
Abstract
Summary
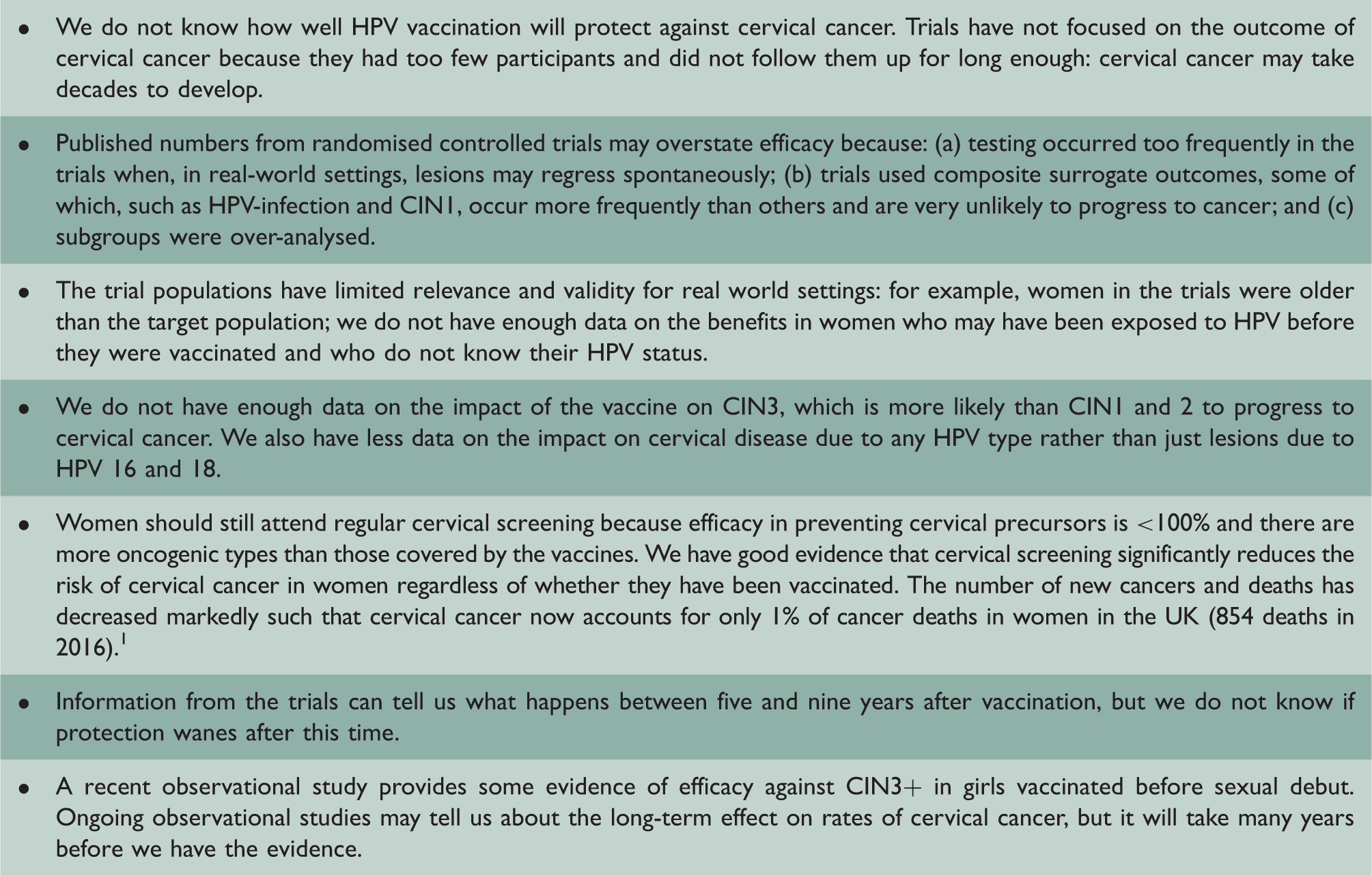
We conducted a critical appraisal of published Phase 2 and 3 efficacy trials in relation to the prevention of cervical cancer in women. Our analysis shows the trials themselves generated significant uncertainties undermining claims of efficacy in these data. There were 12 randomised control trials (RCTs) of Cervarix and Gardasil. The trial populations did not reflect vaccination target groups due to differences in age and restrictive trial inclusion criteria. The use of composite and distant surrogate outcomes makes it impossible to determine effects on clinically significant outcomes. It is still uncertain whether human papillomavirus (HPV) vaccination prevents cervical cancer as trials were not designed to detect this outcome, which takes decades to develop. Although there is evidence that vaccination prevents cervical intraepithelial neoplasia grade 1 (CIN1) this is not a clinically important outcome (no treatment is given). Trials used composite surrogate outcomes which included CIN1. High efficacy against CIN1+ (CIN1, 2, 3 and adenocarcinoma in situ (AIS)) does not necessarily mean high efficacy against CIN3+ (CIN3 and AIS), which occurs much less frequently. There are too few data to clearly conclude that HPV vaccine prevents CIN3+. CIN in general is likely to have been overdiagnosed in the trials because cervical cytology was conducted at intervals of 6–12 months rather than at the normal screening interval of 36 months. This means that the trials may have overestimated the efficacy of the vaccine as some of the lesions would have regressed spontaneously. Many trials diagnosed persistent infection on the basis of frequent testing at short intervals, i.e. less than six months. There is uncertainty as to whether detected infections would clear or persist and lead to cervical changes.
Licensing and guidelines.
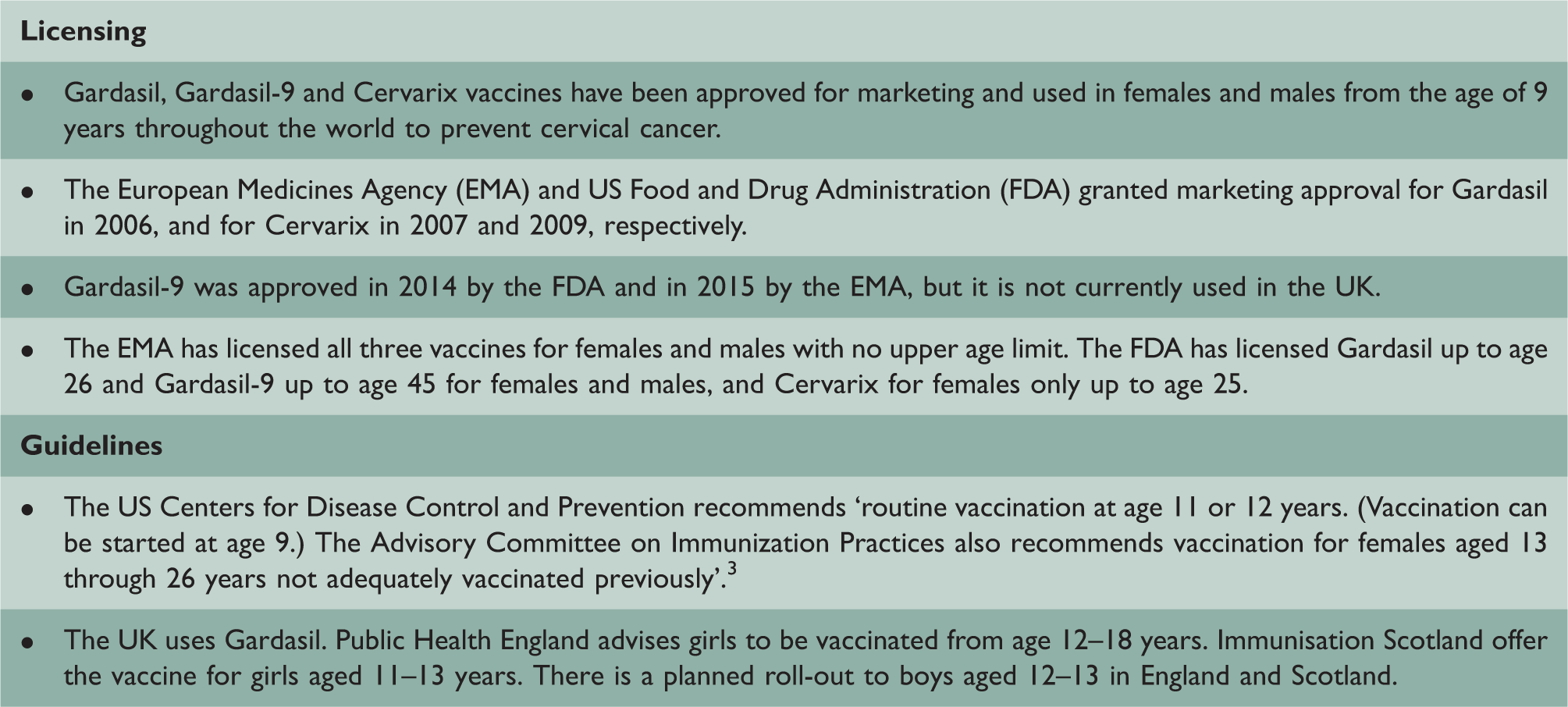
Public health agencies promote the position that the vaccine has been shown to prevent cervical cancer (see Supplement 1). Not all routinely emphasise the limitations of the evidence or the uncertainties which we will discuss.
Background
A key issue for the design of trials and studies of efficacy is the complexity of the epidemiology of the HPV subtypes and the lesions used as surrogate endpoints for cervical cancer, each with their own different natural histories, prevalence and incidence and strength of association with cancer. These measures, especially if combined as composite surrogate endpoints in trials, generate new uncertainties.
i) HPV infection
There are 100+ types of the HPV: 12 of which are carcinogenic to humans, according to the International Association of Cancer Research (IARC). 4 Types vary in prevalence, as does their association with cervical cancer. HPV vaccines are licensed for use against oncogenic HPV types 16 and 18 and now 31, 33, 45, 52, 58 in Gardasil-9. Gardasil and Gardasil-9 are also licensed against non-oncogenic types 6 and 11 linked to genital warts.
The lifetime risk of an incident of HPV infection is 79%;
5
the majority of HPV infections are transient and 67% clear within one year.
6
Around 10% of women without CIN have HPV infection at any one time.
7
The mechanism of progression from HPV infection to cervical cancer and its precursors is not well understood.4,8–11
ii) Cervical cancer and pre-cancerous lesions as surrogate endpoints
Estimated rates of regression and progression for CIN1, 2 and 3 are presented in Figure 1.
12
However, there remain uncertainties due to methodological issues in the epidemiological studies from which these findings originate.
12
CIN natural history.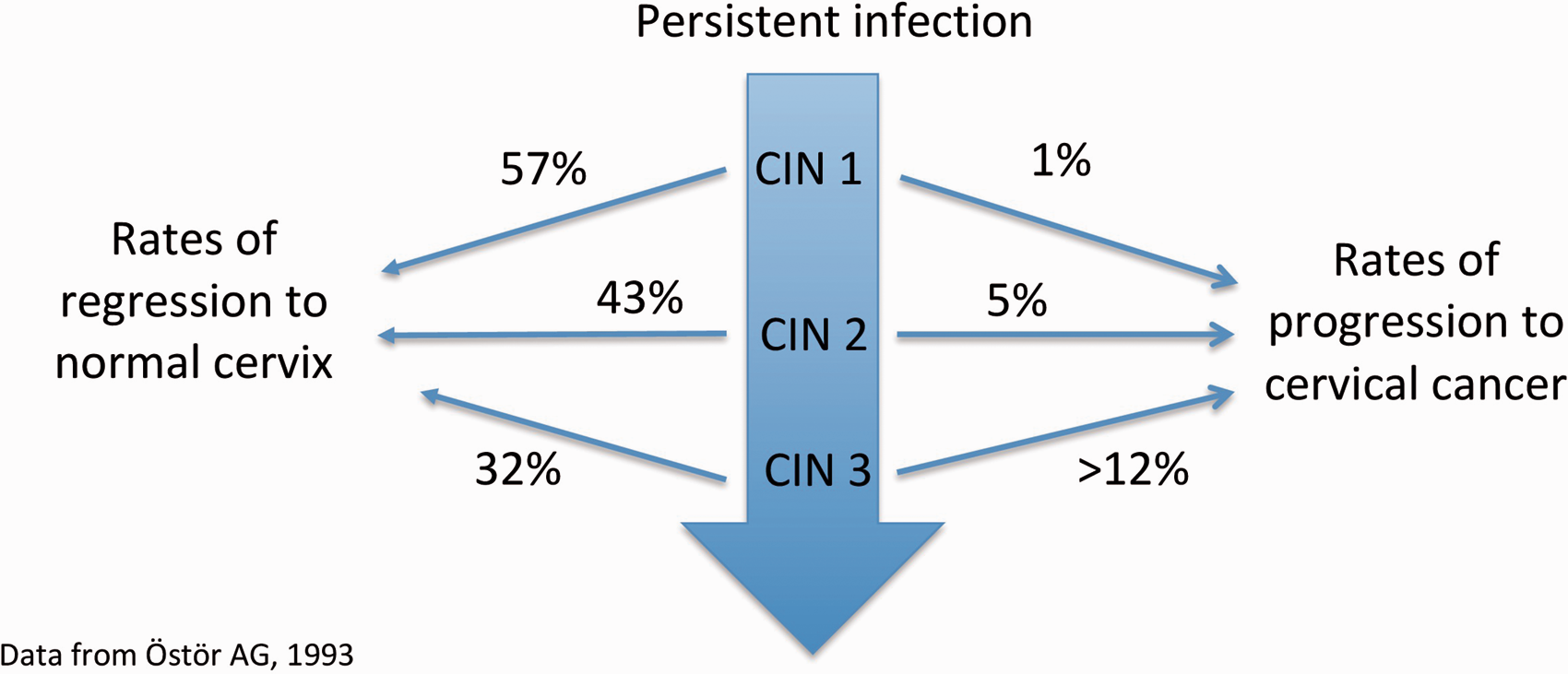
The IARC has acknowledged that composite endpoints in intervention studies involving CIN2 are sub-optimal 13 as CIN2 is often misclassified due to its diagnosis having lower reproducibility and validity. 14 Women with CIN2 are currently offered treatment which complicates research into progression to CIN3.
CIN3 can develop via progression of CIN1 and CIN2 or directly as a result of HPV infection, so CIN1 and CIN2 may not be good predictors of progression. Rate of progression from CIN3 to invasive cancer is likely to be higher than Ostor’s estimate of >12%. 12 Lifetime risk may be up to 40% without cervical screening and treatment. 15
Aim
To describe the uncertainties generated by the design of Phase 2 and 3 efficacy trials for prevention of cervical cancer and its precursors and how they affect the interpretation of efficacy data.
Methods and analysis
We searched Embase and Medline for papers relating to blinded controlled trials of HPV vaccination in females considering efficacy against cervical cancer and its precursors. See Supplement 2 for search strategy. No trial has tested Gardasil and Cervarix vaccines head to head using clinical outcomes (rather than immunological outcomes). We reviewed 35 published papers relating to 12 published randomised blinded non-HPV vaccine-controlled Phase 2 and 3 trials of Gardasil and Cervarix conducted from 2001 to 2016 assessing efficacy against cervical cancer and its precursors (Table 1 and Figure 2). Throughout this article, we refer to trials by their protocol name as presented in bold in Table 1. But for trials 104798 and 107638, we use the name of their first authors, Konno and Zhu, respectively.
Phase 2 and 3 randomised controlled trials on HPV vaccination efficacy. All Phase 2 and 3 trials by vaccine and control, sponsor, country, start and end dates, number and age of participants and length of follow-up.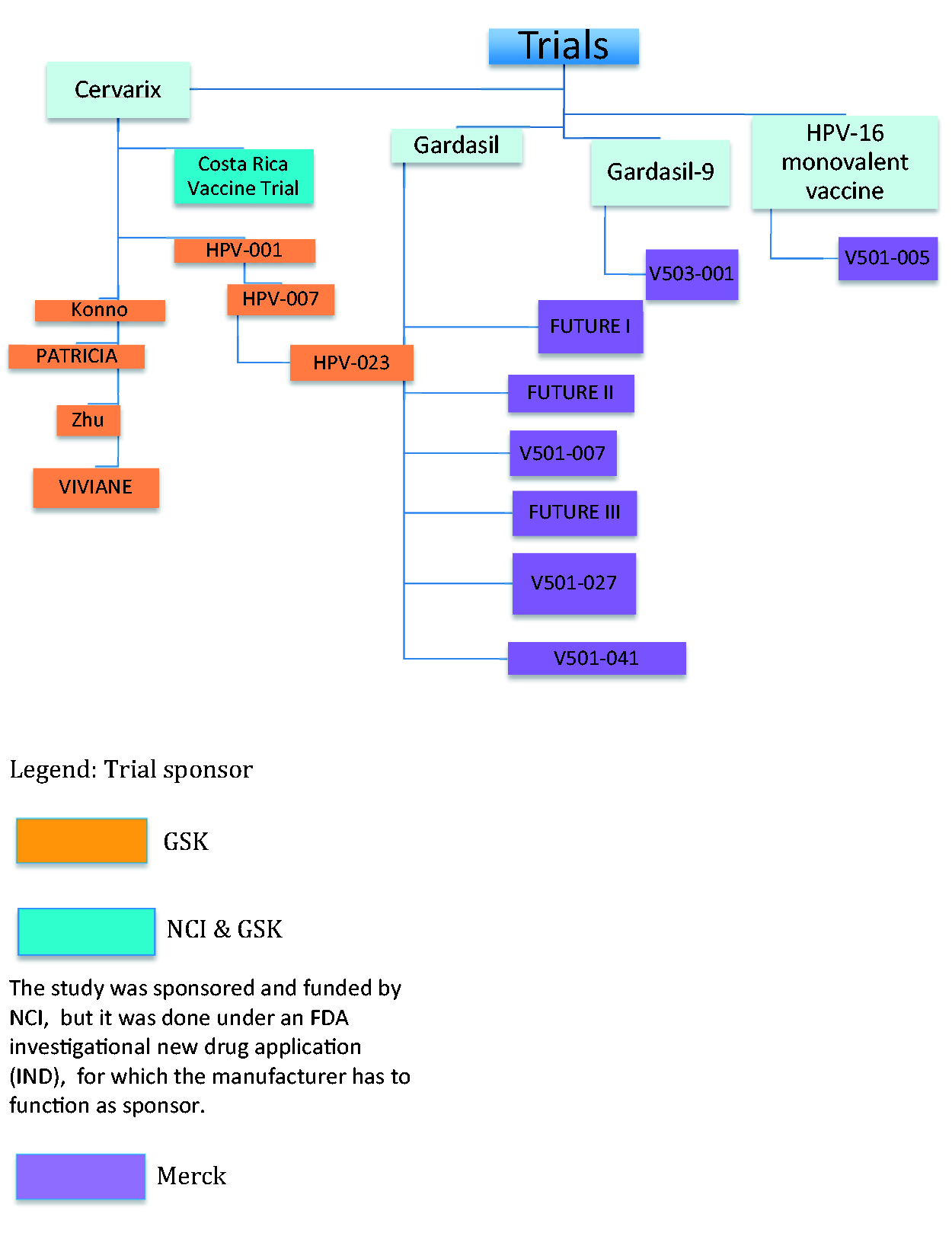

We excluded trials of the HPV 16 monovalent vaccine (as it was not licensed and data suggest it had different pharmacodynamics to Gardasil and Cervarix 16 ) and the one efficacy trial of Gardasil-9 (as the control was Gardasil, not a placebo). 17 All the efficacy studies used an active vaccine (Hepatitis A) as the control, or a control containing an aluminium-adjuvant, rather than a true placebo; this in itself has raised concerns. 11 We chose to focus on randomised controlled trials as this offers the highest level of evidence and this is the evidence used for decisions by regulatory bodies and decisions on initiating vaccination programmes.
We also found 39 meta-analyses and systematic reviews of HPV vaccine efficacy; of them many are restricted to post-hoc analyses of subgroups and have inappropriately combined trials in the same analysis, e.g. for different vaccines (see Supplement 3). The 2018 Cochrane review 18 has been criticised for failing to include all relevant trials, ignoring evidence of harms and using composite endpoints with different natural histories. 19
We compared the eligibility criteria, testing methods for HPV and cervical lesions, outcomes measures, length of follow-up, target group and subgroup definitions used in the different trials. We focused on the evidence for efficacy for CIN3+ and 12-month persistent infection which are deemed the more stringent outcome measures.
Does HPV vaccine prevent cervical cancer?
None of the trials were designed to determine efficacy or effectiveness against cervical cancer. There were no reported cases of cervical cancer in any trials; one case of vulval carcinoma was reported in the vaccinated group of FUTURE I. 48
The time between first exposure to HPV and peak development of CIN3 is 7–10 years. 13 It takes a further 10 years or so for cervical cancer to develop according to natural history studies. 13 All trials had a mean length of follow-up of six or fewer years, apart from the HPV-023 extension with a mean follow-up of 8.9 years.
Does HPV vaccine prevent pre-cancerous lesions?
Powered endpoints across trials.
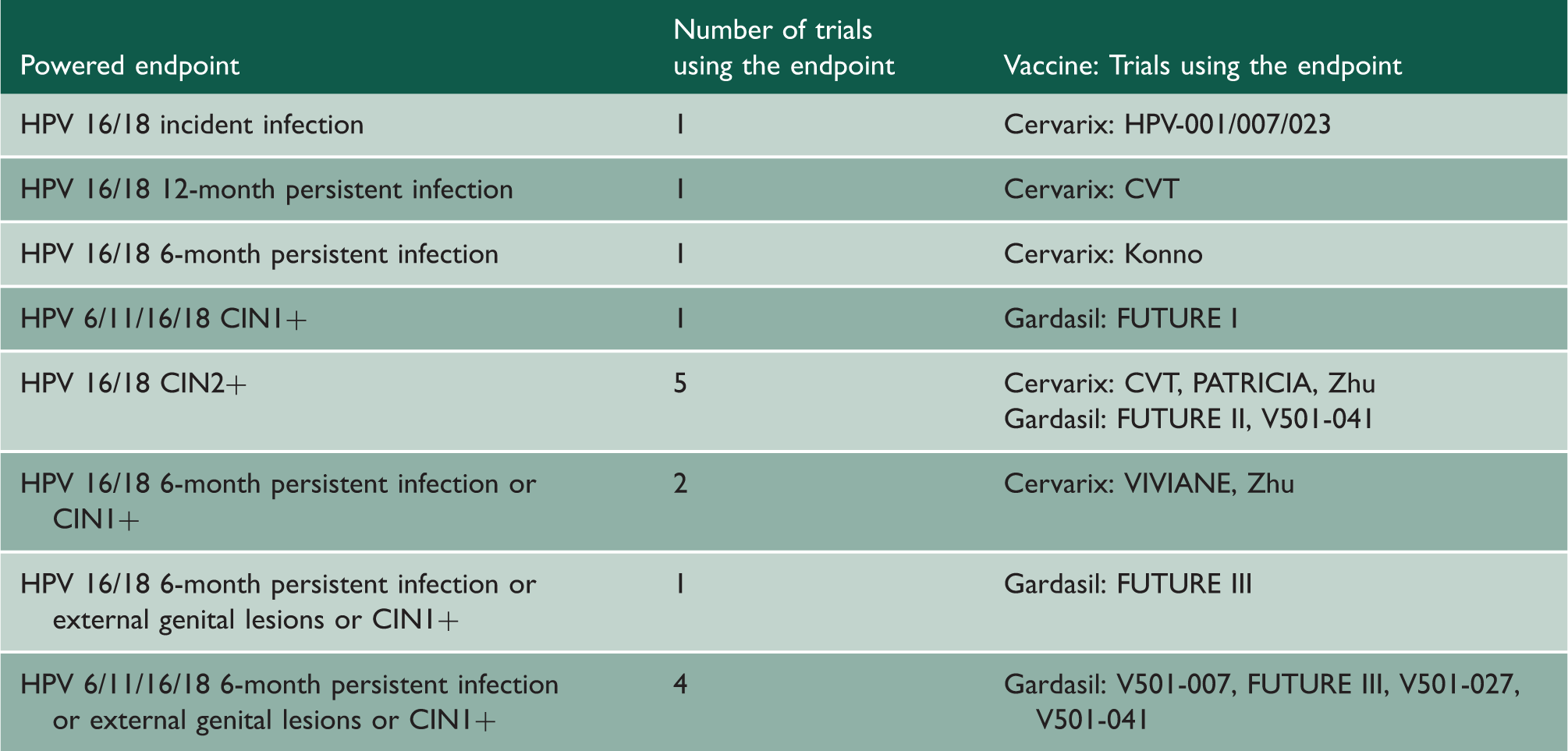
CIN1+
The trial outcomes included surrogates CIN1 and CIN2, which are more common than CIN3/AIS and cervical cancer, but which often regress and are of limited clinical concern (see ‘Background’ section and Figure 1). For example, intervention is not recommended for CIN1. Seven trials (FUTURE I, VIVIANE, V01-007, FUTURE III, V501-027, Zhu, V501-041) included CIN1 with CIN2, CIN3 and AIS in the same primary outcome (making a composite outcome), potentially inflating vaccine efficacy as there are many more CIN1 cases than CIN2+.43,45,47,48,51–53
CIN2+
The incidence (rate of detection) of CIN2, CIN3 and AIS in the trials was low so although many trials showed high efficacy for the vaccine, this was in the context of very few cases of CIN2+. For example, the HPV-023 trial showed high vaccine efficacy (100% against CIN2 and CIN3 over nine years follow-up) with very low incidence (only three cases, all in the control group, out of 212 participants). 25 The trials were powered for the minimum number of events needed to obtain a statistically significant result, and many trials were designed to stop once this number had been achieved. But the powered outcomes often included CIN1, which means those trials were not powered to reach a minimum number of higher-grade CIN cases. Instead of multiple short duration trials, this problem of power could have been overcome by having one large trial of longer duration in each country.
CIN3+
CIN3 is generally agreed to be the best marker for risk of cervical cancer, with rates of progression of at least 12%. 12 New evidence suggests that clinical intervention following detection on screening may be best reserved for women with CIN3. 55 Only three of the 12 trials (FUTURE I, FUTURE II, PATRICIA) reported CIN3+ or AIS in subgroups that represented the target population of women naïve to HPV (see Supplement 4).30,49,56 The incidence of AIS in the trials is very low and only three trials (FUTURE I, FUTURE II, PATRICIA) published results for AIS alone.30,49,56
In these three trials, vaccine efficacy against CIN3 and AIS due to HPV 16/18 was 100% (see Supplement 4) but there were small numbers and wide confidence intervals, sometimes showing non-significance (where the confidence interval crosses zero).49,56 Vaccine efficacy against CIN3 and AIS due to any HPV type varied substantially between the vaccines.30,56
What is the evidence that vaccination prevents clinically meaningful HPV infection?
It is possible to diagnose new HPV infections (incident) and ongoing infection (persistent). Studies have shown median length of HPV 16 infection to be 8.5–19.4 months and HPV 18, 7.8–12 months. 13
The HPV001/007/023 trial used incident infection of HPV 16/18 as the primary outcome.20,22,25 The results are not relevant to policy decision making as the current consensus reported by the WHO is that incident HPV infection is not an adequate surrogate outcome because it rarely progresses to cervical disease. 57
There is a lack of agreement on what time period defines persistent infection, 13 and the trials may have overestimated vaccine efficacy by picking time periods that are shorter than the duration of most self-limiting infections, for example six months. In some trials, the testing interval for diagnosing six-month persistent infection was four months36,47,52 or five months.44,51,53
Only one Gardasil trial, V501-041, used 12-month persistent infection as an outcome; however, the study authors only presented data for combined HPV 6/11/16/18, not for 16/18 or any oncogenic type. 53 In the Cervarix trials, 12-month HPV 16/18 persistent infection vaccine efficacy varied from 85.3 to 100% (see Supplement 5).25,27,29,33,45 Vaccine efficacy for 12-month persistent infection by any oncogenic HPV type ranged from 10.4% to 50.1% across trials with wide confidence intervals for most trials.25,27,29,33,45 The results were not statistically significant for the HPV-023 trial and Zhu (see Supplement 5).25,45
Not all trials analysed HPV types 16 and 18 separately. The incidence of HPV infection varies by HPV type. 30 HPV 18 was much less common than HPV 16. Combining their results makes the efficacy against HPV 18 appear more solid. In some trials the results for HPV 18 on its own were not statistically significant and were only significant when combined with results for HPV 16. For example, in the per-protocol population subgroup of V501-027, the six-month persistent infection or genital disease (the trial primary outcome) vaccine efficacy was 100% (59.7,100) for HPV 16, 86.0% (−8.9, 99.7) for HPV 18 and 94.5% (65.2, 99.9) for HPV 16/18. 52 In the according-to-protocol cohort for efficacy (ATP-E) subgroup of the PATRICIA trial, CIN3+ vaccine efficacy for HPV 16 was 90.2% (59.7, 98.9), HPV 18: 100% (−8.2, 100) and HPV 16/18: 91.7% (66.6, 99.1), respectively. 30 This means the vaccine may not protect as well against cervical cancer related to HPV 18. The proportion of cervical cancers related to HPV 18 ranges from 13% in South/Central America to 22% in North America. 58
How much information is there on long-term outcomes and how long does protection last?
All trials were six or fewer years in length, apart from the extension study HPV-023 with mean follow-up of 8.9 years, (which maintained blinding and kept a control group) it only included 437 of the original 1113 participants in HPV-001. 25 The longest study of Gardasil was V501-041, which was extended from 30 to 78 months with 2601 out of the initial 3006 participants. 53
Features of the trials may bias the findings in overestimating long-term efficacy. For example, HPV 16/18 related CIN3 presents earlier than non-vaccine type CIN3 so shorter efficacy trials will be biased in favour of finding HPV 16/18 related CIN3. 59
Although incidence and progression of disease differ over time and by age, V501-007 combined the results of participants from the original trial with those who completed an extra two-year extension. 47 In HPV-007 and HPV-023, results for participants from the preceding trials were considered together.22,25
How similar were the females in the trials to the target vaccination groups?
Females in the trials are typically older than those in real-life vaccine programmes, and it is unclear whether their outcomes are similar. We do not know efficacy rates in girls aged between 9 and 13 years.
The youngest trial participants were aged 15 years and trials did not restrict recruitment to girls before sexual debut. Therefore, previous exposure to HPV is likely for some girls. Per-protocol subgroups with much fewer participants were used to analyse those with no evidence of previous HPV exposure but as shown earlier, most trials did not present data for CIN3+ outcomes in these subgroups.
Efficacy in girls aged 9–13 years has been estimated using immunobridging trials (where immune response levels are measured) rather than using clinical outcomes. 60 We do not know what level of antibody titres define a surrogate level of protection against cervical cancer or its precursors and how long protection will last (Gardasil anti-HPV 18 titres are not different from natural infection as early as 24 months after vaccination). 60 Therefore, it is possible that protection will wane by time of peak exposure when vaccinated at an earlier age.
Three trials recruited older women (FUTURE III (aged 24–45), VIVIANE (aged 26+) and V501-041 (aged 20–45)).42,50,53 In VIVIANE a subset of up to 15% of women with a history of HPV-associated infection or disease were included (defined as two or more abnormal smears in sequence, abnormal colposcopy, or biopsy or treatment of the cervix after abnormal smear or colposcopy findings) but this means that the Total Vaccine Cohort may not reflect the proportion of women with a history of HPV-associated disease in the wider population. 42 There were then restrictions based on HPV DNA and serostatus for inclusion in the according to protocol for efficacy and total vaccine cohort for efficacy subgroups. In FUTURE III, women with a history of past or present genital warts or cervical disease were excluded; the primary tests of efficacy were in the HPV type-specific per-protocol efficacy analyses (PPE), which required women to be seronegative to relevant type on day 1 and PCR negative to that type in cervicovaginal swabs or biopsy samples, or both, from day 1 until month 7. 50 V501-041 excluded women with more than four previous sexual partners and those with a history of genital warts or ‘significant cervical disease’ – the study authors did not specify what this meant. 53
Seven trials excluded women with more than four to six previous sexual partners.20,28,46,48,52,53,61 Five excluded women with previous abnormal cervical smears20,46,48,52,61 and an additional three excluded women with a history of previous colposcopy.26,28,44 CVT was the only trial with no restrictions based on genital warts or cervical or sexual history. 36 These restrictions may make the vaccine appear more efficacious in the intention-to-treat (ITT) population than in the general population of women of the same age. In CVT, the efficacy in the ITT group for 12-month persistent infection with any oncogenic HPV type was 11% (95% CI 2.2, 19.5); they did not give efficacy against CIN3+ in the ITT group. 36
There is also global variation in the epidemiology of HPV which means that the trial findings may be poorly generalisable to some settings, including Africa, so it is important to know if results differ by study region. None of the trials considering efficacy outcomes were conducted in Africa (we are only aware of a safety and immunogenicity trial in Africa 62 ) despite this being the world region with by far the highest incidence of cervical cancer. 2 The Cochrane review acknowledges that ‘differences in the population HPV prevalence in the trial sites, or differences in study protocols and assays used, may explain the contrast in efficacy’ between Cervarix and Gardasil. 18
What is the risk of oncogenic HPV-type substitution?
Vaccines may protect against HPV types, which are not included in the vaccine. There was some evidence of cross-protection against three high-risk HPV types (31, 33 and 45) for Cervarix (see Supplement 6).31,36,43,45 There was cross-protection against one non-vaccine HPV type by Gardasil 31 (see Supplement 6). 63 But there was evidence of a statistically significant increased risk of HPV type 51 and 58 in the Cervarix trials, compared with the control vaccine.31,36 It is unknown whether vaccine targeting will lead to substitution by other oncogenic types, as with pneumococcal vaccination. 64
Methodological factors from the trials which may affect interpretation of the results
Multiple underpowered analyses
All trials undertook multiple subgroup analyses, which increase the likelihood of positive statistical findings in the absence of true effect. The subgroup definitions varied across trials, so that results cannot be compared across trials. Results were not given for all subgroups, and were not broken down by country, by study site or for each outcome. This is important given different epidemiology of HPV in different areas of the world. It may have been reported this way because incidence was low. We have included a table giving the different subgroup definitions in Supplement 7.
Problems with reporting of trial results
The trials report vaccine efficacy as the primary outcome, which shows relative risk reduction. This can over-emphasise efficacy compared with absolute risk reduction such as numbers needed to vaccinate, which is more useful for clinicians, patients and policy makers. None of the trials gave numbers needed to vaccinate. CVT is the only trial that presented results in terms of absolute risk reduction.36,38,39 The absolute risk reduction for the PATRICIA trial for CIN3+ due to any oncogenic HPV type (see Supplement 4) (our calculation) is 0.75%, giving a number needed to vaccinate of 133.
Frequency of cervical screening
All the trials did Pap cytology at 6–12 monthly intervals. Cervical cancer screening is recommended in England every three years, between the age of 25 and 49 years. 65 Increased frequency of screening can lead to over-diagnosis and overtreatment of cytological abnormalities that would normally resolve and not be detected. 66 Increasing the frequency of testing suits early trial completion but may overestimate vaccine efficacy.
Testing methods for HPV
The tests for DNA positivity to a particular HPV type (indicating ongoing infection) and seropositivity (indicating previous infection) have limited specificity and sensitivity. 67 This is another reason HPV infection has limitations as a surrogate of cervical cancer. Only 50–70% of HPV infections result in detectable anti-HPV responses, 51 and initial seropositive status may revert to negative. 68 So subgroups of women considered naïve to HPV may have had previous exposure. Also, latent infection may be undetectable on current tests. The IARC has noted that ‘it is not known how frequently this [latent infection] occurs in immunocompetent individuals, how long it lasts, what causes re-emergence into a detectable state or what fraction of cancers arises after a period of latency’. 13 This also raises the question of whether subgroups naïve to HPV can reliably represent girls before sexual debut, and whether HPV infection is a valid surrogate outcome.
Meta-analysis of limited value due to trial heterogeneity
Differences in trial endpoints and subgroups limit the ability to compare and aggregate data from trials. This is compounded by lack of standardisation across studies for a range of measures: tests of previous HPV exposure, serological assays to detect HPV infection and sampling methods including frequency of testing. 67
There are no agreed criteria for defining the causal HPV type for clinical lesions, and different trials used different criteria (see Supplement 8). There was no standard approach to assess efficacy against disease and infection due to HPV types not found in the vaccine, for example whether they considered non-vaccine oncogenic types or all non-vaccine HPV types (see Supplement 9). Given that Merck and GSK were involved in all the trials it is unclear why there was no consistency in methods and tests across trials.
Is ongoing research likely to resolve the uncertainties?
The focus of this paper is randomised controlled trials, but we have also looked at whether observational studies can answer some of the uncertainties, acknowledging that this is a lower level of evidence but practically the most likely source of future information in the absence of long-term randomised controlled trials. We identified 19 Phase 4, observational and non-blinded follow-up studies (including a meta-analysis of ecological studies) that are potentially relevant to the uncertainties discussed in this paper (see Supplement 10). None of these studies is ideal. Many are small, of short duration or not looking at CIN3+. One observational study (#5) showed a reduction in relative risk of CIN3 amongst those vaccinated of 0.45. 69 The PATRICIA trial follow-up (#3), the only trial planned for 20 years post-vaccination, and the Mexican FASTER trial (#18) are likely to provide more long-term efficacy data on the more clinically relevant efficacy endpoints.
The recently published observational study conducted in Scotland by Palmer et al. 70 provides new evidence on reduction of CIN3+ regardless of HPV type. The authors note the following limitations which may have inflated measures of efficacy: the study gathered data only on the first round of cervical screening at age 20 years (now changed to age 25 years in line with England) with underrepresentation of the unvaccinated group (23% screening attendance versus 51% in the vaccinated group at aged 20 or 21); and shorter follow-up time for women born in 1995 and 1996 necessarily affects the robustness of the estimate of vaccine effectiveness for younger women. In addition, the basis for the claim of herd protection is not well explained for the unvaccinated women in the 1995–1996 cohort, compared with unvaccinated women in 1988–1990. Nor do the authors consider how changes in sexual activity may have contributed to the observed decrease in CIN prevalence independent of the vaccine: between 2002 and 2014 (the latest period for which there are data) the proportion of 15-year-olds in Scotland who have ever had sex reduced, although socio-economic inequalities persist for sexual initiation and condom use. 71 Screening uptake also varies by socio-economic status. 72
What should we do in the light of the uncertainty?
Policy
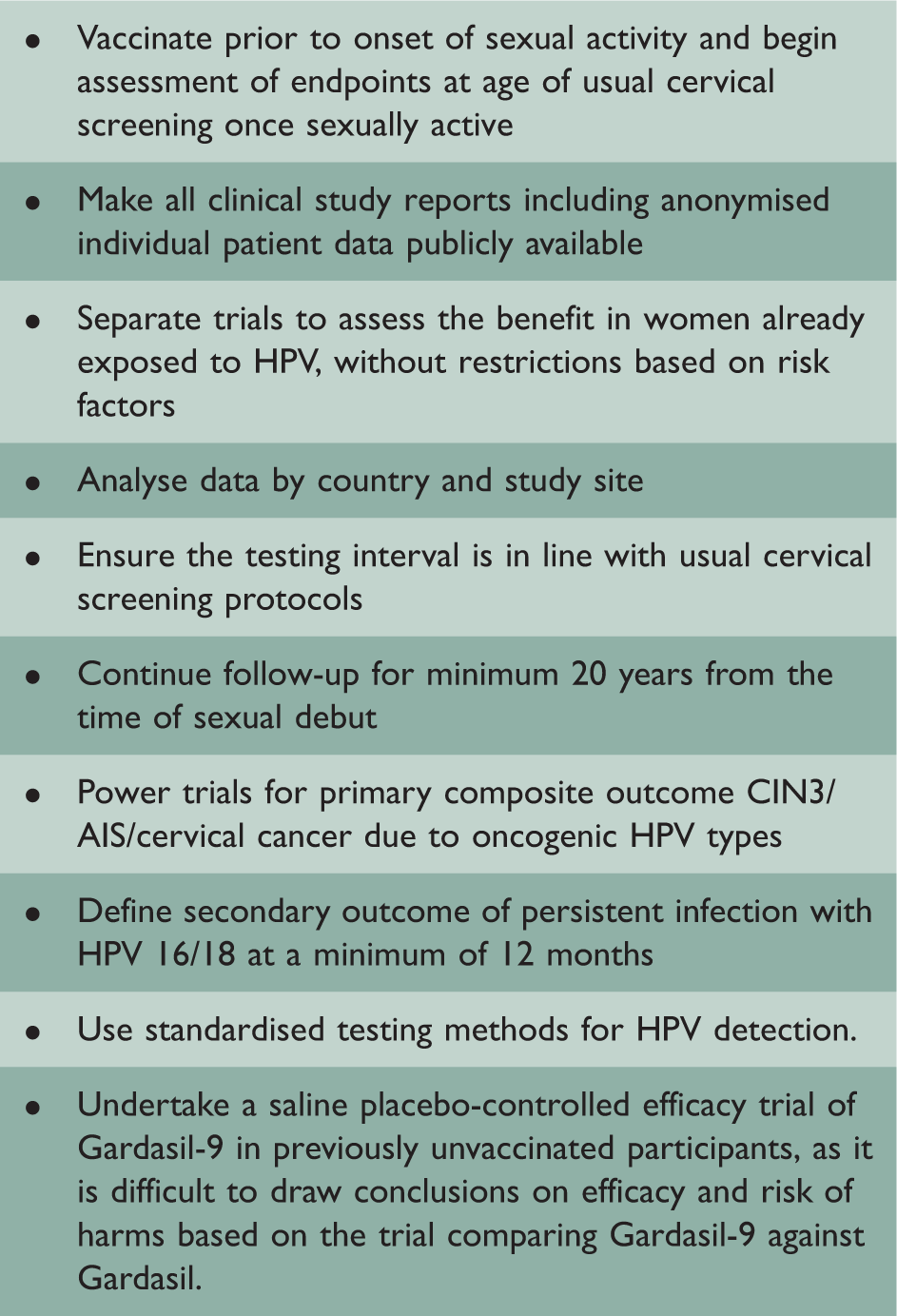
We ask policy makers to:
Establish national baseline epidemiological data on cancer incidence, mortality and HPV subtype prevalence to support evidence based decisions about whether the currently available vaccines are likely to be cost-effective and should be a priority. Ensure that cancer surveillance and registries are in place before any vaccination programme is implemented so that changes in incidence of cervical cancer and its precursors can be studied. Initiate national long-term efficacy and effectiveness studies that are free of industry funding, focus on clinically meaningful outcomes, and enrol and analyse the vaccine target populations.
Research
Recommendation for future trials to address the uncertainties.
Conclusion
This review has revealed many methodological problems with the Phase 2 and 3 efficacy trials of HPV vaccination leading to uncertainty regarding understanding its efficacy.
Cervical cancer – It is uncertain whether HPV vaccination prevents cervical cancer. The trials were not designed to detect this outcome, which takes decades to develop. For most outcomes, follow-up data exist for an average of only four or five years. CIN – There is evidence that vaccination prevents CIN1; however, this is not a clinically important outcome (no treatment is given). Trials used composite surrogate outcomes which included CIN1, but high efficacy against CIN1+ (CIN1, 2, 3 and AIS) does not necessarily mean high efficacy against CIN3+ (CIN3 and AIS), which occurred much less frequently. There are too few data to clearly conclude that HPV vaccine prevents CIN3+. CIN in general is likely to have been overdiagnosed in the trials because most carried out cervical cytology at intervals of 6–12 months rather than at the normal screening interval of 36 months. This means that the trials may have overestimated the efficacy of the vaccine as some of the lesions would have regressed spontaneously. Persistent HPV infection – The outcomes for HPV infection are difficult to interpret. Many trials diagnosed persistent infection on the basis of frequent testing at short intervals, i.e. less than six months. This leaves uncertainty as to whether detected infections would clear or persist and lead to cervical changes. In the current Public Health England cervical screening programme, patients who are HPV positive but cytology negative are not retested for 12 months.
74
Differences between trial and real world populations – Most of the people in the trials were older than the 9- to 13-year-olds who are typically offered vaccination. Efficacy in girls aged 9–13 years has been estimated using immunobridging trials (where immune response levels are measured) rather than using clinical efficacy outcomes.
60
We do not know what level of antibody titres protect against cervical cancer and its precursors, or how long protection will last.
60
Similarly data on the outcomes for women older than 24 years are limited, and all trials apart from the Costa Rica Vaccine Trial (CVT) had exclusions on eligibility related to sexual history or history of genital warts or cervical disease, limiting the generalisability to catch-up vaccination populations.
36
HPV epidemiology varies globally. No efficacy studies were done in Africa. Cross-protection and HPV-type substitution – There is uncertainty about whether the vaccine will provide cross-protection against oncogenic HPV types not targeted by the vaccines. There is also a risk of substitution where a non-vaccine oncogenic HPV type fills the void left by the reduction of an HPV type targeted by the vaccines. Methodological considerations – Many trials included multiple underpowered subgroup analyses, which increase the chance of false-positive findings. All trials except CVT reported relative rather than absolute effects, which tend to overstate efficacy, and none provided numbers needed to vaccinate.
Supplemental Material
JRS899308 Supplemental material - Supplemental material for Will HPV vaccination prevent cervical cancer?
Supplemental material, JRS899308 Supplemental material for Will HPV vaccination prevent cervical cancer? by Claire P Rees, Petra Brhlikova and Allyson M Pollock in Journal of the Royal Society of Medicine
Footnotes
Declarations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.