
Abstract
The “workbook” is an underexplored concept in the literature of cognitive behavioral therapy (CBT). Unlike manuals, workbooks provide resources without prescribing standardized procedures for practitioners to follow, potentially allowing for greater flexibility. This study explored the experiences of six UK-based educational psychologists using a popular workbook, Think Good – Feel Good (TGFG), to support CBT for young people (YP). Semistructured interviews were conducted online, and data were analyzed using thematic analysis. Five themes were identified. Practitioners felt practically and emotionally supported by TGFG. Think Good – Feel Good was used flexibly, combined with other therapeutic modalities, and its resources were adapted. Think Good – Feel Good helped practitioners make CBT developmentally appropriate and engaging for YP. There were potential benefits and challenges to school staff using TGFG in tandem with psychologists. Finally, supplementary resources (e.g., worksheets) helped to contain the emotional intensity of therapeutic interactions and supported practitioners to develop therapeutic alliances with YP.
Introduction
Cognitive behavioral therapy (CBT) is a therapeutic approach to exploring thoughts, feelings, and behaviors (Beck, 1970; Fordham et al., 2021). Cognitive behavioral therapy focusses on interpretations of events, proposing that changing one's cognitive perspective can relieve emotional distress and help one find alternatives to maladaptive behaviors. Cognitive behavioral therapy has a strong evidence base for supporting young people (YP) with common difficulties such as anxiety and low mood (David-Ferdon & Kaslow, 2008). A meta-analysis evaluating CBT for childhood anxiety compared participants with favorable and unfavorable outcomes; there was a medium effect size (odds ratio 2.55, 95% confidence intervals [1.32, 4.93]) across six studies comparing CBT with attention control groups who had nontherapeutic contact with psychotherapists, controlling for participants’ expectations of change (Sigurvinsdóttir et al., 2020). This shows that having CBT is significantly more likely to lead to positive outcomes, such as increased well-being, over and above the effects of simply meeting with a psychotherapist.
Cognitive behavioral therapy workbooks are nonprescriptive collections of evidence-based resources and guidance that practitioners use to design, adapt, and deliver therapeutic interventions (Stallard, 2002). Workbooks can be contrasted with manuals, which provide standardized and prescriptive guidelines about the theory, sequencing, content, and procedures of sessions (Kiesler, 1994; Marshall, 2009). Manuals are favored methodologically in research on CBT effectiveness because they maximize the internal validity of experimental designs (Barker et al., 2016). Manuals also have a significant presence in practice, with 11.4% of 317 US-based CBT practitioners reporting frequent manual usage and 58.7% reporting occasional use (Becker et al., 2013). Workbooks, on the other hand, resist controlled experimental research by the nature of their design; as articulated by one workbook author, “[it] is not intended to be delivered systematically” (Stallard, 2018, p. 26). The guidance and resources within workbooks are evidence-based, but the workbook as a whole does not represent an intervention package to be delivered.
Although previous research on CBT workbooks is scant, there is evidence that, among 21 UK-based educational psychology services delivering CBT, 57% of practitioners use workbooks, suggesting a considerable presence in practice (Greig et al., 2019). Comprehensive guidance has been produced by the British Psychological Society on delivering therapy in schools which highlights theoretical, ethical, training, and contextual factors (Dunsmuir & Hardy, 2016). A review of international educational and school psychologists’ delivery of therapeutic interventions identified 16 studies, with nine focussing on CBT; while all studies identified some positive social–emotional outcomes, six identified no change on certain measures, and four identified negative impacts (Simpson & Atkinson, 2021). These equivocal results are not unusual; a systematic review identified that just 49.5% of adults with anxiety experienced positive outcomes from CBT (Loerinc et al., 2015). However, it is vital to conduct further research into the factors affecting successful delivery of CBT by psychologists in schools.
The current study aims to address the knowledge gap around the function and possible benefits of CBT workbooks. Qualitative methodology was chosen as appropriate to the exploratory nature of the research, which aims to descriptively outline the experiences of practitioner psychologists using a workbook. Such an approach is important in laying the groundwork for future hypothesis-driven research (Barker et al., 2016).
Workbooks may be particularly prevalent and useful for practitioners working with YP, since CBT principles need to be adapted to make them developmentally appropriate (Fuggle et al., 2012). Cognitive behavioral therapy has a strong evidence base for supporting YP, despite around 75% of CBT research being conducted with adult populations (Fordham et al., 2021). For YP to engage effectively in CBT, they require metacognitive awareness, motivation to change, and sufficient language skills (Stallard, 2021). By age seven, most YP can comfortably participate in CBT (Stallard, 2018). Common developmental adaptations include incorporating YP's interests (Rosenstiel & Scott, 1977), using play (Ronen, 1992) and metaphors (Friedberg & Wilt, 2010) to explain concepts, telling stories (Collins-Donnelly, 2013), and using visuals (Scheeringa et al., 2011).
The current study focusses on Think Good – Feel Good (TGFG) as a widely used example of a CBT workbook that incorporates many of the abovementioned, evidence-based examples of developmental adaptation (Stallard, 2002, 2018). The authors have no relationship, commercial or otherwise, to TGFG. Recent mixed-methods survey research with 238 practitioners found that TGFG is used by novices and experts as a planning aid, to boost practitioners’ own feelings of confidence, to read passages aloud during sessions to explain key concepts, and to complete interactive worksheets that engage YP's interest (Redburn & Hayes, 2023). In this study, there was a significant association between whether practitioners read aloud from TGFG during sessions and practitioners’ degree of training, χ2 (2) = 15.34, p < .001, ϕc = .315. Practitioners who were self-taught by reading the guidance chapters of TGFG (as opposed to practitioners with formal CBT training) were more likely to read aloud from TGFG during sessions than expected by chance (z = 2, p = .046). Being self-taught was also associated with having the fewest years’ experience (z = 2.1, p = .036). This suggests that TGFG may be used differently by novices and experts, with novices feeling more reliant on the workbook and experts feeling more confident to adapt resources and use TGFG flexibly.
While this survey research was useful for broadly establishing how TGFG is typically used and the breadth of usage, the data collected had little detail or contextualization. To address this limitation, the current study uses interviews to achieve greater insight into practitioners’ experiences of using the TGFG workbook. This research follows the principles of implementation science, aiming to identify and address facilitators and barriers to intervention usage in practice, considering the acceptability of interventions to providers and recipients, skills and knowledge of providers, and organizational context demands (Bauer & Kirchner, 2020; Forman & Barakat, 2011). Specifically, this study addresses the following research question (RQ): What are the experiences of practitioner psychologists using a CBT workbook (TGFG) when working with YP?
Method
Participants
A purposive sampling strategy was pursued through targeted emails and social media advertising (Robson, 2002). Emails were sent twice to a large mailing list (EPNET), used by many UK-based educational psychologists (EPs) and allied professionals. Posting on the first author's personal Twitter profile led to 224 “engagements” with the posts from potentially eligible users. In addition, at the end of a survey (n = 238) about TGFG described in a previous study (Redburn & Hayes, 2023), participants were invited to contact the authors if they wished to participate in the interviews described in the current study; there was no obligation for participants in the current study to have completed the survey, and it is not known whether any participants took part in both studies. There were three inclusion criteria for participants:
Currently practicing in educational psychology in the UK Formal training in CBT (defined as multiple days’ teaching covering CBT fundamentals) Experience using TGFG with YP aged 5–18 on more than one occasion
Given that TGFG is used by both novices and experts (Redburn & Hayes, 2023), it was considered beneficial for participants to have a range of experiences using TGFG to compare and contrast their viewpoints. Participants gave informed consent. Six individuals were interviewed (see Table 1).
Demographics of interview participants.
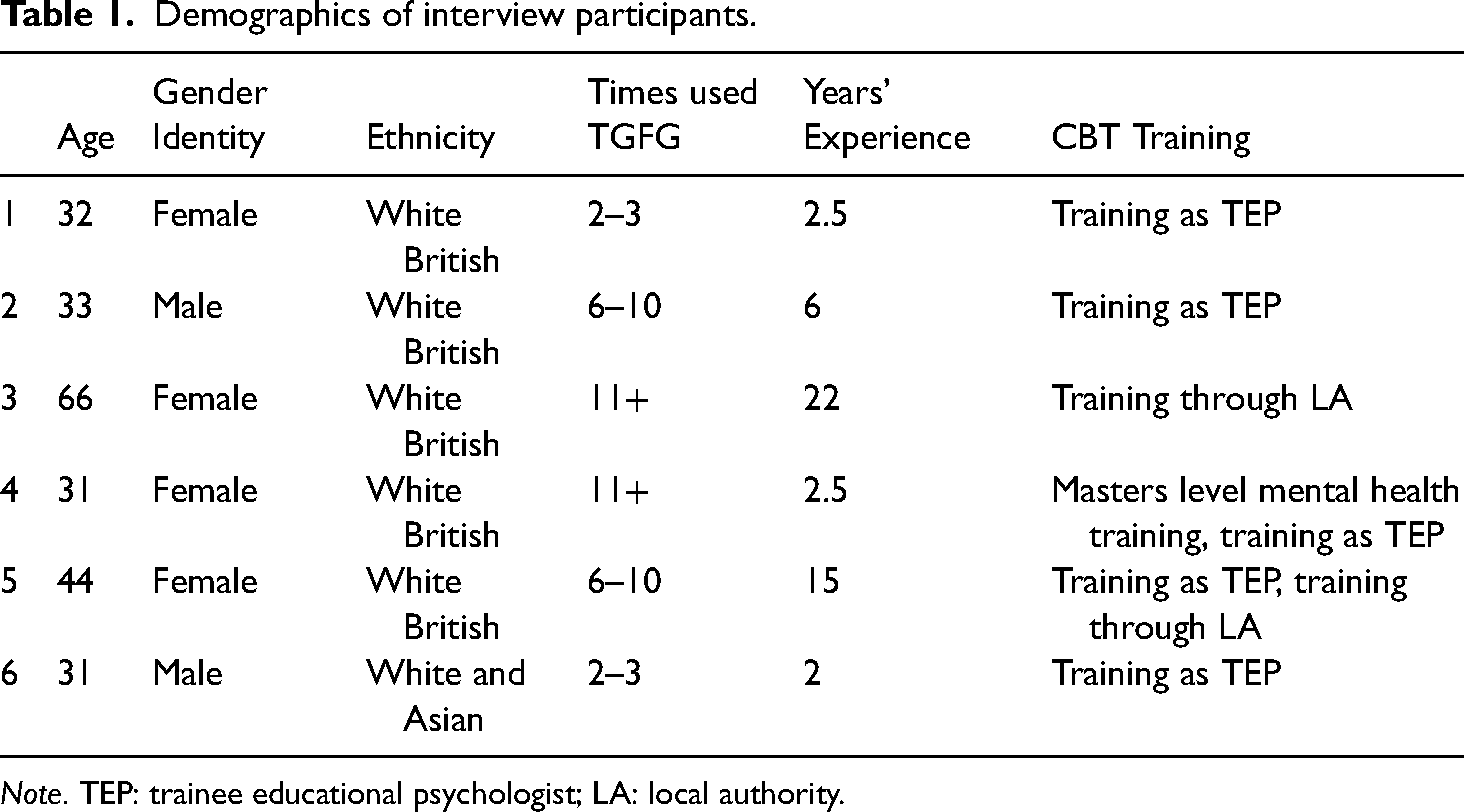
Note. TEP: trainee educational psychologist; LA: local authority.
Participants’ years of experience as EPs ranged from 2 to 22 years (x̄ = 8.3 years, standard deviation [SD] = 8.3 years). Participants’ ages ranged from 31 to 66 years (x̄ = 39.5 years, SD = 13.9 years). Two participants had used TGFG 2–3 times, two had used TGFG 6–10 times, and two had used TGFG 11+ times throughout their professional careers, indicating a range of experience from novices to regular users. Regarding “CBT training,” in the UK trainee EPs routinely get taught the fundamentals of CBT as part of their professional doctoral training courses. Most EPs are employed by local authorities and may receive CBT training via their employers.
Procedure
Ethical approval was obtained from University College London ethics committee. A pilot interview was conducted with an experienced TGFG user and minor alterations to question wording were made. Interviews were conducted online using Microsoft Teams, lasted between 28–53 min (x̄ = 44 min, SD = 9.6 min), and were guided by a semistructured schedule (see Appendix A). Questions addressed professional experience, typical TGFG usage, how TGFG is helpful and engaging, and the comparison of TGFG with other CBT approaches. Follow-up probes were used to further explore issues raised or enquire about issues not raised (Turner, 2010; Zeisel, 1984). Transcripts were produced automatically by Microsoft Teams and edited for accuracy. Data collection was halted at the point of saturation, when further data collection is unnecessary as it would be unlikely to result in important new ideas (Guest et al., 2006; Saunders et al., 2018). The last interview provided no new major ideas.
Data analysis
Data were analyzed by the first author using six-phase thematic analysis (Braun & Clarke, 2006, 2022). Transcripts were read through to enable familiarization and noting of initial impressions. Transcripts were copied verbatim into NVivo. Meaningful ideas were identified as codes before being grouped together under themes and subthemes. Researcher-derived coding was used, going beyond the language of participants and labeling codes based on researcher interpretation while remaining close to the manifest content of responses (Braun & Clarke, 2013; Ely et al., 1998). A complete coding approach was taken, identifying everything of interest within the dataset. Themes were labeled descriptively to convey core ideas that summarized or connected multiple codes. Codes and themes were reviewed against transcripts to ensure accurate and comprehensive reflection. The second author carefully supervised the whole analysis, checking for representativeness and clarity. Illustrative quotes were identified for inclusion in the results and discussion of this article. Familiarization, review, and supervision procedures helped to enhance credibility (ensuring research addresses its intended aims) and trustworthiness (ensuring research is documented systematically; Bazeley, 2013; Braun & Clarke, 2013).
Reflection
This study took a theoretical perspective of pragmatism, which holds that knowledge is important insofar as it is useful for human endeavor (Barker et al., 2016). Epistemologically, pragmatism is informed by constructionism, which holds that knowledge is created through individuals’ interpretations of experiences (Moon & Blackman, 2014). Methodologically, data collection methods are chosen to provide useful information rather than for ideological reasons.
The authors pursued an exploratory approach to the research topic, given the paucity of previous research on TGFG and CBT workbooks in general. This permeated the research process, including the design of data collection measures and the analysis of findings. The researchers’ intention was to explore what is currently going on in practice, an aspect which supports the transferability of the findings to other practice contexts. The researchers did not intend to explicitly define good or poor practice or whether practitioners were adhering to what is recommended by the TGFG author. As such, claims are not made that the participants in this study were espousing best practice; rather, they provided a realistic sample of the current state of practice.
Regarding positionality, the first author has three days’ doctorate-level CBT training, significant research methods training, and experience using TGFG. The second author has been practicing as an EP for over 25 years and has delivered and recommended CBT during that time, including experience with TGFG. In addition, the second author has worked for a university Educational Psychology department with involvement in teaching and research for nearly 20 years. The authors and all interviewees were EPs; shared professional experiences allowed them to build rapport and understanding during interviews, helping participants to feel comfortable sharing their views honestly, and contributing to the credibility of findings. A possible drawback of shared experiences is that researchers and participants may have assumed shared knowledge of certain concepts and contexts that could have been interrogated further.
Measures were taken to bolster the validity of the research (Sabnis & Wolgemuth, 2024). The American Psychological Association's Journal Article Reporting Standards for Qualitative Research were consulted and used as a guide across the manuscript (Levitt et al., 2018). External auditing took place with a group of peers and an experienced qualitative researcher, who offered feedback at the stages of developing the research design and analyzing initial findings. This shaped the subsequent analytic process, prompting reflexivity among the authors. In addition, a detailed audit trail was maintained at all stages of the research process, so that all decisions could be justified and interrogated retrospectively as needed (Onwuegbuzie & Leech, 2007).
Results
The analysis led to five themes, which are outlined in Figure 1.
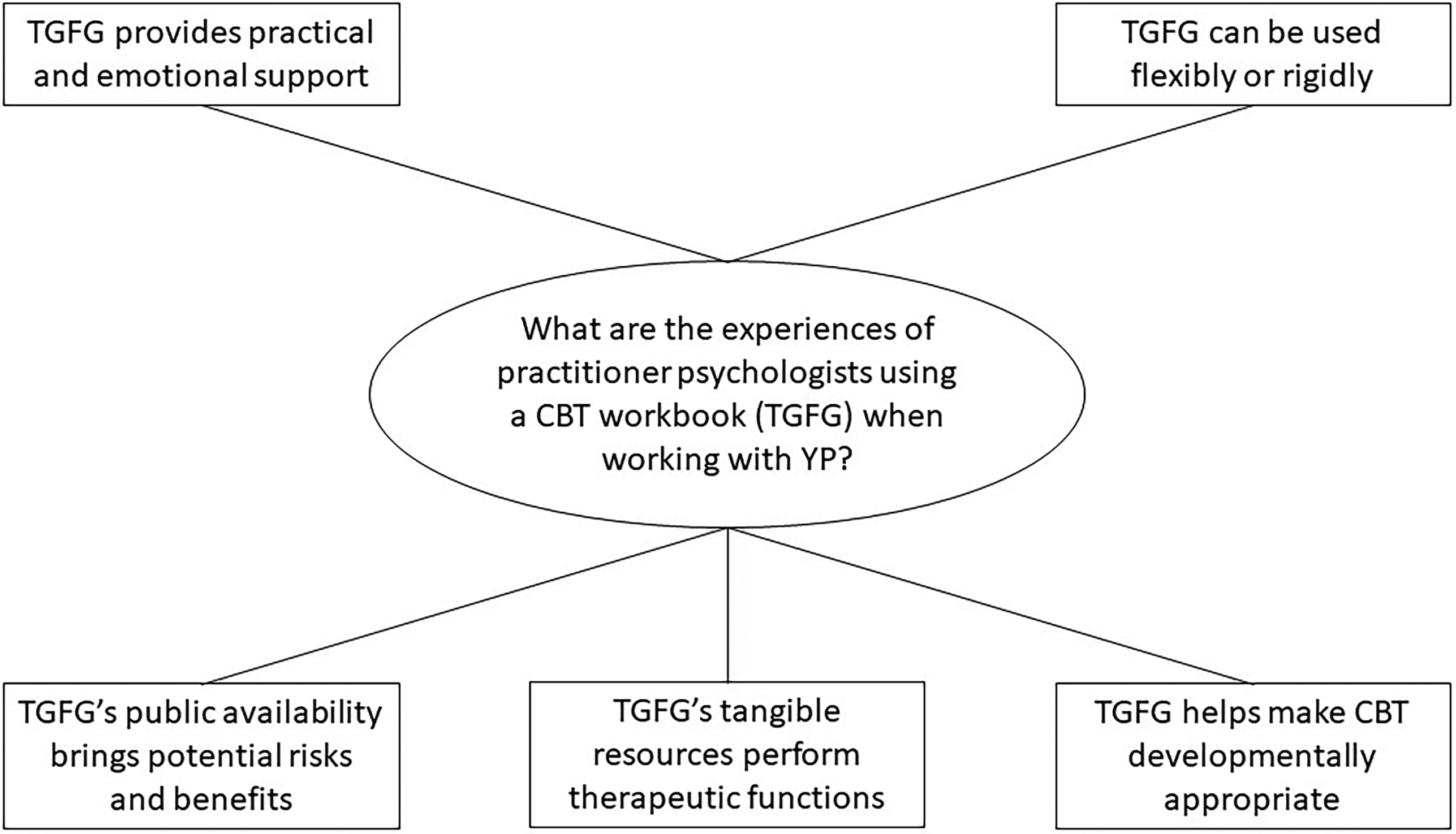
Thematic map of EPs’ experiences using a CBT workbook, “Think Good – Feel Good.”
Think Good – Feel Good provides practical and emotional support
Think Good – Feel Good was seen as a convenient and accessible “planning aid” (Participant 6 [P6]). Practitioners used TGFG as “a quick revision manual… I haven’t got to plough through all the thick tomes, I can just pick this up and see what might be useful” (P3). Think Good – Feel Good helped make the most challenging parts of CBT more accessible; according to P5, “the bit about CBT, I think, is hardest for the clinician and the child is the cognitive element… any concrete prompts that help you with that, like they have in these books, are really useful.”
Tangibility was helpful for reminding practitioners what had been covered before, as suggested by P5, who commented: “I use the worksheets because it records stuff and therefore I don’t have to remember it.” This participant further noted that the recording attribute of worksheets was used as evidence of progress within the therapeutic relationship, explaining that, “we set up a folder … I come to the next session, we review what we did in the previous session and our learning and try to build on it.”
Worksheets could be self-contained and useful to nonpsychologists; P2 stated that “in a consultation if something came up I may have provided a particular resource.” P5 further commented that worksheets could assess YP's understanding and motivation for engaging in CBT, stating: “I might take bits out of TGFG to see if they’re ready for following through with an intervention, that's something they might engage with, by how they engage with a couple of initial worksheets.”
Think Good – Feel Good helped less experienced practitioners feel confident in their ability to deliver CBT, with one participant noting, “It gives you a sense of security, knowing that you aren’t just making things up” (P6). By following TGFG content, practitioners felt “what you’re doing is evidence-informed” (P4). Participants felt confident about the developmental appropriateness of content, with P1 commenting “it's reassurance that this will be appropriate for someone… This is well researched to be helpful for this age group.” For P6, reassurance and evidence base were connected with professional accountability: “You know that if later on you’re questioned, ‘then why did you do this?’, you can go back to those resources and say… ‘look, I was following this program.’ I know that there's evidence behind the program.”
Two participants read passages aloud verbatim to ensure explanations were accurate, with P3 wanting to be “sure I’ve got them right for the child.” Similarly, P5 observed that the book explains things well, commenting “I might say ‘I’m going to read this bit out the book, ‘cause this bit's really important and I can’t teach you this bit any better than what it says here.’” Reading aloud from TGFG emphasizes the importance of particular passages, supporting the pedagogical process.
Over time, participants’ usage of TGFG changed. Illustrating this point, one participant stated: “at the beginning I used it in a structured way and it supported my feelings of confidence and competence… the more you use the materials… the more you can be flexible” (P5). Structured workbook usage was associated with low levels of experience and confidence, perhaps because this provided security. Over time, practitioners saw flexible usage as more effective or desirable.
Think Good – Feel Good can be used flexibly or rigidly
There were positive and negative opinions about using TGFG rigidly (covering all the content in order). P4 suggested, “You might as well just be a robot,” while P6 suggested, “manualized interventions are for slightly lesser skilled professionals.” These opinions were personal for P4, who stated: “It would take away something from my identity. I have a belief that that manualized approach isn’t as useful, so it wouldn’t be as useful because I’m being horrible about it from the beginning.” This participant referenced a self-reinforcing cycle, whereby negative “beliefs” about manualization could negatively influence her practice.
In contrast, some participants contended that rigidly following a structure could “help people feel more confident” (P2) because “you can be sure you’re doing the right thing, whatever the right thing is that the book prescribes” (P6). P4 described the “right thing” as “permission to be creative.” The decision of whether to work in a structured way might be influenced by practitioners’ personalities, as “people are very different to the extent to which they like to be exactingly following things and the extent to which they like to improvise” (P1). Taking the middle ground, P2 highlighted “the combination of having a structure of activities, but being able to equally use them quite creatively. That's what works for me.” P6 emphasized that following the TGFG structure rigidly supports practitioners with limited resources, with P4 similarly stating that “some people don’t have the time, the headspace, the funding to be able to [work creatively], so I understand why it becomes manualized.”
Participants combined TGFG with other therapeutic approaches, describing TGFG as “one strand among other strands, but because it's got so many good child-friendly ideas, it's probably the thickest strand” (P3). Practitioners incorporated techniques from solution-focused therapy, personal construct psychology, or acceptance and commitment therapy. Other approaches help “to get an idea across or to tease an idea out from a child” (P3). Despite this multiplicity, TGFG was seen as the “thickest strand” because: It’s so flexible, it’s hard not to use it from my perspective. Maybe that’s a sign of my level of experience and competence that I go to TGFG. Maybe if I knew more about CBT, I’d have a broader range of tools. (P2)
Participants personalized CBT to individual needs, skills, and preferences. This could happen reactively, “being able to adapt quickly on your feet” (P3). Reactive flexibility could be missed if “you’re ploughing through it bit by bit” (P3), as following the content may take precedence over monitoring YP's engagement and understanding. P3 found the range of resources in TGFG helpful if she needed to change direction, commenting “there's enough in the book that you can pick and choose and work with a child on the one you think is resonating with them.” As noted by P4, the decision of whether to follow a structured approach was influenced by YP's preferences: “When you meet them and realize this is someone that loves structure it's a good idea to go for a more manualized approach, you can adapt it based on their learning style.” P5 expressed a similar sentiment, stating that “some children need the worksheets… sometimes they’re very happy just chatting.”
Practitioners improved the experience for YP by personalizing content, with one participant commenting “the more specific examples are to them… something they’re interested in” (P4). Some felt it necessary to adapt TGFG, with P6 describing a situation in which a “student's level of language necessitated that it was simplified.” Similarly, P3 stated, “it's the thinking errors… there are too many to present to a child, so I tend to… pick maybe two or three.” A large range of material could be overwhelming and detract from learning.
Think Good – Feel Good helps make CBT developmentally appropriate
Participants felt that YP needs the requisite cognitive skills to engage with CBT because “people can find it very difficult to separate thoughts and feelings” (P1). Metacognitive skills help bridge the gap between self-awareness and self-understanding, with P5 commenting that “lots of children don’t know and understand why they think and feel the way they do… they want to know and understand it.” Further illustrating this point, practitioners described YP experiencing a “lightbulb moment” (P3). According to P5, YP who are motivated and able to understand CBT concepts “are typically the children that are really fascinated by the awareness you give them.”
P1 noted a risk of YP being referred for CBT by other people, stating “It's crucial to form the goals with the YP rather than say ‘your teacher said you need to do X, so we’re going to do that with you.’” P4 collaborated when writing formulations to make them pedagogically useful, clarifying that “it's not like a map of 100 things that might go on, which you might see in an adult model, but this is the type of thing you can use but also share with the child.” P4 linked collaboration with transparency by providing evidence for her claims: “You want to show you’re sharing that thought process and it's not all in my head and ‘I’m a magician thinking about stuff’… you’re showing everything you’re doing, and sharing that, and it's a joint understanding.” She further noted that this transparency applied to parents: You’re becoming a team with the parent rather than this special person that knows their child and does these special magic things with them. I think it’s good to be really transparent with the parent then you can find out what things don’t work as well.
By working in a “team,” parents could provide information about how best to work with YP and avoid strategies that “don’t work as well,” contributing to intervention effectiveness.
One reason for transparency was that, “for some people… working in this way [CBT] is just not normal” (P4). The novelty of CBT was seen positively, “to actually have these conversations, to break down thoughts, feelings is quite novel to YP… they can quite like doing it” (P1) and “not all of them have ever had the opportunity to stop and think about that” (P2).
Participants considered the importance of YP being motivated. P1 contended that contextual framing could affect motivation, as YP might “feel like the session is some kind of punishment. Imagine the school's like ‘you’re not having detention, you’re having [CBT].’” In contrast, P5 highlighted intrinsic motivation, stating: “There's something about a YP wanting to do it and to make some changes and be motivated to help themselves and to develop some strategies… it's your choice to be here, you have to want to access this.” P5 further described one sign of intrinsic motivation: “Some YP ask for copies of [worksheets], they want to keep them.” According to this participant, another factor supporting motivation involved providing background explanations so YP: understand why they’re using their strategies and somebody is not just saying “take a deep breath” or “go to your calm box”… You’ll typically get a “no” off them at that point because they have no understanding as to why they’re being asked to do that. (P5)
This highlights the tension between practitioners having knowledge of potentially helpful strategies and the need to avoid directing YP's behavior. According to participants, self-understanding precedes and justifies the benefits of behavioral strategies, with P5 observing that “if you don't understand yourself, I’m never sure how you can make changes.” P1 highlighted tensions within YP's attitudes: “Normally if someone's having emotional problems, part of them does want to change but part of them is safe in what they’re doing at the moment, especially with an avoidance behaviour.”
To make content more accessible to YP, P2 described progression from general concepts to personalized examples: “We might start off exploring the fact that thoughts, feelings, and behaviors are linked, and once we’ve got that and been applying that to life, then I might use that as a linking tool, ‘so now specifically with you…’” This participant illustrated how general discussions could be less intense and lead into the more challenging process of self-reflection. However, as noted by P5, some worksheets were effective “because it's one step removed and it's not personal to them. Sometimes doing everything that's personal to you can be difficult.”
Participants were torn on whether it was helpful that TGFG worksheets resembled schoolwork. P5 was positive, stating that “children are used to worksheets anyway, in schools,” whereas P6 was unsure, commenting: “CBT shouldn’t feel like school in my opinion.” Regarding worksheet design, P1 described that images could aid understanding, as “plenty of YP have reading difficulties or are visual learners.” P4 agreed, describing that illustrations such as “negative glasses” acted as “concrete examples,” making challenging concepts feel tangible.
Think Good – Feel Good's public availability brings potential risks and benefits
The TGFG resource is publicly available, meaning it is open to be read and used by anyone regardless of training. Participants discussed potential benefits of recruiting school staff, such as teaching assistants, with no formal CBT training, to use TGFG: toward the end of the book, lots of that could be done in school with my support. The first bit feels as though it needs therapeutic input then the end bit feels as though I could leave those strategies with the school. (P5)
The emotional and cognitive aspects of CBT were considered challenging, therefore prioritized by practitioners, before behavioral elements could be managed in school. However, there are risks of usage by practitioners without formal CBT training. P5 explained that TGFG was promoted by her service to school staff as “structured enough for somebody to pick it up and use it… even if you just read it to a YP”; however, she further noted that, in reality “[school staff] didn’t feel confident enough to use it in that way. Typically, they’d ask me to come in and I would say, ‘well, you’ve got the book’, and they would say ‘no, we’d much rather you come in.’”
This suggests disconnect between practitioners’ confidence that TGFG could be “just read” and school staff's uncertainty. P3 suggested “it might be overwhelming looking at it thinking ‘Oh my God, I’ve got to work through all this,’” suggesting TGFG might appear like a lengthy manual. P2 noted the skills people might lack without formal CBT training, such as “being able to navigate conversations which are emotionally charged,” and systemic support, such as not “receiving supervision.”
Think Good – Feel Good's tangible resources perform therapeutic functions
P1 described the value of content around setting goals and designing behavioral experiments, “with no content at all, just having a chat, you might be sympathetic, but you might not really move anywhere.” Conversation might make someone feel better but not equip them to cope better. P4 agreed: It’s validating for a YP to see you are listening by writing things down together and they can see whether you’ve got it right or wrong ‘cause you might put something down and they think “that’s definitely not what I would have said.” And then you could change it… It gives them a sense of control and agency over the fact that they’ve got a say in what you’re doing. It’s more collaborative when you’re focusing on the worksheet than if you were just talking.
However, this participant went on to further note that there are risks of overly focussing on content: what can happen with CBT is it becomes all about worksheets and the content of what you’re going to do. But I think your relationship with… people like the parent, the child, whoever… that is still really important and sometimes that can be missed because you’re so blinded by all this amazing information and resource… there is this danger of thinking I must do this, this, this… tick it all off.
Moreover, additional resources play a unique role in achieving therapeutic aims: any worksheet is quite containing for both the child and the clinician. You’ve got a piece of paper between you that you’re looking at with boxes around it, and it focuses the session in… rather than it being scary, “what’s this all about?”… ‘cause working with some adult on some random thinking and talking stuff is not the easiest thing to do (P4).
Worksheets appear to provide an external point of joint attention so practitioners and YP do not have to look at each other. Additionally, they are (a) tangible and therefore offer a clear and familiar grounding; (b) structured, offering achievable steps; and (c) helpful for focusing the session on specific things rather than engaging in open-ended conversation.
Discussion
This study explored the experiences of practitioner psychologists in using a CBT workbook (TGFG) when conducting therapeutic work with YP. Interviews were used to produce data with detail and contextualization, expanding upon previous survey-based research (Redburn & Hayes, 2023). The following positions findings in the context of previous research.
A challenging aspect of CBT is building a therapeutic alliance (the relationship between practitioner and YP) as it is often necessary to overcome feelings of apprehension, vulnerability, embarrassment, weakness, and shame relating to the experience of therapy (Dimic et al., 2023). Alliance is among the most important variables in achieving change and is related to positive outcomes, with an average effect size of 0.24 (Castonguay et al., 2006). In the current study, practitioners described how written worksheets supported their formation and development of alliance. In a study by Redburn and Hayes (2023), worksheets were used during sessions by 80% of TGFG users; in addition, 86% of 49 worksheets were specifically named as useful by at least one survey respondent, showing the broad utility of TGFG's resources. Writing things down means they can be seen, aiding transparent communication; YP consider it valuable to feel understood and heard by therapists (Cunningham et al., 2019). If something inaccurate were written, it could be edited, giving YP control and agency, which could in turn promote engagement (Wilmots et al., 2019). Writing also aids memory and facilitates progress reviews because it allows participants in the therapeutic process to reexamine the significance of physical records over time. During the early stages of CBT, YP may feel uncertain about meeting someone new (Dimic et al., 2023); thus, having worksheets (that resemble schoolwork) could feel familiar and promote rapport-building. Worksheets may reduce the emotional intensity of discussing difficult experiences through containment, providing boundaries and clarity rather than inviting open and unpredictable conversations. This structure incorporates the theory of secondary intersubjectivity, wherein two people jointly attend to an object (i.e., the worksheet) and thus develop shared understandings and goals while retaining awareness of each other's feelings, thoughts, and reactions (Bråten & Trevarthen, 1994; Tomasello et al., 2005). A supplementary resource becomes a third, nonhuman participant in the therapeutic space, moderating the stress potentially associated with one-to-one interactions.
Consideration of how TGFG was used elicited broader thoughts about manualized intervention delivery. According to previous research, only 18% of TGFG users read directly from TGFG, with those who had not received formal CBT training being significantly more likely to do so, χ2 (2) = 15.34, p < .001, ϕc = .315 (Redburn & Hayes, 2023). In the present study, some interviewees dismissed manualization as robotic and an approach for less skilled professionals that did not allow for personalization of content or moment-by-moment adaptations within sessions. Others valued TGFG's structure because it helped them feel confident when they were inexperienced, fit their personal preferences, or saved time. These opinions broadly resembled those found in previous research (Addis & Krasnow, 2000), suggesting manuals remain a divisive concept. A third, dynamic perspective suggested that, because TGFG was evidence-based, recommended by colleagues, and gave “permission to be creative” (P4), this increased practitioners’ confidence in their judgment, leading to more flexible and less manualized workbook usage over time.
Practitioners highlighted that YP have different preferences for structure; manualized programs could provide certainty for some but alienate others. These are important considerations for implementation science, demonstrating potentially contradictory influences. For example, how should practitioners who are professionally opposed to manuals work with YP who value structure and predictability? Previous research has found a significant association between CBT practitioners’ negative attitudes toward manuals (perceiving them as threatening their freedom) and less effective outcomes when treating people with chronic fatigue syndrome, with therapists’ attitudes accounting for 21% of the variance in posttreatment fatigue (Wiborg et al., 2012). Experiencing less favorable outcomes might reinforce practitioners’ original beliefs about the value of manuals, further entrenching a negative cycle. Future qualitative research could explore YP's attitudes toward structure and manualization and whether this affects their therapeutic experience.
While many participants in the current study reported personalising resources to improve engagement, some suggested that nonpersonalized resources also play a role. Genericness was associated with distance from personal experience, which could feel safer and easier to engage with. P5 suggested generic worksheets could be interspersed as productive breaks from personal discussions, while P2 described a linear progression from general to personal applications over the course of therapy as trust and rapport developed.
P5 suggested that therapeutic expertise was required to work on cognitive understanding but school staff could implement behavioral strategies, particularly where they are supported by readymade TGFG worksheets. Cognitive worksheets and chapters of TGFG are by far the most-used (compared with resources with emotional or behavioral foci), likely due to the challenging nature of conveying cognitive concepts (Redburn & Hayes, 2023). P5 could be arguing for efficiency—targeting therapeutic expertise at the early, complex stages of CBT—or suggesting strategies would be more successfully implemented by staff because they have longer-term relationships with YP. This interprofessional suggestion is relevant to EPs, who typically have limited time for therapeutic work (Greig et al., 2019). However, P5 reported that school staff felt uncomfortable, despite being told they could read TGFG aloud to YP. While teachers acknowledge the importance of supporting students’ mental health, many feel underequipped to fulfill this responsibility and want training on practical strategies (Shelemy et al., 2019). The interprofessional approach might be effective and efficient but would require training school staff and perhaps providing ongoing supervision. Future research could explore the feasibility of managing this approach for EPs, the acceptability of responsibility for school staff, and whether school staff already use TGFG.
Limitations
Several limitations of this study should be acknowledged. First, given this study's goal of probing practitioners’ varied experiences with TGFG, some questions posed during the interview (such as “whether TGFG missed out on important aspects of CBT like supervision?”) may have been partially leading, which could have created courtesy bias to respond in a certain way (Simmons & Elias, 1994). Additionally, the homogeneity of participant demographics was helpful for analyzing the EP context; however, all participants were from the same Western, Educated, Industrialized, Rich, and Democratic (WEIRD) society (United Kingdom), meaning they likely shared unspoken cultural values and underlying assumptions about therapy, psychology, and myriad other topics (Henrich et al., 2010). The authors acknowledge the limitations of qualitative research for generalizing findings; where tentative claims for generalization are made, the authors do not claim that findings are representative of other societal populations (Lewis et al., 2003).
Practice implications
Although this research was conducted with UK-based EPs, TGFG and other CBT workbooks are available to practitioners worldwide, so practice implications are of international relevance. It should be acknowledged that the current study did not attempt to define best practice but rather sought to inductively explore the current state of practice. Thus, the following implications are offered tentatively in the spirit of inspiring practitioners to reflect upon their practice.
First, practitioners may benefit from using worksheet resources to their broad potential. Worksheets are familiar to YP from school and thus can be used to build rapport in the early stages of CBT. Worksheets also encourage collaboration and involvement from YP and facilitate shared understanding through tangible recording and editing of ideas. Moreover, these tools may reduce the emotional intensity of direct conversation through providing boundaries and a sense of progress. This is not to say that worksheets are considered universally positive; for some YP, worksheets might make CBT feel like an unengaging, academic exercise, thereby reducing motivation. Ultimately, it is practitioners’ responsibility to judge whether YP would benefit from something familiar (such as a worksheet) or something more stimulating (such as a video or game).
Second, practitioners who are less experienced may benefit from using workbooks like TGFG, as the structure and range of content can support self-confidence. Over time, many practitioners learn to adapt the structure and content. However, it remains important for practitioners to account for YP's preferences regarding structure versus flexibility and to adapt intervention delivery accordingly.
Third, practitioners should consider the possibility of interprofessional collaboration with school staff. Practitioners could deliver more complex therapeutic content before passing on follow-up resources to school staff, capitalizing on their own expertise while also leveraging school staff's increased availability and preexisting rapport with YP. However, it is vital to consider which types of content are comfortable and appropriate for staff to deliver, given their lack of formal CBT training.
Conclusion
This study explored practitioners’ experiences with a CBT workbook (TGFG). The findings suggest several practical implications for practitioner psychologists. Think Good – Feel Good provides benefits including planning support, revision of CBT concepts, emotional reassurance, adaptable resources, and text to read aloud directly. Think Good – Feel Good could facilitate pragmatic approaches incorporating other therapeutic modalities, due to its accessible and flexible nature. Supplementary resources could support the formation and development of therapeutic alliance. Workbook resources may facilitate transparent communication, enabling YP to see their own and practitioners’ developing thinking and to exert control through editing what gets written down. They may also provide an external point of joint attention, containing the emotional intensity of challenging discussions. Notably, TGFG is unlikely to feel accessible to school staff without prior training. Nonetheless, there is potential for efficient and effective interprofessional collaboration where psychologists might cover the more complex cognitive underpinnings of CBT before entrusting practical behavioral strategies to preexisting, established relationships between YP and school staff.
Footnotes
Consent to participate
Written informed consent was obtained from all participants in this study.
Consent for publication
Informed consent for publication was provided by the participants.
Data availability statement
The data are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
This study was approved by the University College London ethics committee (Approval ID: 18753/001).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author biographies
Appendix A
Appendix A—Interview Schedule [italicized questions were posed to all participants; non-italicized questions were follow-up probes based on previous discussion]
Introduction statement:
Thank you for agreeing to take part in this research project. The purpose of the project is to explore how mental health practitioners use the CBT workbook, “Think Good – Feel Good,” and what happens between practitioners and children and YP to bring about positive therapeutic change.
This interview will be recorded and transcribed but everything you say will be kept confidential and will be pseudonymized when the data is analyzed, so your name will be replaced by “Participant X.” When I transcribe the recording any mention of names or any other potentially identifying information will be pseudonymized. After I have transcribed the recording it will be deleted. You can choose to withdraw your data at any point until it is transcribed without providing a reason. The transcript won’t be shared with anyone until it has been pseudonymized.
Please feel free to ask for repetition or clarification of any questions I ask. During the interview, we may talk about mental health of children and YP you have worked with, as well as your feelings and identity as a mental health practitioner. Please only share information that you feel comfortable with and do not feel that you have to answer all the questions that I ask.
The interview today should last between half an hour and one hour. Would you like me to clarify anything or ask any questions before we start?
Opening question: Could you tell me about your experience working in children's mental health?
What kind of CBT training have you had?
What client group do you work with?
When did you start working in children's mental health? What are some of the reasons you wanted to work in children's mental health? Do you enjoy working in children's mental health?
Do you also make use of the clinician's guide? If so, how?
How/when do you choose to use TGFG?
When did you first use TGFG? How did you come across TGFG? Are you still using TGFG? Which edition? [see Demographics Form first] How often do you use TGFG? If you could define TGFG in one sentence, what would you say? Do you use worksheets? How? Do you adapt them? Do you use them within the session or for homework?
Do you use the TGFG workbook to plan your sessions?
Do you make reference to characters (go getter, feelings finder, thought tracker)? Do you read directly from TGFG during sessions? Does the Clinician's Guide help with your planning or reflection?
Do you feel it is helpful/necessary to adapt the worksheets to be more engaging?
Are the things YP find engaging also the things that you, as a practitioner, feel are most helpful for the process of therapeutic change?
If not, are the engaging aspects of TGFG distracting for YP in terms of achieving positive therapeutic change?
How do you get YP to engage with TGFG?
Do you think it is more about the actual content of TGFG (e.g., worksheets) or the way content is delivered that YP find engaging? Worksheets? Characters? Listening to psychoeducation?
Does TGFG reduce any anxieties you may have as a practitioner?
Are there any crucial aspects of the CBT process that are not addressed by TGFG? In terms of support for the practitioner, such as self-care or supervision?
Would you find it helpful for TGFG to have sections or chapters addressing the challenges associated with being a practitioner? Does TGFG boost your confidence as a practitioner? Do you ever feel overwhelmed, given the huge number of resources in TGFG? Do you ever feel restricted when using the workbook or worksheets, to do them as you’re advised by the workbook? Would you prefer that the workbook guided or structured your thinking more in terms of how to run a course of CBT or which areas to focus on? Do you trust that the contents of the TGFG workbook are structured in a helpful way?
Would implementing a manualized approach to CBT, with a predefined structure, feel different from using TGFG?
More confident/less anxious? More restrictive?
Have you used other forms of media (e.g., comic stories, explanatory videos, movie clips) in CBT with YP? What was your experience of that?
What would make you not use TGFG or choose an alternative way to plan/deliver CBT? Have you heard of CBT manuals and could you define what a CBT manual is? Have you used a CBT manual before, for example, “Coping Cat”? If so, how did your experience of that differ from your experience of TGFG? Do you always use worksheets or extra resources when working with YP?
Question 1: Thinking about the “Think Good Feel Good” (TGFG) workbook now, how would you typically use the workbook in your practice?
Question 2: Which aspects of TGFG help you, as a practitioner, to deliver effective mental health support to children and young people (YP)?
Question 3: That question was about what helps you as a practitioner. Which aspects of TGFG do YP find engaging?
Question 4: On a more personal level, is there anything about TGFG that supports you as a mental health practitioner, in terms of your confidence or identity for example?
Question 5: How is TGFG similar or different from other ways of delivering CBT?
Question 6: Thinking back over all aspects of our discussion so far, could you pick out one main reason why you continue using TGFG OR why you kept using TGFG OR why you stopped using TGFG? [depending on practitioner's situation]
Closing question: Is there anything else you would like to say about TGFG and/or the process of delivering CBT to YP?
Closing statement:
Thank you very much for taking part in this interview, I really appreciate your opinions. If you are interested, I can send you a summary of the findings of the research when the project ends. Thank you very much for your time.