
Abstract
Objective:
This study evaluated the surgical and long-term patient-reported quality of life outcomes of patients undergoing esophagectomy with gastric advancement.
Methods:
A retrospective review was performed of all patients undergoing esophagectomy with gastric advancement from 2005 to 2016. Quality of life outcomes were evaluated using the European Organization for research and treatment of cancer quality of life questionnaire - esophageal cancer module (QLQ-OES18), which covered 10 symptom scales: dysphagia, trouble swallowing saliva, choking when swallowing, eating, dry mouth, trouble with taste, trouble with coughing, trouble speaking, reflux, and pain.
Results:
A total of 129 patients were followed up to 16 years (791.3 patient-years). The median age was 63.5 (IQR 55.9-69.3) years, and 79.9% were male. Eighty-six percentage (111/129) of patients had esophageal malignancy as their operative indication. Median survival was 7.1 years, with patients with benign disease experiencing longer postoperative survival (P = .006). The response rate to QLQ-OES18 surveys was 53.7% (22/41; median follow-up: 10.4 years). Patients who experienced early postoperative complications were more likely to report trouble with coughing (P = .032) than those who did not experience early complications. However, postoperative leaks were not associated with worsened QOL. Of note, age ≥ 65 years, obesity status, surgical indication, location of the primary esophageal lesion, tumor stage, and the occurrence of delayed postoperative complications were not associated with long-term QOL (all P > .05).
Conclusion:
Patients undergoing esophagectomy with gastric advancement generally had good quality of life 10 years postoperatively, though early postoperative complications and gender appeared to influence symptom burden. These findings may improve pre and postoperative patient counseling.
Key Learning Points
Patient-reported quality of life outcomes were generally good 10 years following esophagectomy with gastric advancement.
Gender appeared to influence long-term esophageal symptom burden, with females reporting worse quality of life.
Early complications and previous abdominal surgery may also influence long-term quality of life.
Introduction
As the mainstay therapy for esophageal cancer and end-stage benign esophageal disease, esophagectomy rates continue to increase. 1 Despite its benefits, esophagectomy is a morbid procedure, with recent 30-day mortality rates of 3.4% and perioperative complication rates of approximately 30%. 2 Patient-reported outcomes (PROs) include any report of health status directly from the patient without interpretation from the healthcare team. 3 In addition to standard mortality and morbidity outcomes, PROs are a valuable tool to assess outcomes following thoracic surgery and have become increasingly adopted in the field.1,4,5 PROs are an excellent means to assess quality of life (QOL) following surgery, as they can provide valuable insight into patient experiences.
Numerous studies have used PROs to assess QOL following esophagectomy but have relatively limited follow-up duration.6-9 Several high-quality studies assess long-term QOL after esophagectomy, but these are limited to 2 to 5 years of follow-up.2,6,9,10 Moreover, given the relative paucity of studies assessing long-term (beyond 5 years) QOL following esophagectomy for both malignant and benign indications, we aimed to evaluate patient-reported QOL outcomes 10 years following esophagectomy with immediate reconstruction using gastric advancement.
Methods
Study Design and Patient Population
A retrospective review was performed of all patients undergoing immediate reconstruction with gastric advancement following esophagectomy from 2005 to 2016 at our institution. This study was approved by the University of Texas Health Science Center San Antonio Institutional Review Board (Protocol Number: HSC20150617H). Patient characteristics, surgical outcomes, survival, and long-term QOL were assessed. Complications were classified as intraoperative, early, or delayed, depending on their temporal relationship to surgery. Intraoperative complications included tracheobronchial injury, thoracotomy to control bleeding, incidental splenectomy, and colectomy. Early postoperative complications occurred within 30 days and were stratified by pulmonary, cardiac, gastrointestinal, urologic, infectious, neurological, thromboembolic, and wound-related. Delayed postoperative complications, which occurred after discharge or more than 30 days postoperatively, included stenosis or stricture at the anastomotic site, dysphagia requiring a stent or dilations, or delayed gastric emptying.
Quality of Life Questionnaire
Patient-reported QOL outcomes were evaluated using the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire - Esophageal Cancer Module (QLQ-OES18), an 18-item validated metric for assessing esophageal-specific QOL (Supplemental Table 1).11,12 The QLQ-OES18 covered 10 symptom scales: dysphagia (DYS), trouble swallowing saliva (SV), choking when swallowing (CH), eating (EAT), dry mouth (DM), trouble with taste (TA), trouble with coughing (CO), trouble speaking (SP), reflux (RFX), and pain (PA).11,12 Raw scores were standardized via linear transformation using the following formula to create a scale from 0 to 100, with higher scores corresponding to greater symptom burden:

Statistical Analysis
Statistical analysis was performed using GraphPad Prism v9.0 (GraphPad Software Inc, San Diego, CA, USA). For bivariate analysis, Fisher’s exact tests were used for categorical variables. All data were non-normally distributed as assessed by Shapiro-Wilk test; thus, Mann-Whitney U tests were used for continuous variables. Data were presented as numbers and percentages for categorical data and median and interquartile range (IQR) or range for continuous data. Statistical significance was defined a priori as P ≤ .05.
Results
Patient Cohort
A total of 129 patients underwent esophagectomy with immediate reconstruction during the study period. The median age at the time of surgery was 63.5 (IQR 55.9-69.3) years, and 20.2% were female (Table 1). The majority (116/129, 89.9%) were Caucasian race, and 21.7% (28/129) were Hispanic ethnicity. Over half of patients had a history of gastroesophageal reflux disease (72/129, 55.58%). Fifty-seven patients (44.2%) were former smokers, and 26 (20.2%) were current smokers at the time of surgery. Forty-eight (37.2%) had previous abdominal surgery, and 5 (3.9%) had previous foregut surgery.
Demographics, Comorbidities, and Preoperative Characteristics of Patients Undergoing Esophagectomy With Gastric Advancement.
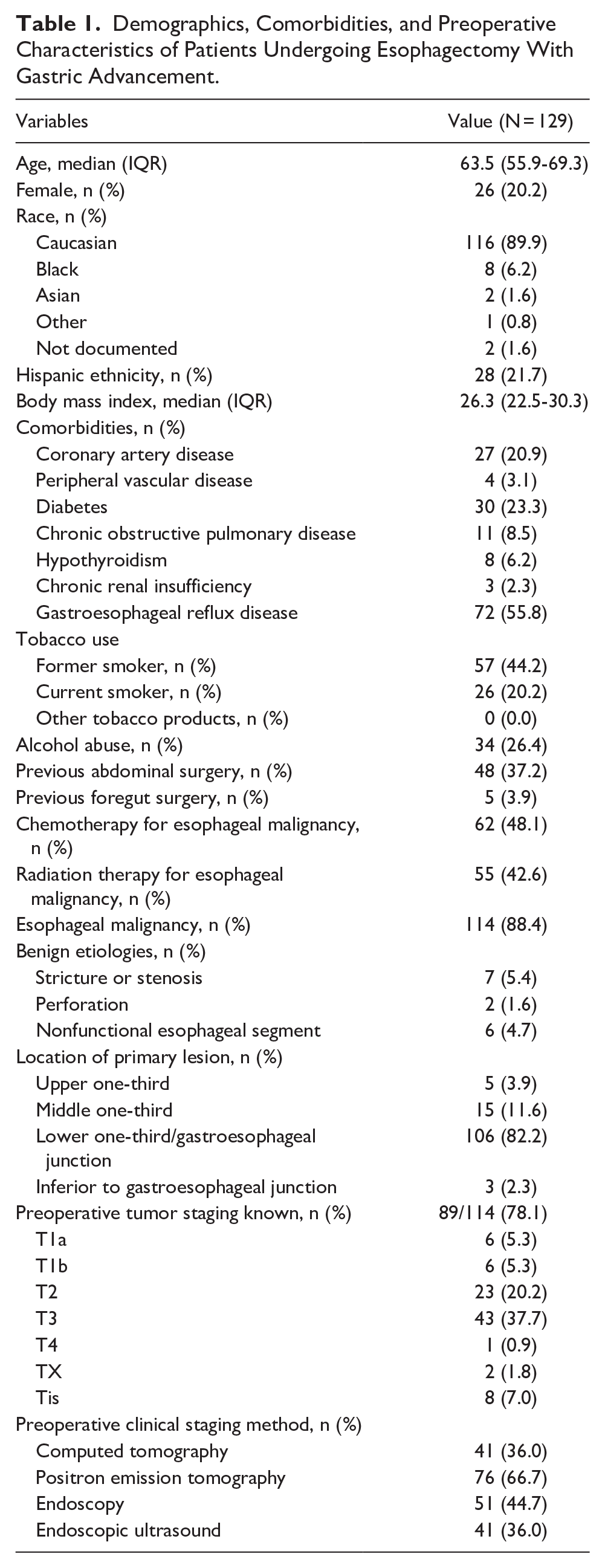
A total of 114 (88.4%) of patients had esophageal malignancy as their operative indication, while 15 (11.6%) had benign disease (stricture or stenosis in 7 [5.4%], nonfunctional esophageal segment in 6 [4.7%], and perforation in 2 [1.6%]). Patients with esophageal malignancy were older at the time of surgery (64.4, IQR 58.7-69.4 years vs 52.2, IQR 46.7-61.5 years; P = .002). Of the 116 with pre-operative biopsies, 96 (82.8%) had adenocarcinoma, 17 (14.7%) had squamous cell carcinoma, 2 (1.7%) were indeterminate, and 1 (0.9%) had both types seen.
The most common location of the primary lesion was the lower one-third of the esophagus or gastroesophageal junction (106/129, 82.2%). Of the 114 patients with esophageal malignancy, 89 (78.1%) had a known tumor stage: 8 (9.2%) were Tis, 6 (6.9%) were T1a, 6 (6.9%) were T1b, 23 (26.4%) were T2, 43 (49.4%) were T3, and 1 (1.2%) was T4. Twenty-seven (20.9%) patients had suspicious nodes identified near the primary lesion, while 2 (1.6%) had suspicious nodes remote from the primary lesion identified. Fifty-five (42.6%) patients received neoadjuvant chemoradiation, 7 (5.4%) received neoadjuvant chemotherapy alone, and 67 (51.9%) received no neoadjuvant therapy.
Intraoperative and Short-Term Outcomes
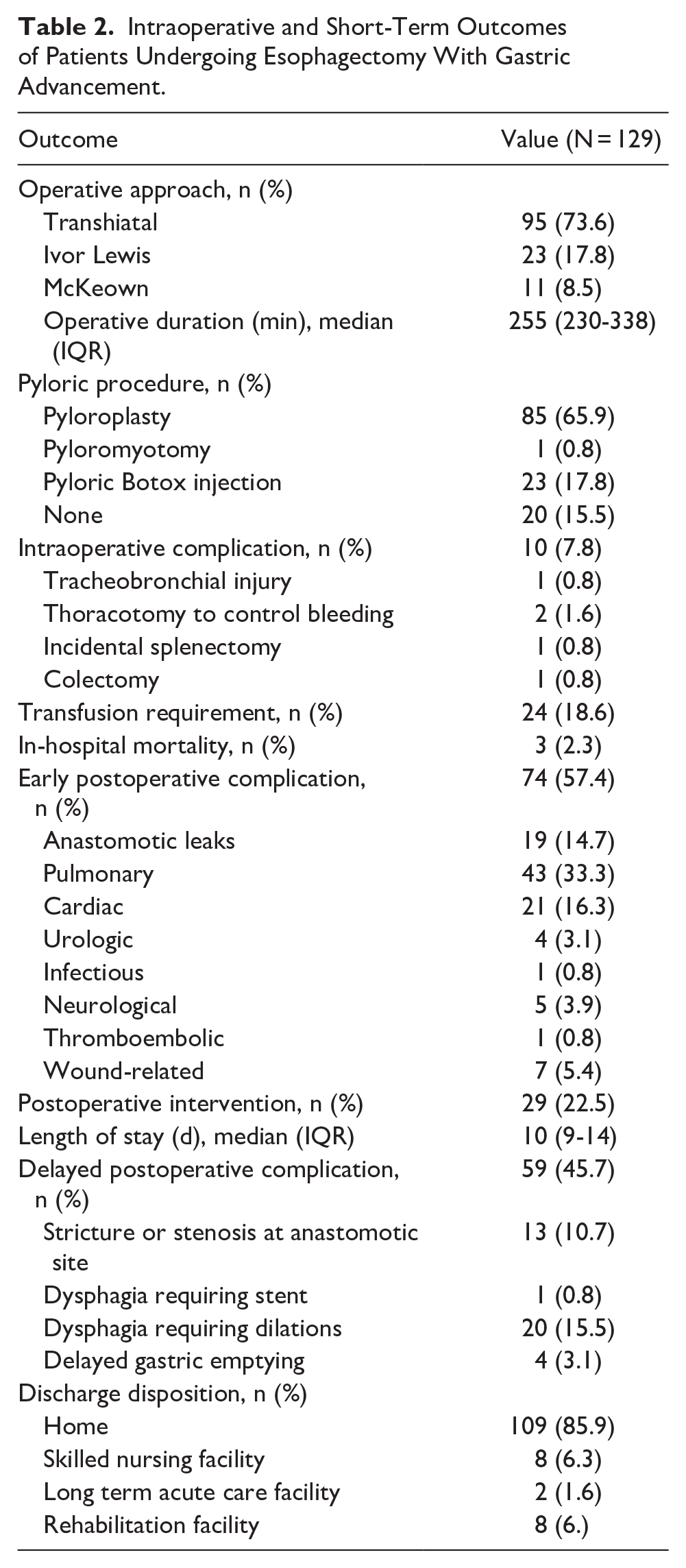
The most common operative approach was transhiatal (95/129, 73.6%), followed by Ivor Lewis (23/129, 17.8%) and McKeown (11/129, 8.5%; Table 2); all surgeries were performed in an open manner. The median operative time was 255 (IQR 230-338) minutes. A total of 109 patients (84.5%) underwent a concomitant pyloric procedure: pyloroplasty in 85 (65.9%), pyloric Botox injection in 23 (17.8%), and pyloromyotomy in 1 (0.8%). Early postoperative complications occurred in 57.4% (74/129) of patients. Pulmonary complications were most common (43/129, 33.3%), and anastomotic leaks occurred in 14.7% (19/129) of patients. The in-hospital mortality rate was 2.3% (3/129). Most patients (109/129, 85.9%) were discharged home.
Intraoperative and Short-Term Outcomes of Patients Undergoing Esophagectomy With Gastric Advancement.
Long-Term Follow-Up and Survival
Patients were followed up to 16 years (791.3 patient-years) postoperatively. The median follow-up duration was 4.7 (IQR 1.6-10.3) years. The median survival was 7.1 years, with a 10-year survival rate of 44.2% (Figure 1A). Patients with benign disease experienced longer postoperative survival than those with malignancy (10-year survival 76.0% vs 39.0%; P = .006; Figure 1B). Of the 51 survivors, 40 (78.4%) had malignancy, 5 (9.8%) had a non-malignant stricture or stenosis, 5 (9.8%) had a non-functional esophageal segment, and 1 (2.0%) had a non-malignant esophageal perforation as their surgical indication.
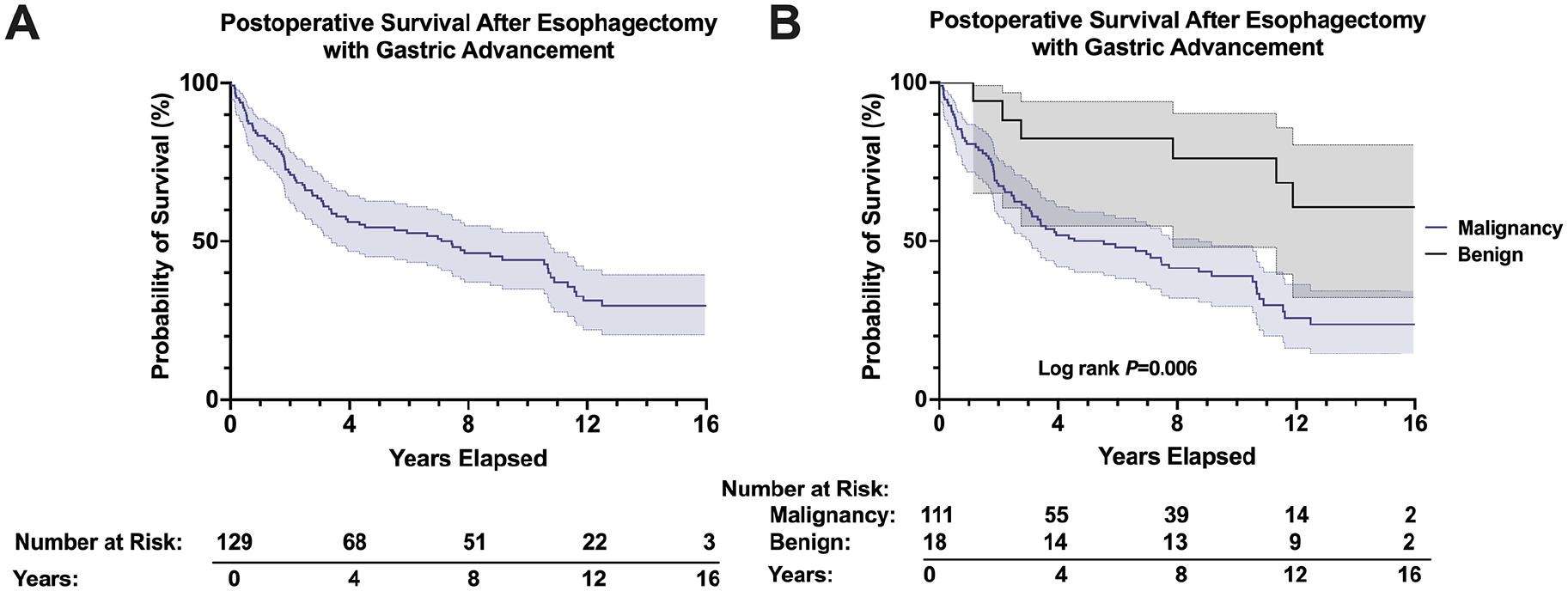
(A) Overall survival of patients undergoing esophagectomy with advancement. (B) Survival stratified by patients undergoing esophagectomy for malignant versus benign indications.
Quality of Life Outcomes
The QLQ-OES18 was mailed out to patients with a documented address and no death on record in June 2022, which included 51 of the original 129 patients (39.5%). Ten (19.6%) surveys were returned as undeliverable. After exclusion of these patients, the response rate was 53.7% (22/41). The median follow-up duration of survey respondents was 10.4 (IQR 9.6-12.9) years. The maximum follow-up duration was 16.0 years. Of the 22 respondents, 1 (4.5%) had evidence of esophageal cancer recurrence 12 years postoperatively, and 1 (4.5%) had newly diagnosed squamous cell carcinoma of the head and neck 9 years postoperatively.
For the QLQ-OES18, a score of zero represents a complete absence of symptoms, with any score above zero defined as abnormal. Patients generally reported low symptom burden, with the most common symptom being reflux (median 50.0, IQR 25.0-75.0), followed by choking while swallowing (33.3, IQR 0.0-33.3), trouble with coughing (33.3, IQR 0.0-33.3), and trouble eating (20.0, IQR 10.0-47.5). All other symptoms, including dysphagia (0.0, IQR 0.0-18.8), trouble swallowing saliva (0.0, IQR 0.0-33.3), dry mouth (0.0, IQR 0.0-33.3), trouble with taste (0.0, IQR 0.0-33.3), trouble speaking (0.0, IQR 0.0-100.0), and pain (0.0, IQR 0.0-25.0), had median symptom scores of zero (Figure 2).
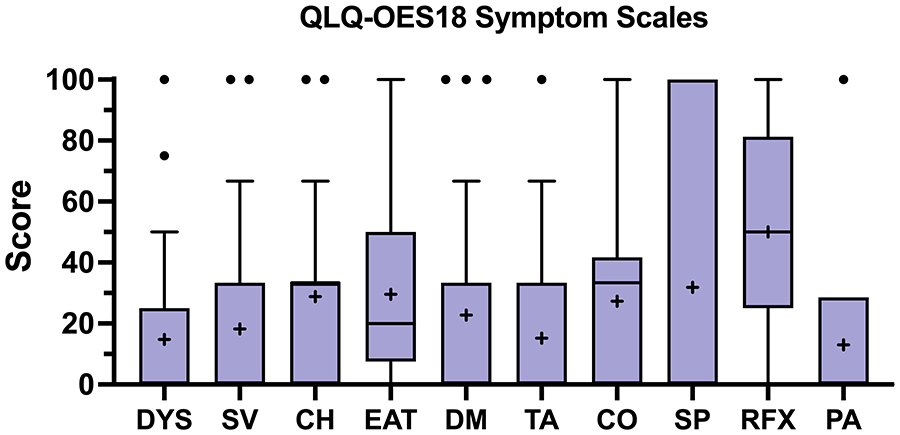
Patient-reported quality of life metrics as assessed by the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire—Esophageal Cancer Module (QLQ-OES18). Whiskers represent Tukey plot and individual points are outliers, box represents 25th and 75th percentiles, middle line represents median, and “+” represents mean.
Gender appeared to influence long-term QOL outcomes, as females (4/22, 18.2%) reported higher rates of trouble swallowing saliva (median 66.7, IQR 25.0-100.0 vs 0.0, IQR, 0.0-0.0; P = .020), trouble tasting (50.0, IQR 25.0-75.0 vs 0.0, IQR, 0.0-0.0; P = .020), trouble coughing (66.7, IQR 58.3-75.0 vs 0.0, IQR, 0.0-33.3; P = .020), and dry mouth (66.7, IQR 25.0-100.0 vs 0.0, IQR, 0.0-25.0; P = .041) compared to males (18/22, 81.8%; Figure 3). Patients with previous abdominal surgery (4/22,18.2%) were more likely to report trouble swallowing saliva (50.0, IQR 25.0-75.0 vs 0.0, IQR, 0.0-0.0; P = .041) and worse dry mouth symptoms (66.7, IQR 25.0-100.0 vs 0.0, IQR, 0.0-25.0; P = .041) than patients who had no previous abdominal surgery (18/22, 81.8%). Patients who experienced early postoperative complications (11/22, 50.0%) were more likely to report trouble with coughing (33.3, IQR 16.7-66.7 vs 0.0, IQR, 0.0-33.3; P = .032) than those who did not experience early complications (11/22, 50.0%). However, postoperative leaks (2/22, 9.1%) were not associated with worsened QOL. Of note, age (<65 vs ≥ 65 years), obesity status, surgical indication (malignancy vs benign disease), location of the primary esophageal lesion, tumor stage, the occurrence of delayed postoperative complications, and follow-up duration (<10 vs ≥10 years) were all not associated with long-term QOL (all P > .05).
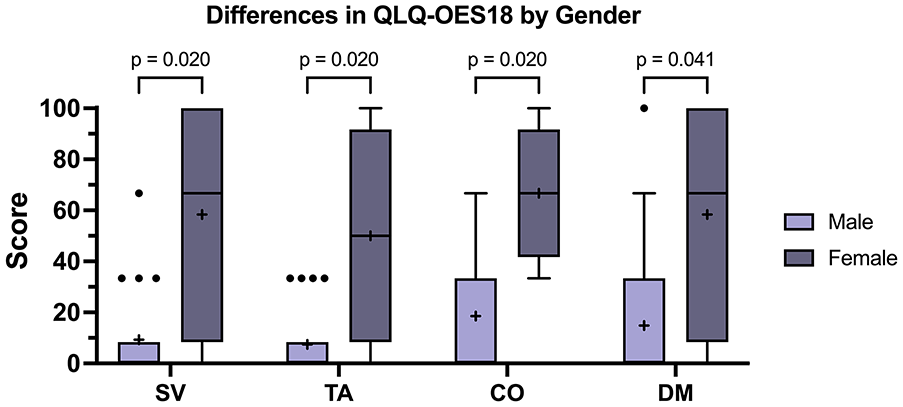
A Significant differences in esophageal-specific symptoms stratified gender. Whiskers represent Tukey plot and individual points are outliers, box represents 25th and 75th percentiles, middle line represents median, and “+” represents mean.
Discussion
This single-institution study evaluated 129 patients undergoing esophagectomy with immediate reconstruction using gastric advancement and assessed patient-reported QOL outcomes 10 years after surgery. Although it is the mainstay therapy for patients with esophageal cancer or end-stage benign disease, esophagectomy is associated with worsened short-term QOL.7,9 Moreover, the results of long-term QOL remain inconsistent.6,9,10,13,14 It is thus important to assess long-term QOL following esophagectomy for both benign and malignant indications. We found that patients reported generally good functional outcomes, such as eating solid foods, and minimal negative symptoms, such as difficulty eating and stomach pain. However, women reported significantly worse long-term QOL outcomes. Additionally, patients who experienced early postoperative complications and those with previous abdominal surgery reported worsened QOL across select scales. These findings may improve pre- and postoperative counseling for patients undergoing esophagectomy with gastric advancement for esophageal malignancy or advanced benign disease.
After a median of 10 years after esophagectomy with gastric advancement, patients in our study generally reported good functional outcomes with minimal negative symptoms. We also found that long-term QOL did not vary by surgical approach (Ivor-Lewis, transhiatal, or McKeown). Similarly, Mantoan et al found that patients undergoing esophagectomy had long-term QOL (median follow-up 4 years) equivalent to healthy subjects, despite persisting issues with eating and reflux. 10 In a scoping review, Darling also noted that long-term health-related QOL after esophagectomy was similar to the average population. 15 In contrast to our findings, she found that QOL recovered more quickly in patients who underwent a transhiatal esophagectomy. 15 Heiden et al 7 found physical function scores were similar among transthoracic or transhiatal approaches 6 months after esophagectomy. If differences by surgical approach were present in our patient cohort, they were likely not captured during our extended follow-up duration. Regardless of approach, we found that patients reported relatively good esophagus-related QOL at 10 years postoperatively.
Gender appeared to significantly influence QOL outcomes, with women being more likely to report trouble swallowing their saliva, food tasting differently, trouble coughing, and dry mouth. Three years following esophagectomy, Akkerman et al 2 similarly described worse physical and social functioning, nausea, dyspnea, and reflux for women compared to men. Although we primarily assessed esophageal-specific QOL, these findings agree with our own. In contrast, Jezerskyte et al 6 found that gender did not significantly influence QOL 2 years after esophagectomy or gastrectomy. Additionally, Reddy et al noted that gender was not associated with OES-18 scores for patients with neoplastic Barrett’s esophagus undergoing esophagectomy or endoscopic therapy (median follow-up 6.8 years). 13 Neither of these studies examined QOL solely after esophagectomy with gastric advancement for benign and malignant disease, which may explain this difference. The modest sample size limited our ability to adjust for other risk factors, which may have influenced esophagus-related QOL. Given these conflicting findings, future studies that assess the effect of gender on QOL outcomes following esophagectomy are warranted.
Patients who experienced early postoperative complications were more likely to report trouble coughing than those who did not experience early complications. However, the occurrence of postoperative leaks was not associated with long-term QOL. Viklund et al found that the occurrence of surgery-related complications, including anastomotic leaks, was the main predictor for decreased QOL 6 months after esophagectomy. This is understandable, given their short postoperative follow-up duration. Interestingly, Derogar and Lagergren 14 found that any major complication following esophagectomy was associated with lower QOL up to 5 years postoperatively. Although it is somewhat surprising that the occurrence of postoperative complications could have significance years after surgery, it supports the association present in this study. In contrast, Katz et al showed that long-term QOL did not significantly vary by postoperative complications. 9 This discrepancy may be attributed to the instrument used to assess QOL. The studies by Viklund et al. and Derogar and Lagergren used the QLQ-OES-18 instrument, which is the same instrument used in this study. Katz et al, however, used the Functional Assessment of Cancer Therapy-Esophageal Module (FACT-E). Given the relatively high rate of postoperative complications observed in this study and others assessing outcomes following esophagectomy, further exploration of the effect of complications on long-term QOL is warranted.
We found relatively low rates of dysphagia and reflux at 10 years postoperatively, which may be related to the anastomotic technique. We stapled the esophagogastric anastomosis using a GIA stapler, laying the stomach posteriorly and superiorly to the esophagus toward the cricopharyngeus. We then closed the common channel using a TA stapler.
The findings of this study, that QOL outcomes 10 years after open esophagectomy are relatively good despite persistent reflux, may aid foregut surgeons, and gastroenterologists as they provide pre- and postoperative counseling. Additionally, women and those who experience early postoperative complications may benefit from further discussion and closer follow-up. As the assessment of QOL and PROs continues to increase in importance for thoracic and foregut surgeons, this study is 1 of few that assesses very long-term outcomes following esophagectomy and may serve as a benchmark for future studies.
This study has a few important limitations, primarily due to the single-institutional design and limited sample size. The low number of returned QOL surveys also may limit the generalizability of our findings. Given the timeframe, we believe that the extended follow-up duration and reasonable response rate (53.7%) help to ameliorate some of these limitations. Importantly, there may be a response bias in our QOL measurements, such that patients who died before the surveys were distributed or who did not complete the survey may have influenced QOL outcomes, either positively or negatively. Third, neither preoperative nor longitudinal QOL measurements were performed in this patient cohort. Thus, we could not assess QOL changes over time or determine how the single QOL survey we measured compared to preoperative QOL. Fourth, despite the numerous benefits of PROs when assessing patient outcomes, it is possible that patients may have misunderstood the QLQ-OES18 without guidance from a healthcare provider. Fifth, we did not capture data regarding adjuvant chemotherapy or radiation, which may have influenced postoperative survival and QOL. Last, all of the surgeries performed in this series were performed by a single surgeon using an open approach. It is possible, though unlikely, that this may limit the generalizability of our findings for surgeons who primarily utilize a minimally invasive approach.
Conclusion
Esophagectomy with gastric advancement resulted in good long-term QOL 10 years after surgery. Females, patients with prior abdominal surgeries, and those who experienced early complications were more likely to report worse long-term, esophagus-related QOL outcomes. Of note, age ≥65 years, obesity status, surgical indication, location of the primary esophageal lesion, tumor stage, and the occurrence of delayed postoperative complications were all not associated with long-term QOL. These findings may improve pre- and postoperative counseling for patients undergoing esophagectomy with gastric advancement for esophageal malignancy or advanced benign disease.
Supplemental Material
sj-docx-1-gut-10.1177_26345161251346926 – Supplemental material for Factors Associated With Quality of Life 10 Years Following Esophagectomy With Gastric Advancement
Supplemental material, sj-docx-1-gut-10.1177_26345161251346926 for Factors Associated With Quality of Life 10 Years Following Esophagectomy With Gastric Advancement by John A. Treffalls, Chirag A Buch, Christian Jacobsen, Nitin A. Das, Rebecca Medina, Marc Koch, Daniel T. DeArmond and Scott B. Johnson in Foregut
Footnotes
Abbreviations
CH: choking when swallowing
CO: trouble with coughing
DM: dry mouth
DYS: dysphagia
EAT: eating
EORTC: European Organization for Research and Treatment of Cancer
IQR: interquartile range
PA: pain
PRO: patient-reported outcomes
QLQ-OES18: Quality of Life Questionnaire - Esophageal Cancer Module
QOL: quality of life
RFX: reflux
SP: trouble speaking
SV: trouble swallowing saliva
TA: trouble with taste
Author Contributions
Conception and design (J.A.T., C.A.B., S.B.J.), analysis and interpretation (J.A.T., C.A.B., D.T.D., S.B.J.), data collection (J.A.T., C.A.B., C.J., N.A.D., R.M., M.K.), statistical analysis (J.A.T., C.A.B.), writing the manuscript (J.A.T, S.B.J.), critical revision (J.A.T., C.A.B., C.J., N.A.D., R.M., M.K., D.T.D., S.B.J.), approval of the manuscript (J.A.T., C.A.B., C.J., N.A.D., R.M., M.K., D.T.D., S.B.J).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the University of Texas Health Science Center San Antonio Institutional Review Board (Protocol Number: HSC20150617H).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Use of Artificial Intelligence
No artificial intelligence (AI) was used in the preparation of this manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.