
Abstract
Purpose
Self-rated physical health (SRPH) and self-rated mental health (SRMH) are both linked to excess morbidity and premature mortality and can vary across rural and urban contexts. This can be particularly problematic for rural residents who have less access to important health care infrastructure. In this paper, we assess the prevalence of and rural-urban disparities at the intersection of SRPH and SRMH, specifically self-rated physical/mental multimorbidity (SRPMM) overall and across rural-urban contexts.
Methods
Using a cross-sectional demographically representative national dataset of over 4000 working age adults in the U.S., we expose rural-urban differences in the prevalence of SRPMM and explore individual-level factors that may explain this disparity.
Results
Approximately 15 percent of working age adults reported SRPMM, but rural adults were at higher risk than their urban counterparts. However, this disadvantage disappeared for remote rural working-age adults and was attenuated for metro-adjacent rural working-age adults when we controlled for the fact that rural adults had lower household incomes.
Conclusion
Findings reveal a higher risk of SRPMM among rural adults, in part because of lower incomes among this group. This work acts as the foundation for facilitating research on and addressing rural-urban disparities in SRPMM.
Keywords
Background
Concurrent self-rated poor/fair mental and poor/fair physical health, or self-reported physical/mental multimorbidity (SRPMM), is a serious public health concern. Studies across diverse populations and health conditions have consistently demonstrated that self-rated poor/fair health is predictive of morbidity and mortality.1-3 Populations with poor/fair mental and physical health incur greater costs due to health care utilization4,5 and health-related productivity loss 6 as well as faster rates of biological aging determined through biomarkers. 7 Moreover, the reinforcing nature of coexisting physical and mental health conditions further increases the risk for future health declines.8-11 It is estimated that 8-17% of adults in the U.S. live with multimorbidity; those persons diagnosed with the co-occurrence of an index condition (mental or physical) with a single chronic condition from the other domain (mental or physical).12,13 However, the prevalence, and therefore the symptom burden of multimorbidity, is likely underestimated13-15 because estimates are largely based on data from specific clinically diagnosed mental or physical health conditions.16,17 Use of self-rated measures of mental and physical health provide an opportunity to assess prevalence of SRPMM as a population-level proxy for multimorbidity, as they are based on symptoms of disease rather than clinical diagnosis. At the same time, there are calls for greater attention to mental and physical comorbidities to be assessed and monitored at the population level. 18 However, lack of access to national demographically representative survey data on SRPMM minimizes our ability to evaluate the population prevalence of SRPMM, or to determine if disparities exist across social determinants of health, including rural-urban populations. Therefore, in this study we answer three research questions: 1) What is the prevalence of SRPMM among working age adults?; 2) Are there rural-urban disparities in SRPMM?; and 3) Are rural-urban disparities in SRPMM explained by individual sociodemographic characteristics?
We operationalize SRPMM using existing single-item measures of SRMH and SRPH. These items have undergone extensive psychometric testing and provide data on symptom burden within a population rather than prevalence data on a clinically diagnosed condition.19-22 Although the validity and reliability of single-item measures of SRMH and SRPH have been criticized,20,23 they demonstrate strong validity and reliability as population health measures. 19 Furthermore, validation studies have reinforced that SRMH and SRPH measures are highly correlated to objective health measures and health states.24,25 While neither measure was designed to discriminate specific health conditions within individuals, they capture self-perceptions of subjective health at the population level.1,19,27 Moreover, some argue that self-report is a better indicator of overall health status than using confirmed diagnoses or other objective health measures.2,20 For example, self-report captures individuals who may experience symptoms of mental or physical health conditions in the absence of a diagnosis, as well as those with diagnosed conditions whose symptoms are well-controlled or who have adapted their lifestyle to prevent symptom burden. 14 Although single-item measures of SRMH and SRPH have some degree of conceptual overlap, each measure captures distinct health domains and have been shown to provide greater information about overall health status when assessed jointly than alone.2,20,23 Considering their strengths and limitations, SRMH and SRPH are recommended for use as indicators of overall population health, or to monitor general mental or physical population health.19,27,28
SRMH and SRPH as single-item questions have been included in population-representative studies.29-31 While nearly all major population representative health surveys in the U.S. include the item for SRPH, these do not include both SRMH and SRPH32-34 preventing assessment of SRPMM. An exception was the National Health Interview Survey (NHIS), which included both items in 2010 only. 30 Although studies on specific populations (e.g., anxiety disorders in those with chronic health conditions) routinely examine the intersection of physical and mental health, infrequent use of the single-item SRMH and SRPH measures combined with the specificity of their target population make data aggregation or generalizing from these studies problematic.35-38 Therefore, a means to assess SRPMM across rural-urban contexts and socio-demographic groups at the population level has not previously been possible.
Rural residents are less likely to receive routine health screening or report a usual source of care or usual health care provider, and they are more likely to forgo care and report chronic symptom burden than their urban counterparts. 39 Moreover, rural populations experience a greater burden of illness39,40 due to access-related barriers such as fewer and unequally distributed healthcare providers , 41 unavailable local services, long travel distances, lack of public transportation options, (e.g., lack of or unreliable vehicle, no driver’s license), and financial burdens associated with care.39,42 In addition, there is a long history of rural and urban disparities in overall mortality, 43 including cancer, heart disease, stroke, unintentional injury,44,45 suicide, 46 and motor vehicle fatalities. 45 Limited work has examined the risk factors of SRPMM and – to the authors’ knowledge – no studies have undertaken rural-urban comparisons. Studies that do exist focus on just SRPH or just SRMH. For example, higher rates of poor/fair SRPH have been reported in some rural areas (e.g. metro-adjacent rural) than urban areas.47,48 However, findings vary for SRMH between rural and urban locales.49,50 When examined across the rural-urban continuum, the data suggest a higher burden of mental health problems in transition regions between urban and rural communities than found in either urban or rural areas.51,52 At this point in time, no prior research has determined if this history of rural-urban health disparities is also present for SRPMM and if other individual-level factors may explain such population-level differences.
SRMH and SRPH also vary across sociodemographic characteristics. Low income, unemployed adults, and racial and ethnic minorities report higher rates of poor/fair SRMH53-55 and SRPH.48,55,56,57 Reports of SRMH and SRPH were lowest for those who were divorced or separated.20,49,58,59 While SRPH tends to decline with age,47,53,55 SRMH varies across different life stages displaying a u-shaped curvilinear relationship, with higher rates of poor/fair mental health during middle adult years, and lower rates for younger- and older-aged persons.54,60 Assessments of self-rated health are also shaped by cultural and linguistic factors20,61,62 contributing to potential measurement differences across race, ethnicity and gender.1,62,63 Research on SRPMM has the potential to identify disparities and inform prevention efforts that could offset long-term health care costs, as well as the costs associated with lost productivity.18,64-66
Methods
Data and sample
In this paper we used data from the National Well-being Survey (NWS), a demographically representative cross-sectional online survey of 4,014 working age adults in the United States that was collected in February and March of 2021. The NWS includes previously validated measures of mental and physical health. Respondents were recruited by Qualtrics Panels and provided electronic informed consent prior to starting the survey. Compensation varied in amount and form depending on the method of recruitment used by Qualtrics. County identifiers were collected from respondents, but no identifying individual information was collected. Quotas were used to ensure the sample was demographically representative of the U.S. working age population by sex, age, and race/ethnicity. Rural areas were over-sampled to ensure a robust sample size from these areas. Given this oversampling and a slight over representation of higher educated respondents, a post-stratification weight was created to ensure the sample was representative by age, sex, race/ethnicity, and education. All analyses incorporate the weight variable unless otherwise stated. Additional details on recruitment, compensation, and the survey weight (including the U.S. population marginals used to create the weight) for the NWS data can be found in Monnat (2021, p 115). 67 The NWS survey received approval from the Syracuse University Institutional Review Board (IRB # 20-290). Use of NWS data for this project was determined to not need review by the Penn State University Institutional Review Board (Submission ID: STUDY00020103).
Measures
In this paper, we examine the prevalence of SRPMM – those reporting both poor/fair mental and physical health – and how it varies across the rural-urban continuum. To create the SRPMM measure, we used two self-rated health questions: “In general, would you say your physical health is,” and “In general, would you say your mental health is.” Response options for both questions included excellent, very good, good, fair, poor, and don’t know. Based on widely reported conventions,22,68,69 responses for each question were recoded into poor/fair=1 and excellent/very good/good=0. Those reporting “don’t know” were excluded from analyses. Responses were merged to create a four-category measure of self-reported mental and physical health: • Concordance: Poor/fair SRMH and SRPH (SRPMM) • Concordance: Good or better SRMH and SRPH • Discordance: Poor/fair SRMH and Good or better SRPH (-MH/+PH) • Discordance: Poor/fair SRPH and Good or better SRMH (-PH/+MH)
Individual socio-demographic variables included self-identified sex (female vs. male), race/ethnicity (Hispanic vs. non-Hispanic Black vs. non-Hispanic White vs. non-Hispanic other race), relationship status (married or in a committed relationship vs. single, divorced or widowed), income (<$25,000 vs. $25,000 < $50,000 vs. $50,000 < $75,000 vs. $75,000 < $100,000 vs. > $100,000 vs. don’t know), and employment status (employed vs. unemployed or on disability vs. students, retirees, and homemakers). The NWS data includes Rural-Urban Continuum Codes (RUCC) from the Economic Research Service. 70 We recoded the RUCC codes into urban counties (RUCCs 1-3), rural counties that are adjacent to metro areas (i.e. metro-adjacent rural counties) (RUCCs 4,6,8) and rural counties that are not adjacent to metro areas (i.e. remote rural counties) (RUCCs 5,7,9). Finally, models were also adjusted for self-reported COVID-19 impacts. Respondents were asked “All things considered, what impact would you say COVID-19 has had on your life?” Those reporting a negative impact were recoded as 1 and those reporting a positive impact or no impact were recoded as 0.
Given concerns about the internal and external validity of the SRMH measure,20,71 we conducted sensitivity analyses using an alternative measure of mental health: psychological distress using the PHQ-4. The PHQ-4 is a brief screening tool used to identify persons with symptoms consistent with anxiety and depression. Although psychological distress is commonly used to describe a positive screen, neither the symptom burden nor a diagnosis can be implied from the results. Respondents were asked “During the past two weeks, how often have you been bothered by…: Having little interest or pleasure in doing things; Feeling down, depressed, or hopeless; Feeling nervous, anxious, or on edge; Not being able to control worrying.” Response options included: not at all (0), some days (1), more than half of days (2), nearly every day (3), and don’t know (98). The scores were summed then categorized into the following four groups: normal (0-2), mild (3-5), moderate (6-8), and severe (9-12). 72 Summed scores were then dichotomized into normal (0-2) and mild/moderate/severe (3-12) for the sensitivity analysis. Those respondents who were missing data from the PHQ-4 screening tool and whose summed scores were not greater than 2 were removed from the dataset. This represented 66 respondents or 1.6% of the dataset. Deletion of missing data when it comprises less than 5% of the sample is consistent with previous work with the PHQ-4. 72
The final sample used for the analyses included 3,925 working age adults. This excludes those respondents with missing data for the model variables (representing less than 2.2% of the sample).
Statistical analyses
Weighted Prevalence of Concordance and Discordance between Self-reported Mental and Physical Health.

Descriptive Statistics for Model Variables.
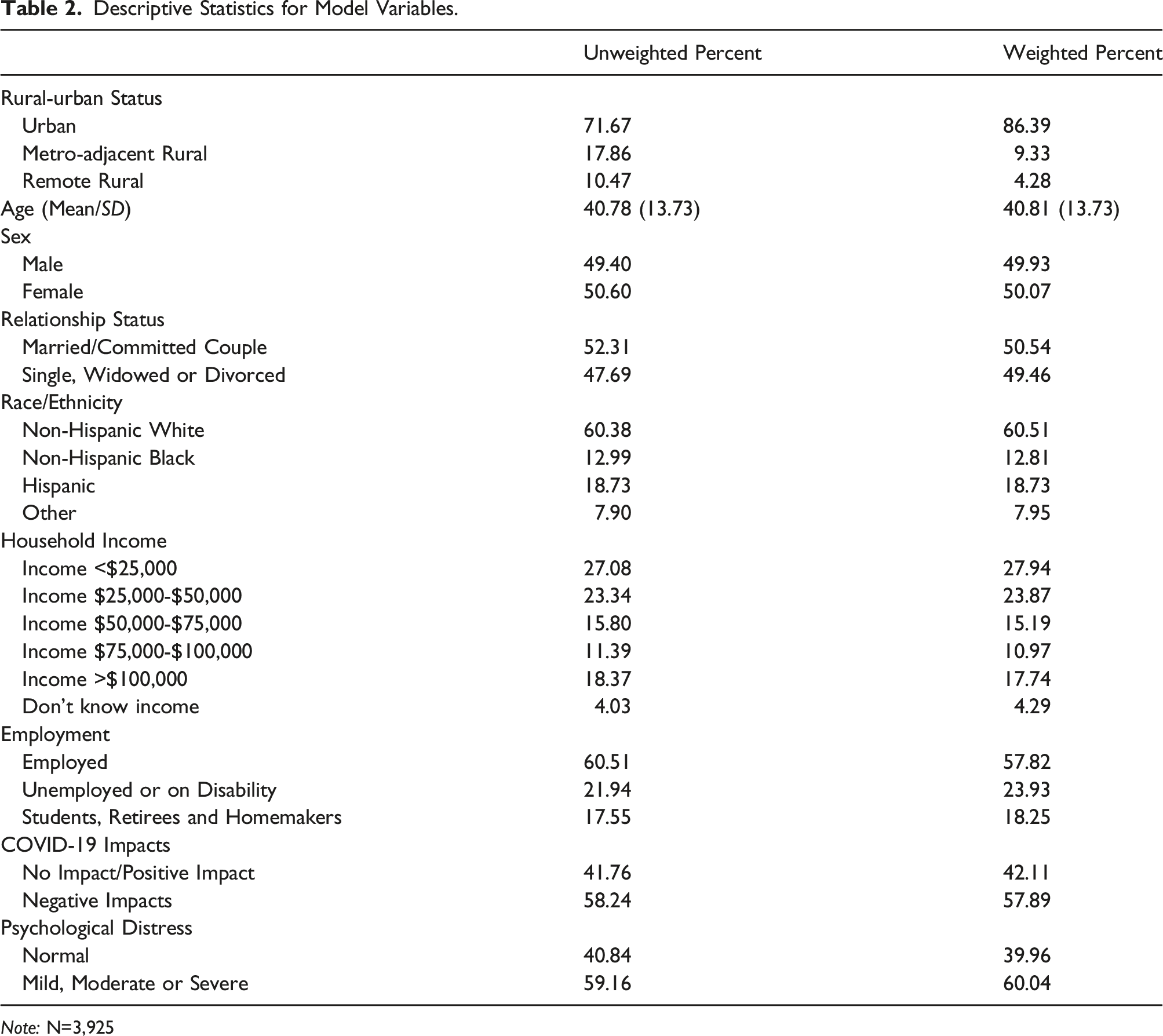
Note: N=3,925
Weighted Multinomial Regression Results Predicting SRPMM and Discordant Self-Reported Health.

Note: N=3,925; Models control for if respondents reported experiencing negative impacts from the COVID-19 pandemic.
Results
Descriptive statistics
Table 1 presents the weighted prevalence of the intersection of SRMH and SRPH among working age adults by urban, metro-adjacent rural, and remote rural status. Metro-adjacent rural working age adults were most likely to report SRPMM (24.19%), followed by remote rural (17.60%) and urban (14.30%) working age adults. In contrast, urban working age adults were most likely to report good or better mental and physical health (65.33%) followed by remote rural (53.74%) and metro-adjacent rural working age adults (48.85%). For both discordant measures, rates were highest for rural remote and metro-adjacent rural working age adults and lowest for urban working age adults.
Table 2 presents the unweighted and weighted descriptive statistics for the model variables. Over one quarter of the study sample (28.33%) lived in rural counties with the remaining residing in urban counties. The average age of those surveyed was approximately 40 years with a relatively even distribution by sex (49.40% male, 50.60% female). Just under half of respondents (47.69%) were single, widowed, or divorced, while the remainder (52.31%) were married or in a committed relationship. The majority of respondents (60.38%) identified as non-Hispanic White, followed by Hispanic (18.73%), non-Hispanic Black (12.99%), and then non-Hispanic other race (7.90%). Roughly half of respondents reported incomes <$50,000, while 15.80% reported incomes of $50,000-$75,000 and 11.39% reported incomes between $75,000 and $100,000. Slightly more than 18% reported incomes of over $100,000 and 4.03% reported not knowing their income. Over half of survey respondents (60.51%) were employed, with approximately a quarter (21.94%) unemployed or on disability, and 17.55% who were students, retirees, or homemakers. The weighted descriptive statistics are comparable except for rural-urban status. The original sample purposefully had disproportionately larger shares of working aged adults residing in rural counties than found in the general population. The post stratification weight attends to this discrepancy.
Regression models
Table 3 presents the unadjusted main effects models and the fully adjusted multinomial regression model results predicting SRPMM and both categories of discordant self-reported health. Compared to urban working age adults, those in metro-adjacent rural and remote rural counties were significantly more likely to report the SRPMM. However, when we adjusted for individual-level characteristics, only those in metro-adjacent rural counties were significantly more likely to report the SRPMM. Separate analyses (Appendix 3.0) show that the inclusion of the income measure in the model was responsible for the loss of significance for adults from remote rural counties and substantial attenuation of the odds ratio for adults from metro-adjacent rural counties. This suggests that the higher risk of working age adults in remote rural counties reporting SRPMM was, in fact, explained by lower incomes among this group (Appendix 4.0). In addition, age was negatively associated with the likelihood of SRPMM, even after controlling for other individual-level factors. Females and those who were single, divorced or widowed were significantly more likely to report SRPMM compared to males and those who were married or in a committed relationship, though the relationship for single, divorced or widowed disappeared when the model covariates were added. Among socioeconomic measures, those who reported higher incomes were significantly less likely to report SRPMM compared to those who reported incomes of <$25,000, with this remaining true even in the adjusted models (except for those making $25,000 < $50,000). Compared to those who were employed, those not working due to unemployment or disability, as well as students, retirees and homemakers were significantly more likely to report the SRPMM. This remained true in the fully adjusted model for those who were unemployed or on disability.
While not our primary focus, Table 3 also reports odds ratios for discordant SRMH and SRPH: fair/poor mental health and good or better physical health (-MH/+PH) and fair/poor physical health and good or better mental health (-PH/+MH). Those living in metro-adjacent rural and remote rural areas were significantly more likely to report -MH/+PH and -PH/+MH as compared to those in urban locations. This remained true for those in metro-adjacent rural areas even after controlling for other individual-level characteristics. Among demographic characteristics, age was associated with a higher odds of -PH/+MH, but a lower odds of -MH/+PH. Females were significantly more likely to report -MH/+PH and -PH/+MH compared to males. This remained true when controlling for all other model covariates, except for -PH/+MH. Those who were single, divorced or widowed were significantly more likely to report both -MH/+PH and -PH/+MH compared to those who are married or are part of a committed couple. This only remained true for -MH/+PH in the fully adjusted models. In terms of socioeconomic factors, only those who made greater than $100,000 per year were significantly less likely than those making <$25,000 per year to have lower odds of -MH/+PH. In contrast, the benefit was evident at other income levels for -PH/+MH. Finally, those who were unemployed, on disability, or were students, retirees, or homemakers were significantly more likely to report -MH/+PH and -PH/+MH, but this effect disappeared for -PH/+MH in the fully adjusted models.
Sensitivity analysis
Sensitivity analyses were conducted to evaluate findings for consistency when an alternative measure of SRMH, the PHQ-4 (Kroenke et al 2009), was used. Given that SRMH is a global indicator of mental health and the PHQ-4 screens for symptoms of depression and anxiety, perfect correlation between these measures was not expected. Appendix 1.0 shows that mild or higher psychological distress was significantly more common among those who reported poor/fair mental health (X 2 =610.30***). This finding suggests that the single-item SRMH is sensitive to different mental health states and supports its use to screen for mental health at the population level. Appendix 2.0 shows that the findings for SRPMM were comparable when psychological distress was used as a proxy for SRMH, except among those who identified as another race. The PHQ-4 was designed to screen only for anxiety and depression, 72 whereas SRMH encompasses a broader spectrum of mental health states.20,72 Therefore, the variation in findings with the sensitivity analysis may be attributed to differences in specificity or internal reliability of these measures.
Discussion
In this paper, we assessed the prevalence of SRPMM – those who report concurrent poor/fair mental and physical health – in a demographically representative working age adult sample and examined if rural-urban disparities exist. We found that among working age adults, the SRPMM was experienced by 15% of working age adults. Our estimates of SRPMM may exceed the estimated 5-17% of adults with co-occurring mental and somatic health conditions13,14 because SRMH and SRPH are more inclusive than the diagnosis-based measures used in prior studies. Individuals with SRPMM potentially face compounding mental and physical health needs that raise their risk of morbidity and mortality1,73 and subsequently higher health care costs and lost productivity.64,65,74 These findings support further research on SRPMM for monitoring change over time and evaluating effects of public health interventions and major historical events (e.g., COVID-19). In addition, 21% of working age adults had discordant self-reported health (i.e., reported poor/fair status for one of the two measures) (12.72% reporting +MH/-PH and 8.62% reporting -MH/+PH). Poor/fair health in one domain (mental or physical) increases the risk for developing co-occurring conditions in the other,8-11 therefore, these groups may be at elevated risk of developing SRPMM.
Previous work has documented rural-urban disparities in SRPH47,48 and mixed rural-urban disparities in SRMH.49,50 Our results build on those previous findings by showing that SRPMM is significantly more common among rural working-age adults and that there is variation within rural areas. When broken down by residence, approximately 14% of those in urban counties, 24% of those in metro-adjacent rural counties, and 18% of those in remote rural counties reported SRPMM. This aligns with previous literature showing worse self-rated health in metro-adjacent rural counties than in remote rural counties – something that has been attributed to metro-adjacent rural counties are disproportionately located in the South. 48 These findings raise several concerns. Rural areas face unique barriers along multiple structural and social determinants of health that may limit the ability of individuals and communities to address SRPMM. Rural areas are – on average – home to higher rates of precarious employment, longer travel distance to healthful food, and more limited health care infrastructure, particularly related to mental health.75-79 Therefore, a number of structural factors are likely at play that may contribute to or limit improvement in the SRPMM within rural communities. We also found that the elevated prevalence for adults from remote rural counties was driven by lower incomes. Efforts to increase livable wages may be important for reducing the risk of SRPMM in rural areas. Further research is needed to better understand how income shapes SRPMM across the rural-urban continuum.
In addition, we found noteworthy socio-demographic disparities in SRPMM. Risk is higher among females, younger working age adults and those who are single, unemployed, or have low incomes. These findings build on prior work that separately document sex, age, and relationship status disparities in SRMH53,55,58,60 and SRPH,20,48,56,59 as well as higher rates of poor/fair SRMH and SRPH (separately) for low income and unemployed adults.48,55-57 This is particularly concerning given the income disparities that persist in rural communities. 80 While we found that non-Hispanic Blacks were significantly less likely to report SRPMM compared to non-Hispanic Whites in the fully adjusted model, we caution this interpretation given previous work documenting racial and ethnic differences in question interpretation and reporting rates of self-rated health across ethnoracial groups.1,20,58,61-63 Additional investigation is needed to understand how SRMH and SRPH items capture the experiences and meanings of different racial and ethnic groups. With already limited or compromised social protections and inequitable access to health services, these groups may experience a disparate share of adverse health outcomes that may not be captured by the SRPMM measure.
Limitations
The findings from this study should be interpreted in light of several limitations. First, the data used for this research are cross-sectional, therefore, causality cannot be asserted. Moreover, measures of self-rated health do not provide information about the mechanisms that contribute to poor/fair health or health inequities.71,81 Therefore, we limited our discussion to the socio-demographic and spatial correlates of SRPMM and discordant SRMH and SRPH. Second, SRMH and SRPH are imperfect measures with internal validity concerns as previously discussed. However, these measures have established validity and reliability for monitoring general trends across populations and subpopulations.82-84 Third, while we were able to use the PHQ4 to corroborate the SRMH measure, we did not have a comparable variable for the SRPH measure. The findings presented here support SRPMM as a population-level tool to assess and monitor health, not as a means to inform or create local interventions strategies.
Conclusion
In this paper, we have shown – using a demographically nationally representative sample of working age adults – that SRPMM is more common among working age adults residing in rural counties than in urban counties. Lower incomes accounted for all of the elevated risk among those from remote rural counties and part of the risk for adults from metro-adjacent rural counties. These findings suggest that nationally representative surveys could include both SRPH and SRMH to help facilitate research needed to inform the use of SRPMM as a measure and its disproportionate prevalence among rural residents and other sub-populations. Research is also needed to understand the compounding effect of SRPMM on long term morbidity and mortality – above and beyond the single measures of SRMH and SRPH. This work serves as the foundation for the use of SRPMM as a concept, a measure, and a population health priority for rural and urban America.
Supplemental Material
Supplemental Material - Rural-Urban disparities in self-reported physical/mental multimorbidity: A cross-sectional study of self-reported mental health and physical health among working age adults in the U.S.
Supplemental Material for Rural-Urban disparities in self-reported physical/mental multimorbidity: A cross-sectional study of self-reported mental health and physical health among working age adults in the U.S. by Danielle Rhubart, Jennifer Kowalkowski and Jordan Yerger in Journal of Multimorbidity and Comorbidity
Footnotes
Acknowledgements
The authors would like to thank Dr. Xiaoyan Zhang for her input on early plans for this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Rhubart acknowledges infrastructural support from the NICHD-funded Population Research Institute at The Pennsylvania State University (P2CHD041025).
Informed consent
This manuscript used data from the National Well-being Survey (2021). A version of this data is publicily available and can be accessed here: https://doi.org/10.3886/ICPSR38879.v2.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.