
Abstract
This paper brings together objective and subjective data on indoor temperature and thermal comfort to examine the magnitude and perception of summertime overheating in two London-based care homes occupying modern and older buildings. Continuous monitoring of indoor and outdoor temperature, relative humidity and CO2 levels was conducted in summer 2019 along with thermal comfort surveys and semi-structured interviews with older residents and staff of the care settings. Indoor temperatures were found to be high (>30°C) with bedroom temperatures often higher at night than daytime across both care settings. Limited opening due to window restrictors constrained night-time ventilation. Overheating was prevalent with four out of the five monitored bedrooms failing all four overheating metrics investigated. While 35–42% of staff responses perceived indoor temperatures to be uncomfortably hot, only 13–19% of resident responses were found to do so, indicating that elderly residents tend to be relatively insensitive to heat, leaving them open to overheating without realising it. Residents and staff in the modern care setting were less satisfied with their thermal conditions. As hybrid buildings, care settings need to keep both residents and staff comfortable and healthy during hot weather through night-time ventilation, management of heating and supportive institutional practices.
Practical application:
Care home designs have focused on keeping residents warm through the winter, neglecting the risks of summertime overheating. Care homes are hybrid buildings serving as living spaces for vulnerable older residents and offices/workspaces for staff. Providing comfort to both groups during periods of hot weather is challenging. Opportunities for ventilation are limited by Health & Safety regulations that mandate up to 10 cm maximum window openings and institutional practices that result in windows routinely kept closed, particularly at night. Utilising natural and where possible cross-ventilation should be considered along with external shading. Heating should be managed to avoid unwanted heat gains in the summer.
Introduction
The relationship between high external temperatures and an increase in mortality has been well studied. 1 Excessive heat has been linked to heat exhaustion and heat stroke, which in turn can lead to cell, organ and brain damage and even death. 2 Heat also increases the risk of dehydration which has been linked with increased risk of bloodstream infections. 3 Indeed, Public Health England have identified the relatively low temperature of 24.5°C as the threshold above which excess heat-related deaths may become apparent, principally through cardiovascular and respiratory disease. 2 The global Covid-19 pandemic has disproportionately affected the elderly, particularly those in care homes. However, excessive heat has also been found to be more of a threat to the elderly,2,4–6 and a warming climate brings with it a longer-term public health risk. Despite care homes being known to be vulnerable settings for heat-related mortality and morbidity, research in this area is limited, both in scope and scale – some focussing on environmental monitoring, others on feedback from residents, but rarely both.
Historically care homes have been designed and built with the aim of keeping residents comfortably warm all year round, particularly during the winter months.7,8 Heating systems are typically designed to operate throughout the year. This bias towards cold management over heat management is evident in the Care Quality Commission (CQC) inspection protocol, which includes checking for low room temperatures and questioning staff on how they respond to residents who feel cold, 9 but no consideration towards high temperatures and questioning staff on how they respond to residents who feel hot. Regulations created for the safety of the residents – such as limiting window openings to a maximum 10 cm to prevent the risk of falls – can have unintended negative consequences when it comes to regulating indoor temperatures, particularly during a heatwave. Frontline carers and managers are trained to view the cold as a danger: an effective strategy during the cold winter months, but when warmer weather arrives, many residents and staff become more vulnerable. 10 Consequently, care homes managers and frontline staff are left ill-equipped to deal with high summertime temperatures.
The research in this paper builds upon the Joseph Rowntree Foundation (JRF) study by the authors, 10 and for the first time, adds thermal comfort surveys and interviews of both elderly residents and staff (frontline carers, nursing staff and managers). Prevalence of overheating is empirically assessed alongside the perception of the environmental conditions by those who live and work in care settings in London.
The paper brings together objective and subjective data on indoor temperature and thermal comfort to examine the magnitude and perception of summertime overheating in two London-based care homes occupying modern and older buildings. Continuous monitoring of indoor and outdoor temperature, relative humidity and CO2 levels was conducted in summer 2019 to establish the magnitude and duration of overheating. To assess the human perception of overheating, thermal comfort surveys and semi-structured interviews were conducted with the elderly residents and staff of the two care settings. Insights were drawn by cross relating the findings from the analysis of monitoring, survey and interview data.
Evidence to date
The 21st century has seen an increase in national and international heatwave events, 11 leading to a growing body of evidence that identifies a relationship between high temperatures and an increase in mortality and morbidity. The European-wide heatwave of 2003 resulted in an estimated 70,000 excess deaths when compared with rates from 1998–2002, 12 with older age groups seeing the greatest increase. During this heatwave, 92% of deaths in Italy occurred among the 75+ age group – an increase of 21%, 5 and in Parisian nursing homes there was a greater increase in mortality amongst the less frail residents compared to those more frail, suggesting medical care was directed towards the more frail to the detriment of the less frail. 13 The 2003 heatwave in London increased mortality by an estimated 17% compared to the average for the previous 5 years, with the elderly being most affected. 14 Over 2000 deaths were attributed to this heatwave in England and Wales, with a 33% increase in mortality for those aged 75 and over compared to a <14% increase in the under-75’s. Excess deaths amongst the over-75’s were much greater in nursing homes compared with those living at home: 42% compared to 33% respectively. 15 In response to these heatwaves, public authorities have developed plans to better anticipate and coordinate the response to future heatwave events, 4 including improving the performance of buildings and installing sustainable air-cooling systems.
The correlation between air temperature and mortality has been found to be as high as R = 0.95 16 with one study suggesting that in London the death rate increased by 3% for every 1°C increase in daily average temperature over 21.5°C 17 – a relatively low threshold for mortality to increase. Elderly people, especially those in nursing and care homes have been found to be most vulnerable to heat mortality. 18 Indeed, heat-related mortality in the UK has been projected to rise by over 250% by the 2050’s compared to a 2014 baseline of 2000 deaths, with the elderly contributing to this most significantly. 19
In addition to high daily average temperatures, high night-time temperatures have been linked to increases in mortality, particularly amongst the elderly. Respiratory mortality rates have been found to be more sensitive to high daytime temperatures, whereas stroke-related mortality has been linked to night time exposure to high temperatures 20 : Hot days followed by hot nights had a greater mortality risk than hot days followed by cool nights. A study of sub-tropical Hong Kong mortality found the strongest association with mortality when two consecutive hot days were framed by three hot nights. 21
In light of this established link between high temperatures and increased mortality – particularly amongst the elderly, studies have focussed their attention on thermal comfort and heat vulnerability amongst care home residents. Indoor overheating in care homes has been attributed to an interaction between occupants' susceptibility to heat, their behaviour and the building's location and characteristics, 22 with the interrelation of these factors expected to vary over time with demographic and climate changes. Very few studies have used interviews with care home residents to determine how they perceive their local indoor environment. One study’s resident interviews revealed that they did not perceive themselves to be particularly vulnerable to heat, believing simple, “common sense” actions were sufficient response during heatwaves. 23 In studies which included staff interviews, some recurring themes appear, notably that staff, particularly those with more physical frontline care roles, often found their buildings too warm – thermally uncomfortable.24–26 Thermal preference temperatures in the elderly have been found to be generally warmer than those in younger adults. 27 The thermal environment was cited as an important factor in determining what spaces residents would occupy – moving to different lounges or dining rooms, or even different parts of these communal spaces. 28
Thermal comfort considerations were found to have a strong bias towards keeping residents comfortably warm in winter rather than comfortably cool in summer,7,8,29 with frontline carers often ill-equipped to manage heat effectively in the summer. 30 Some frontline staff identified care home design being a hindrance to keeping the indoor environment cool. 7 Interviews with care home designers revealed an emphasis on designing to protect residents from the threat of cold, and consequently a lack of effective heat management. 31
Against this backdrop, the UK Government’s 2017 Climate Change Risk Assessment report 32 and the 2018 National Adaptation Programme 33 identified summertime overheating in care settings as a key risk and research priority for the health and social care system. The 2016 JRF report ‘Care provision fit for a future climate’ 10 assessed the risk of summertime overheating using environmental monitoring and modelling with no thermal comfort surveys of residents or staff undertaken. The study found that the priority in both the design and running of homes was in preventing risks associated with under-heating rather than overheating. The perception that older people ‘feel the cold’ was prevalent, but much less was understood about the risks associated with heat. A study by Hughes and Natarajan 34 found thermal comfort models PMV/PPD ISO 7730 and the adaptive ISO 15,251 did not match the occupant responses, with occupants feeling comfortable at temperatures where the models predicted they should feel warm/hot. These studies have reinforced the need to holistically examine the prevalence (magnitude and duration) as well human perception of summertime overheating in care settings using empirical data on thermal environment and cross-related with thermal comfort surveys and thermal experiences of the elderly residents and staff.
Methodology and case studies
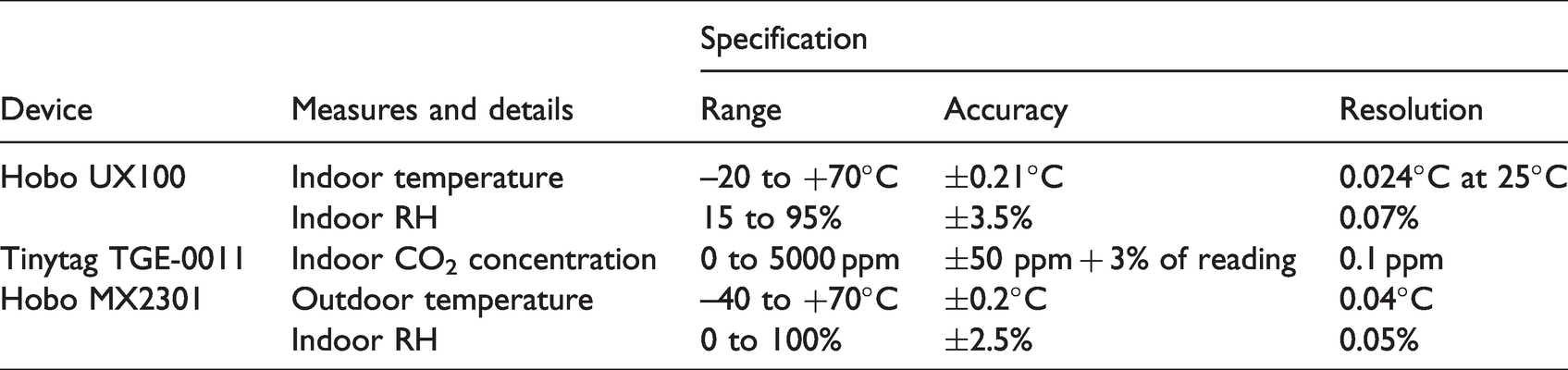
The research methodology for the study was socio-technical combining continuous monitoring of indoor environment (providing objective data) with thermal comfort surveys and interviews (providing subjective data). As part of indoor environmental monitoring, air temperature, RH and CO2 concentration were recorded using Hobo UX100 and Tinytag TGE-0011 data loggers. Outdoor temperature and RH were recorded using MX2301data loggers (Table 1).
Specification, accuracy and resolution of logging devices.
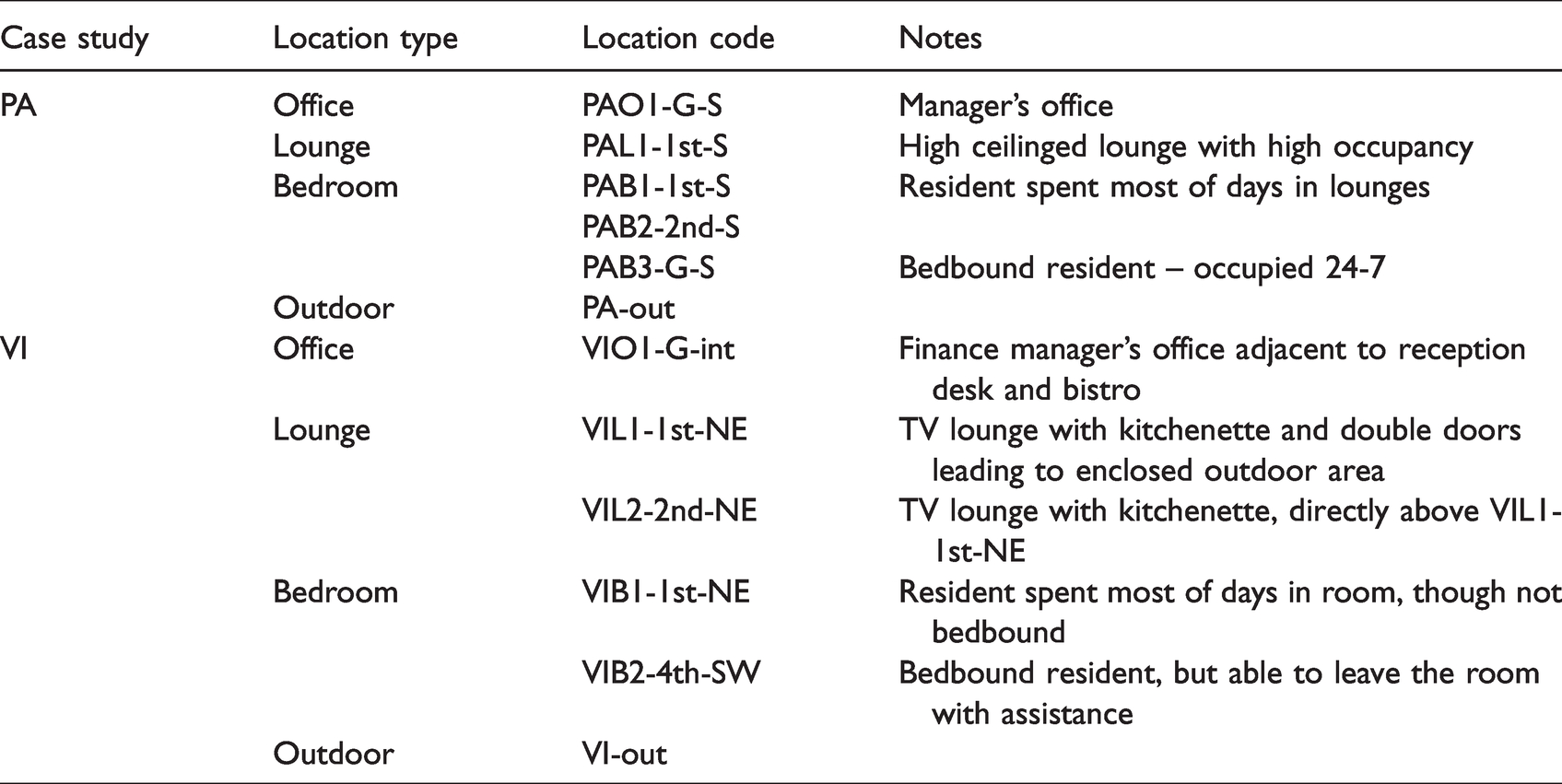
Data was recorded at 5-minute resolution from 17-06-2019 to 31-08-2019 in a range of locations within the care homes (Table 2). The nomenclature for locations in each home consists of care home i.d. (PA or VI) followed by room type (O=office, L=lounge, B=bedroom) and number, followed by floor (G, 1st, etc.) and orientation (N, S, E, W, int=internal).
Locations of data loggers.
Occupied hours were defined as 09:00-18:00 (offices) and 08:00-21:00 (lounges). Bedroom occupancy was more varied - some occupied only at night for sleeping, others occupied day and night, either through necessity or resident choice. Bedrooms were therefore differentiated by day (07:00-21:00), when occupants were more likely to be awake and conscious of their immediate environmental conditions, and night (21:00-07:00), when occupants were more likely to be asleep.
Care homes are hybrid buildings, with some rooms being non-domestic (e.g. offices), some domestic (e.g. bedrooms), and some both domestic and non-domestic – occupied by both residents and staff (e.g. corridors, dining rooms and lounges). Therefore, both static and dynamic (adaptive) overheating metrics were used to assess the prevalence of overheating in terms of magnitude and duration within the two case study buildings. Four overheating metrics considered to be relevant for care setting were used in the analysis (Table 3).
Metrics considered for overheating.
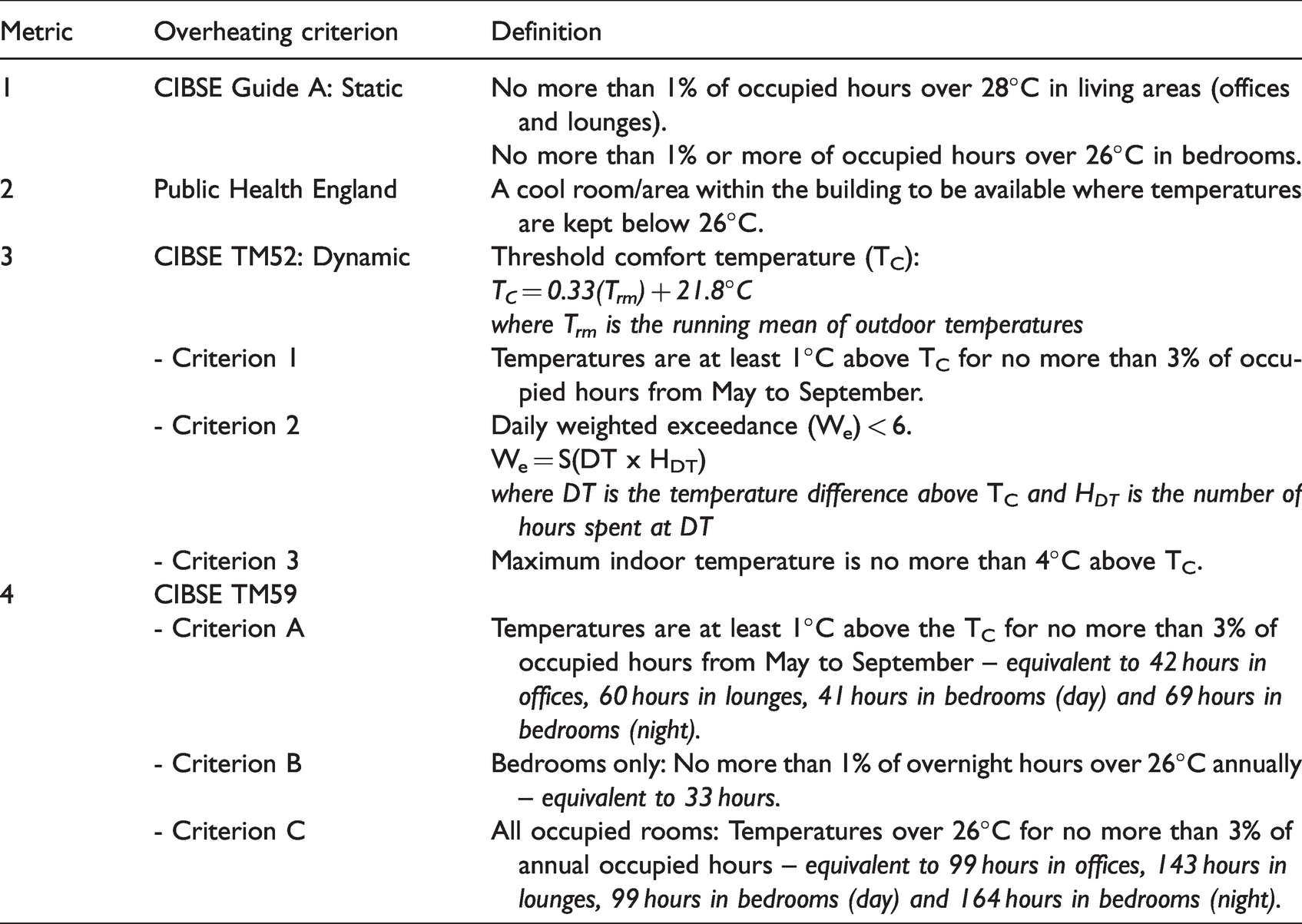
Two of four the overheating metrics used static temperature thresholds to define whether a space was overheating: CIBSE Guide A and Public Health England (PHE). 2 These two metrics provided simple measures of overheating, but did not account for occupants’ ability to adapt to their environment – including external temperatures. Therefore, adaptive overheating metrics were also investigated. CIBSE TM52, developed by Humphreys and Nicol, 35 is applicable to free-running buildings such as the two case study care homes. This method, developed from research into non-domestic buildings, requires more research to determine how best to apply it to hybrid buildings such as care homes since elderly residents’ ability to adapt to their local environment may be more limited. This metric derives threshold comfort temperature (TC) from outdoor temperature, but with the vast majority of residents spending the vast majority of their time indoors – even throughout the summer – outdoor temperatures may have less influence on the comfort temperatures of residents than on the staff who come and go from the building much more often. Nevertheless, the adaptive criteria formed the third metric in the study with overheating deemed to have occurred if at least two out of the three criteria were met (Table 3).
The fourth overheating metric, CIBSE TM59, used a combination of dynamic and static criteria: Criterion A was dynamic, based on CIBSE TM52 Criterion 1; criteria B and C were static. Criterion C considered Type I occupancy (sedentary residents) and mechanical ventilation. Although the case study care homes were not mechanically ventilated, they did have restricted window openings, and therefore Criterion C was considered. Overheating was deemed to have occurred if any one of these three criteria were failed. TM59 was intended for modelled simulations using annual data rather than measured data from the limited period presented here. Therefore, the percentage thresholds for annual occupied hours have been converted to total hours thresholds for this analysis, which provides indicative rather than definitive results for TM59.
To measure perception of overheating amongst residents and staff, thermal comfort surveys and interviews were conducted. Surveys were conducted up to three times a day on multiple days throughout the summer period, with a focus on days when outdoor temperatures were at their warmest. No individual contributed to a survey more than once during each round, but may have contributed more than once on the same day – e.g. in the morning and afternoon. The surveys collected asked respondents to rate their thermal sensation and thermal preference, and also gathered contextual information (date, time, location, gender, role, clothing, activity during previous 15 minutes). Hand-held monitoring devices (Extec HT200 and ATP Hotwire Anemometer) recorded concurrent indoor environmental conditions which were cross-related with survey responses. Interviews were conducted during September 2019, and asked interviewees to reflect on the summer of 2019: their perceptions of temperatures, responses to high temperatures (for themselves and/or for those they cared for), and care home policies relating to overheating. Interviewees were classified as either managers (one from PA, two from VI), frontline staff (six from PA, seven from VI) or residents (three from PA, seven from VI). Since the majority of residents in both homes had Alzheimer’s and other dementia-related conditions, many lacked the cognitive or communicative ability to respond to the survey and interview questions meaningfully. Resident contributors were therefore selected under advisement from care home staff.
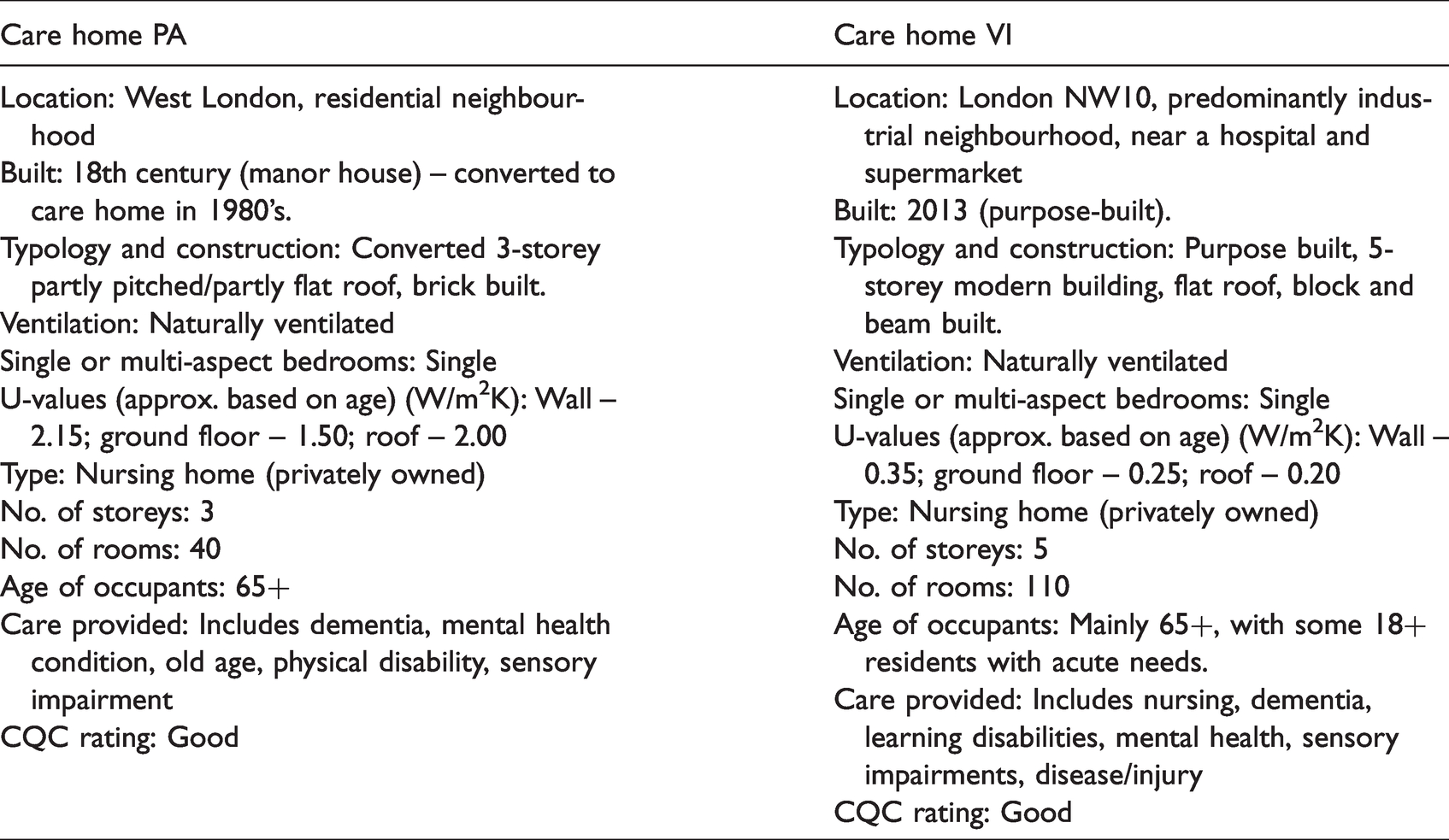
The two care homes, located in central and west London, had several similar characteristics but some contrasting characteristics, particularly in terms of age and size (Table 4). Case study PA was originally a Georgian manor house, a heavyweight stone and brick building constructed in the mid-18th century, with additional rooms added in the 1920’s and was converted to a care home in the 1980’s. Key physical features included high ceilings on the ground and first floors, with tall sash windows and internal shutters in the lounges. Bedroom windows were much smaller and had curtains for shading. Case study VI was a medium-weight steel and concrete building, custom-built in 2013. There was no external shading, with curtains used for shading.
Key characteristics of case study care homes.
Findings
Thermal environment
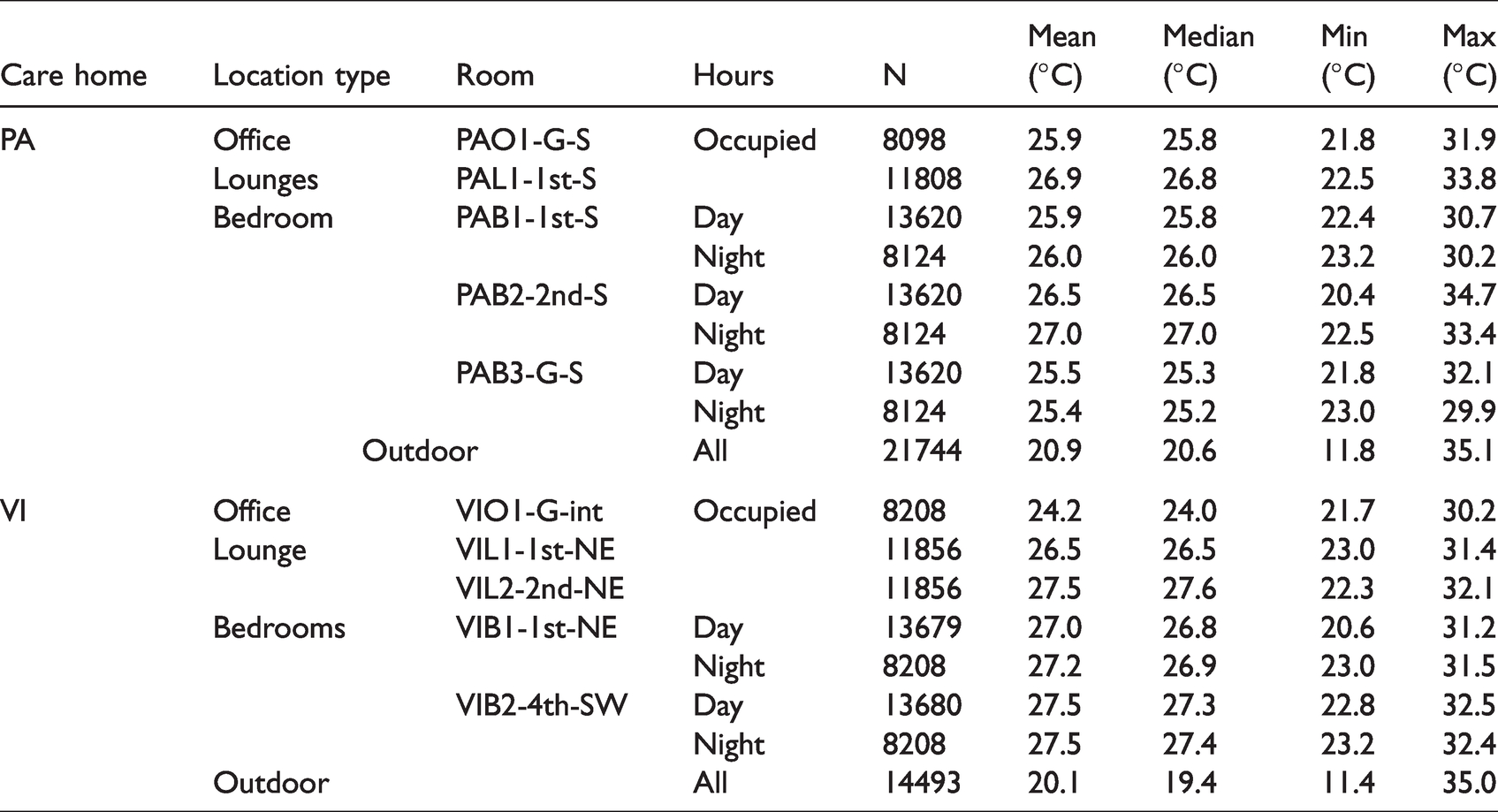
Monitored outdoor operative temperatures were found to be as high as 35°C at both sites during the hottest days of the summer (Table 5). In PA, indoor temperatures reached as high as 34.7°C in bedroom PAB2-2nd-S and 33.8°C in lounge PAL1-1st-S. In VI, indoor temperatures reached as high as 32.5°C in bedroom VIB2-4th-SW and 32.1°C in lounge VIL2-2nd-NE. In both care homes, temperatures remained in the 24–28°C range for the majority of the time, and did not fall below 20°C in any of the monitored spaces for the whole of the monitored period, even overnight. Of particular interest was the fact that temperatures in the bedroom remained high overnight: Although maximum temperatures tended to be slightly lower overnight than during the day, in four of the five monitored bedrooms, median temperatures were slightly higher overnight.
Descriptive temperature statistics for monitored location in PA and VI.
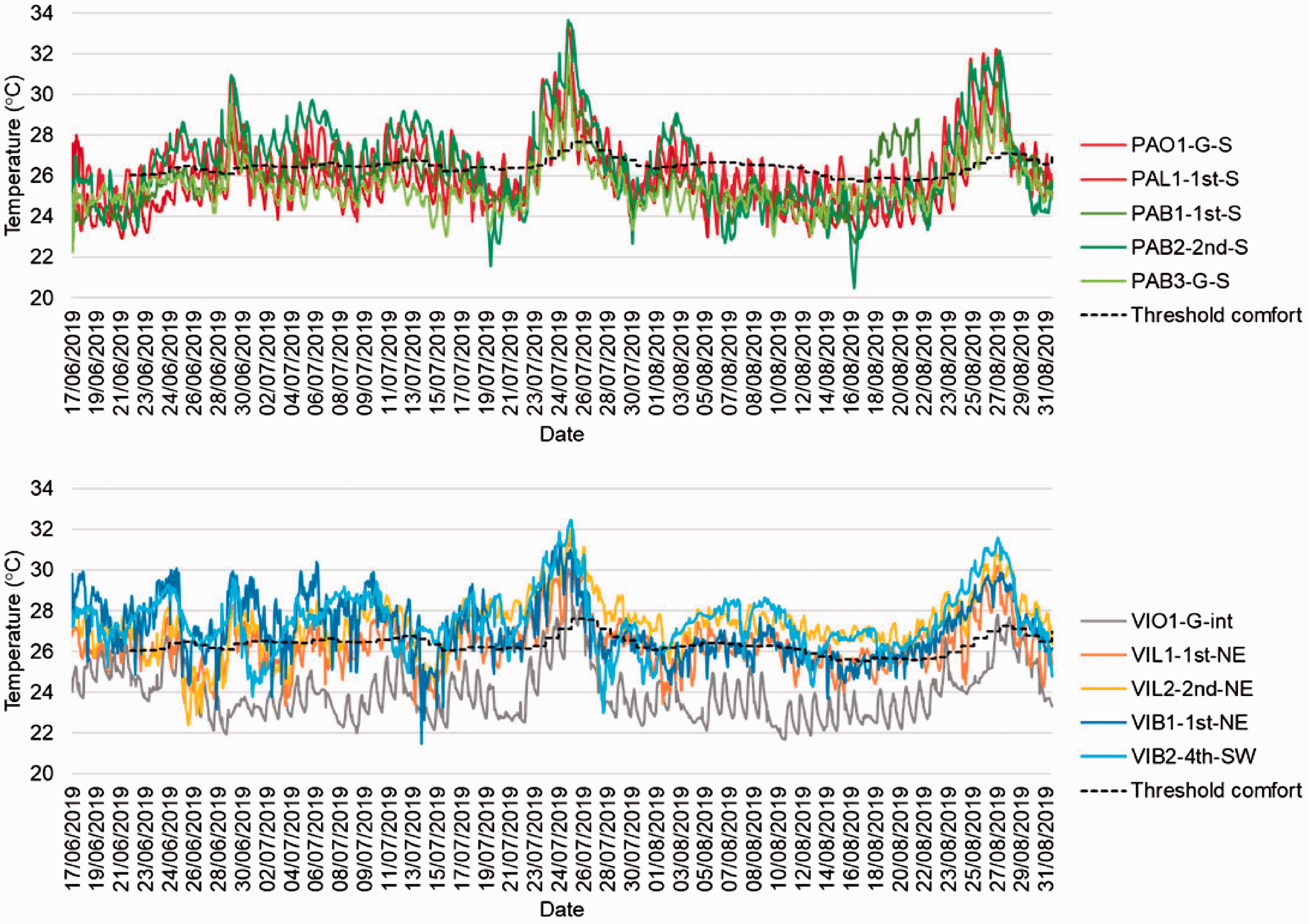
Taking the daily average temperatures during occupied hours (offices and lounges) and all hours (bedrooms) masks the peak temperatures that were reached in the monitored locations, but clearly shows temperatures remaining consistently high – in the 24–28°C range for the majority of the monitored period (Figure 1). It is also clear from these graphs how much warmer the indoor temperatures were compared to outdoor temperatures.
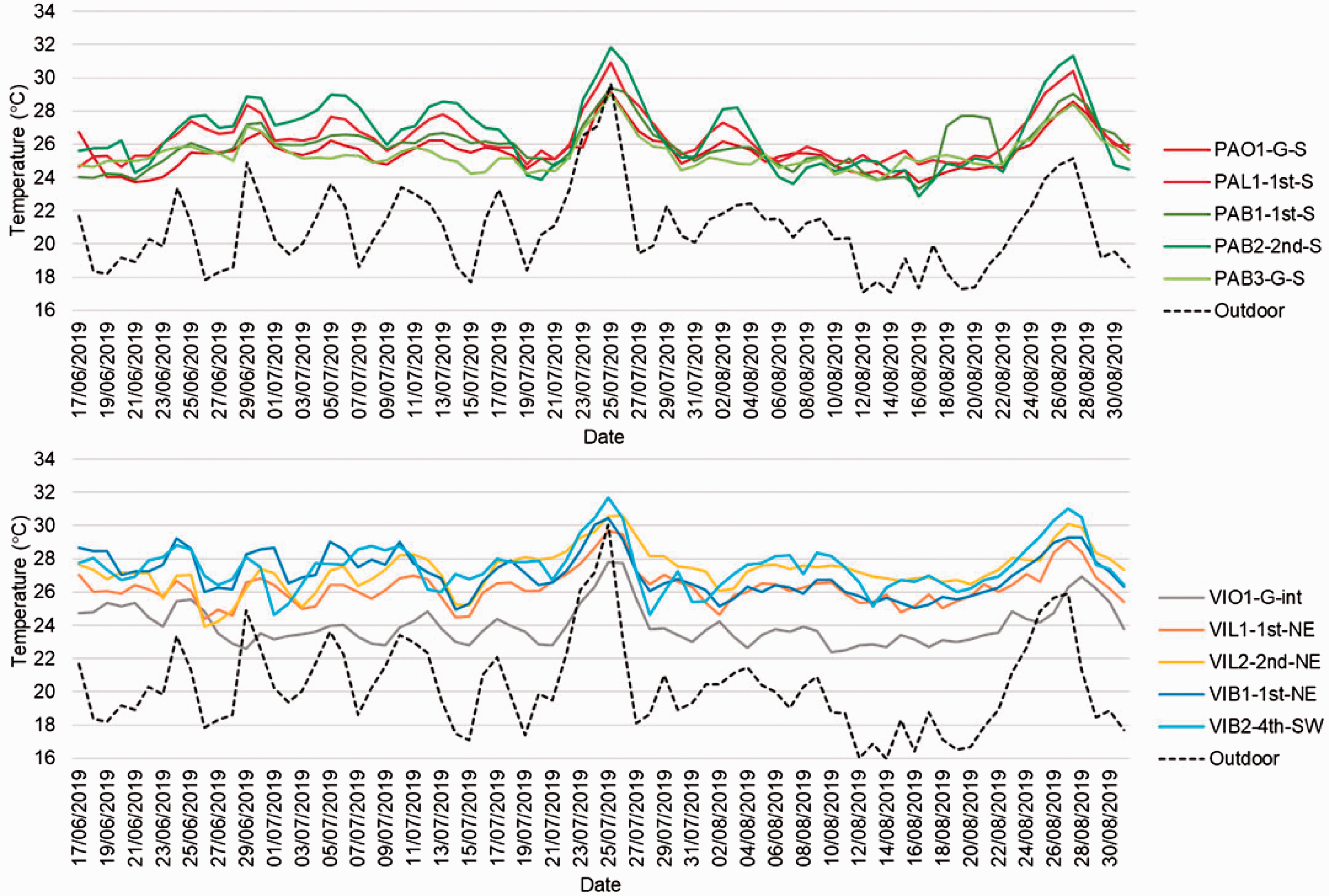
Daily average temperatures for case studies PA (top) and VI (bottom).
Boxplots showing the distribution of temperatures in monitored locations in both care homes illustrate the significant differences between locations (Figure 2). In PA, bedroom PAB3-G-S had a much narrower IQR, both day and night, than the monitored first and second floor bedrooms. Second floor bedroom PAB2-2nd-S had the widest IQR and reached the highest and lowest temperatures of any monitored location. In VI, office VIO1-G-int was significantly less hot than monitored locations on the higher floors. First floor lounge VIL1-1st-NE had a lower IQR than lounge VIL2-2nd-NE directly above it, the lower lounge benefitting from two pairs of doors which opened out onto an enclosed outdoor space. Although whiskers – the extremes of temperature – were generally shorter in VI than in PA, median temperatures were generally higher.
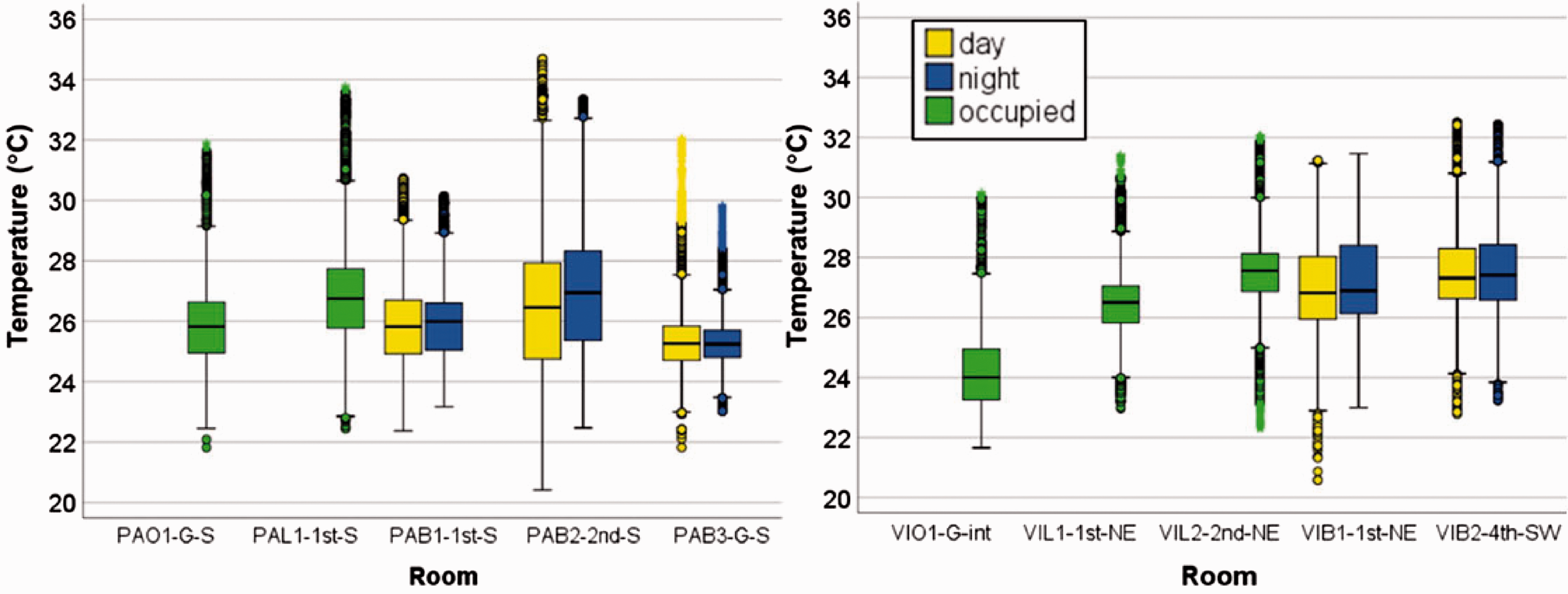
Boxplot showing distribution of temperatures in monitored PA (left) and VI (right) locations.
Temperature monitoring revealed sustained high temperatures throughout both care homes. Augmenting this dataset, monitored RH and CO2 concentration provided valuable contextual data, giving a deeper understanding of the indoor environmental conditions.
Indoor relative humidity and CO2 concentration
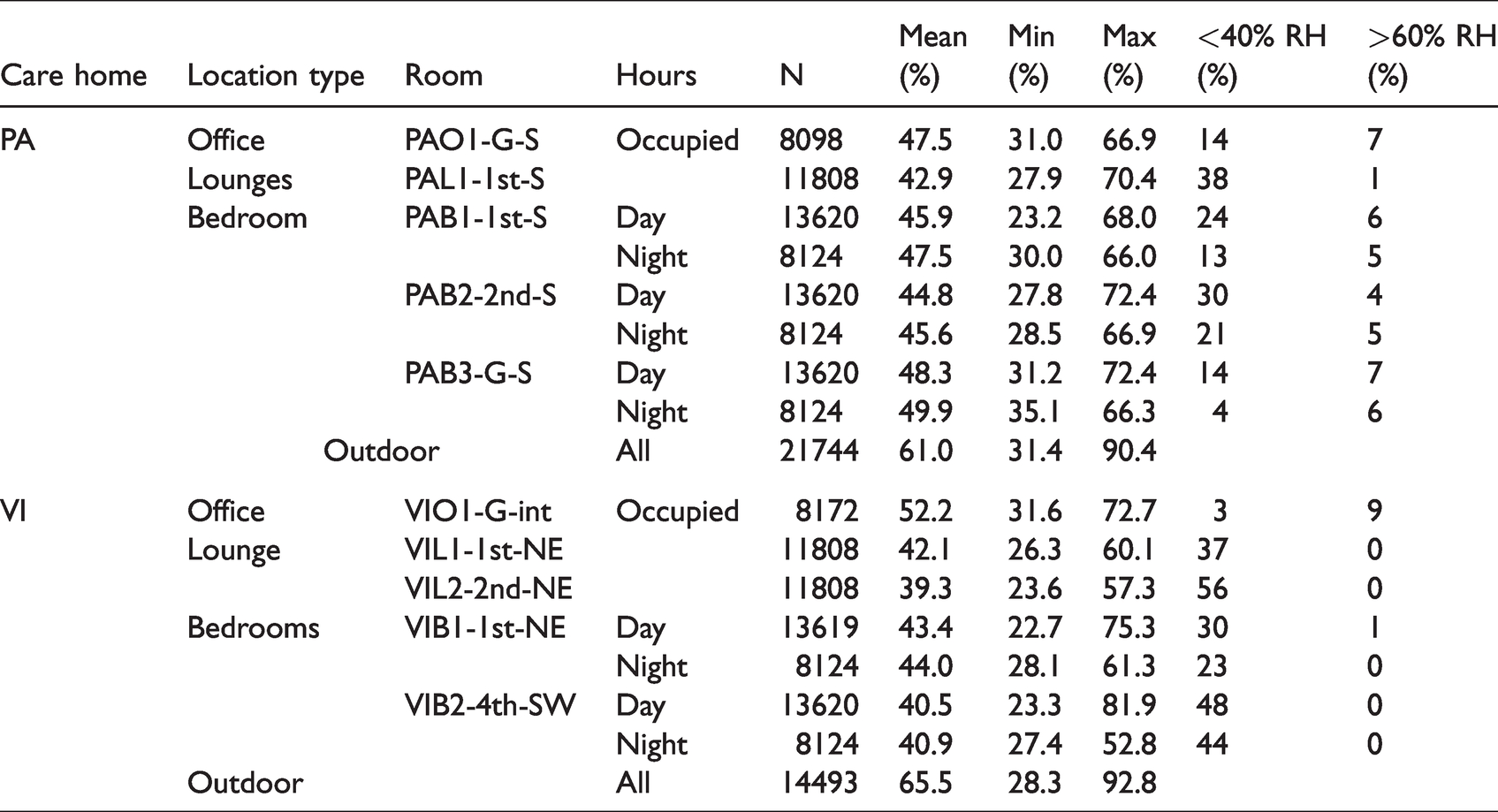
Mean RH was found to be in the 42–50% range in monitored PA locations, and in the 39–52% range in monitored VI locations (Table 6). Ideally, RH should be within the 40–60% range, particularly during occupied hours. In VI, levels rarely exceeded 60%, with the internal office VIO1-G-int being the most likely monitored location by far to have RH above 60%. In PA, RH exceeded 60% in all locations, but never more than 7% of occupied/day/night hours. However, RH below 40% was far more common in both care homes. RH below 40% was observed for more than half of occupied hours in lounge VIL2-2nd-NE, and more than a third of occupied hours in lounges VIL1-1st-NE and PAL1-1st-S. Monitored bedrooms also experienced low RH, with levels more likely to be below 40% during daytime hours than night time hours.
Descriptive RH statistics for monitored location in PA and VI.
Monitored CO2 concentration revealed some interesting trends, similar in both care homes. Both offices saw levels rise and fall in line with occupied hours, with the internal office VIO1-G-int having a steeper rise (and fall) due to the limited ventilation – two internal doors which generally remained closed (Figure 3). Interestingly, PAO1-G-S’s overnight CO2 concentration remained around 550 ppm, possibly due to the windows and door being closed for security reasons outside of occupied hours. Lounge PAL1-1st-S had mean CO2 concentration of 1027 ppm during occupied hours, when it regularly had around twelve occupants. Overnight, levels fell but still averaged above 900 ppm, indicating windows, and possibly the internal door, were closed overnight. In contrast to this, lounge VIL1-1st-NE had CO2 concentrations averaging below 500 ppm throughout the day. This lounge had advantages over PAL1-1st-S by being larger – and therefore lower density of occupants – and having two pairs of external doors and windows which remained open for much of the day, allowing a much greater level of ventilation. Diurnal CO2 profiles for the bedrooms revealed daytime averages of 500–700 ppm in PA and 400–500 ppm in VI, indicating that the rooms were either vacated and/or windows were opened. However, in the evenings, CO2 concentrations rose significantly in four of the five bedrooms (VIB2-4th-SW being the exception), and remained high overnight. This strongly suggested that windows in the bedrooms were closed overnight, despite high temperatures both indoors and outdoors, severely limiting the opportunities for nocturnal purging of heat.
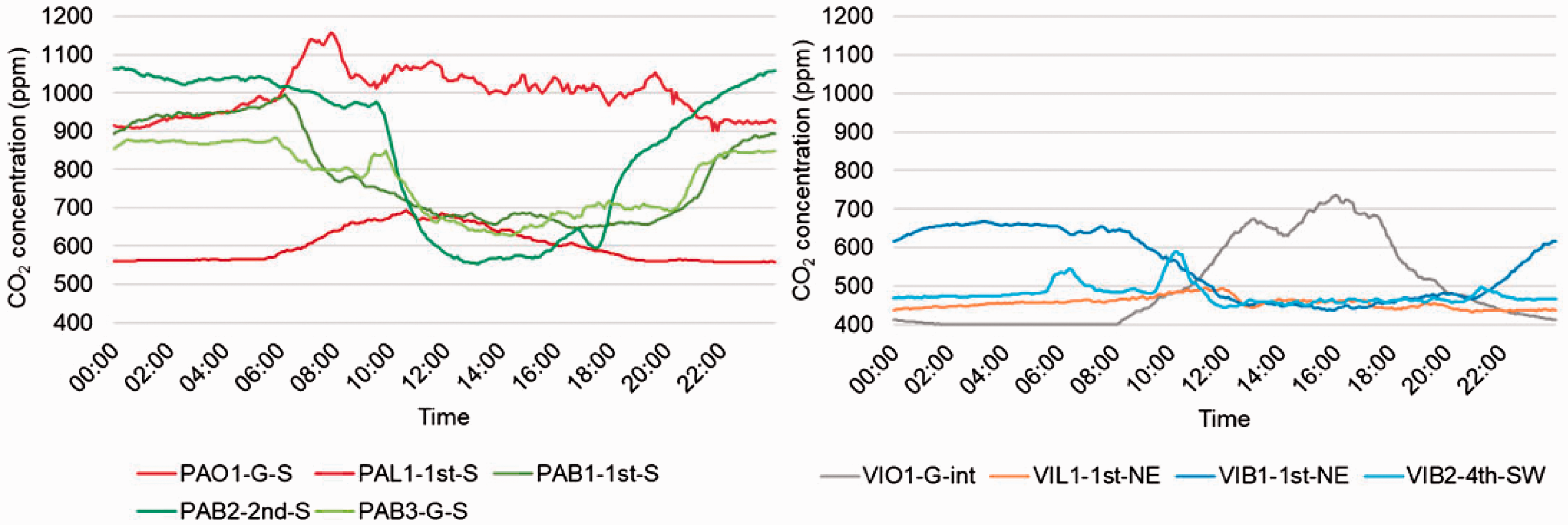
Diurnal CO2 concentration profiles in PA (left) and VI (right).
In summary, the indoor environmental monitoring revealed that the two care homes had RH which was often below the recommended 40%, and CO2 concentrations which indicated a lack of nigh-time ventilation. Indoor temperatures were found to be high during occupied hours – and often higher in the bedrooms at night than day-time. How these temperature datasets faired against the various overheating metrics was then investigated.
Overheating assessment: magnitude and duration
Each of the four overheating metrics were assessed against the monitoring data on outdoor and indoor temperatures in different spaces of the care settings. Plotting office and lounge temperatures over the monitored period alongside CIBSE Guide A’s static overheating threshold of 28°C revealed two significant periods when the threshold temperature was exceeded (Figure 4, top). These periods – 21st-29th July and 23rd–29th August 2019 – corresponded to periods of sustained high outdoor temperatures. Bedroom temperatures also had peaks during these same two periods but exceeded the 26°C threshold much more regularly and consistently throughout the whole monitored period (Figure 4, bottom). Indeed, it is clear from this graph that even 28°C was exceeded much more often in the bedrooms than in the offices and lounges.
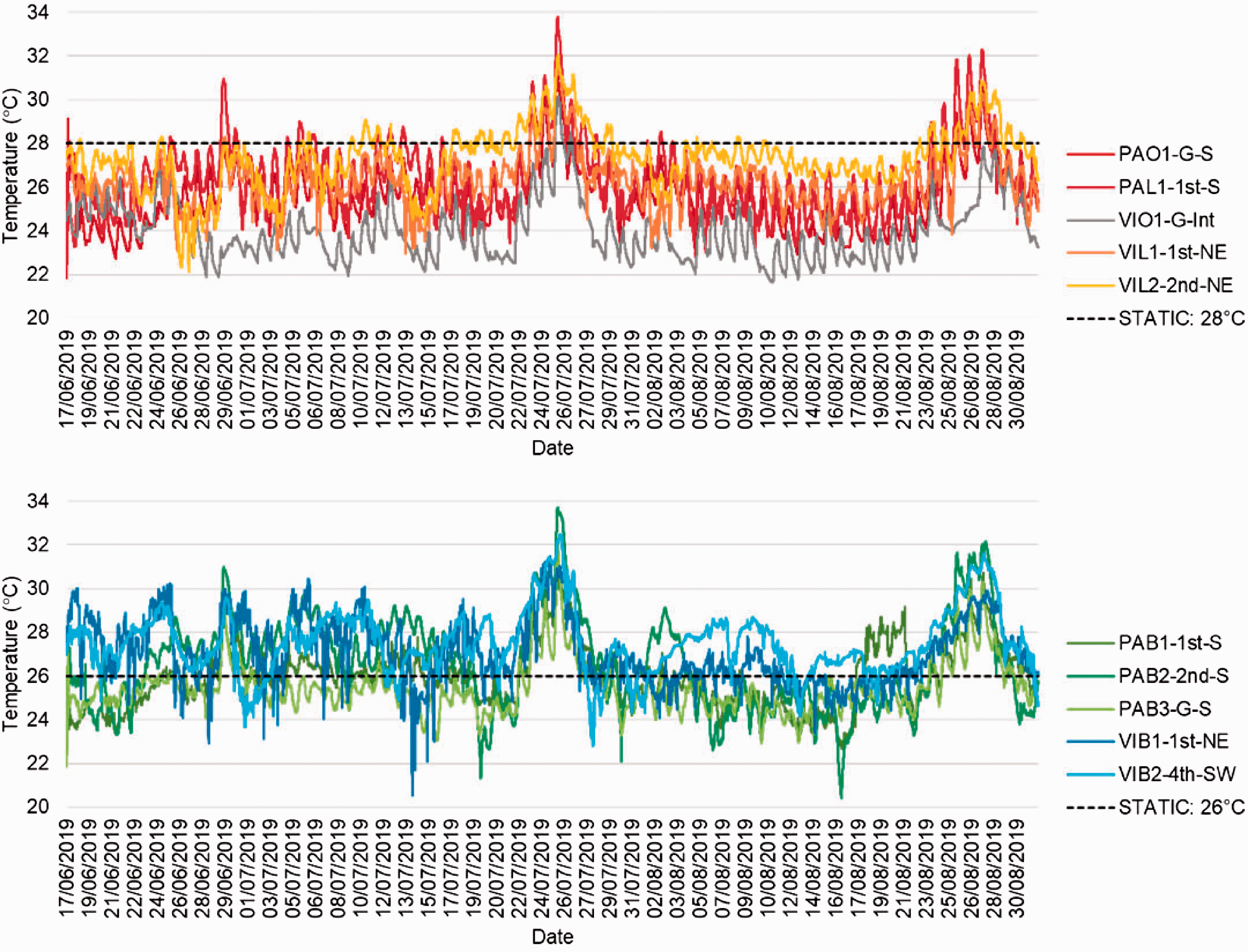
Temperatures (5-minute resolution) in monitored offices and lounges (top) and bedrooms (bottom) with static threshold temperatures shown.
Statistical analysis revealed that all of the monitored locations within both care homes exceeded the 28°C or 26°C thresholds for at least 1% of occupied hours (Table 7). Both offices exceeded 28°C for the least amount of time in their respective buildings – PAO1-G-S for 7.5% of occupied hours and VIO1-G-int for only 1.5% of occupied hours. The higher temperatures in VIL2-2nd-NE compared to VIL1-1st-NE resulted in it spending almost three times more occupied hours above 28°C.
Proportion of occupied/day/night hours exceeding CIBSE Guide A static threshold temperatures.
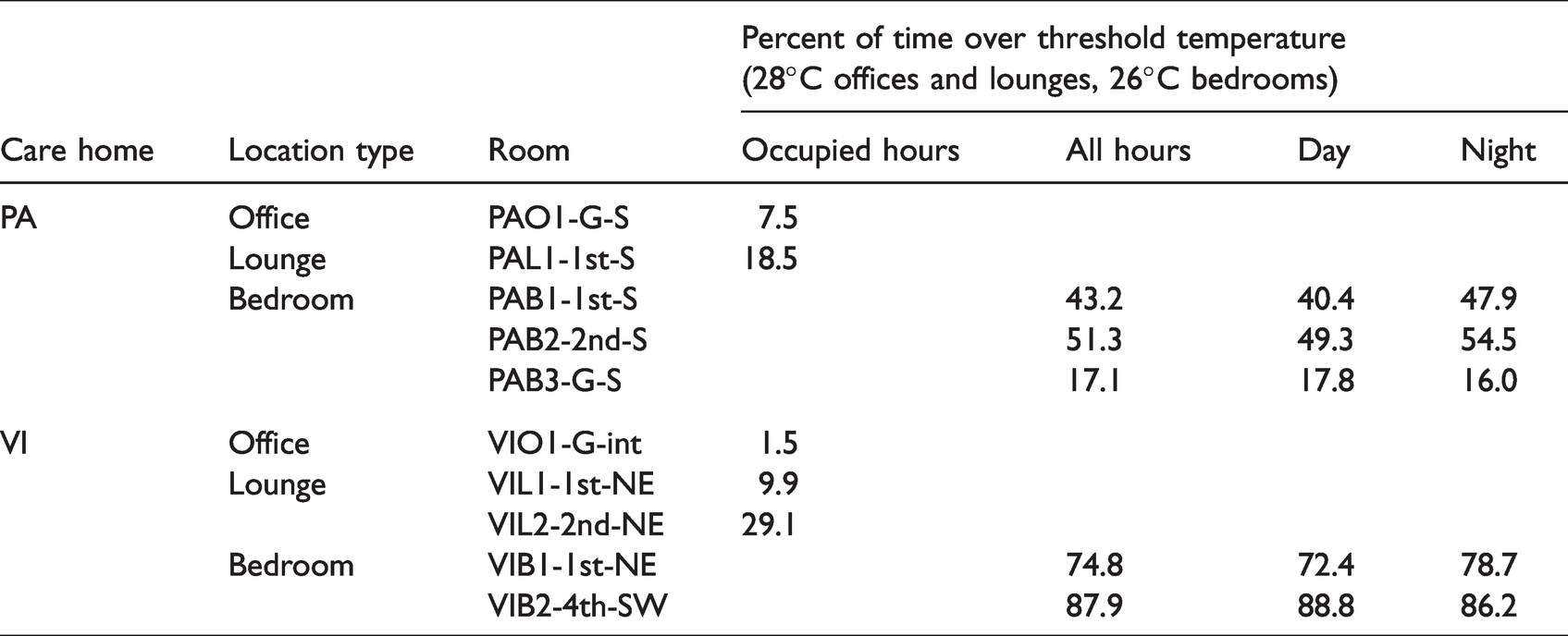
In both care homes, it was the bedrooms that failed the static threshold by the highest proportion of time, both during the day and night. Indeed, several bedrooms – PAB1-1st-S, PAB2-2nd-S and VIB1-1st-NE – had a higher proportion of nighttime hours over 26°C than they did daytime hours.
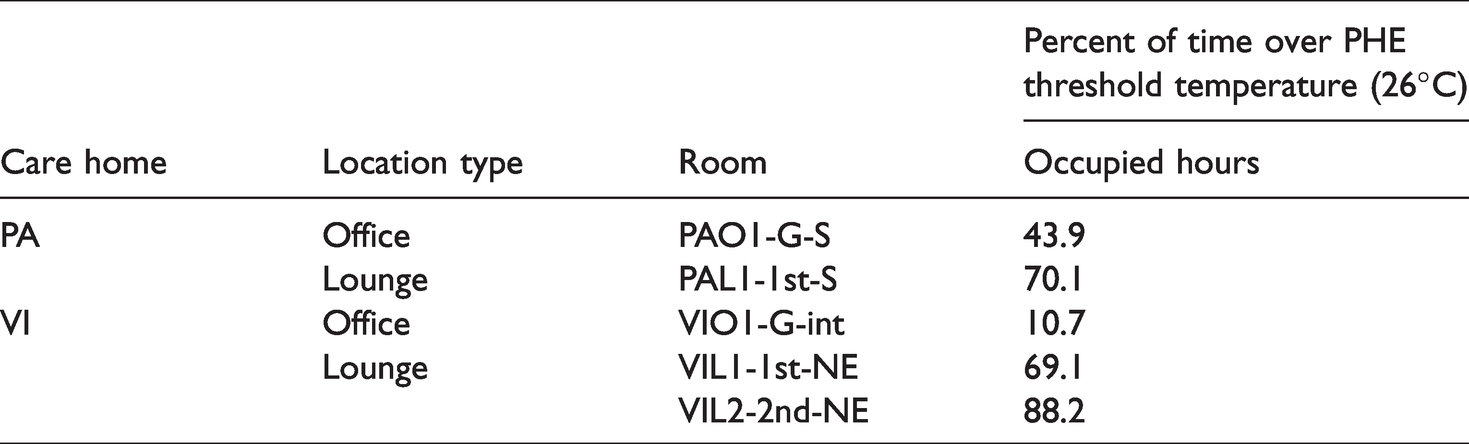
With the lower static temperature threshold of 26°C, it follows that all monitored spaces failed the PHE overheating criterion, bedrooms by the proportions detailed in Table 7, offices and lounges by those detailed in Table 8. Again, the two offices failed by the lowest proportion of occupied hours, but were still far from passing the criterion. The three monitored lounges exceeded 26°C for 69–88% of occupied hours.
Proportion of occupied hours exceeding PHE threshold temperature in offices and lounges.
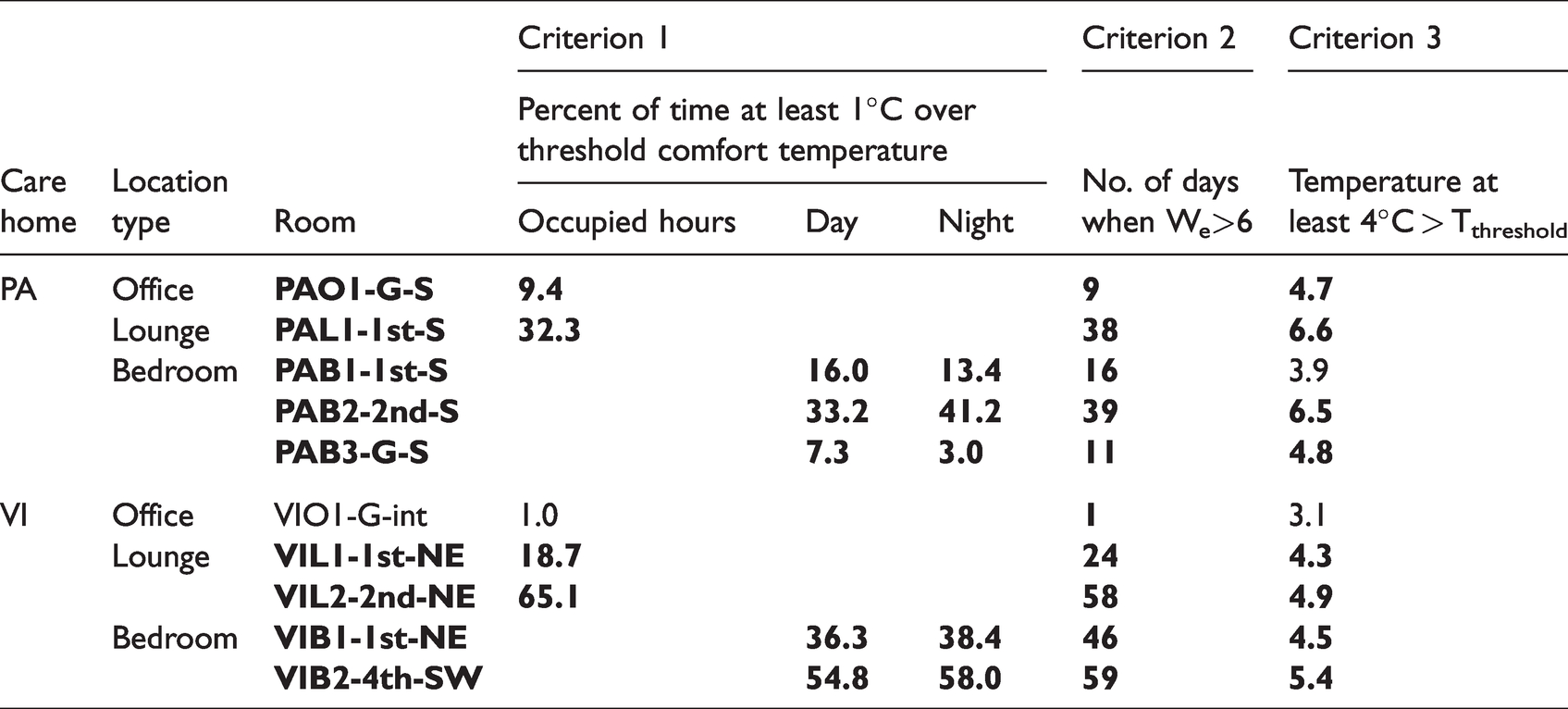
Dynamic overheating metric CIBSE TM52 uses a temperature threshold (TC) dependent on outdoor temperatures: higher outdoor temperatures mean higher TC. Criterion 1 – no more than 3% of occupied hours at temperatures 1°C or more above TC – was failed in all monitored locations except for office VIO1-G-int (Figure 5). All three monitored lounges failed Criterion 1, with VIL2-2nd-NE exceeding TC by more than 1°C for over 65% of occupied hours. Interestingly, three of the monitored bedrooms, PAB2-2nd-S, VIB1-1st-NE and VIB2-4th-SW, had a higher proportion of night hours fail the criterion than day hours.
Temperatures (hourly resolution) in monitored PA (top) and VI (bottom) locations, with threshold comfort temperature shown.
Criterion 2 (We<6) was failed in all monitored locations. In VIO1-G-int it was only failed on one day, but in five of the monitored locations it was failed for over half of the monitored days. Ground floor bedroom PAB3-G-S had significantly fewer days failing criterion 2 than the monitored bedrooms on the first and second floor of PA. Criterion 3 (indoor temperature no more than 4°C higher than the Tc) was failed in all but two of the monitored spaces – PAB1-1st-S and VIO1-G-int. A summary of how the monitored locations measured up against the three criteria (Table 9) highlights how much worse the bedrooms performed compared to offices and lounges. Only one monitored location, VIO1-G-int, was deemed to not be overheating according to CIBSE TM52.
CIBSE TM52 criteria in monitored locations (bold text indicating criterion failed).
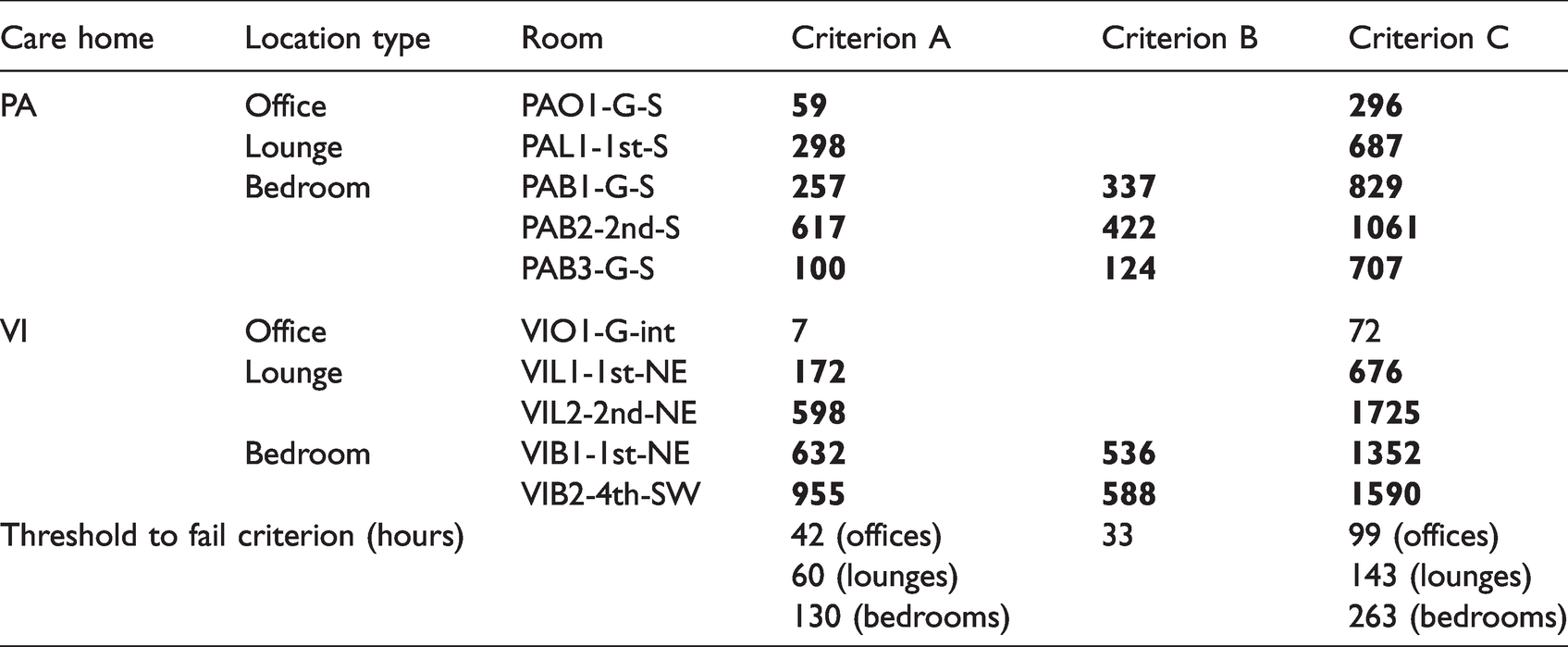
The fourth overheating metric, TM59, combined static and dynamic criteria, with threshold proportions of occupied/day/night hours being relative to total non-heating season (May-September) occupied hours (Criterion A) or total annual occupied hours (Criteria B and C). For criterion A (no more than 3% of May-Sep occupied hours >=1°C above TC), all monitored locations failed except for office VIO1-G-int (Table 10). However, since data was only available for around half of the May-September period, it is possible that even this location may have failed this criterion if monitored for the whole non-heating season. Criterion B (no more than 1% of annual nighttime hours over 26°C in bedrooms) was failed by all bedrooms, being over 26°C for between 124 and 588 of the monitored 675 nighttime hours – far in excess of the 33-hour limit. Criterion C (no more than 3% of annual occupied hours >26°C) was failed by every monitored location other than VIO1-G-int, with ground floor bedroom PAB3-G-S passing the criterion for nighttime hours but failing during daytime hours. Again, with only limited data available, it is very possible that VIO1-G-int would have failed this criterion if monitored for longer, given that in the 75 days monitored, 72 hours were above 26°C, the limit being 99 hours.
Evaluation of TM59 criteria for each monitored location, showing number of monitored hours criteria were failed (bold text cells indicating threshold number of hours were exceeded.
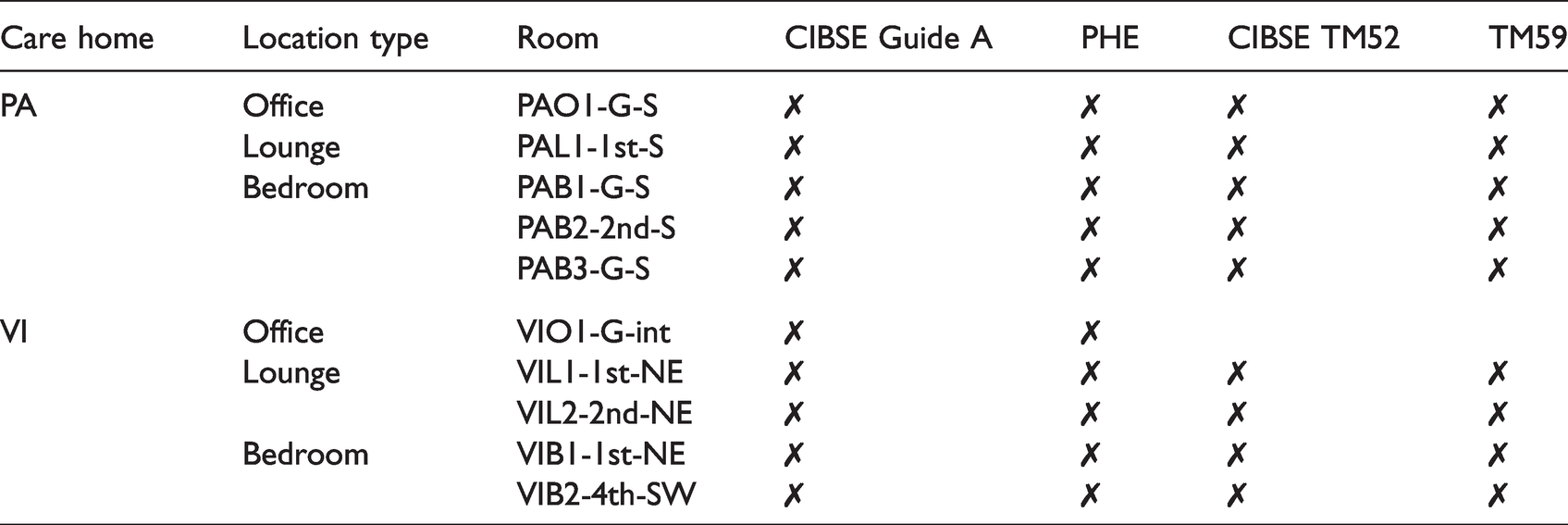
In summary, when applied to the monitored locations, the four metrics investigated all found overheating to be prevalent throughout both care homes (Table 11). Only one monitored location – ground-floor internal office VIO1-G-int – passed any of the four metrics. With all four metrics, bedrooms were found to fail the criteria by the greatest amount.
Summary of overheating metrics in all monitored locations.
It was evident that summertime overheating was prevalent throughout both care homes, particularly in bedrooms, regardless of the overheating metric used. How this overheating was perceived by residents and staff of the care homes was revealed in the surveys and interviews conducted over the same period.
Perception of overheating: thermal comfort surveys
Thermal comfort surveys were conducted over fourteen days: 137 surveys over nine days in PA; 153 surveys over five days in VI. Both care homes showed similar trends, with significantly higher proportions of residents than staff describing their thermal sensation as ‘neutral (neither warm nor cool)’ (Figure 6). As warmer days were targeted for the surveys, very few respondents indicated they felt anywhere on the cool end of the scale. The proportion of ‘warm’ or ‘hot’ responses was around twice as much for staff than for residents in both care homes.
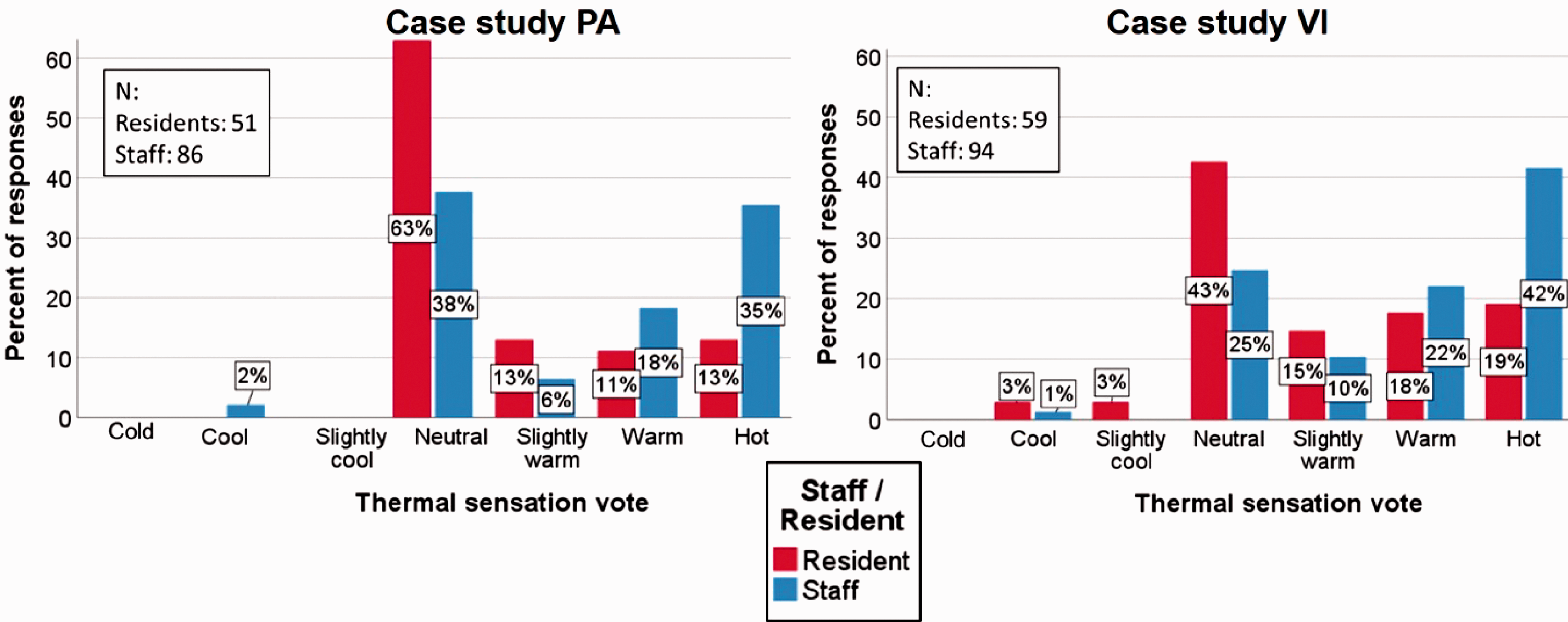
Distribution of thermal sensation votes for residents and staff in case studies PA (left) and VI (right).
The results were similar for thermal preference votes, with significantly higher proportions of residents than staff voting for ‘not change’: 70% (residents) compared to 48% (staff) in PA; 54% (residents) compared to 26% (staff) in VI. Only 9% (PA) and 22% (VI) of resident responses wanted to be ‘much cooler’ compared to 29% (PA) and 38% (VI) of staff responses.
There were moderately strong Pearson correlations between thermal sensation votes and concurrent black globe temperatures for staff in PA (N: 86, R: 0.40), residents in PA (N: 51, R: 0.54) and staff in VI (N: 67, R: 0.44), all significant at the 0.01 level. Interestingly, there was no statistically significant correlation for residents in VI (N: 59, R: 0.08). Boxplots of thermal sensation votes showing the distribution of concurrent black globe temperatures highlight the disparity between temperatures that staff considered warm and hot and those that residents found warm and hot, particularly clear in PA, where the median temperature when staff described themselves as feeling ‘hot’ was just over 29°C, compared to over 32°C for residents (Figure 7). The differences between staff and residents were less pronounced in VI, the most significant difference being the median temperature for ‘neutral’ thermal sensation – around 29.5°C for residents compared to 28°C for staff.
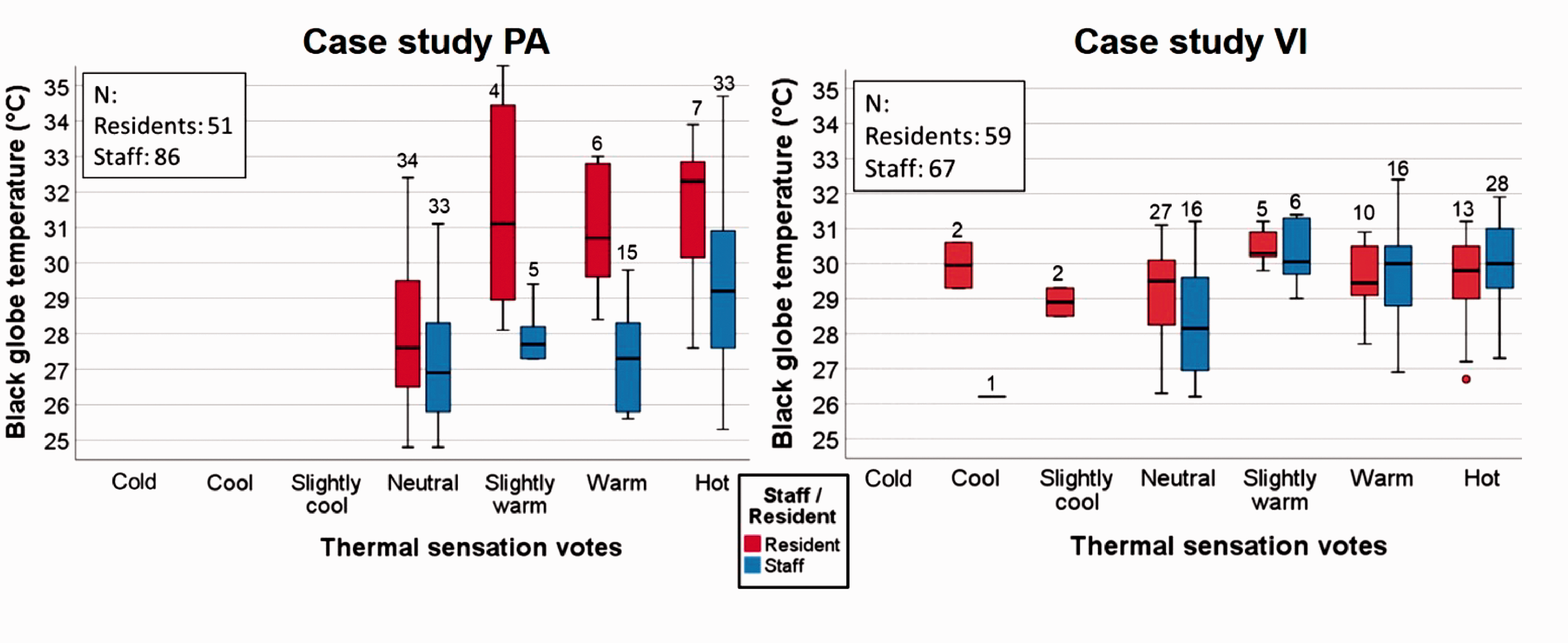
Boxplots showing distribution of temperatures for each thermal sensation vote category for case study PA (left) and VI (right)
Independent samples T-tests showed no statistically significant difference in the distribution of thermal sensation or thermal preference votes for males and females, and no correlations were found between clothing insulation levels and thermal sensation or thermal preference votes. It was notable that staff members, particularly front-line carers, were often limited in what they could wear as they had a set uniform. Residents by contrast were able to choose their clothing (to a greater or lesser extent depending on their cognitive ability) and would often select cardigans and jumpers despite the warm conditions and advice offered from their carers.
Experience of overheating: interviews
From the 26 semi-structured interviews conducted, several themes emerged, many of them were found to be common to both care homes. Key themes that emerged from the interviews are presented below, with quote attributions coded by care home (PA or VI), role (RE: resident, CW: front line care worker, MA: manager of care home) and number. Staff from each care home were more likely to have similar responses to their counterparts than they were with the residents in their own care home, and likewise for the residents.
Awareness of health risks associated with excessive heat
In both care homes, the majority of care workers were able to identify at least one health risk associated with excessive heat, the most common mentioned being dehydration, and associated confusion and urinary tract infections. None of the residents in either care home expressed any concern about their health being affected by excessive heat.
In PA, all three interviewed residents expressed satisfaction at the indoor temperatures during the summer, describing it as comfortable: “In that back lounge where we sit, it never really gets hot, because it’s all shaded, you see” (PA-RE2). Resident PA-RE3 found that by keeping her bedroom and en-suite windows open she would get “a lovely cross draught” (PA-RE3) and rarely felt the need to use her fan. Similarly, VI’s interviewed residents described conditions as “reasonable” (VI-RE2) and “not excessively hot” (VI-RE1).
Care workers, however, consistently described their working environments as hot, although there was no consensus as to whether their respective care homes “overheated” – the definitions of which were clearly subjective. Several care workers in both homes described the indoor environmental conditions during heatwaves negatively: “some days it is not easy to work in here… sometimes it is really hard to cope with [the heat]” (VI-CW1); “You dread coming in because you know how hot it’s going to be” (PA-CW5). However, others tolerated the high temperatures, suggesting a willingness to put the comfort of the residents ahead of their own comfort needs.
Managing heat during the summer
In both care homes, the most common measure identified for managing heat during the summer was opening windows. One PA care worker said when bedrooms were empty staff made a point of opening windows and doors, noting that not all residents liked having their windows open: “Some residents they don’t like to open the window and some say it’s ok” (PA-CW6). Only one interviewed care worker actually said she took the opposite approach, closing windows, doors and curtains when it was hot, because “heat comes from the outside, so we put the fan on [instead]” (VI-CW6).
Following several summers of high indoor temperatures, VI’s facilities manager had invested in fans for every bedroom in the care home. These had been installed earlier that summer and were commonly cited by the care workers as an effective heat mitigation measure. Only the facilities manager acknowledged the fans’ limitations – able to circulate air but not lower temperatures: “…It helps a little bit but doesn’t actually solve the problem as such” (VI-MA2). Fans were also used in PA, with many care workers viewing them as useful and effective. In PA’s lounges, care workers were able to arrange the residents according to their thermal preferences – in the path of the fans or away from them. However, there was unclear how much bedroom fans were used, and it was noted by the nurse that using fans risked spreading infections. “We don’t like to use [the fans] because of the spreading of the infections, we don’t like it but we need to use if it’s hot” (PA-CW2).
In both care homes, many care workers and some residents described closing the curtains as an effective measure to keep the sun out of the bedroom, although some opened curtains along with windows and vents to allow better air circulation – likely to have been more effective in rooms which were not receiving direct sunlight.
The care home managers interviewed acknowledged that although they were officially responsible for the management of heat mitigation measures, in practical terms it was the frontline carers who implemented them. The frontline care workers agreed with this sentiment, although there were mixed opinions as to what would trigger them taking action: some said that they would take the initiative themselves, others that they would only act if residents asked. This is a complex situation, with some residents more independent and able to open windows, close curtains, turn on fans themselves, but many others not only physically unable, but with cognitive and communicative impairments that rendered them unaware of or unable to communicate their thermal comfort or preference levels. Ultimately it was up to the care workers to determine the best course of action for each situation. But with many residents making requests that were not in their best interest – e.g. keeping windows closed when temperatures were high – the care workers often had make a choice between what the residents wanted and what they needed – not always the same thing.
As a personal response to high temperatures, frontline care workers would drink more fluids and take (more) short breaks, although it was acknowledged that this could be difficult because of the constant demands of their job. In both care homes, the uniforms of the staff were described as being too hot, particularly for those serving food and having to wear plastic aprons. Care home managers had less physically demanding roles and therefore seemed more adaptable to the high temperatures: with more clothing options, walking to cooler parts of the building or outside, drinking and benefiting from open windows and fans at their desks.
Managing expectations and needs of residents
Providing residents with plenty of drinks during hot weather was mentioned by nearly all interviewed members of staff – managers, care workers and nurses. Fluid input and output was monitored carefully. Ice pops and ice lollies were also mentioned as an alternative way of getting fluids into the residents. However, many residents needed encouragement to take their drinks: “Some of them it’s really hard to push even one glass inside them. It really depends on the patient, the condition, the diagnosis…” (VI-CW4). Interestingly, when asked whether they thought they drank more in the summer and in hot weather, some residents thought they did, but others were adamant that they did not: “No, I don’t think so. I think you do if you’re hot, but like I say, you don’t really get hot here” (PA-RE2).
In both care homes, care workers described residents having seasonal menus, the summer menu offering more salads, fruit and cold desserts. However, there was no consensus amongst staff as to whether residents would necessarily choose these lighter options over their regular hot dish: “They like their meat and two veg regardless” (PA-MA1). This concurred with what the residents said about their diet, most believing that they did not change what they ate during the hot weather. One resident admitted that she sometimes felt like “not eating at all. Sometimes I can’t be bothered” (VI-RE3). This loss of appetite and lethargy could be linked to feeling too hot.
Both care homes’ care workers described giving the residents more baths and showers during hot weather, with PA’s manager suggesting that residents “might even request a bath or a shower… to cool them down” (PA-MA1). However, the majority of the interviewed residents did not perceive having more baths or showers during hot weather.
Adapting what the residents were wearing proved to be a challenge for the care workers. Since many residents suffered from dementia, they were less aware of their thermal conditions and often unwilling to dress accordingly: “…Some of them even it’s like this summer like 33 degrees and the gentleman still was wearing vest, t-shirt and shirt on top of that… We had a lady, she is 97, so she was actually wearing woolly cardigan when there was this heat” (VI-CW4). Care workers had learned ways around this, for example “give them a blanket, but quite an airy one, so it’s not too hot and it’s not too cold” (PA-CW1). Resident responses generally concurred, some saying that they would wear lighter clothes in hotter weather, others saying they would not vary what they wore even on hot days.
Barriers to implementation of heat risk mitigation strategies
Very few members of staff, including managers, identified any building-related barriers to implementing heat mitigation strategies. However, some care workers and VI’s facilities manager noted that having window restrictors limit openings was a challenge, with few perceiving the restrictors to be a necessary precaution: “4 inches, that doesn’t allow a lot of airflow, especially without the fans, there’s not enough airflow” (VI-MA2). Only the care home managers mentioned their necessity: “…It is a health and safety executive requirement to have the restrictors” (PA-MA1). PA’s 1st floor lounge had trickle vents which were about 3 m high and never opened because “we can’t reach them” (PA-CW1). VI’s facilities manager also described how VI’s pipework had sprung numerous leaks when it was turned off for the first time after construction. In response, the boiler was left running throughout the year and each radiator turned off instead. Although this helped, the pipes running through the building, particularly along the corridors, remained hot throughout the summer, exacerbating the already high temperatures.
Only VI’s facilities manager had considered the building design as a whole: “…The way the building is built, obviously they weren’t thinking of this climate change and I think they could have done it a lot different… all we think about is cold, cold, cold, you know, we worry about heating, heating, but you know never cooling, you know” (VI-MA2).
The main behavioural challenge was managing residents who perceived the heat differently not only from the staff but from one another. Communal spaces often proved challenging, with some residents feeling too hot, but their neighbours feeling too cold. This manifested itself in residents not adapting their behaviour to meet their physical needs – e.g. not drinking enough fluids, adapting what they ate or wore.
The interviews with residents and staff reinforced the survey findings that residents and staff perceived their environmental conditions differently in both care homes: staff finding conditions hot while residents feeling less sensitive to heat. Consequently, the measures taken by staff to reduce temperatures or mitigate their effect were often met by resistance from the residents: windows were kept closed, fans not being fully utilised, extra fluids not being consumed, clothing and diet not being adapted. Understanding of the health risks of overheating was limited amongst the staff and virtually non-existent amongst the residents.
Discussion
Continuous monitoring of indoor temperatures during the summer 2019 revealed the prevalence of overheating in both care homes settings with some notable differences. Case study PA was a smaller and much older care home than VI. Consequently, although monitored rooms in PA reached higher peaks than those in VI (34.7°C in PAB2-2nd-S compared to 32.5°C in VIB2-4th-SW), the overall interquartile range of temperatures was lower in PA (24.8–27.0°C) than in VI (25.3–27.7°C). Both buildings remained warm overnight, with indoor temperatures never falling below 20°C in PA or 21°C in VI. Examination of diurnal CO2 profiles alongside evidence from interviews revealed that it was common practice to close windows at night (an institutional practice routed in a concern that residents should not get cold), severely hampering the ability for the building to purge its daytime heat gains. Indeed, in both care homes, the warmest locations were the bedrooms, where temperatures were often higher at night than during the day. Several factors contributed to this counterintuitive finding: Overnight, bedrooms were occupied, with doors and windows closed. During the day, residents may have vacated their bedrooms and doors and windows were more likely to have been open; Bedrooms were smaller spaces and had only one window and door. By comparison, lounges had several windows and larger doors, allowing more opportunity for cross ventilation during the day and (where possible) purging of heat overnight; Though deployed in bedrooms, fans were often not used, often because the residents did not like them; In VI, bedrooms had en-suite facilities, so heat from bathing would increase room temperatures.
Static overheating metrics, CIBSE Guide A and PHE, found all monitored locations to be overheating. Metrics CIBSE TM52 and TM59 found all but one monitored location to be overheating. The fact that bedrooms were found to be overheating even at night was concerning, particularly for those residents who were unable (or unwilling) to leave their bedrooms to find a less hot part of the building or even go outside. However, although the communal areas were less likely to be overheating, they still remained in the 26–28°C range and higher for the majority of occupied hours, offering little respite to residents or staff.
Relative humidity in monitored locations in both care homes was found to be low. Lounges were below the recommended 40% for between 37 and 56% of occupied hours. Bedrooms had slightly higher RH in PA than in VI, and levels tended to be slightly higher at night than during the day, but still 14–48% of daytime hours and 4–44% of night time hours were below 40%. Low RH has been linked to dry throats, noses and eyes and an increase in the spread of airborne viruses – particularly significant in the Covid-19 era. Measures to bring RH more into the 40–60% range are recommended.
A significant finding from this study was the disparity between how the indoor environment was perceived by the elderly residents as compared to the care home staff. The majority of residents rated their thermal comfort as neutral, even when black globe temperatures were over 30°C. Staff members were twice as likely as residents to rate their thermal sensation as warm or hot, and at black globe temperatures as low as 25–26°C. Thermal preference votes showed similar disparities. The reasons for these differences in perception included the differences in activity (passive residents, active frontline carers) and metabolism (slower in elderly residents than in younger carers.36,37 It is worth noting that both residents and staff in PA seemed more content with their indoor environmental conditions than their counterparts in VI: thermal comfort votes of ‘neutral’ or ‘slightly warm’ received 76% of PA resident responses compared to 58% of VI resident responses and 44% of PA staff responses compared to 35% of VI staff responses. This was interesting, considering VI was a modern purpose-built care home and PA a 200-year-old converted care home.
Despite being aware that their local environment could get hot at times, residents in both care homes perceived themselves to be comfortable in those conditions and did not recognise their susceptibility to heat stress. Frontline staff were much less satisfied with their conditions, but felt that there was little that they could do to alleviate their suffering: the care of the residents had to come first, so very few tasks were optional, and their uniforms limited how much they could adapt their clothing to alleviate overheating. In both care homes, the understanding of health risks associated with overheating was limited amongst the staff and non-existent amongst the residents. The responses to overheating tended to be reactive rather than proactive – e.g. opening windows and providing more fluids. There was little mention of keeping windows shut to keep heat out when outdoor temperatures exceeded indoor temperature, and it was evident that routines of closing windows at night were often maintained even during the hottest periods, preventing nocturnal purging of heat and resulting in bedrooms being warmer at night than during the day.
The limited window openings proved to be a significant feature of the care settings, with many frontline carers expressing frustration at how much they reduced the effectiveness of ventilation measures. The regulations regarding window openings were introduced decades ago at a time when overheating in care homes was not considered. Although the care home managers felt the restrictions were necessary for the safety of the residents, a strong case could be made for this regulation to be reviewed, weighing up the perceived benefits to resident safety against the increased risks associated with overheating. This is not necessarily a binary situation – window restrictors or no window restrictors. Increasing the limit on window openings may allow significantly more ventilation whilst still preventing residents falling out. Alternatively, care home windows could be designed in such a way as to allow several small openings rather than a single large one.
Conclusions
This paper has empirically assessed the magnitude, duration and perception of summertime overheating during summer 2019 in two contrasting care settings - one modern and one older care home located in London. Alongside objective environmental monitoring, thermal comfort surveys and interviews provided subjective insight into how these environmental conditions were perceived by residents and staff. Both care homes were found to experience overheating, particularly in bedrooms, even overnight when residents were asleep, opportunities for adaptation were minimal. Overheating was found to be more severe in the modern, medium-weight purpose-built care home than in the 200-year-old, heavyweight converted care home. This is an important find, as it challenges the design choices for the modern care home – with its bespoke features aiming to accommodate vulnerable occupants – if it then performs worse than a 200-year-old building which would have faced multiple limiting factors in its conversion to a care setting. The low RH measured posed a further risk to the health and wellbeing of the staff and particularly the residents and should be addressed in parallel with overheating.
It is evident that the design of care homes matters. Health and safety regulations restricting the extent to which windows can be opened limit ventilation during the day and purging of heat at night. Other options such as utilising thermal mass in the building fabric, and opportunities for more effective cross-ventilation need to be considered. External window shading may offer a relatively low cost option, designed to take account of seasonal variations: brise-soleil could provide shade from the high summer sun but allow low winter sun to permeate into the building. With a focus on keeping residents warm through the winter, care home designs have neglected the risks of summertime overheating. With the warming UK climate, the potential for this continues to increase and must be considered in the design of care settings. This is not an easy task.
Given that care homes are by their very nature hybrid buildings (serving both as living spaces for the residents and offices/workspaces for the staff members), it is vital to provide adequate comfort to both groups, particularly during periods of hot weather. This is confounded by the fact that the elderly residents were relatively insensitive to high temperatures. Heat management in care homes needs to be customised for the season, rather than being left on throughout the year. Institutionalised attitudes and routines need to be more flexible depending on the varying indoor environment. This requires radical changes in the building design, heat management and care infrastructure to prevent any ill-health effects of overheating amongst the elderly residents and care home staff.
Footnotes
Acknowledgements
The authors are grateful to the staff and residents of the case study care homes for their engagement in the project and assistance in data collection. This research was performed in compliance with UK laws and guidelines and was approved by Oxford Brookes University’s research ethics committee (UREC Registration No: 191287).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to thank NERC (Grant ref: NE/S016767/1) for funding the ClimaCare research project.