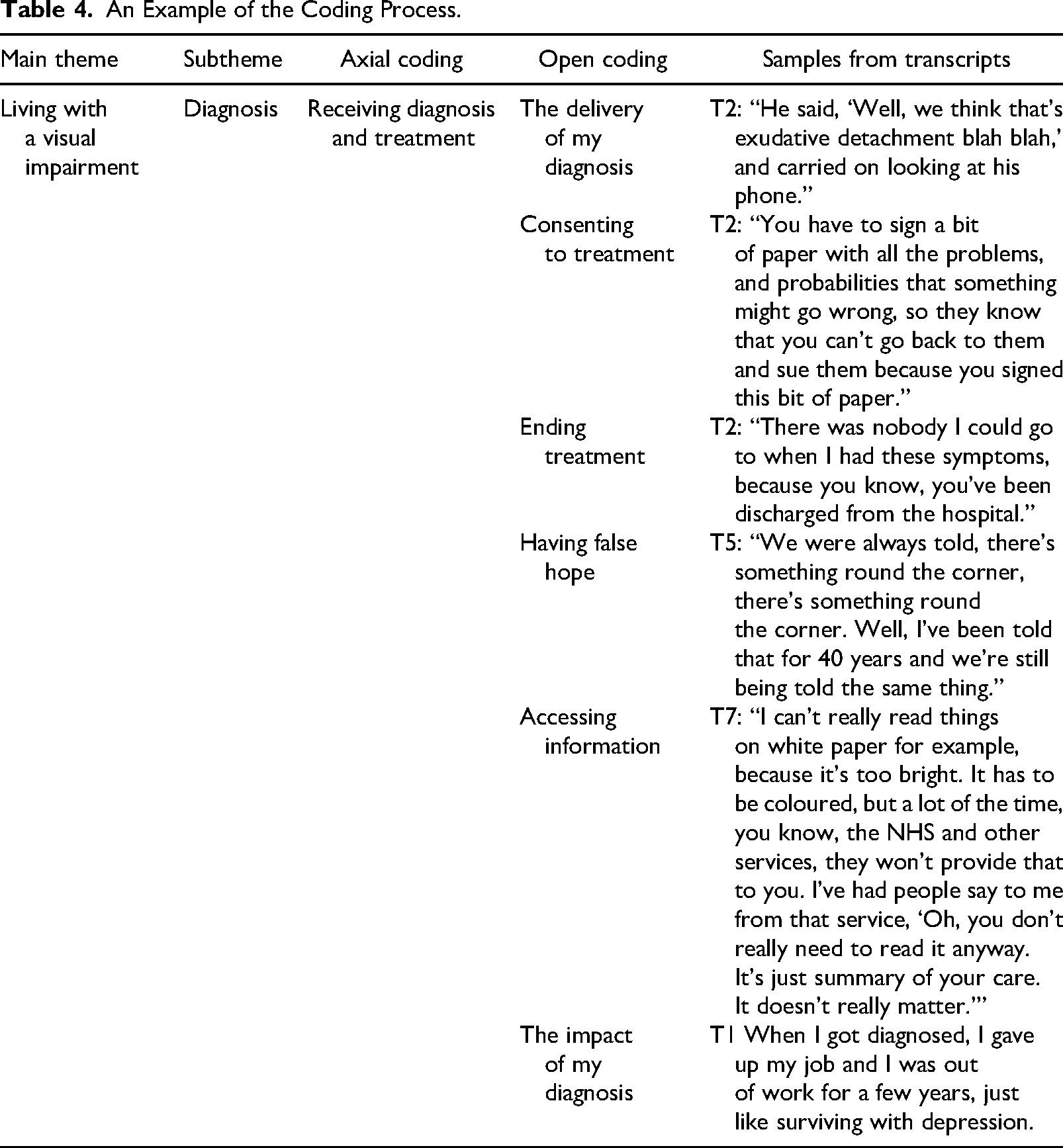
Interview transcripts were analyzed by the interviewer and verified by a senior researcher. Themes were identified within the transcripts using a grounded theory approach (Corbin & Strauss, 2015), and analysis remained open to what participants brought to the interviews, rather than the discussion being led by any existing theories or knowledge. A sample of the coding process is included in Table 4.
An Example of the Coding Process.
The survey data on the prevalence of loneliness were analyzed using descriptive statistics. The answers to the open questions in the survey were assessed for their consistency with the themes identified during the interviews.
Results
Three over-arching themes were identified, each of which had several subthemes:
living with a visual impairment, psychosocial impacts, and mitigating factors.
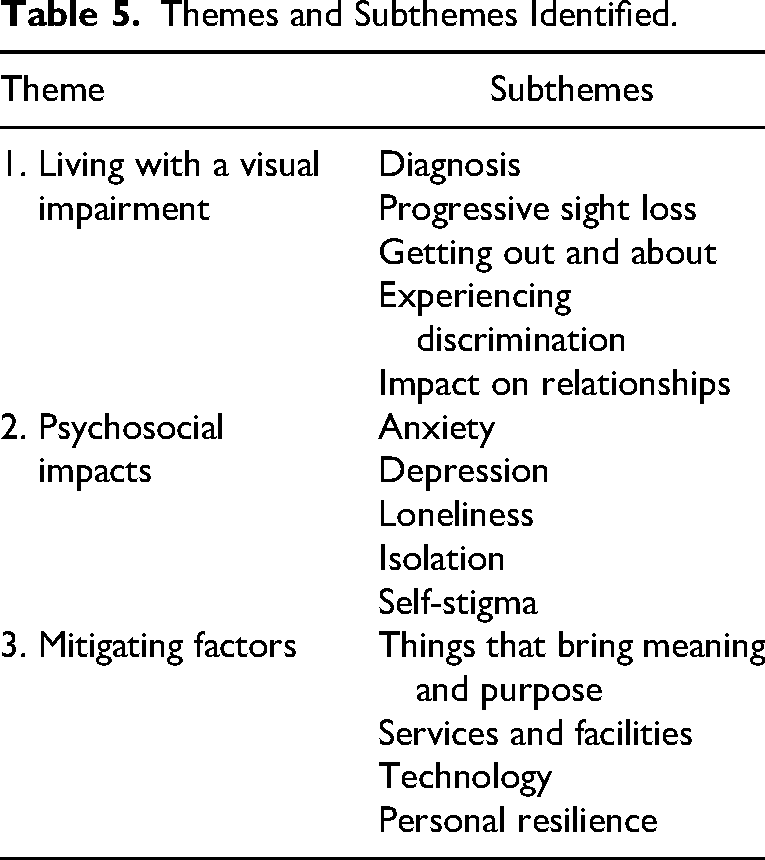
Table 5 shows the subthemes identified in relation to each of these main themes. These themes were reflected in the open-question answers of the survey. No new themes emerged.
Themes and Subthemes Identified.
Theme 1: Living With a Visual Impairment
Diagnosis
Being diagnosed with a visual impairment (i.e. blindness or low vision) was frequently identified as being an experience of shock, fear, and trauma. Interviewees highlighted they were offered little support in dealing with the emotional impact of receiving this news. As one participant stated: It's still very devastating when you do get the diagnosis. … You just feel like the rug's been pulled out from underneath you. There's absolutely no help or support, they don’t give you any counseling or anything like that. (Female, aged 58 years)
For some of the participants, the point of diagnosis could also be accompanied by major life changes, such as having to give up working or driving. These changes could have significant effects on their sense of connectedness, contributing to loneliness and isolation: That [diagnosis] was the start of me not being able to drive … when that happened, I went through a very low spot, when it was obviously clear that I wasn't going to be able to get around and I wasn't going to be able to do certain things. (Male, aged 63 years)
Progressive Vision Loss
Most of the interviewees were living with progressive vision loss conditions, which require individuals to have to continually adjust and readjust to the effects of their diminishing eyesight. For most of the interviewees in this study, this process was gradual and tended to unfold over many years. As one participant stated: I think that the challenge for my particular condition is, it doesn't stop. What used to happen, … it still is happening, is that the change is much more impactful. I wake up certainly every week and sometimes even every day and I think, umm, I can see less today than I could see yesterday. (Male, aged 55 years)
Interviewees described fear and anxiety which entailed a sense of dread over the future, knowing that their vision would continue to deteriorate: Oh lord, it's only going to get worse. … [C]oncern about what the future might hold, it's in the back of my mind all the time, and I would guess it probably is for most of us in this situation. (Female, aged 73 years)
Getting Out and About
Virtually all the interviewees spoke of difficulties they routinely experienced in getting out and about. These issues were mainly in relation to two broad areas: the inaccessibility of environments, venues, transport, and navigation, and the attitudes and behavior of other people in the community. Comments from four participants illustrate these concerns. I can't use the buses at all because the stations aren't manned. They’re on diversion so often and the voiceover sometimes isn’t in use, so you just don’t know where you are. (Gender fluid, aged 30 years) More and more local authorities are actually putting street furniture in the middle of the pavement. (Male, aged 63 years) I find it just wears you down. If you’re just going to the shop or you want a quiet pint or a meal with a friend or whatever, and people are like, “Been blind all your life, have you?” … I'm just trying to chill out. Why are you putting the spotlight on me like this? (Male, aged 37 years) Everybody goes quiet when they see you, you can feel them tensing up, they don't say anything. … I say to people, “Do say something, you know, being quiet, it's the worst thing you can do.” (Male, aged 52 years)
Experiencing Discrimination
Most of the participants were able to recount experiences of discrimination, either indirectly or directly, while out and about. I was within my white cane training. Not, an actual session, but within the month or two months I was training, and there were these elderly women and one said to the other, “Oh, what the hell is he doing out? If he can't see, he shouldn't come out.” (Male, aged 65 years)
The impact of incidents like these was reported as being particularly difficult to deal with: It would be so easy to curl up in a shell and think, you know, bollocks to it. I ain't going out. I'm not doing it. (Male, aged 65 years)
Impact on Relationships
Among the most direct impacts on isolation and loneliness were the effects that having a visual impairment had on relationships. There was a wider spectrum of friends, but their lives have changed, and they’ve moved and had families. They forget, you know; you’re just forgotten about. (Female, aged 55 years)
Often people attributed diminishing friendships to their being unable to participate fully in activities or a self-perception that they would be a burden. The friends that you thought you had, they also sort of slowly disappear. Nobody wants to drag a blind person ‘round with them when you go to the shops or what have you. I don’t know, all the friends I thought I had, which was a lot, I could now sort of most probably count less than a handful now. (Female, aged 58 years)
Participants spoke of the effect of visual impairment on their ability to form and maintain intimate or romantic relationships. For some, their visual impairment meant that they did not seek to form this type of intimacy with others. Because of my sight, I haven’t sought a relationship, because I just can’t read people like I used to be able to. (Female, aged 55 years)
Others who had sought romantic relationships believed their visual impairment was an impediment to forming one, and that they were less attractive to potential partners as a result of it. I attempted last year to go back to dating, and I did actually specify that I was disabled. Obviously, the end result was that I had no contact with anybody. I knew that that would be the case. (Male, aged 63 years)
Some interviewees believed their visual impairment had contributed to the breakdown of relationships, mainly due to their not being able to fulfill expected roles within relationships. It assisted in causing the breakdown of my first marriage due to the fact that I think that my wife, well she had to do all the driving and everything else. It strained the marriage, and we had 3 young children at the time. Yeah, it wasn’t easy. (Male, aged 66 years)
Theme 2: Psychosocial Impacts
Having to continually deal with aspects of living with visual impairment appeared to contribute to a range of impacts on participants’ sense of well-being and mental health.
Specific screening for mental health difficulties was not performed within the interviews, however, 15 of the 18 interview participants disclosed that they had experienced mental health problems or distress that they related to the effects of their visual impairment.
Anxiety
One of the most reported effects was people living with a heightened sense of anxiety: I suppose there's this degree of anxiety all the time. (Female, aged 73 years)
For some participants, to manage their anxiety, they would limit their participation in activities and avoid social situations that involved going out: I won’t go out on my own because you never know what you’re going to encounter. I talk myself out of going to places because I don’t feel safe. I’ll just sit in at home where I feel safe. (Female, aged 66 years)
Since anxiety was also felt by participants regarding their relationships with other people, some also chose not to engage with others. I isolate myself a lot now because I just think, I don't want to get hurt again. (Gender fluid, aged 30 years)
Depression
The experience of depression, low moods, and hopelessness were also frequently described within the interviews. … I think there were periods where I was definitely having extended periods of low mood and hopelessness, you know, not wanting to do anything, just generally being in quite a low mood. (Female, 21)
Four participants, either directly or indirectly, mentioned that they had experienced suicidal thoughts.
Loneliness
Since the UCLA-3 and direct loneliness questions were asked across both the interviews and the survey, the results of both of these parts of the study are described within this section. The mean UCLA-3 score across the interview participants was 6.8.
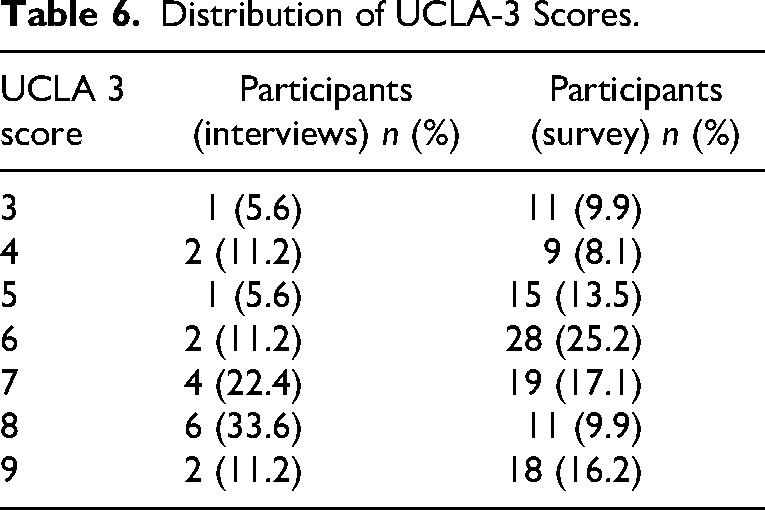
In the online survey, 111 responses were received to the UCLA-3 part of the questionnaire. The mean score across these responses was 6.3. The distribution of scores across participants is shown in Table 6.
Distribution of UCLA-3 Scores.
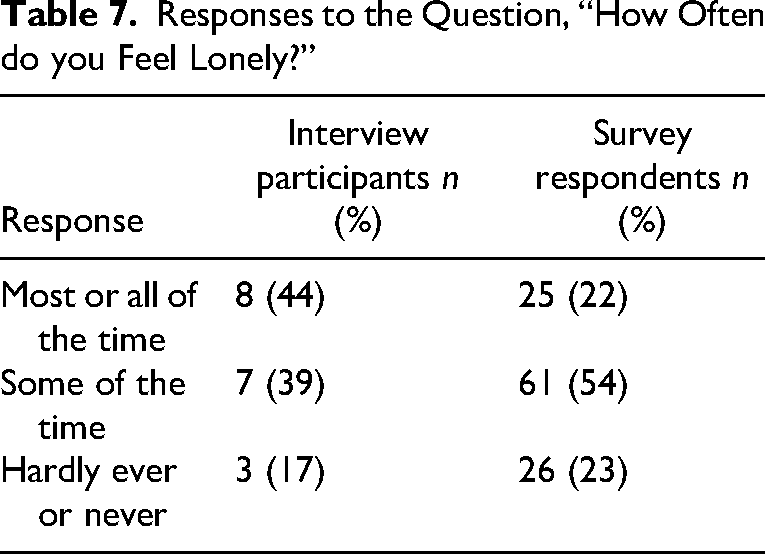
In answering the direct question, “How often do you feel lonely?” Eight interview participants (44%) and 25 (22%) of the survey respondents reported that they feel lonely most or all of the time; seven interviewees (39%) and 61 (54%) of those who completed the online survey stated that they feel lonely some of the time; three individuals (17%) who were interviewed and 26 survey respondents (23%) said that they hardly ever or never feel lonely (see Table 7).
Responses to the Question, “How Often do you Feel Lonely?”
All but one of the interview participants were able to describe lived experiences of loneliness; for many, this feeling was a recurring, if not constant, part of their lives. Loneliness was felt by interviewees in several circumstances.
Within the interviews, participants described emotional loneliness because of the effect of visual impairment on their relationships and social interactions: I think as human beings we need “people contact.” I do sometimes feel lonely and wish there was somebody here. (Female, aged 55 years)
Social loneliness was evident as people described their inability to access fulfilling relationships and opportunities for connection: People don't approach you, people don't get involved, and very few people help. It's like you’re living in a world of one, all the time. (Male, aged 52 years)
Existential loneliness, as a feeling of being separate or different from others, was also in evidence for some of the interviewees: When people are talking, I’d like to have some happy banter, but they get so nervous. [They think,] I can’t say see, I can’t say sight, don’t talk about books or the telly. It makes you feel that bit more lonely that they have got to have a guarded conversation, because you are losing your eyesight. … They can't have a natural conversation, which is a great shame. (Male, aged 65 years)
Isolation
Isolation was also commonly experienced by participants: I do have days when I’m completely on my own and I don’t see or speak to anybody other than the telly, which becomes your best friend, basically. (Female, aged 58 years)
People expressed a sense of being isolated while in the company of others through being excluded, ignored, overlooked, or treated inappropriately within social situations. This treatment could result in them feeling that they were not accepted by others. It's not said, but I often get the feeling of um not really quite fitting into the group. (Female, aged 57 years)
Several participants spoke of deliberately choosing to isolate themselves rather than being exposed to potential experiences of rejection or exclusion by others. Some of the isolation and loneliness comes out as a result of the fact that I am blind and out of the choice that it is more comfortable for myself to live this sort of lifestyle than it is for me to be in places where I feel out of my depth and not able to deal with the situation that I’m in. (Female, aged 68 years)
Self-stigma
Self-stigma is the internalized adoption of negative attitudes and stereotypes that are held about a group of people sharing a particular characteristic such as a disability (Bulk et al., 2020). Several statements were made within interviews displaying levels of self-stigma that participants held toward themselves. A lot of people wouldn’t want to spend time with a blind person. You can’t do the things that they want to do any more. You’re just much more limited, I think. (Female, aged 66 years)
These negative attitudes resulted in individuals trying to conceal their visual impairment from others, as well as to deny the reality of it themselves. For example, a person could reject low vision devices and adaptations, such as guide dogs or white canes, since these items would involve the person having to accept the effect of their visual impairment, as well as making it visible to others. I didn’t use a stick [white cane] then. You also think to yourself, “I'm giving in to it.” If you use a stick, it's won. (Male, 52)
Theme 3: Mitigating Factors
Participants identified a wide range of aspects of their lives that promoted well-being, connections, and could alleviate loneliness. Alongside this recognition, however, was the awareness that there were often obstacles in being able to maintain these elements.
Things That Bring Meaning and Purpose
All the participants described aspects of their lives that provided meaning and purpose for them as individuals. Their engagement with these things helped them live with or overcome loneliness and isolation. Some of the more commonly mentioned activities included:
engaging with nature and being outdoors; physical activity, exercise, and sports; cultural and artistic activities; and employment and work, including voluntary and community-based activities.
Comments demonstrating meaningful and purposeful engagement include: I’ve got my own fishing boat, as well, and I can hear dolphins and porpoises from a long way away, and that sort of thing. I can smell ships—smell the smoke from ships from a long, long way—long before the other people on the boat can see them. (Male, aged 66 years) I do yoga, body strength, running, walking, swimming in the sea. (Male, aged 65 years) I love theater. Last night, we went to Shakespeare. (Female, aged 73 years) … I knew I liked helping people. … [Working as a vision rehabilitation officer] was something I felt I could do and would be a positive move. (Female, aged 68 years) I’m a bit of an entrepreneur, so I’ve been involved in projects making products that help other people with visual impairments. (Male, aged 66 years)
Most of the participants pointed out there could be barriers to accessing these activities, which were generally related to the difficulties getting out and about, the inaccessibility of venues, and experiences of discrimination.
Services and Facilities
Participants mentioned that counseling had helped them in coming to terms with vision loss. The importance of being able to access the right type of counseling was highlighted. Some participants accessed counseling privately, while others had been provided access to counselors through their employers. For others who did not have these options available to them, counseling appeared to be out of reach. If counseling was offered to me, I would definitely go, I think, but you try and get it through the doctor. It's just not available out there to anybody. (Female, aged 58 years)
Some participants had engaged with groups and activities specifically designed for people with visual impairments within their areas. Although noting the potential value of these activities, most individuals had the impression that they catered to an older demographic. Subsequently, such interactions were of limited interest to those who took part in this research. Where are all the young blind people? I really don’t know. All of the organizations that there are seem to be [for people who are] about 80 plus [years old]. (Male, aged 65 years) You know any clubs or any associations out there are all for retired people in their 60s and 70s, and you go along and you’re only 50. … [E]verybody looks at you as if to say, “Well, what are you here for?” It's just you feel more and more and more isolated. (Female, aged 58 years)
The opportunity to take part in activities or groups with a focus meaningful to that individual, rather than merely the shared experience of living with visual impairment, appeared more valuable to participants.
Technology
Several participants noted the value of being able to interact online and that social media groups and other forums for people with particular conditions were a useful source of information and support. The use of technology as a means of connecting with people more generally was regarded as a relatively poor substitute for in-person interactions. There were also concerns about the honesty and authenticity of people and relationships developed through social media or other internet-based means. [Forming a relationship] [o]nline doesn't necessarily make up for what it would be like to know someone personally who actually relates [to this] kind of thing. (Female, aged 21 years)
Discussion
There is not a great deal of previous research that has examined the qualitative experiences of people with visual impairments in relation to isolation and loneliness. What evidence exists has been inconsistent, with some studies finding higher levels of loneliness described by people living with visual impairments, while others have not drawn the same conclusions. The findings of this research support a relationship between loneliness and visual impairment and describe potential contributing factors.
Most participants in the interviews undertaken for this research had experience of isolation and of feeling lonely. For some, these feelings were constant features of their everyday existence. Measured levels of loneliness were higher than those reported by the UK Government for the general population and for people with disabilities. The mean score across the sample on the UCLA-3 questionnaire was 6.8 among the interview participants and 6.3 in the survey responses, both of which lie in the range assessed as “lonely.” Forty-four percent of interview participants and 22% of survey respondents scored 8 or 9 on this measure, indicating that they experience a severe and enduring level of loneliness in comparison to 8% of the population of England as a whole (UK Department of Culture, Media & Sport, 2023). Similarly, on the direct loneliness question, 44% reported feeling lonely most or all of the time, compared to 6% for the population as a whole and 13% of people living with a disability or long-term health condition (UK Department of Culture, Media & Sport, 2023). Figure 1 compares responses to the direct loneliness question across these populations.
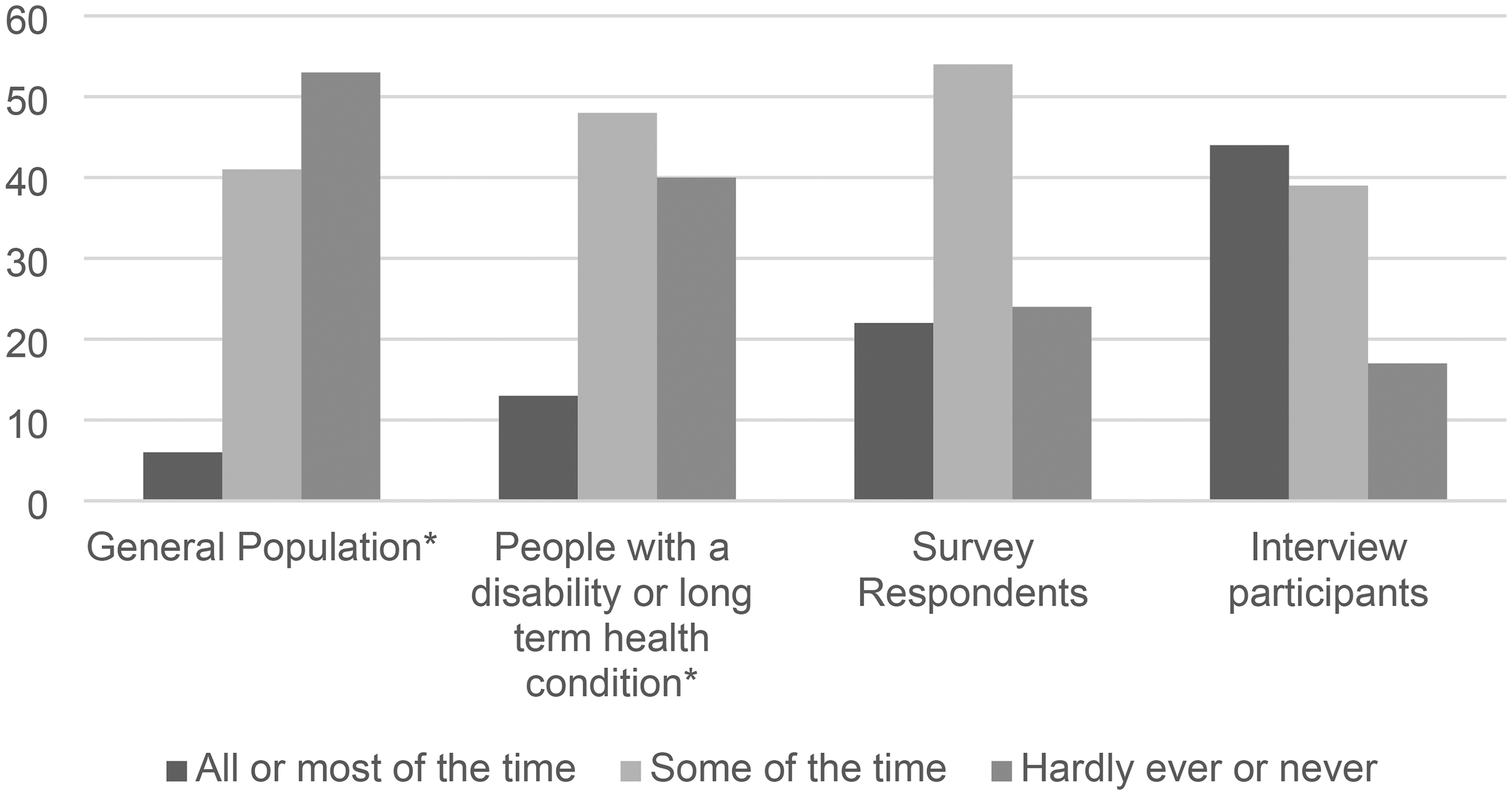
Direct Loneliness Question.
Participants highlighted the effect of visual impairments on relationships and spoke of disruptions to friendships, familial, and romantic or partner relationships that were distressing and painful, leading to feelings of rejection, isolation, and loneliness. Participants also highlighted difficulties in being able to make new connections through being excluded by the actions and attitudes of others, either through ignorance or deliberate discrimination.
Almost all of the participants said they regularly felt anxious about interacting with others or taking part in activities that required them to leave their homes. Often these feelings appeared to be a reaction to negative experiences. For some participants, their chosen coping mechanism for dealing with anxiety was simply not to engage with opportunities. Although effective at managing anxiety in the immediate term, this strategy also has the effect of reducing contact and connection, furthering isolation, and potentially fueling loneliness, which is then associated with experiences of depression. Furthermore, depression is related to anxiety (Kalin, 2020), social withdrawal and avoidance (Fabry, 2019; Ratcliffe, 2015), loneliness (Kraav et al., 2021), and isolation (Ratcliffe, 2015). Although the possibility exists that there is a causal relationship between these factors, there is also potential for each of these effects to interact with each other and a form of cyclical process to become established, which leads to severe, long-term isolation and loneliness, along with the related effects it has on physical and mental health. These potential interactions are illustrated in the model of Figure 2.
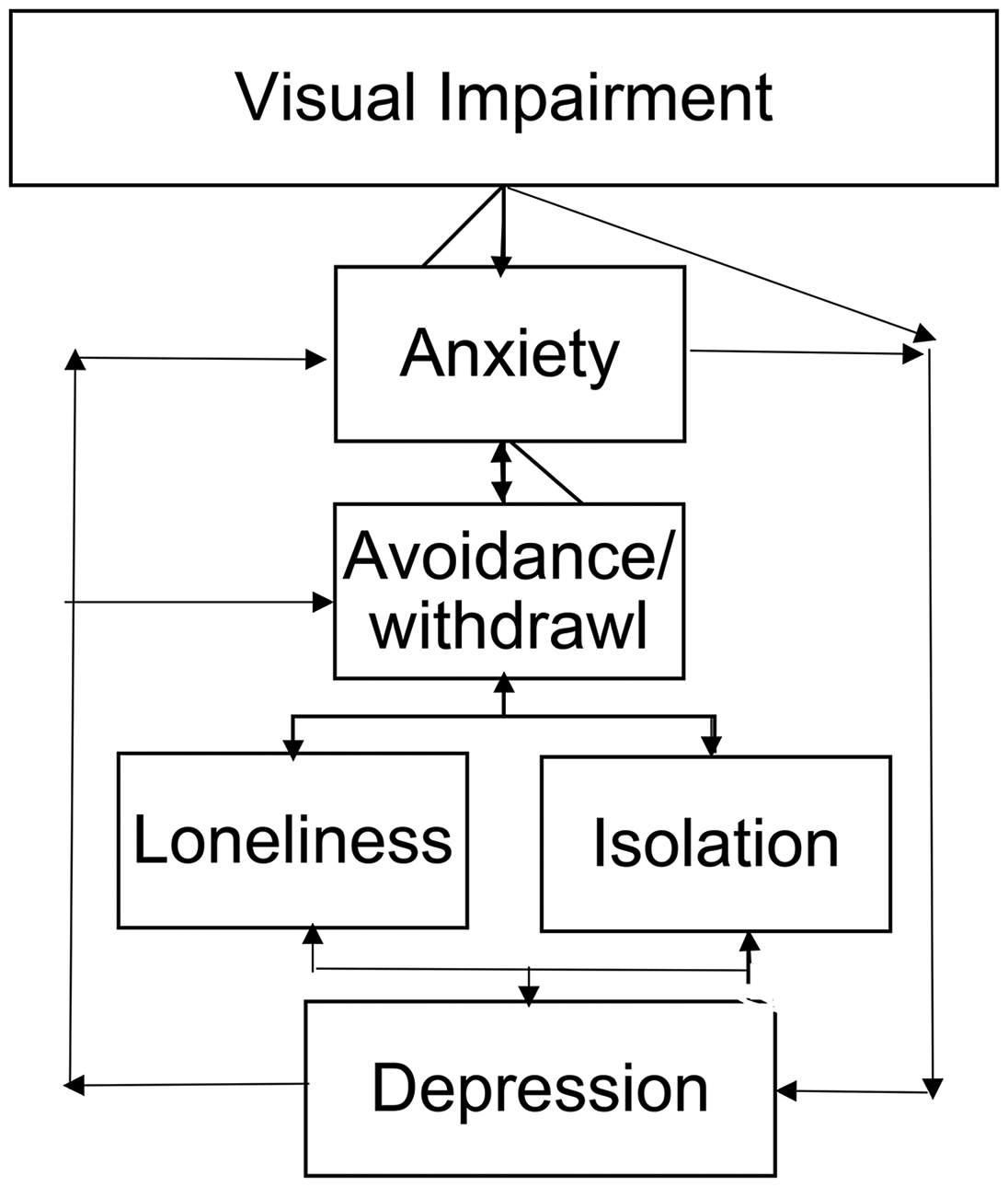
Influence of Anxiety.
Binder et al. (2020) described relationships of an association between visual impairment and anxiety. Munster et al. (2021) reported that although there is little empirical information on that relationship, in comparison to visual impairment and depression, the evidence points to symptoms of anxiety being more common among people with visual impairments than those with depression. Further research would be useful to explore this relationship. Although it is becoming clear that an association exists, the nature of it is less clear. For example, the extent to which experiences of anxiety are a natural emotional reaction to stress invoking stimuli or a reflection of a diagnosable mental health condition. Exploring these areas could inform the types of support or interventions that might assist people with visual impairments in being able to manage symptoms of anxiety.
Most participants were able to identify things that helped them deal with or overcome feelings of loneliness or isolation or both. However, there were common obstacles in accessing these things. People with visual impairments are not a homogenous group, and the things that provide meaning and purpose reflect individual interests, passions, and priorities. However, obstacles to participation were commonly reported as inaccessible venues and transport, as well as attitudes and treatment from other people.
Several participants mentioned that counseling had been useful to them in their being able to adapt to vision loss. Those diagnosed with visual impairments also described that, at the point of diagnosis, their emotional or psychological needs were overlooked, which was described as being isolating in itself. Several interviewees expressed that counseling or emotional support should routinely be made available to people at the point they are diagnosed with a visual impairment.
Limitations
This research specifically sought to explore the experiences of people with visual impairments in relation to loneliness and isolation, and it is likely that the individuals who volunteered to take part did so because these issues were important to them based on their lived experiences. For this reason, the high levels of loneliness that were found among the participants may not be reflective of the wider population of people living with visual impairments.
The wide range of ages represented among the interviewees was a deliberate attempt to uncover whether there were specific factors related to age that affected experiences of loneliness and isolation. We had anticipated being able to further explore the prevalence of loneliness at different life stages through the survey. However, there were insufficient responses, especially among younger visually impaired people, to be able to meaningfully investigate this idea. Furthermore, since the sample was relatively small and not particularly diverse, it was not possible to analyze some of the other risk factors affecting people's vulnerability to loneliness and isolation. Whether or not an individual becomes lonely or isolated is likely to be a result of several complex and interrelated factors within that individual's experiences, environments, and personal circumstances, which could not be explored in-depth within the current research context.
Conclusion
This study examined experiences of loneliness and isolation among people with visual impairments in the United Kingdom and found the prevalence of loneliness among participants was greater than in the general UK population. Furthermore, qualitative insights showed the multifaceted nature of loneliness, stemming from disruptions in relationships, social exclusion, and heightened anxiety surrounding social interactions and activities outside the home.
Loneliness, anxiety, depression, and isolation potentially influence and exacerbate each other in a cyclical fashion, and further research is needed to understand the nature of visual impairment and anxiety and to inform interventions. Systemic barriers, such as inaccessible venues and transport, compounded the challenges faced by people with visual impairments, highlighting the need for greater accessibility and attitudinal shifts in society. Addressing these barriers and providing counseling support for people with visual impairments could mitigate the detrimental effects of loneliness on physical and mental well-being. In light of these findings, there is a clear call to action for tailored support programs that prioritize emotional well-being and address the unique challenges faced by individuals with visual impairments.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Fight for Sight UK (grant number n/a).
Ethical Approval
Abertay University, School of Applied Sciences Number EMS7474.