
Abstract
Objectives
There has been growing concern about doctors’ conflicts of interests (COIs) but it is unclear what processes and tools exist to enable the consistent declaration and management of such interests. This study mapped existing policies across a variety of organisations and settings to better understand the degree of variation and identify opportunities for improvement.
Design
Thematic analysis.
Setting
We studied the COI policies of 31 UK and international organisations which set or influence professional standards or engage doctors in healthcare commissioning and provision settings.
Participants
31 UK and international organisations.
Main outcome measures
Organisational policy similarities and differences.
Results
Most policies (29/31) referred to the need for individuals to apply judgement when deciding whether an interest is a conflict, with just over half (18/31) advocating a low threshold. Policies differed on the perception of frequency of COI, the timings of declarations, the type of interests that needed to be declared, and how COI and policy breaches should be managed. Just 14/31 policies stated a duty to report concerns in relation to COI. Only 18/31 policies advised COI would be published, while three stated that any disclosures would remain confidential.
Conclusions
The analysis of organisational policies revealed wide variation in what interests should be declared, when and how. This variation suggests that the current system may not be adequate to maintain a high level of professional integrity in all settings and that there is a need for better standardisation that reduces the risk of errors while addressing the needs of doctors, organisations and the public.
Keywords
Introduction
Medical ethics recognise the moral obligation of doctors to act for the benefit of their patients (beneficence). 1 Conflicts of interests (COIs) arise when doctors’ professional judgement and duties are influenced by secondary interests. 2 These interests may be financial or non-financial and fuel a moral tension between personal interests and professional responsibilities. 3 COIs can cause harm, thus violating another ethical principle (non-maleficence), even though the harm may be in the future, subtle or not formally reported. 3 For example, conflicting interests can lead to bias in the design and reporting of clinical trials, resulting in an overestimation of their benefits and an underestimation of their risks. 4 Evidence shows that professionals alter their practice when financial COIs are present,5–8 often underestimating the influence of industry interests.8,9 COIs may also undermine public health evidence and impede the development of health processes and policies, 10 thereby negatively impacting on healthcare provision, equity, justice and costs. 11
The identification and disclosure of COIs is the first step in analysing risks to patients 3 and organisations and is being advocated by medical regulators internationally.12–14 Since the 1990s, a significant push has been made for medical organisations to implement COI disclosure policies. However, studies within academic and research settings have shown variability in the COI disclosures and suggested that the different definitions of COIs, as well as the ambiguity of disclosure guidelines, make it difficult for academics to know what they need to disclose.15,16 In addition, the degree to which these policies are enforced within academic settings can vary, from voluntary questionnaires to mandated full-disclosure, and the interpretation can also be variable, resulting in disclosure discrepancies.17,18 In the UK, the Association of British Pharmaceutical Industries has a voluntary register, but a significant amount of funding remains unreported, 19 partly because healthcare professionals can decline to have their names listed. 20 However, even when commanding transparency of financial interests through legislation, such as in the case of the Physician Payments Sunshine Act in the U.S., implementation can be inconsistent, arduous and the data difficult to interpret in the absence of contextual and comparative information. 21
Inconsistencies in the disclosure and management of doctors’ COIs are likely to exist beyond industry-related financial interests and beyond research and academic settings. With the expansion of flexible working and of opportunities to engage in a variety of roles within provider and commissioner organisations, as well as professional bodies, it is likely that an increasing number of doctors may find declaring their interests and complying with the different organisational policies challenging. In the UK, there is currently a debate on whether there is a need for a central register of doctors’ interests. 22 , 23
This study aimed to map existing processes and tools used for doctors’ declaration of interests across a variety of organisations and settings, to better understand the degree of variation and identify good practice and opportunities for improvement.
Methodology
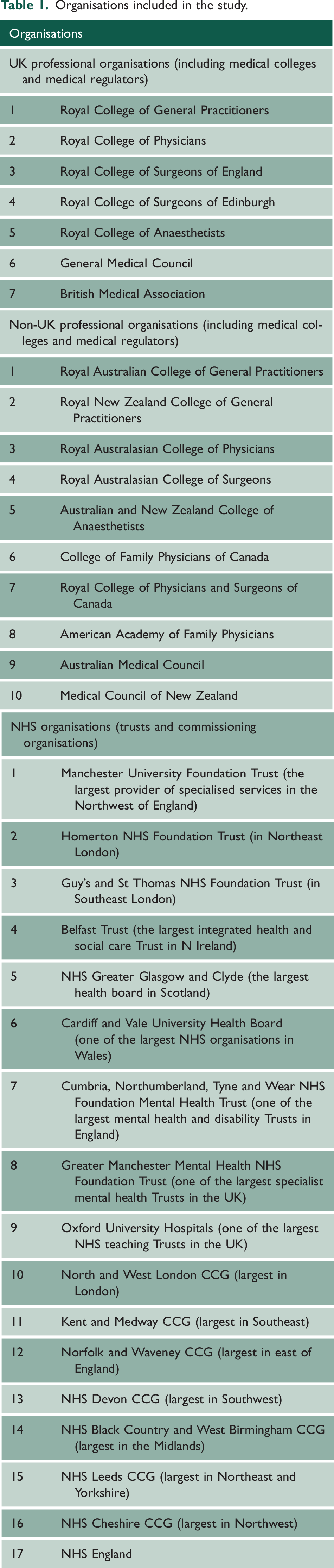
Between April 2021 and November 2021, we studied the policies of the five largest UK Royal Medical Colleges, the equivalent Medical Colleges in Australia, New Zealand and Canada, the medical regulators in these countries, the American Academy of Family Physicians, the British Medical Association, eight NHS Trusts and seven Clinical Commissioning Groups (CCGs).
The sample strategy was developed with the intention of producing a purposeful sample including organisations that either set or influence professional standards or engage doctors in work related to healthcare commissioning and provision. During scoping work, it was noted that similar debates around declarations of interest were occurring internationally. The country case studies were selected because of their similar professional training and use of English language. We sought to hold relatively constant the formal institutions so as to provide a relevant base for comparing actual practice in these countries with that in the UK and inform learning with realistic potential for policy transfer.
NHS Trusts and CCGs were chosen based on their size and location, trying to ensure wide geographical coverage across the UK.
We searched for COI policies in the organisations’ web home pages. If this search failed to identify a COI policy, we contacted the organisations directly and invited them to take part in the study and send us a copy of their policy, if there was one. The full list of the 34 included organisations is presented in Table 1.
Organisations included in the study.
Analysis
Thematic and content analyses were carried out, which helped to identify and code key themes and patterns from the study sample through an inductive method. 24 A thematic mind map was created to explain how the themes and sub-themes related. This process allowed the categorisation of the data into sections that were then cross-analysed.
Deductive content analysis was then used to analyse the policies and assess the frequency of data occurring in different categories. 25 This analysis helped us identify similarities and differences in the sample of COI policies examined. Each policy was reviewed independently by two members of the research team.
The data were not attributed to individual organisations and were summarised using descriptive statistics.
Results
Out of the 34 organisations included in the study, two had no policy on the management of COI and one did not respond to two invitations to take part in the study. Most of the remaining organisations (24/31) published their COI policy online. Two policies focused on educational activities.
The length of the policy documents varied between 2 and 47 pages, with an average of 16 pages.
The thematic analysis resulted in 6 themes and 24 sub-themes, which presented key concepts identified in the data (Figure 1).
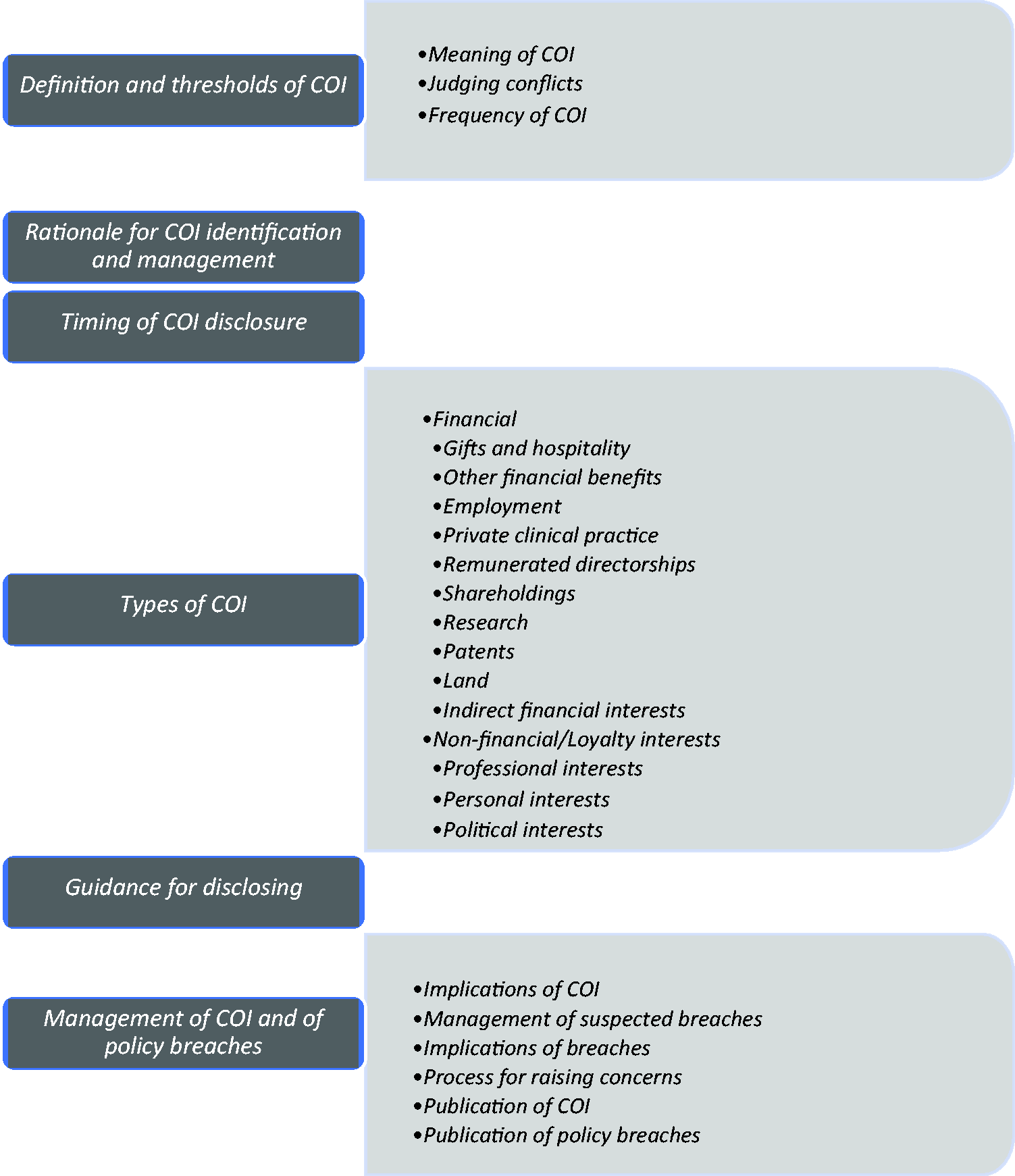
Themes and subthemes of organisational policies on doctors’ declarations of interests. COI: conflict of interest.
Theme 1: Definition of COI
One out of the 31 organisational policies did not contain a definition of COI. The definitions in the remaining policies varied and included the collision between different interests – Thompson’s 2 definition on the potential of interests impairing judgement, and the potential resultant benefit for the individual or third parties.
Most of the policies (29/31) referred to the importance of including actual (‘where there is a material conflict between one or more interests’), potential (‘where there is the possibility of a material conflict between one or more interests in the future’) and perceived interests (‘where an observer could reasonably suspect there to be a conflict of interest regardless of whether there is one or not’).
Eighteen policies (13 from NHS, 2 from UK and 3 from non-UK professional organisations) advocated a low threshold for declaring interests, while three advised that only ‘relevant’, ‘significant’ and ‘material’ interests should be declared.
There was a lack of clarity surrounding the scope of interests that physicians were asked to disclose. In certain areas (e.g. research), organisations requested declarations of all interests, while in others (e.g. shareholdings) only conflicts should be declared. Policies also differed on the perception of the frequency of COI. The majority (29/31) of policies referred to the need for applying judgement on which interest can be seen as or create a conflict.
Table 2 gives illustrative quotes on the definition and thresholds of COI.
Sub-themes and illustrative quotes on the definition and thresholds of conflicts of interest.
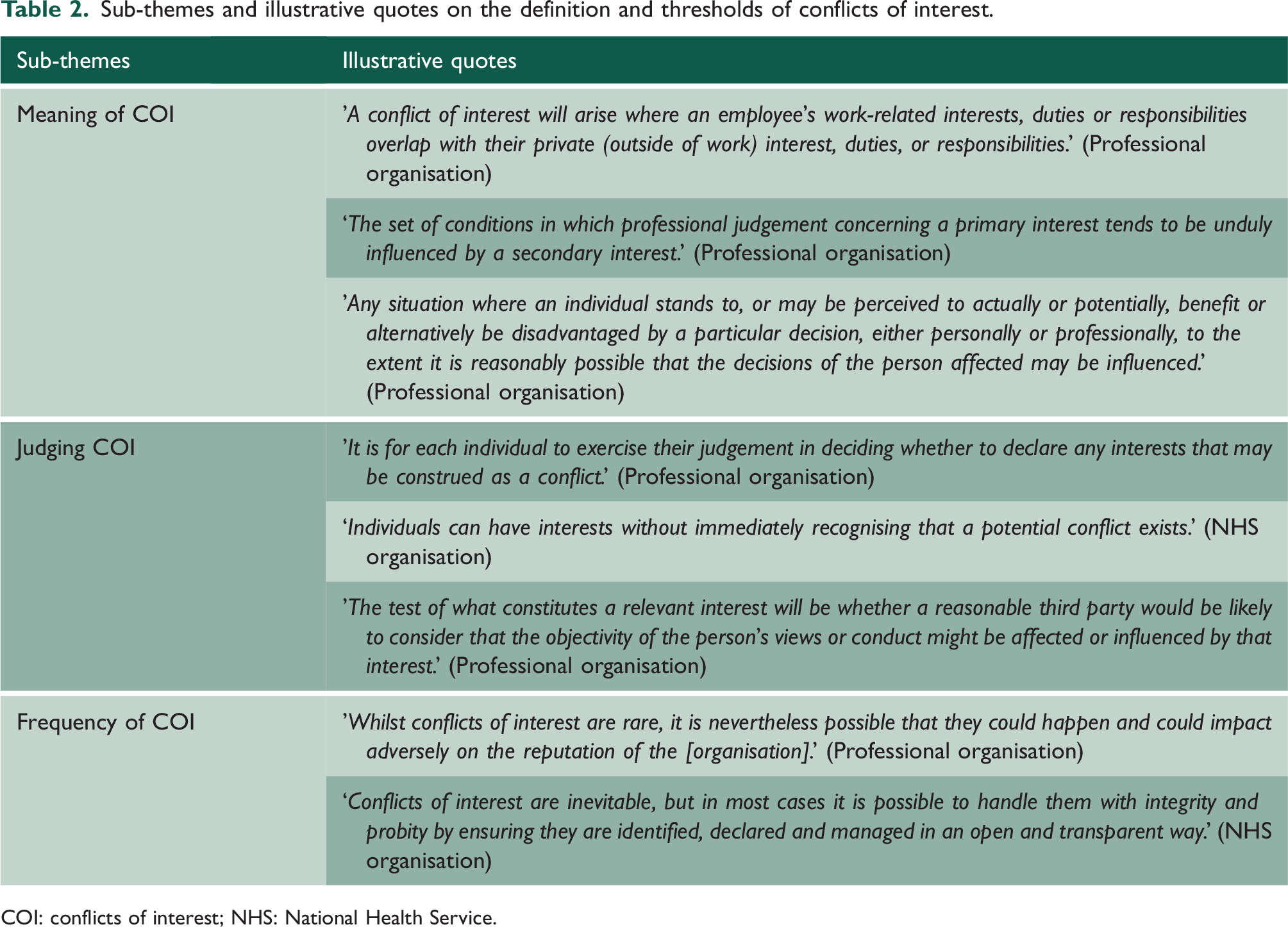
COI: conflicts of interest; NHS: National Health Service.
Theme 2: Rationale for COI identification and management
Out of the 31 organisational policies, the majority (26/31) mentioned a general commitment to transparency, integrity or good governance. However, only 18 articulated a clear rationale on why the identification and management of COI needed to take place in a consistent and rigorous way.
The majority of those who provided a clear justification (14/18) were NHS organisations, bound by the relevant legislative requirements and following NHS guidance. A total of 11 NHS policies referred to the Nolan principles, which encompass selflessness, integrity, objectivity, accountability, openness, honesty and leadership. 26 Out of the 18 policies, 14 (11 NHS, 1 UK professional and 2 non-UK professional), referred to legal requirements due to corporate, charity or NHS-related legislation and 12 NHS policies referred to public financial accountability and that physicians and organisations have a duty to ensure that public money is used not for one’s profit, but for the benefit of the population.
Out of the 15 professional organisations who had a COI policy, only two (one UK and one non-UK) referred explicitly to their duty to promote the declaration and management of COI within their own organisation and set an example reflecting ‘the highest standards’.
Theme 3: Timing of COI disclosure
Table 3 presents the results on the timing of declarations of interests as reported in the 31 organisational policies. In most policies, there was an expectation for updating the declarations at different points during a doctor’s engagement with the organisation.
Timing of disclosure of declarations of interests.
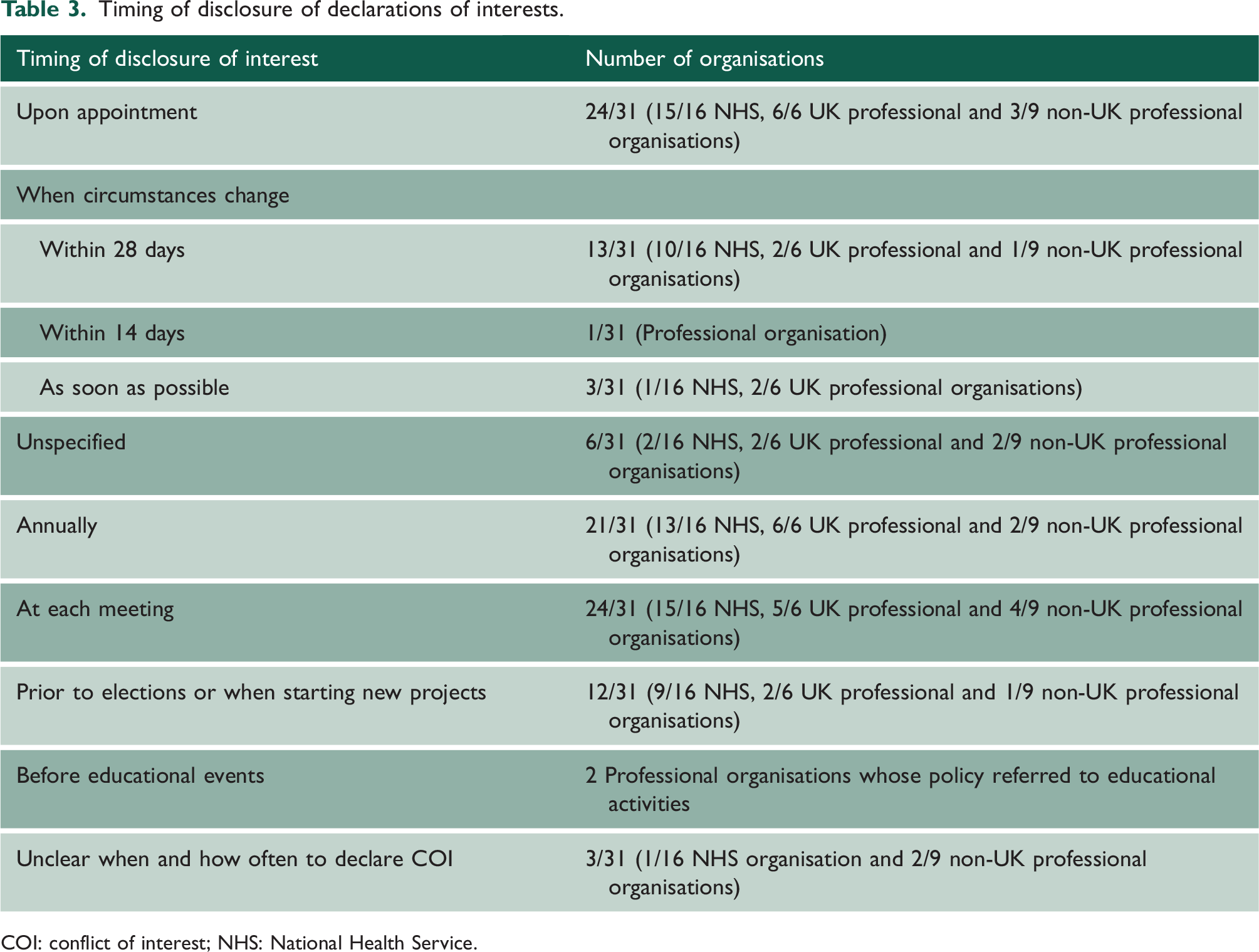
COI: conflict of interest; NHS: National Health Service.
Three policies (two of which were from NHS organisations) specified that retrospective COIs in the previous 12–36 months should also be declared. One policy by a non-UK professional organisation also asked for the declaration of future interests that ‘are known to be going to occur during the next 12 months’.
Theme 4: Types of COIs
Financial interests were identified by all organisations as concerning and, thus, in need of disclosing. Several organisations acknowledged other important categories and sub-categories of financial and non-financial (loyalty) interests, which are presented in Table 4.
Types of COIs in organisational policies with illustrative quotes.
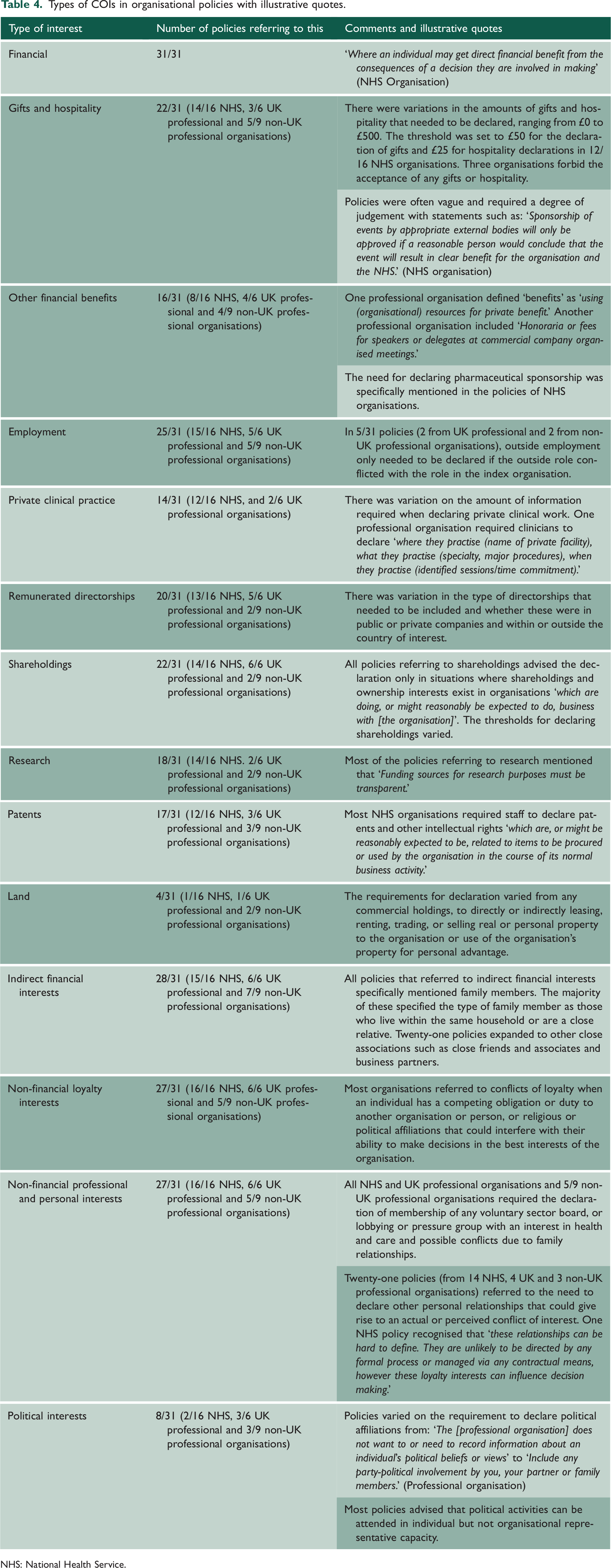
NHS: National Health Service.
Theme 5: Guidance for disclosing
Most of the policies (28/31) gave examples of potential conflicts to assist understanding. Eighteen policies (nine of which were NHS, five UK and four non-UK professional organisations) had forms for the declaration of interests incorporated into their policy documents and two policies provided links to the forms that were not working. Seventeen of the forms (10 from NHS, 3 from UK and 4 from non-UK organisations) used direct questions, guiding readers on what to include.
Eleven policies (5 of which were NHS, 3 UK professional and 3 non-UK professional organisations) provided clear details about whom individuals should contact if there was a need for clarification regarding the declarations.
Theme 6: Management of COI and of policy breaches
Six sub-themes were identified on the management of COI and of policy breaches. The results are summarised in Table 5.
Management of COI and policy breaches.
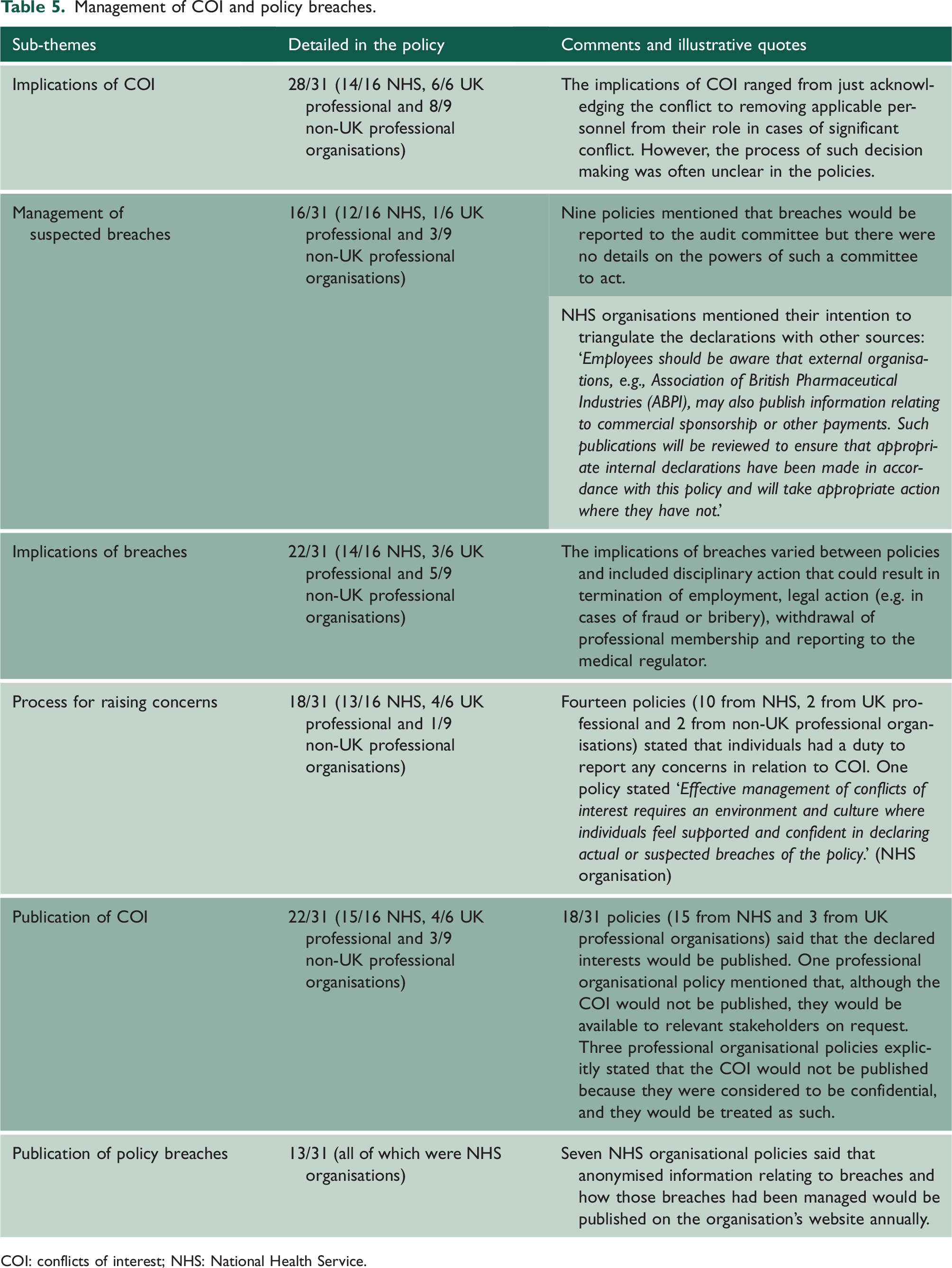
COI: conflicts of interest; NHS: National Health Service.
Discussion
The analysis of organisational policies on the declaration and management of doctors’ COIs revealed wide variation in what should be declared, when and how. There were also variations on how such COIs and policy breaches should be managed and on how transparently they should be communicated.
Our study is limited by the fact that we focused on a sample of policies of professional, regulatory and NHS organisations and we did not investigate the actual processes that institutions use to record and manage COI. However, this is the first study analysing organisational policies on doctors’ COIs, and the findings highlight the degree of variation and the need for standardisation. Similar variations have been found in policies within medical schools and other research institutions. 18 It is important for both practical and ethical reasons that healthcare professionals know which guidance they should follow and are clear about what they are expected to declare and how to do it. 27
Only eight policies advised on declaring political activities, and none mentioned religious beliefs. Professional and financial interests can be easier to record, investigate and verify. However, other interests, such as political or religious affiliations, may also cause conflicts, 28 can be harder to establish and verify and are considered protected characteristics, which may explain their very limited reference in existing COI policies.
The fact that most policies referred to conflicts, rather than interests, presents a challenge for two reasons. First, defining what constitutes a conflict heavily relies on self-perception and individual judgement and is therefore reliant on individual skills to navigate ethical issues and behave impartially. Much of the existing guidance asks the person declaring to consider how much of an interest would constitute a conflict. This can be difficult to gauge – it is often inferred from the amount of a financial stake someone has or from how formally or overtly they have manifested their loyalty to an external cause. Such judgements are made not just on the subject of the declaration but also on whether the interest is current, in the recent or even distant past. In addition, most policies referred to the importance of declaring perceived, and not just actual, conflicts. This is known as ‘the appearance standard’ and is quite common in COI regulation, recognising that the appearance of conflict can in itself undermine trust in the system and therefore cause harm. However, given that existing policies rely to a great extent on self-regulation of COIs, this creates a further layer of complexity: doctors are asked not only to identify and evaluate their own COIs, but also to estimate how these interests will appear to patients and the public. 29
The second challenge of declaring conflicts rather than interests presents because conflicts are judged in the context of the organisational role or activity the doctor is undertaking. Therefore, the same interest may constitute a conflict for a position in one organisation but not for another. In addition, the very different thresholds for declaring conflicts in existing policies, coupled with the fact that increasingly more doctors are involved in multiple roles in various settings, means that the same doctor may have to submit and update very different COI declaration forms for each of their roles, which is burdensome and increases the risk of mistakes and omissions.
Almost half of the policies lacked a clear rationale for declaring COIs and did not refer to the management of breaches and the process of raising concerns. The policies also differed in their stance on the publication of COIs with conflicting messages on the need for confidentiality versus transparency. There was less variation among NHS organisations, with the majority, albeit not always consistently, following the published guidance on COIs by NHS England. This highlights the positive effect of central standard setting. It has been shown that clear and specific instructions can lead to better compliance and performance. 30 In addition, policy consistency can assist with the training of doctors and can help with setting clearer expectations for the public. However, the NHS England guidance only applies to NHS Trusts and commissioning organisations 31 and there is currently no system in place for the declaration of doctors’ interests in other settings such as general practice and primary care.
On the basis of our findings, we propose using the term ‘declaration of interest’ instead of ‘conflict of interest’. This would mean that disclosure is encouraged even of interests that are not necessarily thought by the individual to produce a conflict and would allow independent third-party judgement. Agreed criteria about when a declared interest would be a conflict, and importantly, what action should be taken if so, would assist individuals, organisations and the public with the interpretation of such declarations.
Further research is needed on the expectations of the public on the type of interests that need to be declared, the optimum way of conveying such information and the potential merits, feasibility and acceptability of a well-maintained and protected database of doctors’ interests, with the possibility of both private and public settings, enabling searching and cross-checking through automation. This could work in a similar manner to ORCID, which assists funding bodies and journals to identify authors and applicants. The process should be minimally burdensome for those entering information while being sufficiently comprehensive and reliable for those seeking information, 32 thereby improving the consistency, efficiency and transparency of declarations of interests.
Supplemental Material
sj-pdf-1-jrs-10.1177_01410768231181248 - Supplemental material for Policies on doctors’ declaration of interests in medical organisations: a thematic analysis
Supplemental material, sj-pdf-1-jrs-10.1177_01410768231181248 for Policies on doctors’ declaration of interests in medical organisations: a thematic analysis by Victoria Tzortziou Brown, Margaret McCartney, Patrycja Talaga, Richard Huxtable, Andrew Papanikitas and Elizabeth David-Barrett in Journal of the Royal Society of Medicine
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.