
Abstract
Summary
Objectives
To examine sponsorship of Australian and New Zealand medical societies by healthcare companies and whether societies have policies to deal with conflicts of interest.
Design
Cross-sectional study conducted in March 2022.
Setting
Australia and New Zealand
Participants
Medical societies in both countries.
Main outcome measures
The percent of medical societies that list sponsorship from healthcare companies on either their home webpages or the webpages of their annual meetings and/or that issue prospectuses to potential sponsors. The percent of societies with sponsorship that also have policies about their interactions with their sponsors. Whether societies feature their sponsors’ logos on their webpages and have hyperlinks to sponsors’ webpages and what percent of societies' annual revenue comes from sponsorships.
Results
Ninety-two medical societies were identified. Sixty-two had healthcare company sponsorship and 10 of the societies with sponsorship had policies to deal with interactions with their sponsors. Fifty-four societies displayed the logos of their sponsors on their home webpages and/or the webpages of their annual meetings. Only 6 societies provided enough information to calculate what percent of their revenue comes from sponsorships. For 5 of the 6 the percent was well below 50%.
Conclusions
The acceptance of sponsorships from healthcare companies by Australian and New Zealand societies is common and few societies have policies to deal with these relationships. In general, societies appear to get only a small percent of their annual revenue from sponsorships.
Keywords
Introduction
Medical societies are voluntary membership organisations primarily of doctors who share a common expertise in either a medical specialty (e.g. cardiology) or a common interest in a particular area of practice (e.g. rural medicine). Societies serve important purposes: they provide continuing professional education to their membership, they advocate to government and others on behalf of their membership and the patients that they treat and they promote continual improvement in their area of knowledge.
The work of medical societies means that they often interact with healthcare companies – companies that produce drugs, medical devices and medical technology and there have been concerns raised about the effect of these interactions on societies.1,2 For example, in 2016 the Royal College of Paediatrics and Child Health in the United Kingdom announced that it would continue to accept funding from manufacturers of breast milk substitutes. 2 After a trial showed that hydroxyprogesterone caproate (Makena), a long-acting form of a naturally occurring progesterone, failed to prevent preterm deliveries, an advisory committee to the United States Food and Drug Administration narrowly voted that it should be removed from the market. This recommendation was disputed by the Society for Maternal-Fetal Medicine and the American College of Obstetricians and Gynecologists, both of whom accepted donations from the maker of Makena. 3
Researchers in Australia have used the information about payments to doctors that is posted on the website of Medicines Australia (MA) to examine interactions between medical professionals and pharmaceutical companies.4–6 However, payments to medical societies are not included in the reports from companies to MA and therefore sponsorship of these organisations has not been studied. This study investigates sponsorship of Australian and New Zealand societies by healthcare companies. In addition, it looks at whether societies actively solicit sponsorship, the presence or absence of company logos and hyperlinks to company websites on the websites of societies, whether societies have policies about interactions with companies and what percent of societies’ annual revenue comes from sponsorships.
Methods
Identification of medical societies
There is no consolidated list of medical societies. In the absence of such a list, on March 24, 2022, a Google search was done using the phrase ‘medical societies in Australia’. The search yielded five sites that listed possible societies: Australian Health Directory, Colleges, societies & associations – Choosing Wisely Australia, Medical associations based in Australia, Royal Australian College of Physicians and Royal Australian College of Surgeons. The names and URLs of the possible societies from these websites were entered into an Excel spreadsheet. Duplicates were deleted and then the following exclusion criteria were applied: Colleges and chapters of colleges (not voluntary societies), societies which were not primarily composed of doctors, societies that were subsidiaries of another society, no active website. Because of the overlap between Australian and New Zealand societies, ones from the latter country were also included.
Data from society home and annual meeting webpages
Between March 25–29, the home webpages and annual meeting webpages (and webpages linked to either of them) of the societies were searched. If sponsors were mentioned in either place, the names of the companies, amount of sponsorship, year of meeting, presence of company logo on society webpage and hyperlink to company website were entered into the Excel spreadsheet. In addition, if a prospectus for sponsors was present, the value of different levels of sponsorship was recorded. When no prospectus was found but there was an announcement that a prospectus was available on request that information was also recorded. In the absence of company names on home and meeting webpages, the presence of a prospectus was taken as evidence that the society had sponsorship.
Sponsorship from companies that did not make drugs, devices or produce technology, sponsorship of trainees’ travel and accommodation and sponsorship of society awards was not recorded.
Information about annual revenue, percent of revenue from company sponsorships and presence of policy for interactions with companies
Webpages were searched for information about the society's annual revenue, the value of sponsorship(s) in dollar amounts (all amounts are in Australian dollars) and the presence of a policy dealing with interactions with sponsors. If a policy was present then it was examined to determine if it dealt with individual society members, the society itself or both; otherwise, the contents of the policies were not examined.
Analysis
Only descriptive statistics are reported. Medians and interquartile ranges (IQR) are used as the data were not normally distributed.
Ethics
Societies were not directly contacted as the aim was to determine if information about sponsorships was publicly available. Since all the data was public, ethics approval was not required. All data collected for this study are available from the author on request.
Results
Degree of sponsorship
After the elimination of duplicates and the application of the exclusion criteria 92 societies were left for analysis (Figure 1). Sixty-two of the 92 societies (67.4%) had sponsorships (Table 1). Evidence of sponsorship usually came from a combination of companies being named on annual meeting webpages and the presence of a prospectus (30 societies) or from just the name of companies on meeting webpages (13 societies). Other evidence of sponsorship was less common (Table 1). For 17 societies there was no mention of sponsors on either home or meeting webpages and there was no prospectus. The remaining 13 societies did no mention sponsors on home webpages and there was no annual meeting webpage or mention of a prospectus. Thirty sponsored annual meetings took place or will take place in 2022, 29 in 2021, 1 in 2020 and 2 in 2019.

Identification of Australian voluntary medical societies.
Determination of presence of sponsorship.

In addition, one society reported sponsorship of its foundation and one reported sponsorship of research it conducted.
Logos of sponsors and value of sponsorship
A median of 5 (IQR 2, 9) companies were named on the home webpage of 11 societies and a median of 6 (IQR 3, 12) companies were named on the annual meeting webpages of 53 societies. The logos of sponsoring companies appeared in all cases where sponsors were named. When logos appeared, there were hyperlinks from home webpages to the websites of sponsors 81.8% of the time and 64.2% of the time from annual meeting webpages. The value of the sponsorships was given by categories (e.g. platinum, gold, silver, etc.) and not monetary amounts. Sponsorship was categorised on home webpages of 5 societies and on annual meeting webpages of 42 societies (Table 2).
Presence of logos and value of sponsorships on webpages.
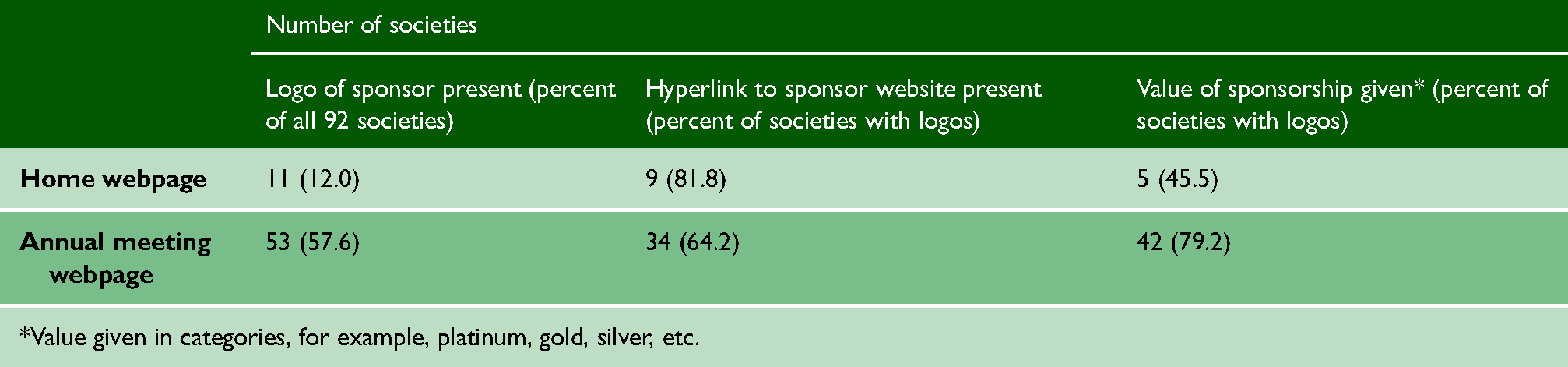
*Value given in categories, for example, platinum, gold, silver, etc.
Information in prospectuses
Prospectuses were present on the annual meeting webpages of 23 societies. In all cases sponsorships were put into categories and values (e.g. platinum $80,000) were assigned to each category. Each category of sponsorship granted sponsors different degrees of access to attendees. For example, a platinum sponsorship from one society, valued at $100,000, gave the sponsor, among other things, recognition as the dinner sponsor, inclusion of the company logo on menus, the exclusive use of the company logo on the delegate name badges, six exhibition booths with the opportunity to purchase additional booths prior to the general sale of the industry exhibition, the opportunity to select the location of its exhibition space within the exhibition hall, acknowledgement at the opening ceremony by the society president and acknowledgement on the society website including a link to the sponsor's website.
Sponsorships as a percent of society revenue
Six societies provided information to calculate sponsorship as a percent of total revenue. In one case it was 75% but otherwise it was well below 50% and as low as 0.24% (Table 3).
Sponsorship as a percent of society total annual revenue.

Presence of policy about interactions between society and sponsors
Out of the 62 societies that had sponsorship, there was a policy about interactions with sponsors in 16 (25.8%) cases and no policy was found in the other 46 (74.2%). Three societies cited the Australian Consensus Framework for Ethical Collaboration in the Healthcare Sector, a document endorsed by multiple organisations. Ten (62.5%) of the 16 policies applied to the society, 5 (31.3) applied only to individual members of the society and 1 was only available to society members and could not be evaluated.
When societies did not state whether sponsorship was present on either their home or annual meeting webpages and there was no prospectus, 2 (11.8%) of 17 had a policy and 15 (88.2%) did not. One of those policies applied at the individual level and one at the society level. If no annual meeting was identified for a society, there was no sponsorship found on the home webpage and no prospectus was mentioned, none of these 13 societies had a policy (Table 4).
Sponsorship and policy about relationship with healthcare companies.
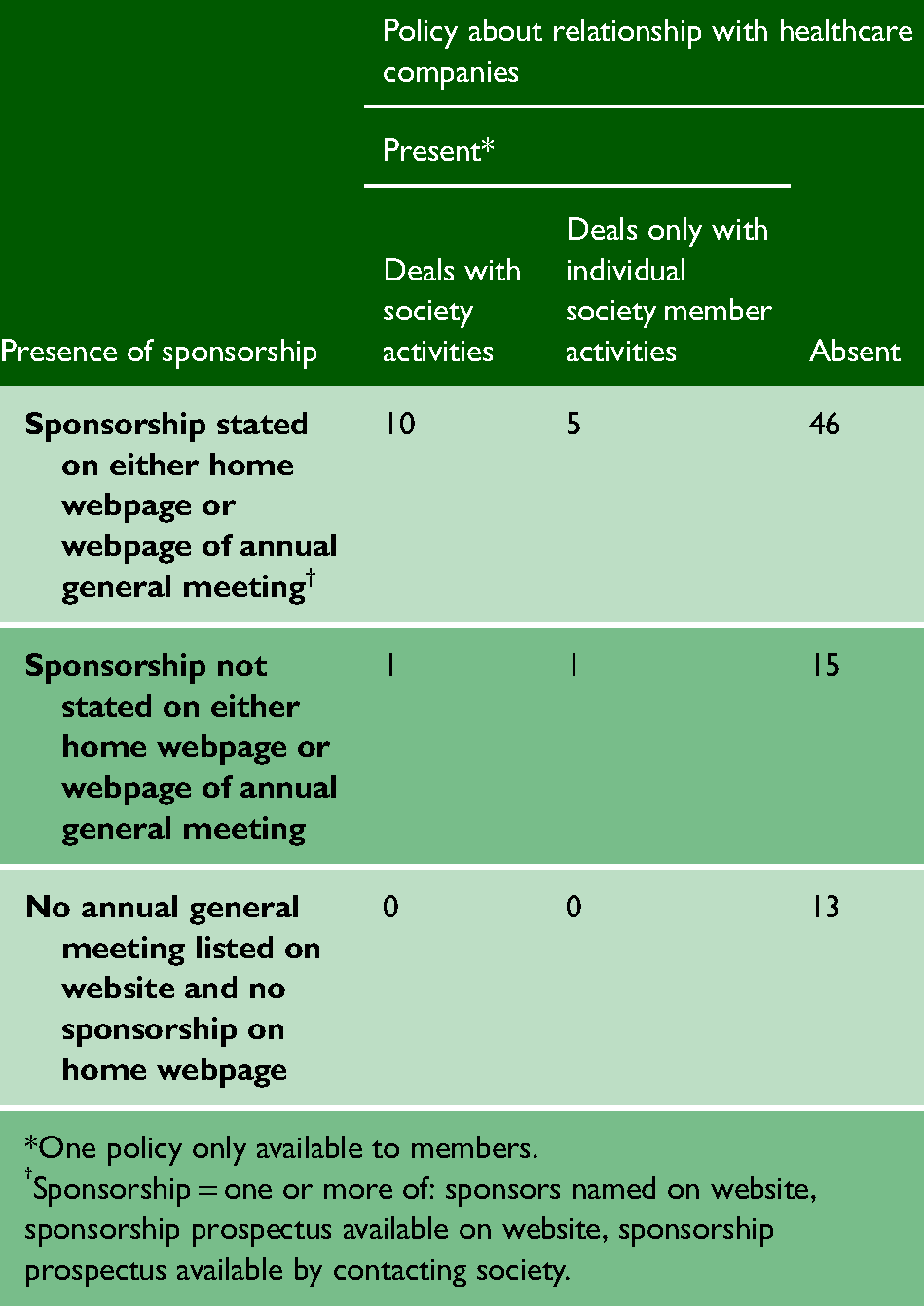
*One policy only available to members.
Sponsorship = one or more of: sponsors named on website, sponsorship prospectus available on website, sponsorship prospectus available by contacting society.
Discussion
Over two thirds of the societies in Australia and New Zealand had sponsorship from one or more healthcare companies. Out of the 62 societies with sponsorship, only 10 (62.5%) had policies about interactions with sponsors that applied to the society itself. The general absence of a policy raises the question about what measures societies take to govern their relationships with their sponsors.
Whether sponsorship affected the actions of the societies was not investigated, research in other countries has pointed to an association between societies having conflicts of interest and taking positions favourable to their funders.
Contraception guidelines from the Society of Obstetricians and Gynaecologists of Canada (SOGC) that endorsed the use of two oral contraceptives Yaz and Yasmin (drospirenone and ethinyl estradiol), were an almost identical copy of a consensus statement from a Bayer workshop. The SOGC received funding from Bayer and its executive vice-president defended the guidelines. 7 Guidelines on the prescribing of opioids for chronic non-cancer pain produced by four organisations with conflicts of interest with companies making opioids had multiple ‘red flags’, that is, items known to introduce potential bias. 8 In 2009, the American Society of Hypertension partnered with its then largest donor, Daiichi Sankyo, to create a training programme for the company's sales representatives. 9 The American Academy of Family Physicians has previously partnered with the Coca-Cola Corporation to support patient education materials on obesity prevention. 1
Hyperlinks from societies’ webpages to the websites of their sponsors potentially expose viewers to information about products produced by their makers. A 2010 systematic review examined the relationship between exposure to information from pharmaceutical companies and the quality, quantity and cost of physicians’ prescribing. The authors concluded that ‘with rare exceptions, studies of exposure to information provided directly by pharmaceutical companies have found associations with higher prescribing frequency, higher costs, or lower prescribing quality or have not found significant associations.’ 10
Although sponsorships from healthcare companies generally only provide a small percentage of a societies’ overall annual revenue, this finding is tempered by being based on only 6 out of 62 societies with sponsorship.
The results of this study are in-line with reporting on medical societies in other countries. Out of 131 Italian societies, 29.0% had manufacturers’ logos on their webpage, 4.6% had an ethical code covering relationships with industry, 6.1% published an annual financial report and 64.9% received sponsorship for their last conference. 11 Twenty-three (35.4%) out of 65 Canadian societies reported company sponsorship on their home webpages and 25 (38.5%) reported sponsorship for annual meetings. Most societies with either type of sponsorship displayed the logos of their sponsors and provided hyperlinks to their websites. Only two societies gave information to calculate what percent of their revenue came from sponsorships. Over one-fifth of societies solicited sponsorships but only 10 had policies about how to deal with relationships. 12
Limitations
The results only apply to the societies that were examined and may not reflect other Australian and New Zealand societies that might have been missed in the search, for example ones composed of clinical and basic pharmacologists and pharmaceutical medicine specialists. When information was absent, it is not known if societies did not receive or did not report sponsorships. Using medians to describe the number of relationships between societies and healthcare companies might obscure differences between broad and narrow interest societies. Broad interest societies are likely to have interactions with more companies than narrow interest ones. Furthermore, there may be overlapping interests between broad and narrow interest societies and the narrow interest societies may feel that their concerns about interactions have been addressed by the broader interest ones. Virtually all the societies had member-only sites that may have contained additional information. The COVID-19 pandemic caused a large number of annual meetings to go virtual or be postponed and that may have affected sponsorship. The data were gathered and analysed by one person.
Conclusion
The acceptance of sponsorships from healthcare companies by Australian and New Zealand societies is common and few societies have policies to deal with these relationships. In general, societies appear to get only a small percent of their annual revenue from sponsorships. Further research should be undertaken to determine if sponsorships affect the activities of societies.
Footnotes
Acknowledgements
None
Competing interests
In 2019-2021, Joel Lexchin received payments for writing a brief on the role of promotion in generating prescriptions for Goodmans LLP and from the Canadian Institutes of Health Research for presenting at a workshop on conflict-of-interest in clinical practice guidelines. He is a member of the Foundation Board of Health Action International and the Board of Canadian Doctors for Medicare. He receives royalties from University of Toronto Press and James Lorimer & Co. Ltd. for books he has written.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All data was publicly available and no ethical approval was necessary.
Guarantor
Joel Lexchin is the guarantor
Contributorship
None