
Abstract
The global demand for hospital treatment exceeds capacity.The COVID-19 pandemic has exacerbated this issue, leading to increased backlogs and longer wait times for patients. The amount of outpatient attendances undertaken in many settings is still below pre-pandemic levels and this, combined with delayed referrals, means that patients are facing delays in treatment and poorer health outcomes. Use of digital health technologies, notably the use of remote symptom monitoring systems based on patient-reported outcomes (PROs), may offer a solution to reduce outpatient waiting lists and tailor care to those in greatest need. Drawing on international examples, the authors explore the use of electronic PRO systems to triage clinical care. We summarise the key benefits of the approach and also highlight the challenges for implementation, which need to be addressed to promote equitable healthcare delivery.
Keywords
One way to address hospital outpatient pressures might be the effective ‘triaging’ of patients so that only those who really need to be seen in person at clinics are given face-to-face appointments. Since the beginning of the COVID-19 pandemic, telehealth has been increasingly deployed for the purpose of remotely monitoring and screening patients. One form of telehealth that may be beneficial in the outpatient setting is the use of electronic patient-reported outcome (ePRO) systems to capture patients’ symptoms, functioning and experience with treatments. PROs have been defined as ‘… any report of the status of a patient’s health condition that comes directly from the patient, without interpretation of the patient’s response by a clinician or anyone else’. 1 While the collection and use of PROs is well established in research settings to evaluate the effectiveness, cost-effectiveness and tolerability of interventions from a patient perspective, 2 in recent years, interest in the routine use of PROs to enhance the quality of patient care has increased and clinicians are more interested in patient-level PRO data for the clinical management of individual patients in routine practice.2–4 The technological innovations that have led to a rapid adoption and increased ownership of electronic devices have also facilitated the development and dissemination of ePROs, which allow patients to be sent ePRO questionnaires to fill out at home or at a location of their choice and have the results sent back to the clinician in near real time to use in clinical decision-making. 5 Various studies have demonstrated that the collection of ePROs in routine clinical practice is both acceptable and feasible, with patients increasingly expressing a preference for an electronic mode of administration.6,7
In this article, we offer an international perspective on the potential benefits of using ePRO solutions to support the management of outpatient care. We summarise the benefits reported by publications on existing ePRO systems on clinical workflow and patient care. We consider and propose solutions to address barriers to implementation and use.
Methods
Search strategy
For this narrative review, we searched PubMed from inception on 4 July 2022, for articles that described the use of ePRO solutions in outpatient care using the words ‘clinic’, ‘outpatient’, ‘electronic patient reported outcomes’, ‘ePROs’ as search terms. We also conducted hand searching of reference lists of selected articles. Two researchers independently performed the screening of titles and abstracts and evaluation of full texts. They discussed and agreed on the included articles.
Eligibility criteria
We included studies in English language that reported specific benefits or outcomes of using ePRO solutions in outpatient settings. We excluded narrative or systematic reviews, commentaries, opinion pieces and letters that do not report primary findings.
Search results
Our database search retrieved 135 entries that were independently screened by OLA and MJC. The full texts for 41 articles were examined and 16 were selected. The 25 articles excluded did not meet our eligibility criteria. These either focused on the development of ePRO systems or the use of ePROs in other settings such as in clinical trials. Two more articles were identified through hand searching, bringing the total number of included articles to 18.
Benefits of implementing ePRO systems for outpatient care
There were several reported benefits of implementing ePRO systems for outpatient care. When ePROs were administered remotely, it facilitated the triaging of patients. Symptom support was provided to clinically stable patients who did not require outpatient appointments, while patients who needed to be seen in person were given appointments and seen more quickly. This led to significant reductions in outpatient appointments and the timely provision of interventions in several clinical specialties. The administration of ePRO before clinic appointments and the discussion of ePRO results with patients during their appointment fostered a better understanding and documentation of patient symptoms, timely initiation of interventions and enhanced patient–clinician interactions. Evidence was provided by studies conducted with various groups of patients including those with epilepsy, sleep apnoea, type 1 diabetes, cancer, rheumatoid arthritis (RA) and HIV. The ePROs for most of the studies were provided remotely (14 of 16 studies), while only two studies gave patients the option of providing remotely or in clinic. The use of reminders to patients to provide their ePROs was reported by 8 (50%) of the studies, while patient training was reported by 3 (19%) and clinical staff training by 5 (31%). Key findings from the studies are provided below. Table 1 provides the details of the administration of the ePRO systems used by the studies while Table 2 summarises the study characteristics and findings.
Administration of ePROs in the studies reviewed.
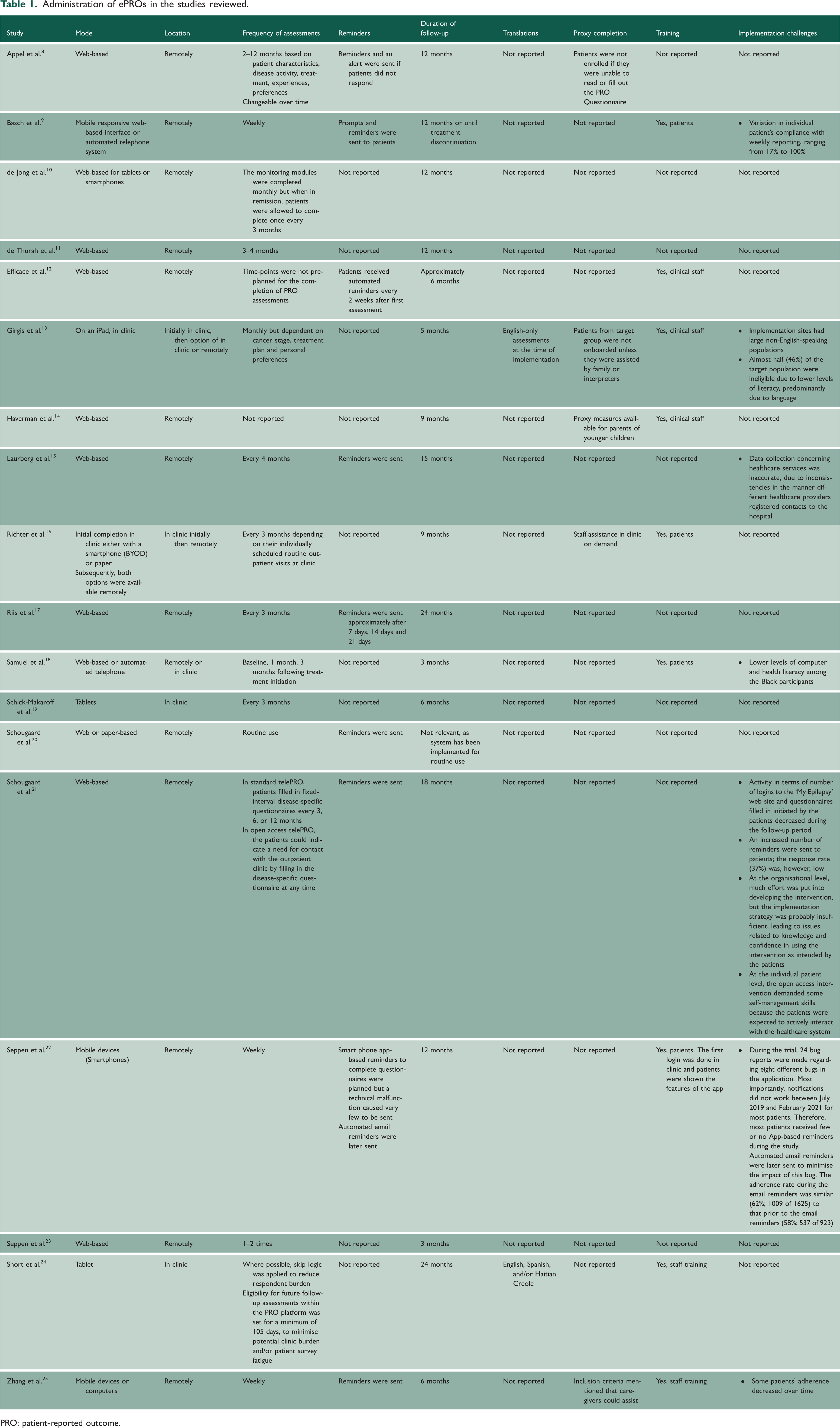
PRO: patient-reported outcome.
Study characteristics and findings.

irAE: immune-related adverse events; ePROM: electronic patient-reported outcome measure; QOL: quality of life; RA: rheumatoid arthritis; RCT, randomised controlled trial.
Reduction in outpatient appointments
Ambuflex, a generic ePRO system, is currently being used in Denmark for outpatient management of patients across several chronic conditions. 26 Use of the system has led to substantial reductions in outpatient appointments of 48% (epilepsy), 57% (sleep apnoea), 20 45% (inflammatory bowel disease [IBD] with mild or no disease activity), 8 2.4 fewer extra visits per year (RA) 11 and a 23% change of face-to-face appointments to telephone consultations (type 1 diabetes). 15 However, socioeconomically disadvantaged patients with epilepsy may be less likely to be referred for remote outpatient follow-up. 27 Evidence suggests no differences between flexible patient-initiated PRO-based follow-up and fixed-interval PRO-based follow-up in the use of healthcare resources, patient self-management or satisfaction. 21
Findings from studies of other ePRO systems included significantly fewer in-person visits for problematic symptoms in patients with lung cancer 13 ; reduced outpatient visits and hospital admissions in patients with IBD 10 ; a decrease in the need for follow-up visits after breast reconstruction surgery 28 ; fewer consultations in patients treated for early breast cancer on ePRO-based follow-up 17 ; approximately 28 min lower mean time requirement for implementing follow-up in patients on cancer immunotherapy 25 ; and the potential to predict which patients with RA (who have low disease activity scores) can skip a clinic visit and those who may not require certain medication for 2 weeks after providing their ePROs. 23
Better understanding and documentation of patients’ symptoms
The use of ePROs led to a significant difference of 13% in incidence of serious immune-related adverse events (irAEs), 7.4% lower rates of treatment discontinuation and better quality of life in patients on cancer immunotherapy. 25 Clinicians reported that ePRO data facilitated their understanding of patients’ general health status and symptoms, 12 identification of low-grade and high-grade symptomatic adverse events, 12 accurate documentation of patients’ symptoms9,12,24 and improved patient adherence to treatment.10,16,29
Initiation of timely interventions
Various studies described clinician responses to ePRO data, which suggest timely/earlier intervention when symptoms of clinical concern are present.30,31 These included: telephoning patients upon receiving ePRO alerts of clinically important symptoms 12 ; referrals to other healthcare professionals 19 ; mental health services 24 ; further assessments; requests for blood tests; recommendations to wait and monitor symptoms; and patient education. 19 Clinicians also stated that ePRO data were useful in the clinical management of patients and shared decision-making. 12
Facilitation of patient–clinician interactions/communication
Several studies reported that the use of ePRO data facilitated patient–clinician interactions.9,12,14,16 Specifically, ePRO data were used to initiate discussions including those around complex health and behavioural issues such as suicidal ideation and anxiety in people with HIV, 24 and clarify symptoms through focused assessments during clinical appointments. 19 Clinicians may review the ePRO data before starting their general assessment or integrate elements of the ePROs into their regular practice. 19 For example, a recent implementation of a co-designed ePRO dashboard for IBD reported that it helped focus discussions on what mattered most to the patient; use of this dashboard during the clinic visit versus outside the visit was also associated with a twofold increase in shared decision-making. 32 While clinicians often initiated the discussion of various issues highlighted by the ePRO data, 33 there may be some reluctance in initiating discussions about sensitive issues such as sexual function and physical appearance. 19
Patients confirmed that providing ePROs helped them consider their overall health, recall health concerns to raise,18,24 discuss topics that might otherwise not have arisen, discuss sensitive issues, decide what to talk about and feel more in control of their own care.9,24,34 There might be racial differences in the benefits patients derive from the use of ePROs. 18 A study reported that white patients valued the ePRO system for facilitating a better understanding of their symptoms and enabling symptom tracking, while black patients valued the ePRO system more for facilitating symptom-related discussions and improving communication with clinicians. 18
Barriers to implementation and potential solutions
Several barriers to implementation were identified as outlined below.
Inclusive, equitable data collection
Low levels of computer and health literacy or challenges with language have limited implementation within certain groups, predominantly black and non-English-speaking populations.13,18 Patients from socioeconomically disadvantaged backgrounds may be less likely to be considered for ePRO-based follow-up. 27 Therefore, the successful implementation of ePROs in clinical care could exacerbate health disparities if the advantages of ePRO are not also available to already disadvantaged patients. Interestingly, it has been reported that computer-inexperienced patients may derive greater benefit from ePRO monitoring in terms of emergency department visits, hospitalisation and survival compared to computer-experienced patients. 31 Similarly, the use of ePROs in outpatient care may be more beneficial for black patients in improving patient–clinician communication. 18
These findings demonstrate why it is crucial that the use of ePROs for outpatient care is carefully considered, planned and implemented to ensure that people from underserved populations are not further disadvantaged. 35 Ways to promote inclusive and equitable and inclusive completion have recently been described, including co-designing systems with user input, considering the needs of the target population such as clinical characteristics, cultural and language needs, literacy and health literacy and considering ways to promote digital inclusion. 35 User-centred design may also help promote adherence to completion of ePROs. Digital inclusion and adherence could be promoted by providing alternative modes of delivery, for example, bring your own device, provision of device, web completion or voice response systems (that do not require internet access), phone calls from staff and the options of remote or in-clinic PRO provision. 35
Impact on clinical workflow
Concerns have been expressed that using ePROs for routine patient management could potentially increase clinical workload and negatively impact on workflow if clinicians are uncertain about the benefits of ePRO, are not clear how to integrate ePRO into their practice, do not find PROs clinically actionable and are not consulted on how to build ePRO into their workflow.33,36–39 However, a survey of clinicians who participated in the PROgress study showed that generally the implementation of ePROs was perceived as having a minimal and/or manageable impact on providers’ workload. The clinicians were not unanimous on whether the use of ePROs saved time during consultations. 24 Co-development of systems with clinical input may help ensure that systems meet end user needs; however, further work is required to assess the impact of systems on workflow and workloads.
Cost and cost-effectiveness
The issues of cost and cost-effectiveness could significantly influence the decision by healthcare providers to commission the development and implementation of ePRO systems. 40 A recent review showed that in the long run, ePRO systems could be cost-effective when implemented for routine clinical practice. 40 However, there is a need for studies to evaluate cost-effectiveness specifically in outpatient contexts. There are some important requirements with cost implications that need to be considered early during the planning phase of implementation. For instance, many of the studies we found employed an algorithm to automatically analyse patients’ ePROs and flag concerning issues for attention removing the need for clinicians to review every assessment. Automatic reminders and training (patient and/or clinician) were provided by several studies to enhance completion rates and uptake. Short et al. reported that for in-clinic ePRO provision, on-site research coordinators required approximately 4 min per patient to explain the procedure, monitor ePRO completion and sanitise the tablet used (patients did not have the option of using their own devices). 24
Implications of findings
Our review provides evidence to support the implementation of ePRO systems for outpatient care. The studies reported improvements in healthcare resource utilisation including significant reductions in outpatient appointments without compromising patient outcomes or satisfaction with care. Stable patients who remotely provide their ePROs do not have to attend appointments unnecessarily and only those patients who really need to be seen in person are scheduled for face-to-face consultations. However, further studies will be required to evaluate the long-term impacts on patient safety and outcomes. It is also important to acknowledge that a proportion of patients, especially the elderly, may prefer face-to-face or telephone outpatient consultations regardless of their health status and may be concerned about or averse to the use of ePROs as a triaging tool. Brief telephone consultations in combination with ePRO reporting could be offered to stable patients.
Other potential benefits highlighted in this review include facilitation of the documentation and monitoring of patient symptoms, provision of timely interventions when required and improvement of patient–clinician interaction. While these may have positive effects on patient outcomes and satisfaction with the processes of care, there is an important concern that using ePROs for routine patient management could potentially increase clinical workload and negatively impact on workflow.36–38
ePROs may be implemented for flexible patient-initiated follow-up or for fixed-interval clinician-initiated follow-up. Only one study compared these approaches and there were no significant differences in healthcare resource utilisation or patient satisfaction. 21 The authors suggested that patient-initiated PRO-based follow-up may be used as an alternative to fixed-interval PRO-based follow-up in patients who prefer this approach. 21 The adoption of this approach will require the provision of appropriate patient education to ensure patient safety.
Finally, while several studies in this review confirmed that ePRO systems are highly acceptable to patients, some patients will choose not to engage. It should be noted that aside from the study by Schougaard et al., 20 the duration of the studies was between 3 and 24 months. Therefore, it is not certain that acceptability of the ePRO systems will remain at the same level in the long term.
Looking ahead
Utilisation of ePROs for outpatient care could facilitate the tailoring of care to patient needs. Stable patients can be monitored remotely using ePROs, thereby avoiding unnecessary check-ups in outpatient clinics, associated costs such as travel and time off work, without lowering the quality of treatment. This efficient use of scarce healthcare resources could free up outpatient clinics for patients with high symptom burden/concerning symptoms, so they can be seen more quickly. With appropriate patient education, training and support, patients may potentially engage more in self-monitoring, management and shared decision-making if given access to their ePRO data. Other potential barriers that have been reported in literature can be appropriately addressed to facilitate implementation and uptake of ePROs. 41
In all the studies, ePROs were used to inform clinical decision-making; however, as systems develop, wearables or blood tests could be used to supplement data collected via ePROs, and prediction models could be developed and refined using artificial intelligence to optimise triage approaches. However, these developments may lead to the classification of more ePRO systems as medical devices for regulatory purposes. Developers should ensure that systems are developed in accordance with medical device regulations for the jurisdiction of use. As medical devices, ePRO systems will be required to comply with stricter standards that may be challenging and influence their implementation and evaluation in clinical practice.
The utilisation of ePROs in the delivery of outpatient care could potentially allow a more responsive healthcare system, reduce demand for clinic appointments, reduce time to care with associated improved outcomes and enhance cost-effectiveness of healthcare delivery – all of which are beneficial for patients, their families and society.