
Abstract
Objectives
Research suggests that antisocial lifestyles constitute significant health risks. However, there are marked individual differences in the stability of antisocial behaviour. These different offending pathways may bear differential risks for adult health.
Design
Injury and illness data were collected prospectively in the longitudinal Cambridge Study in Delinquent Development.
Setting
Working-class inner-city area of South London.
Participants
Participants included the 411 men from the Cambridge Study in Delinquent Development, with interview data collected at ages 18, 32 and 48 years for each individual.
Main outcome measures
Organic illness, hospitalisation and injuries.
Results
By age 48, adjusted odds ratios showed that the incidence of organic illness was higher among Life-Course-Persistent, Late-Onset offenders and offenders in general. Based on adjusted odds ratios at age 32, the incidence of hospitalisations was higher for Late-Onset offenders. Adjusted odds ratios at age 48 also showed that the incidence of hospitalisations was higher for all three offender types and offenders in general. Our results also provide evidence that offenders were more likely to suffer injuries than non-offenders.
Conclusions
The findings of this study imply that preventing individuals from offending is likely to have substantial benefits for health.
Offending is part of a constellation of social disorders, including truancy and substance abuse, many of which constitute significant health risks and reduction in life success across a multitude of measures, including unemployment, relationship problems, accommodation problems and low educational achievement. 1
The research so far undertaken in this area has suggested that offending may in some way cause poor health.2,3 There is evidence that juvenile delinquents and adult criminals are at increased risk of injury in general. 4 Earlier literature also suggested that sexually transmitted and blood-borne infections are common among criminal offenders.5,6 In addition, tuberculosis, respiratory illness and epilepsy 7 are also frequently seen among offenders.
However, longitudinal investigations of associations between offending and health outcomes are rare. In this regard, an important new opportunity has emerged from the Cambridge Study in Delinquent Development, which provides prospective longitudinal data on injury, illness and treatment-seeking behaviour as well as data concerning offending trajectories.
These data have already been studied in men at ages 16–18 and 27–32 years,3,8 and both positive and negative associations have emerged. For example, convictions up to the age of 32 years were found to be associated with fewer respiratory illnesses and fewer illnesses overall at age 16–18 years and fewer organic illnesses at age 27–32 years. Furthermore, concurrent antisocial behaviour was inversely related to respiratory infections at age 16–18 years and to hospital admissions at age 27–32 years, possibly because of a protective effect of alcohol against infection. 9 Childhood precursors of offending, which were linked to lower risk of infections at age 16–18 years, were high daring and low income. However, poor parental supervision predicted a higher risk of cardiovascular illness at age 27–32 years, while low non-verbal IQ predicted a higher risk of psychological illness at the same age.3,8
Further inverse relations were found between antisocial behaviour at age 18 years and health outcomes at age 32 years – principally between heavy alcohol consumption and infections and organic illness. Self-reported offending at age 32 years was related to low hospital admissions at the same age, although this may be because offenders were less likely to seek treatment.3,8 On the other hand, by age 32 years, earlier antisocial behaviours, like fighting after drinking and heavy smoking, had become positively related to illness 9 – particularly psychological disorders, and low job status was positively related to hospital admissions. Overall, a consistent finding up to age 32 years in the Cambridge Study in Delinquent Development was the link between childhood precursors of antisocial behaviour and later injury, convictions and concurrent antisocial behaviour.
However, there are marked individual differences in the stability of antisocial behaviour. Many people behave antisocially, but their antisocial behaviour is temporary and situational. In contrast, the antisocial behaviour of other people is very stable and persistent. 10 Temporary, situational antisocial behaviour is quite common in the population, especially among adolescents. Persistent, stable antisocial behaviour has been found among a relatively small number of men whose behaviour problems are also quite extreme. 10
The central focus of this article, in contrast to the conviction and risk factor analyses previously performed, 11 is on temporary versus persistently antisocial persons, defined according to Moffitt’s 10 and Jolliffe et al.’s 12 three offending trajectories (Life-Course-Persistent, Adolescence-Limited, and Late-Onset offenders), who constitute qualitatively distinct types of persons.12–17 These different offending pathways may bear differential risks for adult health.12,16–18
By using data from the Cambridge Study in Delinquent Development, this new approach investigates the longitudinal impact of criminal behaviour on physical health problems by testing the following hypotheses: Individuals who commit offences earlier in their lives and have prolonged criminal careers (Life-Course-Persistent offenders) will suffer from greater physical and mental health problems than individuals who have short criminal careers (adolescence-limited offenders). These early onset individuals will also have greater odds of injury and hospitalisation 19 than late-onset offenders, who in turn will have greater odds than non-offenders.
Methods
Cambridge Study in Delinquent Development
Research methods used in this study are described in detail in a report of an investigation of links between offending trajectories, injuries and illness up to the age of 18 years. 3 The Cambridge Study in Delinquent Development is a prospective longitudinal survey of the development of offending and antisocial behaviour in 411 London boys. At the time they were first contacted, in 1961/62, they were all living in a working-class inner-city area of South London. The sample included all the boys then aged 8–9 years and on the registers of six state primary schools within a 1-mile radius of a research office that had been established. Hence, the most common year of birth of these boys was 1953. In nearly all cases (94%), the family breadwinner at that time, usually the father, had a working-class occupation (skilled, semi-skilled or unskilled manual worker). Most of the boys were white (97%) and of British origin.
Interviews and tests
Details of interviews and tests involving the boys, teachers, parents and peers have been published.3,8 The tests at age 8–14 years measured individual characteristics such as intelligence, attainment, personality and psychomotor impulsivity, while the interviews collected information about such topics as living circumstances, employment histories, relationships with females, offending behaviour and leisure activities such as drinking and fighting. The men were interviewed in a research office at ages 16, 18 and 21 years and in their homes at ages 25, 32 and 48 years by trained social science graduates. At all ages except 21 and 25 years, the aim was to interview the whole sample, and it was always possible to trace and interview a high proportion, for example 389 out of 410 who were still alive at age 18 years (95%), 378 out of 403 who were still alive at age 32 years (94%) and 365 out of 394 who were still alive at age 48 years (93%). 1 Criminal records of these men have been traced up to age 61 years, by which time 360 men were still at risk of offending.
Health data
Injury and illness data were only studied 10 years after the data collection began because, previously, no hypotheses relating to health outcomes had been considered. 3 However, it should be emphasised that although health data were not studied for these 10 years, health data collection was prospective in every Cambridge Study in Delinquent Development sweep. Interviewers recorded all illnesses and injuries that had occurred at ages 16–18, 27–32 and 43–48 years, and the number of hospital visits at ages 27–32 and 43–48 years. The illnesses recorded by the interviewers were categorised as Mental, Respiratory Tract, Cardiovascular, Musculoskeletal, Skin, Allergic, Gastrointestinal and Infectious Illness at ages 18 and 32 years. However, at age 48 years, illness data were only categorised into Organic Illnesses and Mental Illnesses. We have therefore chosen to aggregate the illness categories at ages 18 and 32 years into ‘Organic Illness’ and ‘Mental Illness’ variables to allow a direct comparison across these three age groups. This method ensured that data were complete for all individuals across all ages (N = 392). Injuries were categorised according to their cause as sport injuries, assault injuries, industrial injuries and road accident injuries.
In addition to simple odds ratios, adjusted odds ratios are provided, based on binary logistic regressions that controlled for five risk factors at age 8–10 years, which have consistently been among the most important risk factors for convictions 20 : a convicted parent, poor parental supervision, low family income, low non-verbal IQ and high daring. Parental convictions were obtained from criminal record searches. Poor parental supervision referred to the father not knowing where his children were when they were out. Low family income at age 8 years was rated by the psychiatric social workers based on interviews with the parents. Low non-verbal IQ (90 or less) of the boy was measured by the Progressive Matrices test. High daring was rated by parents and peers and identified boys who took many risks in traffic, climbing and exploring. Data were analysed by means of the Statistical Package for the Social Sciences version 24.
Results
Offending trajectories
Descriptive frequencies.
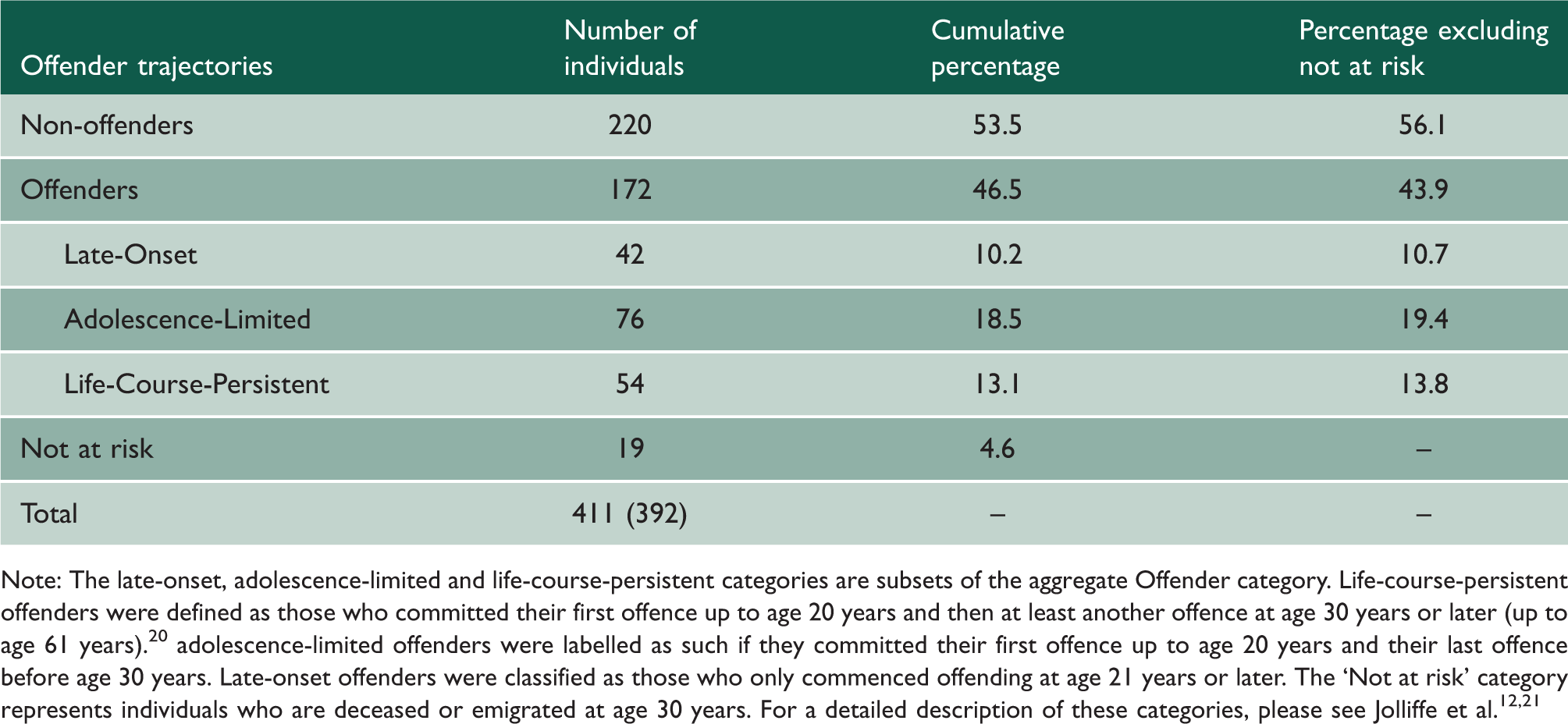
Note: The late-onset, adolescence-limited and life-course-persistent categories are subsets of the aggregate Offender category. Life-course-persistent offenders were defined as those who committed their first offence up to age 20 years and then at least another offence at age 30 years or later (up to age 61 years). 20 adolescence-limited offenders were labelled as such if they committed their first offence up to age 20 years and their last offence before age 30 years. Late-onset offenders were classified as those who only commenced offending at age 21 years or later. The ‘Not at risk’ category represents individuals who are deceased or emigrated at age 30 years. For a detailed description of these categories, please see Jolliffe et al.12,21
Incidence of illness in offender trajectories versus non-offenders up to age 48 years
Incidence and odds ratios of illness and hospitalisation for offenders compared to non-offenders up to age 48 years.
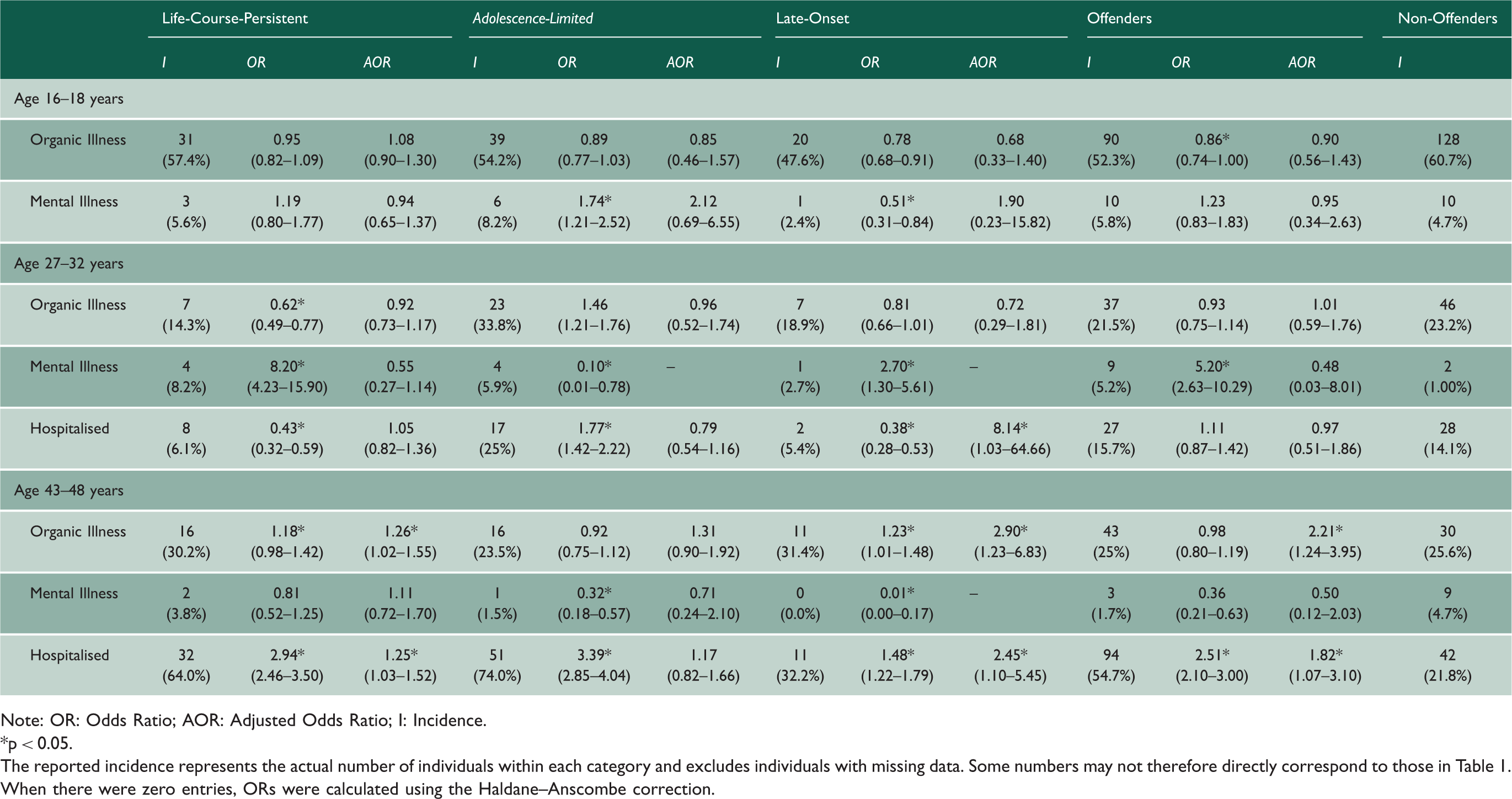
Note: OR: Odds Ratio; AOR: Adjusted Odds Ratio; I: Incidence. *p < 0.05.
The reported incidence represents the actual number of individuals within each category and excludes individuals with missing data. Some numbers may not therefore directly correspond to those in Table 1. When there were zero entries, ORs were calculated using the Haldane–Anscombe correction.
Hospitalisation for offender trajectories versus non-offenders up to age 48 years
Table 2 also presents the incidence and odds ratios of hospitalisation for each offender trajectory at ages 32 and 48 years. Based on unadjusted odds ratios at age 32 years, the incidence of hospitalisation was lower for life-course-persistent and late-onset offenders, but higher for adolescence-limited offenders. Based on adjusted odds ratios at age 32 years, the incidence of hospitalisations was higher for late-onset offenders. Both unadjusted and adjusted odds ratios at age 48 years showed that the incidence of hospitalisations was higher for all three offender types and offenders in general.
Physical injuries of offender trajectories versus non-offenders up to age 48 years
Incidence and odds ratios of physical injuries for offenders compared to non-offenders up to age 48 years.
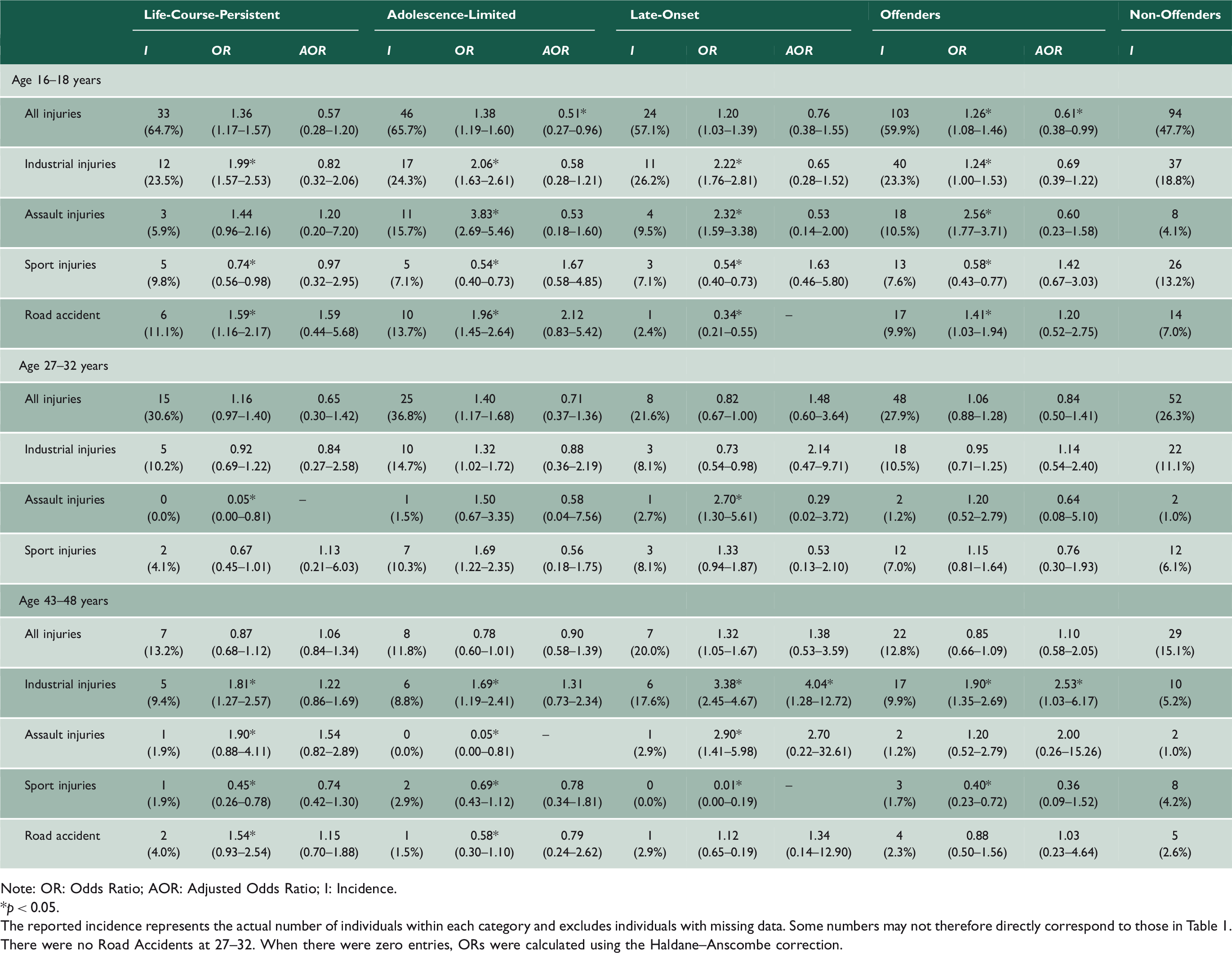
Note: OR: Odds Ratio; AOR: Adjusted Odds Ratio; I: Incidence. *p < 0.05. The reported incidence represents the actual number of individuals within each category and excludes individuals with missing data. Some numbers may not therefore directly correspond to those in Table 1. There were no Road Accidents at 27–32. When there were zero entries, ORs were calculated using the Haldane–Anscombe correction.
At age 32 years, life-course-persistent offenders had a lower incidence of assault injuries, whereas late-onset offenders had a higher incidence of assault injuries. At age 48 years, life-course-persistent offenders had a higher incidence of industrial injuries, assault injuries and road accidents, but a lower incidence of sports injuries. Adolescence-limited offenders had a higher incidence of industrial injuries, but a lower incidence of assault injuries, sports injuries and road accidents. Late-onset offenders had a higher incidence of industrial and assault injuries, and a lower incidence of sports injuries. Offenders in general had a higher incidence of industrial injuries, but a lower incidence of sports injuries.
Based on adjusted odds ratios, at age 18 years, adolescence-limited offenders had a lower incidence of all injuries. Offenders in general, however, had a higher incidence of all injuries, including industrial injuries, assault injuries and road accidents. Offenders in general had a lower incidence of sports injuries. At age 48 years, late-onset offenders had a higher incidence of industrial injuries, as did offenders in general.
Discussion
Principal findings and interpretation in the context of wider literature
This study categorised offenders into three trajectories: Adolescence-Limited, Late-Onset and Life-Course-Persistent; and compared their respective odds of illnesses, injury and hospitalisation. Studies have shown that, while offending rates decrease after adolescence, the impact on health of an antisocial lifestyle during adolescence persists and becomes more apparent in the later decades of life. However, previous researchers have not studied distinct offending trajectories, nor have they controlled for key risk factors. This allows us to ask whether offending predicts worse health after controlling for these predictors. Or, in other words, do these predictors explain the link between offending and health.
Our findings, when considering organic illnesses (Respiratory Tract, Cardiovascular, Musculoskeletal, Skin, Allergic, Gastrointestinal and Infectious Illnesses) and hospitalisations (the number of hospital visits), confirm other work and our hypotheses.3,8,23 They suggest that the impact of offending on health becomes more serious if offending persists beyond adolescence. Our analyses also highlight age-specific health implications related to the ages at which offenders begin and end their delinquent behaviour. When considering mental illness, that is to say individuals with any clinical or sub-clinical indication of a mental illness classified under the DSM-IV, our results somewhat reaffirm conclusions of previous research. For example, Shepherd et al. 8 found that an antisocial lifestyle and offending were linked to more psychological illnesses up to the age of 32 years. 8 The present study found that the incidence of mental illness was higher among life-course-persistent and late-onset offenders and among offenders in general at age 32 years, but lower among adolescence-limited and late-onset offenders at age 48 years. Our results also provide evidence that offenders are more likely to suffer injuries than non-offenders. It is possible that getting injured is another symptom or consequence of an antisocial personality, which arises in childhood and persists into adulthood. Therefore, measures that prevent or reduce offending and antisocial behaviour are likely also to reduce injuries. 24
It is also important to highlight the large impact of adjusting for our risk factors, often minimising odds ratios and in some cases changing the direction of the odds ratio. Although the differences in odds ratios are sometimes large, this is not necessarily surprising. First, the five risk factors were chosen because of their strong established association with convictions. 20 Second, these risk factors were measured at age 8–10 years, after which there were long periods of time for historical forces to shape the social trajectories of family, education and work, which in turn influence behaviour and particular lines of development.
Strengths and limitations
The Cambridge Study in Delinquent Development provides a wealth of detailed information about criminal careers and its association to health, with over a 50-year follow-up period and high retention of the original participants. However, the Cambridge Study in Delinquent Development only contains data mainly on British white, working class, inner city males born around 1953, so the results may not be generalisable to women, Black, Asian, suburban, rural, middle- or upper-class people; people born more recently than the 1950s; or those who spent their childhood in other countries. There was also no opportunity to investigate individuals with gender dysphoria, who are at particularly high risk of psychiatric disorders. 25 The infrequency of the interviews means that accuracy and detail may have been lost as the men had to recall their health over a long period of time. The nature of the measurement of medical data, namely that it was self-reported rather than based on recorded medical data, may have also influenced results. Furthermore, it is important to acknowledge that the large number of odds ratios displayed here means that the interpretation of ‘significant’ odds ratios should be made with care. Overall, this study provides some predictive information, but more information about causal paths from offending to poor health outcomes is needed. Intervention studies using designs that successfully adapt the traditional randomised controlled trial structure are necessary to clarify these.
Implications
The findings of this study imply that preventing individuals from offending is likely to have substantial benefits for health. This has extremely important implications for society. Antisocial behaviour, which persists from childhood into and beyond adolescence, causes a burden and cost to society.26,27 Offenders are more likely than their non-offending peers, or, indeed, their peers with other offending trajectories, to fail to do productive work and impose long-term costs on the health and welfare services. 1
Overall, our findings in relation to organic illness and hospitalisation suggest that addressing the predictors of chronic offending, by reducing childhood risk factors,14,15 for example, through nurse–family partnerships and child skills-training programmes, which are both known to be effective, may contribute to improving health in middle-aged men as well as reducing long-term offending.28–30 Our findings also highlight the importance of preventing individuals from commencing offending at a later age, due to the increased odds of injury and possible disability. 22
Conclusion
This study has highlighted that offending is a public health issue, 23 and collaborative research between clinical academics and criminologists is important in advancing knowledge about offending and about ill-health associated with offending, aiming to minimise disability of individuals and costs to society. 31 At present, the prevention of offending and the prevention of injury and illness are considered and organised separately. The findings of this study suggest that a more integrated and targeted approach to prevention – in which offender rehabilitation and public health academics collaborate – would pay substantial dividends.