
Abstract
Resilience comprises positive adaptation to stress and has been extensively studied in the context of breast cancer. Nevertheless, specific experiences of breast cancer survivors in relation to resilience are unknown. The aim of this study was to explore the diverse experiences of important resilience aspects in breast cancer survivors. We conducted semi-structured interviews with 25 breast cancer survivors residing in Sweden. We used thematic analysis to analyze the data. We identified three themes relevant for resilience, each containing several subthemes: “I will try to keep the spirits up”: Struggling with agency in the face of uncontrollability, “You know that you are not alone”: Social support and collective survivorship for better and for worse, and “I try to leave that behind me”: Conceptualizing cancer as a closed chapter or a constant. Thus, having agency in relation to one’s thoughts, feelings, treatment, health, and daily functioning, having support from others, and conceptualizing breast cancer as a closed chapter were interpreted as important aspects of resilience.
Plain Language Summary
Breast cancer diagnosis and treatment can be physically and psychologically stressful. Women have different ways of coping with these experiences and are thus affected to a varying extent. Whereas some women manage to maintain their wellbeing, others experience depression and anxiety, among other problems. The former group of women can be labeled as resilient. Resilience refers to the ability to maintain high wellbeing in face of adverse life events. However, it is unclear what the specific aspects of resilience are when handling breast cancer. The aim of this study was to illuminate this question by exploring the specific experiences of breast cancer survivors which may be relevant for resilient handling of breast cancer. We conducted interviews with 25 women to address this aim. We found that there are three main aspects relevant for resilience in the context of breast cancer. First, feeling in control of one’s emotions, thoughts, health, treatment, and everyday life was found to be an important aspect of resilience. Second, we found that it is important to have social support in form of close family members, friends, but also other women who previously went through, or are currently going through the same experiences. Third, conceptualizing breast cancer as a closed chapter helped women to move on from their breast cancer. These findings give specific clues as to the aspects which should be encouraged in women with breast cancer in order to help them cope. These findings should be replicated with quantitative methods and other cultural contexts.
Breast cancer is the most common type of cancer among women in Sweden (Swedish Cancer Registry, 2019) and getting the diagnosis can be a life-changing event. It can give rise to feelings of anger, shock, and fear, as well as changes in life expectations, perceptions of the future, will to live, but also an increased awareness of values and finding unknown strength (Beatty et al., 2008; Landmark et al., 2001; Landmark & Wahl, 2002). This has led research to shift focus from short-term outcomes toward examining the long-term psychosocial components of breast cancer-related experiences. Such studies show that screening for breast cancer, receiving the diagnosis, treatment, survivorship, and end-of-life care are uniquely stressful experiences that can affect not only physical wellbeing, but also psychological wellbeing and quality of life after the treatment has been completed (Mohlin et al., 2021; Molina et al., 2014). Nevertheless, there is variability in the experiences that breast cancer survivors report. While some studies report experiences of emotional distress, depression and feeling helpless (Beatty et al., 2008), other studies show increased perception of own strength (Landmark & Wahl, 2002). There is evidently a variation in the extent to which women experience negative versus positive emotions, thoughts, and experiences when handling their breast cancer. Thus, some women seem to exhibit more resilient responses than others. Still, it is unclear what resilience represents in the context of breast cancer. The focus of this study is to explore the lived experiences and aspects of resilience in women who once had breast cancer.
Psychological Resilience and Agency
Resilience is commonly defined as positive adaptation in face of significant adversity (Fletcher & Sarkar, 2013). Given that living with breast cancer consists of several significantly adverse events, exhibiting resilience is of great relevance in this context. Nevertheless, researchers on resilience still debate what gives rise to a resilient response to a stressful event. Recently, several models of resilience have been proposed, consisting of a combination of personality-related and social factors and processes (Li et al., 2021; Seiler & Jenewein, 2019; Ye et al., 2017). Moreover, some authors have focused on biological markers of resilience, including changes in neural circuits and molecular pathways and neurotransmiters (Feder et al., 2009). These studies thus suggest an interplay of a multitude of factors that comprise resilience, which may be more or less susceptible to change with psychosocial interventions.
Similarly, there is a great variability in the literature with regards to the aspects of resilience relevant for handling cancer-related events. Resilience seems to be an important determinant of quality of life outcomes in cancer patients and should thus be promoted (Eicher et al., 2015). However, to promote resilience, we need to understand the lived experiences of dealing with breast cancer. A few qualitative studies have investigated aspects of resilience in breast cancer patients and survivors. In these studies, authors have identified aspects such as hope for rehabilitation (Zhang et al., 2018), hardiness (Pieters, 2016; Zhang et al., 2018), optimism (Kennedy & Rollins, 2016; Pieters, 2016; Zhang et al., 2018), gratitude (Zhang et al., 2018), living in the present (Lam et al., 2017), social support (Guruge et al., 2011; Lam et al., 2017; Pieters, 2016), spirituality, and pragmatism (Kennedy & Rollins, 2016). Drawing on research on general and cancer-specific resilience, resilience can usefully be understood as a set of dynamic personal and interpersonal qualities, resources, and processes which may help one cope with breast cancer-related experiences.
A concept which could be useful to better understand resilience in breast cancer is agency. Agency is a concept theorized as intentionally handling one’s life circumstances and functioning (Bandura, 2006). As such, agency is closely related to the experiences of mastery, that is, perceived control over outcomes (Pearlin & Schooler, 1978) and perceived self-efficacy, that is, one’s ability to exert control over one’s functioning and circumstances (Ajzen, 2006). Mastery and agency thus relate to one’s ability to control outcomes, whereas optimism relates to one’s expectations of positive outcomes, regardless of one’s ability to control them (Serpentini et al., 2019). Both optimism and mastery have been found to predict successful coping and health (Serpentini et al., 2019). Optimism has been cited as one of components of resilience (Ong et al., 2006), whereas agency has not been explored in relation to resilience. New models of cancer care incorporate viewing the patient as an agent in handling their psychosocial and physical challenges (Serpentini et al., 2019) and restoring agency has been characterized as crucial in recovery from illness (Lysaker & Leonhardt, 2012). This paper explores the role of agency for resilience in women who had breast cancer.
Investigating Resilience in Oncology Populations
A recent review by Tan et al. (2019) concluded that resilience was poorly defined in previous qualitative studies, resulting in great heterogeneity in resilience literature, which gives way to ambiguity in our understanding of resilience. In addition, very few studies included experiences of survivors with different, good and poor, wellbeing trajectories. One exception is a qualitative study by Lam et al. (2017) which investigated meanings of illness among women with breast cancer with transient or low distress and those with persistent distress. They found that women with high distress experienced biased information processing, thought suppression, demoralization, and pre-existing distress, whereas those with low or transient distress described acceptance, taking charge of the illness, and good social support. The results of this study indicate that women with low and those with high distress may exhibit different responses and strategies when coping with their illness.
Given the complexity of the construct and the ambiguity in how researchers, as well as study participants, conceptualize resilience, exploring resilience in the context of breast cancer can be difficult. One way of dealing with such difficulty in qualitative studies is to be as open and explorative as possible. This could include a focus on highlighting the phenomenon from different perspectives by exploring as much variability in the experiences as possible while simultaneously attending to core aspects (Levitt, 2021). Maximizing variation can happen in different ways, for example by seeking diversity in participants characteristics.
Like Lam et al. (2017), we therefore aimed to obtain a high variation in our sample by recruiting participants that scored high and low on the Connor-Davidson Resilience Scale (CD-RISC; Connor & Davidson, 2003). CD-RISC is the most reliable and well used scale for assessing resilience as a set of characteristics that enable one to handle stress and has been consistently associated with higher quality of life among breast cancer patients cross-sectionally (Harms et al., 2019; Ristevska-Dimitrovska et al., 2015) and longitudinally (Mohlin et al., 2021). While CD-RISC seems to be a good predictor of distress in this population and a useful tool for screening patients who may need additional psychosocial support, it is unclear how experiences of women who score low versus high on the scale may differ. Understanding these differences would bring attention to specific areas that should be targeted when providing support. To the best of our knowledge, no qualitative studies thus far explored aspects of resilience in such a manner.
Therefore, the aim of this study was to explore the lived experiences of women who once had breast cancer, focusing on how they have experienced important aspects of resilience, with a specific emphasis on their experiences from diagnosis to the present day.
Methods
This qualitative interview study was conducted as a follow-up to a quantitative study named SCAN-B Resilience (Axelsson et al., 2018), which aims to investigate the relationship between resilience as measured by CD-RISC and health-related quality of life in breast cancer patients in southern Sweden. The whole project, including this study, has been approved by the ethical review authority (Dnr 2009/658, 2010/383, 2012/58, 2013/459, 2015/277, 2015/522, 2016/944, 2017/88, 2017/875, 2019-00700, 2019-01351, 2020-05492).
Procedure and Participants
We utilized purposive sampling in this study. After reviewing the quantitative results from the larger project, we asked women who scored either very high (Mean + 2SD) or very low (Mean – 2SD) on CD-RISC at the time of diagnosis to participate in semi-structured interviews. Our aim of inviting participants with such large differences in their resilience scores was to maximize the variation in experiences and descriptions of resilience in order to highlight core aspects of resilience (Levitt, 2021). By finding similarities and differences in the data, key areas where interventions may be needed can be identified (Lindsay, 2019).
In addition to high or low scores on CD-RISC, other inclusion criteria for the study were having completed treatment at least 6 months prior, in order to also be able to cover the extended survivorship phase, that is, the phase that begins after formal treatment (Mullan, 1985), and not having a second primary cancer diagnosis or cancer recurrence.
A total of 83 women (equal distribution of low and high resilient) were contacted via letters, which explained the aims of the interview study and the content of interviews. Of these, 34 initially agreed and signed the consent form. Nine women dropped out at a later stage due to scheduling difficulties.
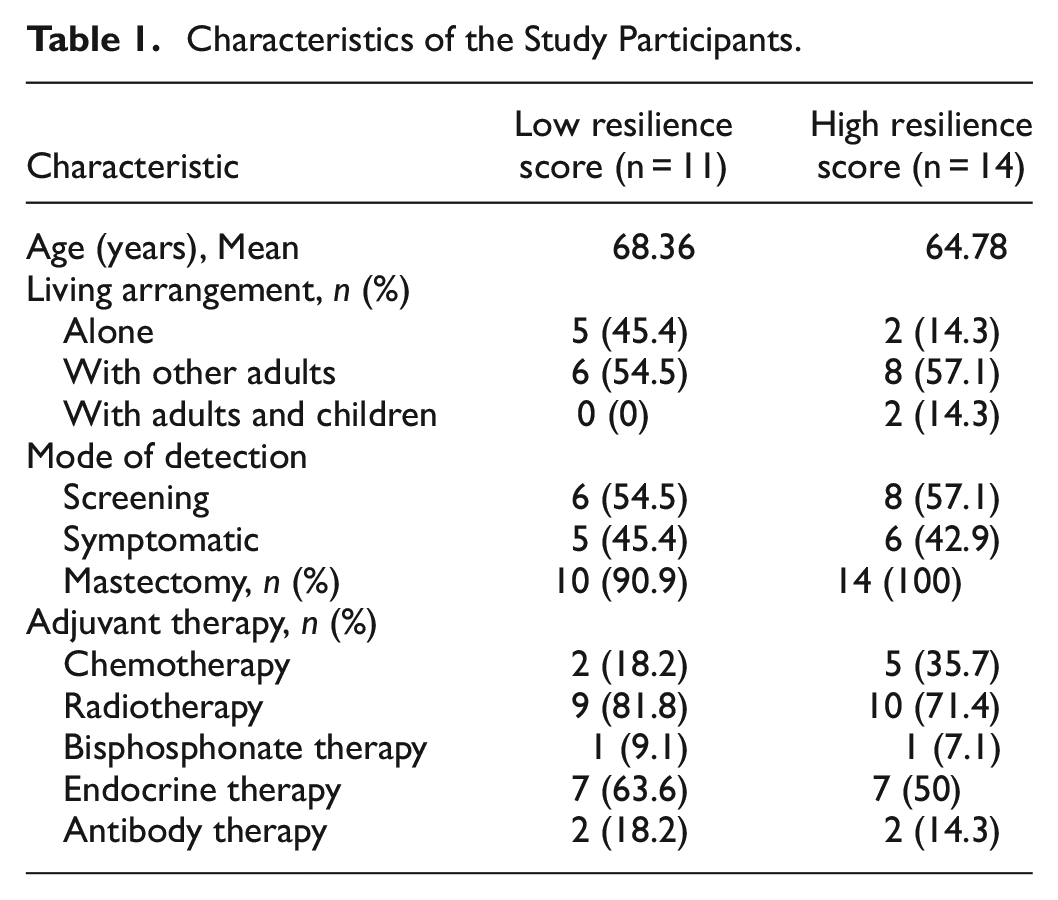
In the end, 25 women residing in southern Sweden participated in the study, consistent with methodologically and thematically similar studies in the field (e.g., Bridges et al., 2015; Carlson et al., 2022; Tod et al., 2008). Data collection lasted between February and June 2021. Clinical and socio-demographic characteristics of study participants are presented in Table 1. Of the 25 participants, 14 women had a high CD-RISC score at diagnosis (Range 88–100; Mean = 92.71), and 11 had a low score (Range 33–50, Mean = 42.82). Clinically, the majority of women had received a combination of mastectomy and adjuvant therapy. The socio-demographic and clinical characteristics of interviewees in both high and low resilience groups were deemed comparable (Table 1), with the exception of living arrangement. However, it is not surprising that the women with a high resilience score lived with other adults to a higher degree than those with low resilience score, as having social support in form of close others is a part of resilience.
Characteristics of the Study Participants.
Two of the authors, PJ and JM, who are licensed clinical psychologists, conducted semi-structured in-depth interviews with participants by telephone. Telephone interviews were chosen as the study was conducted during the COVID-19 pandemic and participants were deemed as a particularly vulnerable group due to their age and health. Telephone interviews were found to be a viable method for collecting rich narrative data (Drabble et al., 2016). Interviews lasted between 20 and 53 min. Interviewers were blind to the CD-RISC score of the interviewees. The interview guide followed the psychosocial definition of survivorship as a process starting from diagnosis until the end of life (Zebrack, 2000), covering the stages of diagnosis, treatment, and post-treatment. Interview questions were open-ended and related to women’s experiences from screening to the present day, as well as the ways in which women reasoned about their experiences and what they did to handle them. Questions included for example, “How did you find out you had breast cancer?,”“Can you tell me what you did when you received the diagnosis,”“How did you feel during the treatment period?” and “Has your life changed, as compared to before diagnosis? In what way?.” Interviews were audio recorded and transcribed verbatim. In this process, all potentially identifying information was anonymized.
Analysis
We analyzed the transcripts using reflexive thematic analysis (Braun & Clarke, 2023), as it can be used to extract shared meanings and experiences across a data set, but also note the differences between participants (i.e., those with a lower and higher score on resilience). In analyzing the data, we utilized a critical realist perspective (Jackson, 2016), acknowledging the interpretative, subjective, and contextual nature of human meaning-making of lived reality as well as the interpretative features of our analysis. In the analysis, this meant trying to attend to the unique texture in each participants’ descriptions as well as analyzing more general themes underlying all participants’ different experiences.
When it comes to the interpretative aspects of our analysis, the transcripts were first analyzed by KV, who first read the transcripts to get familiarized with the data, and then coded the transcripts whilst being blind to the CD-RISC scores using inductive codes, in accordance with Braun and Clarke’s (2023) two first steps. In accordance with step three and four in reflexive thematic analysis, initial themes and subthemes were then derived, by comparing and contrasting the codes depending on the resilience scores. Subsequently all the authors reviewed the data codes, themes, and subthemes. This process was repeated until we obtained consensus on emerging themes and subthemes, according to step five in reflexive thematic analysis. Finally, the themes were defined, named and written up.
Results
We identified three themes, (1) “I will try to keep the spirits up”: Struggling with agency in the face of uncontrollability; (2) “You know that you are not alone”: Social support and collective survivorship for better and for worse; and (3) “I try to leave that behind me”: Conceptualizing cancer as a closed chapter or a constant. Each theme was identified both in women with high and those with low resilience scores. However, the expression of the themes and subthemes differed, which gives nuance to what constituted experiences and aspects of resilience in relation to breast cancer. The themes with relevant subthemes are presented in Table 2.
Themes and Subthemes.

“I Will Try to Keep the Spirits Up”: Struggling With Agency in the Face of Uncontrollability
Living with breast cancer was described as uncontrollable by all participants. One participant described the feeling of just having to submit to the course of the illness and not knowing where it will take you: It is precisely as if we just hop on the bus and ride along, we have no choice. And then, when everything is over, when we get off, then we are completely… Then we don’t know where we are anymore. (I16, low resilience score).
At the same time, many described how they were struggling with agency in relation to the uncontrollable and unpredictable aspects of cancer. This included being able to actively engage in everyday life and relate to thoughts, emotions as well as the illness itself. The notion of agency thus permeated every aspect of the experiences of women; from managing their treatment, wellbeing, and daily routines during treatment, to handling their thoughts and feelings arising throughout. Having, or not having, agency thus appeared to be a defining element of how the women reflected the experience of having breast cancer, where those who expressed more agency seemed to have more resilient score profiles. The theme of agency consisted of four subthemes related to different elements of their experiences.
Navigating Uncertainty When Cancer is the Agent
Breast cancer can be invisible and unpredictable in many ways. A person can have breast cancer without having any symptoms, or discover a lump in the breast that is harmless. One can have breast cancer once, or the cancer can come back again, in the same place or elsewhere in the body. These aspects of cancer as uncontrollable were described by all participants. As such, a woman can have no agency over the invisible enemy, as cancer is being the agent. This uncertainty of breast cancer, for example not being able to influence or predict the result of a mammography check-up, shaped women’s emotional experiences and thoughts. Being put in a position with no agency in relation to the illness lent itself to intense worry and anxiety. Women felt helpless waiting for the results, allowing their thoughts to go uncontrolled, fearing the worst and hoping for the best: I was more affected during the waiting time, so when one goes and waits for it, it was in the summer too so it was obviously difficult to unwind, because not knowing is almost worse or it is terrible to say that maybe but it is the worst, not knowing, I think, when one goes and ponders all the thoughts before one knows what one should do. (I11, high resilience score)
The “not knowing” whether they had breast cancer or not was uncomfortable, worrisome, and sometimes worse than the treatment itself. This was the case in the period between discovering a lump in the breast or being called for additional tests after screening and receiving the diagnosis.
A frightening aspect of cancer is that it can also come back, in the same location, or elsewhere in the body. Not having agency over a relapse of cancer shaped women’s experiences post-treatment. The time of the year when a yearly mammography check-up is due is thus highly stressful in its uncertainty, for women across the resilience score spectrum: Every Christmas, like, that’s when it begins, then the thoughts come because then I know that I will be called again in January for another mammography, and that before one gets the results, there it takes one week or two weeks, like the last time, so that time is horrible and it was hard before, but now it is like, come on, why am I not getting the results, or am I going into this again? (I9, low resilience score)
Being called back for a check-up creates anxiety and takes their thoughts back to the beginning of the breast cancer journey. As a result of their experience, women are more sensitive to warning signs of cancer: “as you feel something maybe not only in the breast but somewhere else so thoughts come directly [that it might be cancer].” (I5, high resilience score)
To conclude, navigating uncertainty when cancer is the agent was hard for all participants, irrespective of resilience scores. However, while agency was compromised by cancer, several participants felt they could exercise some kind of agency in relation to other aspects of their life, as described next.
Maintaining Normalcy to be Able to Deal With Illness
Breast cancer can be very disruptive, bringing one’s everyday routines to a halt. It can also permanently change the way one looks and functions. Normalcy can thus be taken away from women with breast cancer, and maintaining normalcy becomes both a priority and challenge. Having a sense of agency in relation to their daily functioning helped women maintain normalcy during the breast cancer experience. Women perceived looking normal, maintaining normal activities throughout treatment, and return to normalcy after treatment, as some of the main needs throughout the experience. Several participants highlighted the importance of being able “to start working normally again […] maybe not work fulltime, but halftime at least, I wanted to work” (I16, low resilience score) to maintain a sense of normalcy. Others described how maintaining normalcy was also something that happened in relation to others: The nice thing was that no one ever treated me as ill but they treated me “as usual” and I appreciated that very much[…] they asked how I felt of course, […] but we talked about work as usual and, ehh, I didn’t think so much about me being ill. (I11, high resilience score)
The importance of maintaining normalcy was described by all participants irrespective of resilience scores. However, fulfilling this need seemed to rely on whether the participants viewed themselves as having agency in relation to their everyday routines and functioning when handling the disruptions caused by breast cancer, or not. Women with high resilience scores were interpreted as able to maintain normalcy during and after treatment to a greater extent. They did so either by maintaining normal activities and routines or by adapting their routines to the new demands of breast cancer treatment.
They described themselves as being flexible in making changes in their hobbies and routines, for example by lowering the tempo of physical activity or incorporating chemotherapy or radiotherapy schedules into their existing routines. One participant gave an illustrative example of how she dealt with exercise during this time: I had to give up the thought that I would be able to begin yoga directly, but perhaps I can only sit here and breathe, I can maybe only sit and meditate. Maybe I only get to go around the house with the dogs like, before I get started again. (I17, high resilience score)
Disruptions in normalcy, on the other hand, seemed to have occurred in women with low resilience scores who described not being able to handle the changes that arose as a result of their breast cancer. As breast cancer encompasses temporary or permanent bodily changes such as losing hair after chemotherapy and removal of the breast following a mastectomy, many said they struggled to cope with these bodily changes. This negatively affected their ability to continue with regular routines and activities they used to enjoy, for example going swimming, and prevented them from maintaining normalcy: I tried to live as usual. It was of course a little difficult when I had the breast removed, to learn how to, like, be normal again […] we used to, for example, bathe in the sauna, but I said no, I thought, I don’t want that because, no, people are naked in the shower. So yes, there were many things that I didn’t do which I did before [the surgery][…] [because] that can of course affect people negatively, to see someone [like me] who looks like that, so I didn’t like my body that much. (I14, low resilience score)
Thus, although all women felt the need to look, feel, and function normally, the ability to meet those needs depended on whether they viewed themselves as able to handle the disruptions caused by breast cancer or not.
Exercising Agency in Relation to Thoughts and Feelings
Immediately at diagnosis, most women experienced intense feelings, including fear, anger, sadness, and shock. However, emotions are temporary and after this initial reaction and once the treatment begins, one’s experience of agency in relation to emotions and thoughts becomes an important aspect of handling breast cancer. Unlike the illness itself, some of the participants described that they had agency in relation to their inner experiences, such as their feelings and thoughts, and thus could keep a positive attitude: “I am in essence a positive and strong person, so I decided early that now it is me who needs to handle the whole process and I will try to keep the spirits up.” (I2, high resilience score). This way of exercising agency was typically described by those with high resilience scores. Being able to exercise agency in relation to one’s emotions and thoughts was described as preventing overwhelming feelings of anxiety and worry. Feelings of excessive worrying about the outcome of treatment was also understood as useless, as it is out of their control, and would only make them feel even worse. Instead, they put effort into thinking positively and being optimistic in relation to the outcome: It is about looking ahead and so, you can’t bring yourself down, because if you do then it gets even worse, and you become ill in a whole different way. I am not the kind of person who brings myself down so much, I can of course also feel depressed, but not in that way. (I4, high resilience score)
Exercising this kind of agency helped these participants view themselves as strong individuals who can successfully cope with adversity.
In contrast, several participants described not being able to exercise agency in relation to their thoughts and feelings which led to experiencing a more intense and persistent fear that was harder to manage and contain. Uncontrolled, thoughts can spiral and present themselves in a form of rumination about the experiences related to breast cancer: When everything was over after three weeks in [city of treatment], then I know that everything was repeating in my head, like every detail from the first mammography until the last visit there in [city of treatment] and the return visit to the nurse who would take a look at my wounds […] all the details were repeating in my head time and time again. (I12, low resilience score)
In addition, some women even described feeling disconnected from the experience of diagnosis and treatment: “like it wasn’t happening to me” (I10, low resilience score). These descriptions were more present among women with low resilience scores and manifested themselves in pervasive mental images of treatment procedures, or thoughts that they themselves might have caused the illness, for example by taking hormone replacement therapy prior to diagnosis. Some women viewed themselves as prone to worrying and dwelling on things, including health-related issues: I adhere to the type of people who, when something happens […] I get a bit scared and ruminate and investigate and, they have also made fun of me at work and called me a hypochondriac even before I got breast cancer […] it was a damn luck I was a hypochondriac then because otherwise I probably wouldn’t have discovered this tumor if I hadn’t been so careful to check myself […] I believe that was actually what saved me. (I3, low resilience score)
Interestingly, some women, like the participant above, also perceived this tendency to worry about health-related issues as an adaptive strategy, as such vigilance had encouraged them to seek help and get diagnosed in time. However, while this vigilance might have helped this participant to act in order to get diagnosed, the same strategy did not seem to help her deal with the illness to the same extent.
Taking Charge of One’s Health
Despite breast cancer itself being uncontrollable and the treatment procedures for breast cancer being strict, taking charge of one’s own experience during treatment was an important aspect of resilience when dealing with breast cancer. While the participants could not control their illness nor the outcome, some described a sense of agency in relation to their overall health and what happened to their body. One participant described this illustratively as “you can’t influence illness, but you can influence everything else.” (I15, high resilience score). This sense of agency was particularly evident for women with high resilience scores and resulted in them proactively making decisions regarding their own treatment and relying on themselves to make those decisions. One participant was offered endocrine therapy as part of her treatment, which is usually recommended to be taken for several years after the formal treatment is completed, but she decided to stop it because it reduced her quality of life: I of course got the pills later but I felt so bad from them that I decided that I would rather feel good during the time I have left then go and suffer and have many side-effects, so I stopped taking them. (I1, high resilience score)
Similarly, many women with high resilience scores pursued actions to improve their wellbeing during treatment and wanted to focus on what they could control.
Women with high resilience scores were able to identify the strategies and resources they relied on to focus on what they could control, whilst handling their breast cancer experience and actively monitoring how they felt. One participant described utilizing strategies for navigating her energy levels and state of being as her “toolbox” for coping: It was my toolbox to select from, which I have talked about with everyone else that they should use when they feel bad and so on. So I only had to apply that to myself […] So like I wanted to know what my strategy would be, how I should behave, when I could go out, when I would have the energy, or when I would be able to do this or that. It was more that type of thinking I had, that I wanted to like find a system which could work in the long run. (I17, high resilience score)
In addition, participants described strategies of resilience as including hobbies, such as reading, knitting, solving a puzzle, meditation, and work, which they utilized to either keep themselves busy, distract their thoughts, or relax. Physical activity was also noted as helpful in maintaining physical and mental wellbeing: I thought, now I have to exercise so that I keep myself healthy […] that was my first thought, it was that I started to exercise more, I exercise either way, but I exercised even more, so I trained very much. (I11, high resilience score)
In contrast, participants with lower resilience scores described feeling that there “is nothing to do about it [but] keeping my fingers crossed that health care will manage to help me” (I13, low resilience score). In other words, they described a more passive role, that of a patient. In these instances, women viewed breast cancer treatment as something that they had to withstand in order to feel better later. They also relied on the opinions of doctors and close relatives to help with making important decisions during treatment: I went into a patient role, I am not one to question things, why are you doing this or why are you doing that or why not but I only, I am a kind person, adaptable […] I just follow along. (I9, low resilience score)
In these cases, trusting others becomes largely important. Not having a doctor that they trusted was experienced as hard, whereas being surrounded by medical staff they trusted was comforting. This was in some cases a challenge, as women in general have little control over who will be treating them: Yes, the thing that helped me was that this doctor at the time whom I didn’t like, he was going on holiday, and so there was another doctor, and I knew him because of my husband and that felt very good that I would be operated on by him […] it resolved itself by there being a staff change there. (I12, low resilience score)
In contrast to the participants who described themselves as being able to act in relation to their health, these participants’ health was described as in someone else’s hands.
“You Know That You Are Not Alone”: Social Support and Collective Survivorship for Better and for Worse
A person does not experience breast cancer in a vacuum. Throughout the process, women are surrounded by others, including close family and friends, hospital staff, and other women who have, or once had, breast cancer. The role of others in handling experiences related to breast cancer is complex. In many ways, sharing experiences with others can have emotional and practical benefits. Conversely, having had earlier experiences of breast cancer in the family and not having close others to talk to can make the experience more challenging. Nevertheless, social support plays an important, yet complex role in resiliently dealing with breast cancer, as highlighted in three subthemes.
Dealing With Illness With or Without Social Support
An important element of handling breast cancer was seeking social support in form of family and friends. This included being open to actively share one’s experiences, thoughts, and feelings with others, which was especially evident in women with high resilience scores. Several participants said that talking to others was a way of making their burden lighter and regulating their thoughts and feelings: I spoke with others and I was very, very open about my breast cancer and that has of course helped me very, very much. So just getting to explain how everything went was very good. That way I could relieve some of the pressure. (I7, high resilience score)
The importance of having close others to talk to is further highlighted by several women with low resilience scores who said that they had no close others to turn to. Many women with breast cancer, especially older women, live alone, which can lead to feeling isolated and lonely in their experience as it is “very difficult to be sick when you are alone, really” (I10, low resilience score). Additionally, perceiving breast cancer as a private matter led to some women not sharing their experience and having to handle their thoughts and feelings on their own: No I didn’t speak so much and we didn’t let many know, we only told our daughters […] And a whole year went by before I told my old work friends […] I think nevertheless that cancer, it is something, no it is not something you tell whomever that you have or do not have. (I12, low resilience score)
While some participants with low resilience scores said that not having close others to talk to also made it a bit easier, because then they did not have to talk about it, most participants agreed that having others to talk to, when needed, was important to deal with illness.
Being “On the Same Bus” With Others With Breast Cancer
The fact that breast cancer is a very common illness among women, especially older women, was described as beneficial in a variety of ways by the participants in handling their experiences. Across the spectrum of resilience scores, knowing that breast cancer is a very common illness was a comforting factor, which helped them “know that you are not alone but so many others suffer from it when you reach this age” (I6, high resilience score). It also helped many that breast cancer was so evident in society as a whole. One participant described how this framed her response to receiving the diagnosis: She felt my breast and then she said like this to me “you have cancer do you understand,” Aah, I said, it is half of the female population that has it soon […] it wasn’t any special feeling, you read about breast cancer in the news every other day and you hear about it on the radio and TV, it is such a common illness so you understand that anyone can get it, so it was nothing special about it. (I8, low resilience score)
Many also found consolation in knowing of other specific women from their social circles who had survived breast cancer. This normalization of breast cancer helped women reduce the fear of breast cancer. Moreover, women found gratitude in knowing that some others had a worse experience compared to theirs.
Women who had had breast cancer earlier also served as an important source of emotional and practical support. The participants described how they had reached out to someone else who once had had breast cancer to seek support, receive information about treatment and its side effects, thus preparing themselves for upcoming treatment: A girl in my network, we had lunch and then she told me how it felt to lose hair and I was prepared for that and it went very quickly when I felt I began to feel the hair was, like, falling off, so then I went and shaved it off at once, and it was also like this, because I could mentally prepare myself so it was easier to handle. (I2, high resilience score)
Women perceived this as a very valuable resource that made all the difference and helped them prepare for future events, both mentally and practically.
Similarly, a sense of community with women who were simultaneously going through the same experience served as an important source of support. Many women had to travel to bigger neighboring towns to receive treatment. They often took the bus (called the “radiation bus” by many participants) organized by the healthcare sector, which transported women with breast cancer from smaller towns to nearby hospitals. Taking the bus together with women in the same position was described as positive, as they could socialize and share experiences with each other becoming “a little family there on the bus” (I9, low resilience score). One participant described: I thought “ohhh to go there for three weeks every day, how boring will that get” but then you could take that bus and we were four-five people in the same situation that we spoke to each other and some days we slept there in the patient hotel and met up when we ate there and talked in the evenings and so. (I6, high resilience score)
Irrespective of resilience scores, the participants highlighted the importance of having a sense of community when coping with illness.
Reliving Past Occurrences of Breast Cancer in the Family
The commonality of breast cancer was nevertheless also interpreted as a double-edged sword, especially for those who have had previous experiences of someone else in the family having had breast cancer. This was evident irrespective of the resilience scores. Having had previous experience of breast cancer in the family was thus understood as complex; although it made the diagnosis seem less unexpected for the participants, it also increased the burden felt by the women in question: My mom had breast cancer when she was about the same age as me so I have lived with breast cancer in my family […] [I have] some frustration about having to go through the same thing again. Because, yes, I have known how everything works, I have known how everything has been during those different chemotherapies that mom got and so, so it was of course nothing new to me. And I have been with mom in all those stages like, during different treatments and different tests and different, like, I have seen her in the bed when she was doing bad, and seen her lose hair in different stages and like all of those bits. So, so it was more like “aha, it was my turn then.” (I17, high resilience score)
Participants described they had to bear the burden of not only their own breast cancer, but also that of their mothers, sisters, and close relatives. Thus, after receiving the diagnosis themselves, they felt that they had to relive the experiences of their close ones. Additionally, women feared that their breast cancer was hereditary and that their daughters and sisters would have to experience the same challenges in the future: I then asked her [the doctor] if this [breast cancer] is something my daughters can get. She said that it is not something that is hereditary, which I thought was a little strange. I still worry that somehow they can get it more easily now, but I am not sure. (I18, low resilience score)
Thus, breast cancer being a shared experience can be both a comforting factor and an additional burden, depending on the nature of the personal relationship.
“I Try to Leave That Behind Me”: Conceptualizing Cancer as a Closed Chapter or a Constant
Breast cancer is an invisible, yet potentially deadly threat that may or may not come back at any point. This is a fact that require participants to relate to cancer. As one woman said: “cancer as a concept has come much closer to me” (I13, low resilience score). The way in which the participants understood cancer seemed to shape their experiences, feelings, and thoughts after treatment. Perceiving cancer as only a closed chapter in the book of life was interpreted to help women move on after treatment and prevent reoccurring negative thoughts and worry. In contrast, perceiving cancer as a constant lurking threat was interpreted as burdening, which seemed to influence other areas of life. Two subthemes were identified in relation to the ways women think about the (non)finality of breast cancer after treatment.
Understanding Cancer as Removed or as Constantly Lurking
Thinking about one’s cancer as cured versus as an illness that may possibly come back or spread elsewhere in the body was interpreted as an important element of handling the breast cancer experience after treatment. Women with a high resilience score described themselves as healthy and that “one has to try and move on from [cancer]” (I11, high resilience score). Many of these women conceptualized breast cancer as having been removed with surgery and all additional treatment being merely preventative: Because then it is a certainty, that I will be able to hang out with my children. It is nothing else, because it is only preventative. The cancer was removed, but then what I went through [additional treatment] was only preventative. (I15, high resilience score)
This way of conceptualizing breast cancer as a threat that has been removed was interpreted as bringing a sense of safety and finality of the experience because this let participants feel that they “didn’t have any cancer left in the body” (I17, high resilience score). This allowed them to close that chapter and move on.
Conversely, other participants described breast cancer as a lurking threat that may come back at any moment. This way of thinking about breast cancer was more present in women with a low resilience score: I always have it at the back of my mind and I examine my breast every day and underarms and everything there and yes it has brought me down mentally […] As soon as I get pain somewhere or feel something strange, I think like “is it something that has spread and appeared somewhere else in the body?” (I3, low resilience score)
Just like this participant, many described a threat of cancer as constantly there, threatening their health. These thoughts become uncontrolled and affect daily functioning, sometimes leading to constant checking for symptoms of cancer. This was interpreted as making it hard for them to move on from cancer.
Returning to Your Normal (Better) Self or as a Weaker Self
Perceiving breast cancer as removed seemed to allow women to contain their experience and move on with their life after treatment. Women with a high resilience score described continuing with their lives as they were before treatment. The thoughts about cancer were described to be replaced by thoughts about everyday activities and experiences: I think that everything is as usual, I try to leave that behind me and we play golf now in this wonderful time of the year. Yes, I don’t know how I would, everything went so well, so there is nothing that seems to have become either worse or better. Life moves on as usual. (I6, high resilience score)
These participants did not experience reoccurring thoughts about cancer and were not occupied worrying about cancer. As such, it seems as though having breast cancer did not become a defining element of their identity. For others with high resilience scores, having breast cancer represented one of their life experiences that they could learn from: You can be only a victim and bring yourself down, or you can rise up and try to make the best of it and see it from another angle and get, get like, how can I say, new tools in your toolbox that you can use […] So I feel that it has only given me more tools, more education, more, eh, how can I say, fighting experience. (I17, high resilience score)
In contrast, having had breast cancer can occupy one’s mind even after treatment and become a more influential part of one’s identity. Worries about cancer and the possibility of it returning can affect other areas of women’s lives. For women with low resilience scores, the reality of having had breast cancer seemed more present in their daily thoughts and feelings. Some said that they experienced more anxiety, brain fog, reoccurring thoughts about cancer, for example: I feel a little more so, brain fog so to speak, I feel [that] has stayed a bit (…) [It’s] difficult to make decisions and focus, many times it is hard to remember things if one doesn’t really try to and decide “okay this I have to remember, I cannot forget this.” (I16, low resilience score).
Of these participants, many described feeling like different people compared to who they were before breast cancer: I am not as psychologically strong as I was before. And I don’t believe I ever will be, because it was a trauma to go through, you feel more vulnerable and fragile […] I get so much anxiety always, I feel that I have anxiety in my body that I haven’t had before, which is permanent. It is there all the time, it is there when I wake up at night, it is there when I wake up in the morning, and it is like cancer-fear, anxiety that I will discover something more myself, or that someone from my family will get sick. No, I don’t believe it will ever calm down, I believe that some people can drop it and leave it behind, […] but not me. (I3, low resilience score)
As this participant describes, several participants described being more vulnerable now than before their cancer diagnoses and that this vulnerability was part of not being able to close the chapter of cancer in their lives.
Discussion
The aim of this study was to explore the lived experiences of important resilience aspects among women who had breast cancer. We focused on obtaining a large variation in resilience scores in our sample to allow for a diverse range of experiences. By doing so, we aimed to pinpoint themes that may reflect resilient responses in a nuanced way. The reflexive thematic analysis resulted in three themes, each containing several subthemes. Some of the subthemes were expressed in the same way among women across the resilience scores spectrum. However, the majority of the subthemes had a different expression depending on the resilience scores of the women. The themes we arrived at can serve as directions for interventions aimed at increasing resilience in women with breast cancer.
The first theme “I will try to keep the spirits up” addressed experiences of agency that women had relating to the illness itself, their thoughts and feelings, maintaining normalcy in their daily functioning, and their body and wellbeing. According to Bandura (2006), agency involves intentionality, which refers to forming intentions to make action plans and ways of executing them. Further, agency requires forethought in setting goals and anticipating likely outcomes of these goals. Then, it involves turning the thoughts into concrete actions. Finally, the core element of agency is reflecting upon one’s actions and thoughts, as well as their adequacy to achieve desired outcomes (Bandura, 2006). The results of this study suggest that resilience in the context of breast cancer may involve acting as an agent throughout the experience. This includes taking charge of one’s treatment procedures, wellbeing, and health. Women with higher resilience scores were interpreted to exhibit intentionality and forethought in performing activities that made them feel better and made proactive decisions regarding their treatment procedures. This further seemed to help them maintain normalcy in their daily functioning, thus fulfilling the need for normalcy that all women had. They also seemed to be able to pinpoint different strategies they used to achieve desired outcomes, exhibiting a sense of self-reflection and self-reactivity. Some of these strategies included physical activity, various hobbies, and meditation. Physical activity and meditation have previously been linked with both mental health (Lynch et al., 2018; Paluska & Schwenk, 2000) and physical health (Warburton et al., 2006). Maintaining normalcy was found as an important aspect of resilience in a previous study conducted in Norway (Haug et al., 2015).
Furthermore, acting as an agent in this context also seemed to involve regulation of thoughts and emotions, that is, directing them in accordance with the outcomes they wished to achieve. Women on the higher end of the resilience scores spectrum expressed being able to keep their negative emotions at bay. They perceived themselves as positive and strong, and described worrying as useless as breast cancer itself is outside of one’s control. Positivity and strength have previously been identified as constituents of resilience in breast cancer survivors (Pieters, 2016; Zhang et al., 2018). In contrast, not having agency in relation to one’s emotions seemed to be connected to lingering worry, as well as rumination and self-blame. These cognitive emotion regulation strategies have previously been described as maladaptive, as they are associated with depressive and anxiety symptoms (Garnefski et al., 2001).
However, there are elements of the breast cancer experience relating to which women seemed to have no agency. This refers to the illness itself, which is unpredictable. According to Bandura, people do not act as autonomous agents, but depend on situational circumstances (2006). Having no agency over the diagnosis and possibility of relapse was interpreted as having given rise to distress and anxiety, regardless of the resilience scores. This is in line with previous quantitative and qualitative research, which has shown that women experience strong negative emotions (Doré et al., 2013) and anxiety (Montgomery & McCrone, 2010) while waiting for a diagnosis, which may be more stressful than diagnostic procedures themselves (Flory & Lang, 2011). Some estimations are that 51% of women are moderately or highly anxious at the prediagnostic stage (Pineault, 2007). After finding a lump or an abnormality on a mammogram, women usually feel stunned and have to control distress during the waiting period (Morse et al., 2014). Fear of cancer recurrence also has a substantial prevalence, negatively affects quality of life in all types of cancer (Crist & Grunfeld, 2013; Simonelli et al., 2017), and is associated with higher levels of depression in breast cancer survivors (Koch et al., 2014).
Nevertheless, it is difficult to discern the causality between resilience and expressions of agency we arrived at in the study. It is unclear whether women might be resilient because they are acting as agents, or whether resilience might cause them to act as agents relating to their breast cancer experiences. To be able to draw such conclusions, quantitative research is needed. A concept of health locus of control (HLoC) might be a useful concept when discussing agency relating to one’s breast cancer. HLoC refers to individual beliefs about whether internal or external factors control one’s health (Norman & Bennett, 1996). Internal HLoC is the belief that the individuals themselves can affect their health, whereas external HLoC refers to the belief that health is within the control of external factors, namely “powerful others” and “chance” (Devin et al., 2012). In the case of women who had breast cancer, powerful others may refer to medical staff. Having external HLoC may thus reflect taking on a more passive role in treatment, which is likely if one does not have agency relating to their health and treatment procedures. Internal HLoC has been associated with positive psychological and behavioral outcomes, whereas external was found to predict loneliness and helplessness (Stenström & Andersson, 2000), as well as burnout (França et al., 2012). To the best of our knowledge, HLoC has not been previously investigated in relation to resilience.
The second theme in the study, “You Know that You are not Alone,” reflects the complexity of the role of others in the context of breast cancer. Others played a role in women’s experiences indirectly and directly. More directly, social support in form of close family members and friends and openness to share their experiences was an important aspect of resilience in this context. Social support has been consistently found as one of the aspects of resilience (Guruge et al., 2011; Lam et al., 2017; Pieters, 2016), highlighting the need to reconceptualize resilience as a set of not only internal, but also external resources. This is also in line with previous research conducted in the Nordic region. In two studies from Norway, having close relationships was found as a crucial component of resilience among older cancer patients (Haug et al., 2015, 2016). In a study conducted in Denmark with breast cancer patients, having a supportive partner and family was highlighted as crucial to cope with the disease (Lee Mortensen et al., 2018). Most women who get breast cancer in Sweden are older than 65, including the women interviewed for this study. Many of these women live alone and have adult children who do not live in the same town. This highlights the need for providing a support network to these women, which may include access to psychologists and, perhaps more importantly, support groups. It also highlights the need to encourage women to share their experience with others and to normalize breast cancer in the general population even further, so that sharing becomes easier.
Indirectly, the notion of breast cancer being the most common type of cancer among women in Sweden (Swedish Cancer Registry, 2019) facilitates its normalization in the general public. This normalization of breast cancer helps women to reconceptualize breast cancer from a rare and frightening disease to an illness that many go through and overcome. It also helped them feel less isolated, but a part of a bigger group of women who had to go through the same experiences. Another direct way others play a role in breast cancer is having other women who have or previously had breast cancer as a valuable resource. Most women knew someone who previously had breast cancer and they considered speaking to them as highly helpful, both practically and emotionally. Women who were going through treatment at the same time were another valuable resource. Enabling the situations for women with breast cancer to meet would thus be encouraged, especially for low resilient women who may otherwise lack social support in their regular network. A good example of this are buses that transport breast cancer patients to a nearby hospital, where they get to socialize with other patients. Nevertheless, breast cancer being a shared experience seems to be a double-edged sword. When someone from their close family was the one who previously had breast cancer, fear, anger, and burden of breast cancer seemed even larger. Previous research has suggested that daughters of breast cancer patients experience increased sense of their own vulnerability (Raveis & Pretter, 2005; Spira & Kenemore, 2000). There is thus a need for increased support for women with a family history of breast cancer, as well as for daughters of breast cancer patients and survivors.
The last theme we identified, “I Try to Leave that Behind Me,” reflects the aspect of cancer that distinguishes it from most other diseases. It is very difficult to say whether one has been “cured” from cancer. Mullan discusses this in his essay (1985), describing that one can live disease-free for many years, only for cancer to come back in a deadlier form. This can lead to high uncertainty and inability to move on. Important for resilience in the context of breast cancer in this study was conceptualizing breast cancer surgery as a method of “removing the breast cancer,” and receiving any additional adjuvant treatment as preventative, so that the cancer does not come back. This way of thinking about breast cancer as “removed” helped women move on from the experience and close the chapter of breast cancer. While doing so, women were able to move on with their lives as they were before breast cancer, or perhaps gaining new strengths and resources. This way of conceptualizing one’s illness experiences resembles Frank’s (1995) restitution and quest illness narratives, which also has been described in other studies on breast cancer (Thomas-MacLean, 2004). Restitution narratives involve anticipation of the cure and feeling better, whereas quest narratives involve gaining higher purpose as a result of the illness. Conceptualizing breast cancer as a chapter thus resembles both restitution and quest illness narratives. In addition, Frank (1995) also describes a chaos narrative, which involves no redeeming insights, as the illness seems to stretch forever. The chaos narrative resembles conceptualizing breast cancer as a constant that is still lingering and negatively affecting one’s life. Thus, resilience in the context of breast cancer might also be viewed from how a person constructs the story of their illness experiences. Interventions focusing on narratives, or storytelling, could be explored in relation to breast cancer where research on resilience should be put in constructive dialog with research focusing on narratives (e.g., Smit et al., 2019).
Strengths and Weaknesses of the Study
A big strength of this study was our use of purposive sampling. We were able to obtain a high variation of resilience scores in our sample, which allowed us to compare and contrast codes and themes across interviews. This allowed us to describe important aspects of resilience in women who once had breast cancer by noting where the important differences were expressed in women’s experiences. Further, we identified women for this study based on their scores on CD-RISC at the time of diagnosis. Nevertheless, the original study found that CD-RISC scores do not change substantially 1 year after diagnosis. Moreover, the time between treatment completion and being interviewed varied, despite it being more than 6 months for all women. It is thus important to note the possibility of recall bias when remembering experiences from the prediagnostic, diagnostic, and treatment phases. Additionally, treatment modalities and severity of breast cancer vary a lot among breast cancer patients, which might have resulted in varying experiences. These differences might frame the transferability of the study findings. The clinical and socio-demographic characteristics of the sample (Table 1) add to maximization of variability of the sample and are representative of treatment for breast cancer most often being multimodal. Moreover, although the study was conducted in southern Sweden, screening, diagnostic, and treatment procedures are standardized across the country (National Board of Health and Welfare Sweden, 2019), enhancing transferability of study findings in this setting. We aimed to provide a rich description of participants’ experiences, incorporating cases that add complexity to the themes we arrived at, further adding to credibility of the study.
Conclusions
In summary, this study highlighted three important aspects relevant for resilience in women who had breast cancer. First, having agency relating to one’s body, health, treatment procedures, thoughts, feelings, and daily functioning may play a role in resilience in this context. Although the illness itself is outside of one’s control, women can exercise agency in relation to how they handle and reflect upon their experiences. Future studies should investigate this link between agency and resilience. Moreover, interventions aimed at promoting a sense of agency in these areas may be beneficial for women with breast cancer. Beliefs related to being able to affect one’s treatment and overall wellbeing, emotions, and thoughts should be encouraged. Holding these beliefs may subsequently increase women’s intention to perform activities. Another important aspect of resilience in this context included having close others to turn to and being open to sharing the burden of breast cancer with close others. Social support can be provided in support groups and enabling breast cancer patients and survivors to meet each other. The third important aspect of resilience included perceiving the finality of breast cancer. Physicians can help women achieve this by using the language that expresses finality, such as explaining surgery as a way to remove the breast cancer and receiving additional treatment as preventative.
Footnotes
Acknowledgements
We would like to acknowledge all the women who took time to be interviewed for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the European Research Council (EUMSCA-COFUND 754299 CanFaster), the department of Psychology and the Faculty of Medicine at Lund University, the Mats Paulsson Foundation, and the CREATE Health Cancer Center. SCAN-B was funded by the Swedish Cancer Society, the Mrs Berta Kamprad Foundation, the Lund-Lausanne L2-Bridge/Biltema Foundation, the Mats Paulsson Foundation and Swedish governmental funding (ALF).
Ethics Statement
SCAN-B and SCAN-B Resilience were approved by the Regional Ethical Review Board in Lund/Swedish Ethical Review Authority (Dnr 2009/658, 2010/383, 2012/58, 2013/459, 2015/277, 2015/522, 2016/944, 2017/88, 2017/875, 2019-00700, 2019-01351). The amendment needed for the qualitative study was approved by the same Authority (Dnr 2020-05492).
Data Availability Statement
The audio recordings generated and analyzed during the current study are not publicly available due to privacy concerns. Anonymized interview transcripts can be made available from the corresponding author on reasonable request.