
Abstract
Introduction
This study explores the association between self-perceived personal and community changes due to COVID-19 and health among vulnerable primary care patients experiencing multiple chronic conditions.
Methods
Between September 2017 and February 2021, we obtained data from 2,426 primary care patients managing multiple chronic conditions from across the United States. We assessed the relationship between self-perceived personal and community changes due to COVID-19 and change in health measured by the PROMIS-29 mental and physical health summary scores, GAD-7 (anxiety), andPHQ-9 (depression), and DASI (functional capacity) adjusting for relevant demographic, neighborhood characteristics, and county covariates.
Results
After adjustment, self-perceived personal and community changes due to COVID-19 were associated with significantly worse mental health summary scores (ß = -0.55; 95% Confidence Interval (CI) = -0.72, -0.37), anxiety (ß = 0.28; 95% CI = 0.16, 0.39), depression (ß = 0.35; 95% CI = 0.22, 0.47), and physical health summary scores (ß = -0.44; 95% CI = 0.88, 0.00). There was no association with functional capacity (ß = - 0.05; 95% CI = -0.16, 0.05).
Discussion
Among adults managing multiple chronic conditions, self-perceived personal and community changes due to COVID-19 were associated with health. This vulnerable population may be particularly susceptible to the negative effects of COVID-19. As we do not know the long-term health effects of COVID, this paper establishes a baseline of epidemiological data on COVID-19 burden and health among primary care patients with multiple chronic conditions.
Introduction
The SARS-Cov-2 (COVID-19) pandemic and associated public health crises has impacted health and wellness.1,2 Although the impact can be severe for those infected with COVID-19, the societal and economic disruptions have change personal routines and behaviors for many others. High rates of unemployment and loss of health insurance amplify the negative health consequences. 3 Many people have been staying home, either voluntarily or under state order, which can lead to reduced levels of physical activity 4 and subsequent poor mental and physical health, 5 social isolation, and depression. 6 Reduced childcare and school closures increases stress for parents, which may have a ripple effect on their health. 7 Closures and reduced access to medical care can lead to delays in seeking healthcare and worse health. 8 The influence of the pandemic is pervasive with the potential to have a long-lasting impact on both mental and physical health.
Both being infected with COVID-19 and the societal and economic disruptions of the pandemic can affect vulnerable populations more intensely. A cross-sectional study found significant relationships between socioeconomic characteristics, racial, and environmental factors (such as crowded housing and reliance on public transportation) and COVID-19 incidence and mortality. 9 Counties with less wealth and more individuals experiencing disability have higher morbidity rates. 10 COVID-19 infections and fatalities are both associated with social determinants of health, racial and ethnic minority populations, crowded housing, and decreased access to primary care.11–13
Individuals living with multiple chronic conditions may be particularly vulnerable to poorer health outcomes due to COVID-19. 14 Indeed, COVID-19 hospitalization and case fatality rates are higher among those with multiple chronic conditions. 15 Further, the emotional burden may be greater among those already struggling to maintain their health. 16 A recent study found an association between COVID-19 burden and worsening mental health among patients with anxiety or depression disorders, but did not focus on multiple chronic conditions. 17 A literature review of 28 articles highlighted the deficit of studies examining the impact of COVID-19 on patients’ managing multiple chronic conditions and concluded a critical need for future research. 15
This study addresses several gaps in the literature. First, aside from the physical activity literature, there is a paucity of studies assessing the impact of COVID-19 burden on physical health, especially among those with multiple chronic conditions. Second, very few studies have investigated the mental health impact of COVID-19 on patients with multiple chronic conditions. Third, few COVID-19 studies have controlled for pre-pandemic health. We sought to address these gaps and establish a baseline of epidemiological data by assessing the impact of the COVID-19 pandemic on health in primary care patients with multiple chronic conditions. We hypothesized that participants with a higher self-perceived personal and community changes due to COVID-19 would have worse health outcomes.
Methods
Setting and sample
This is a secondary data analysis of a large, cluster-randomized, pragmatic clinical trial, Integrating Behavioral Health and Primary Care (IBH-PC), which assessed the effectiveness of a practice-level intervention designed to improve outcomes in patients with multiple chronic medical and behavioral health conditions by increasing the practice’s degree of behavioral health integration. 18 The original trial found no effect of the practice-level intervention on patient health. Patients with multiple chronic conditions were recruited from 41 primary care practices in 13 states and patient-reported surveys were collected via phone, mail, or online at three time points.
Baseline surveys were collected pre-COVID-19, while follow-up surveys were collected during the COVID-19 pandemic. Surveys were administered between September 2020, and February 2021, a median of 227 days (IQR 208 to 243). All data was collected prior to vaccines being widely available. Eligible participants had both a chronic medical and a behavioral health condition, or three or more chronic medical conditions from the following list (arthritis; obstructive lung disease; non-gestational diabetes; heart disease; mood disorder; chronic pain; insomnia; irritable bowel syndrome; or substance misuse). Electronic medical records were reviewed to determine patient eligibility.
Measures
Patient surveys included demographic information, health outcomes at both baseline and follow-up, and for follow-up data only, specific questions on self-perceived personal and community changes due to COVID-19. County-level unemployment rates as well as COVID-19 prevalence, incidence, and mortality rates based on state and local health agency reports were gathered from The New York Times data. 19
Health outcomes
The outcome measures were the change in Patient-Reported Outcomes Measurement Information System®-29 (PROMIS-29) physical and mental health summary scores, 20 Generalized Anxiety Disorder-7 (GAD-7), 21 Patient Health Questionnaire-9 (PHQ-9), 22 and Duke Activity Status Index (DASI), 23 collected at both baseline (pre-COVID-19) and follow-up (during COVID-19). The PROMIS-29 24 is a self-reported questionnaire that assesses eight domains of health including pain interference, pain intensity, physical function, depression, anxiety, fatigue, sleep disturbance, and social participation. From these domains, physical and mental health summary scores are calculated. These summary scores are reported in t-scores such that the mean of the adult US population is 50 and the standard deviation is 10. Higher scores indicate better health. The PHQ-9 and GAD-7 are questionnaires that measure depression and anxiety symptom severity on continuous scales from 0-27 and 0-21, respectively. Higher scores indicate increased severity. The DASI is a 12-item questionnaire that estimates highest achievable Metabolic Equivalent of Task (METs) units (2.74-9.89) where higher METs indicate better functional capacity. All outcomes were measured continuously.
Self-perceived personal and community changes due to COVID-19
Self-perceived personal and community changes due to COVID-19.

Information on change in income, disruption in schooling, delay of medical care, and loss of employment childcare, and insurance due to COVID-19 was collected as binary yes/no questions for descriptive purposes.
Covariates
For each of the five outcomes, the respective baseline measure of health was included as a covariate in the model, effectively assessing change in health. For example, in the mental health summary score (PROMIS-29) model, the primary outcome was mental health at the follow up visit (during the pandemic); the baseline pre-pandemic mental health summary score (PROMIS-29) was included as a covariate in the model.
Potential confounders were chosen based on clinical knowledge and prior literature including age, gender, race, ethnicity, marital status, employment, annual household income, education, the number of qualifying chronic conditions, financial, housing or food insecurity, county-level estimates of unemployment, county-level incidence of COVID-19, and the Social Deprivation Index 25 (SDI), all measured at baseline. The SDI is a census tract-level composite measure of deprivation derived from the American Community Survey based on income, education, employment, housing, single-parent household, and access to transportation.
For the county-level variables, participant’s home addresses were geocoded, and the appropriate county was assigned to the record. County-level incidence data were merged with the patient dataset based on county in which the participant’s home address resides and the date they took the survey. Unemployment data were matched to the month the participants completed the survey.
In several subanalyses, the practice-level intervention used in the parent trial was included as a covariate and effect modifier in each model.
Statistical analysis
We summarized patient information by the five levels of self-perceived personal and community changes due to COVID-19. Chi-squared tests and analysis of variance were used to assess bivariate relationships. Relative differences in health outcomes were calculated between the highest and lowest quintiles of self-perceived personal and community changes due to COVID-19. Multivariable regression models accounting for baseline mental and physical health were used to assess how self-perceived personal and community changes due to COVID-19 were associated with mental and physical health during the COVID-19 pandemic. Linear regression was used to assess perceived personal and community changes and mental health. However, the bivariate relationship between self-perceived personal and community changes due to COVID-19 and physical health violated the linearity assumption for linear regression, therefore we dichotomized self-perceived personal and community changes due to COVID-19 for physical health (Not at all, A little, Some, vs. A lot, Everything is different now) and used logistic regression. Stata (Version 16; StataCorp, College Station, Texas) was used for data management and analysis.
All study procedures were approved by The University of Vermont Committees on Human Research (CHRMS#16-554). Informed consent was provided by all study participants.
Results
Characteristics of the participants at follow-up stratified by self-perceived personal and community changes due to COVID-19.

*Reverse scale: higher scores are better.
IQR = inter-quartile range; DASI = Duke Activity Status Index; METs = metabolic equivalents.
Multiple regression coefficients of self-perceived personal and community changes due to COVID-19 on mental health.
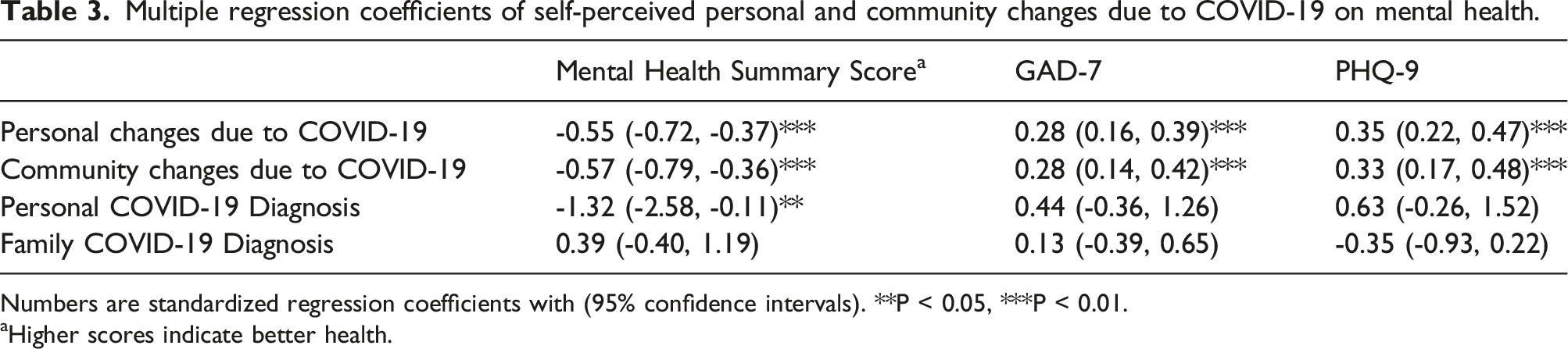
Numbers are standardized regression coefficients with (95% confidence intervals). **P < 0.05, ***P < 0.01.
aHigher scores indicate better health.
Multiple regression coefficients of self-perceived personal and community changes due to COVID-19 on physical health

Numbers are standardized regression coefficients with (95% confidence intervals). **P < 0.05, ***P < 0.01.
aHigher scores indicate better health.
bDichotomized due to non-monotonic relationship with physical health outcomes.
Several subanalyses was performed which included the practice-level intervention of the parent trial as a covariate and interaction in independent models. In each model in which the intervention was included in the model as a covariate, there was no change to the thousands place in the coefficient. Similarly, changes due to COVID-19 did not significantly vary by whether the patients were form and intervention or control site.
Discussion
This study examined the longitudinal impact of self-perceived personal and community changes due to COVID-19 on mental and physical health outcomes. We found that perceived personal and community changes due to COVID-19 were associated with worse mental and physical health, even after accounting for pre-pandemic health, personal and neighborhood characteristics, and local incidence of COVID-19. We do not know the long-term health effects of COVID, which amplifies the importance of this paper establishing a baseline of epidemiological data on self-perceived personal and community changes due to COVID-19 and health.
The impact of the pandemic, especially on mental health, was quite large. Across the range of reported change due to COVID-19 (from “not at all” to “Everything”), there was a 10% difference in mental health summary scores, 64% difference in GAD-7, and a 47% difference in PHQ-9 scores. However, the differences in physical health (0-1.5%) were not as dramatic. Interestingly, personal diagnosis of COVID-19 was only associated with a modest decrease in mental health function and a COVID-19 diagnosis of a family member was not related to any measure of health. This suggests that the personal changes due to COVID-19 may be more associated with mental and physical health than being diagnosed with COVID-19.
Our findings are consistent with previous literature on the negative impacts of COVID-19 on mental health. A systematic review of 43 studies found mental health (post-traumatic stress and depression) was worse among those directly and indirectly affected by the COVID-19 pandemic. 26 Among a generalizable sample of US adults, diagnosis of COVID-19, mortality in acquaintances, and COVID-19-associated stress were predictive of worse mental health. 27 Less than a month into the pandemic, a sample of the general population from Italy reported worse mental health than before COVID-19. 28 Similarly, we found that mental health decreases with increased reported self-perceived personal and community changes due to COVID-19.
Although we did not see a statistically significant association between COVID-19 diagnosis and anxiety or depression as measured by the GAD-7 and PHQ-9, the coefficients were going in the expected direction, suggesting we had too few cases. 2 The PROMIS-29 mental health functioning subscale includes questions related to anxiety, depression and social function. 20 As individual emotional reactions to COVID-19 may vary, it makes sense that a global measure that captures the broad range of emotional functioning would lead to a stronger outcome. Future research exploring emotional and physical functioning among a larger sample of patients with multiple chronic conditions that had personally experienced COVID-19 and/or had family members that had been diagnosed is recommended to better understand this relationship.
Although the COVID-19 pandemic is associated with reduced physical activity, 29 few studies have investigated the impact of self-perceived personal and community changes due to COVID-19 on physical health. A study of patients with advanced respiratory disease, found that the number of months spent in isolation was associated with worse mental and physical health. 5 Nationally, we know that citizens were asked to isolate and distance as part of government and public health measures. Although this isolation varied based on local policy and individual preference, our findings that self-perceived personal and community changes due to COVID-19 was associated with worse health support previous findings. Future research could explore the relationships between degree of isolation and health among patients with multiple chronic conditions.
There are a multitude of mechanisms by which self-perceived personal and community changes due to COVID-19 may affect health. Mandated restrictions of social gatherings, social distancing, and quarantining are necessary measures to slow the spread of COVID-19, but can lead to social isolation and loneliness as well as reduced physical activity. These effects may be exacerbated among older populations with chronic conditions.30,31 COVID-19 has increased levels of stress from disruptions in schedules, changes in finances, loss of jobs, uncertainty about the future, loss of childcare, housing instability etc. which all affect overall health and wellbeing.6,32,33 Twenty percent of our participants reported a change in income due to COVID-19. Meanwhile, in a time of great need, there has been a reduction in routine medical and mental health care utilization. 34 These factors lead to a vicious cycle that negatively impacts wellness, as evidenced by our findings.
This study exhibited several strengths. The longitudinal nature of the data and the timing of the assessments (pre-& during-COVID-19) allowed the unique opportunity to control for pre-COVID health status. Not controlling for baseline health status can result in artificially inflated coefficients, resulting in an overestimation of the effect. 35 In this study, even after adjusting for baseline health, self-perceived personal and community changes due to COVID-19 significantly affected both mental and physical health.
There were also several limitations. These data were collected prior to vaccines being widely available and may not reflect more recent conditions. However, this study established a baseline measure to which similar future studies can be compared. The survey items about self-perceived personal and community changes due to COVID-19 questions were created by the authors, as no suitable surveys were available at the time. Although not validated, they have face validity, low burden and good response rates, and show promise in terms of construct validity, as they are associated in the expected way with several demographic and health outcomes. The results of this study may not generalize beyond US primary care patients who have multiple chronic conditions and access to primary care. However, the sample did include a broad spectrum of age, race, gender and geographic groups, including both urban and rural participants. COVID-19 vaccines were not available during data collection periods.
The COVID-19 pandemic has increased uncertainty, which can lead to psychological and physiological distress. 36 Here, we show that self-perceived changes due to COVID-19 affect mental and physical health. Future studies should investigate this relationship during the era of vaccines and as society adjusts to the new normal. 37
Footnotes
Authors’ note
The views, statements, and opinions presented are solely the responsibility of the authors and do not necessarily represent the views of PCORI, its Board of Governors or Methodology Committee.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded through a Patient-Centered Outcomes Research Institute (PCORI) Award (PCS-1409-24372).