
Abstract
Objectives
The number of doctors directly entering UK specialty training after their foundation year 2 (F2) has steadily declined from 83% in 2010 to 42.6% in 2017. The year following F2, outside the UK training pathway, is informally termed an ‘F3’ year. There is a paucity of qualitative research exploring why increasingly doctors are taking F3s. The aim of this study is to explore the reasons why F2 doctors are choosing to take a year out of training and the impact upon future career choices.
Design
This is an exploratory qualitative study, using in-depth interviews and content analysis.
Setting
UK.
Participants
Fourteen participants were interviewed from one foundation school. Participants included five doctors who commenced their F3 in 2015, five who started in 2016 and finally four recently starting this in 2017.
Main outcome measures
Content analysis was conducted to distill the themes which exemplified the totality of the experience of the three groups.
Results
There were four predominant themes arising within the data set which can be framed as ‘unmet needs’ arising within foundation years, sought to be fulfilled by the F3 year. First, doctors describe exhaustion and stress resulting in a need for a ‘break’. Second, doctors required more time to make decisions surrounding specialty applications and prepare competitive portfolios. Third, participants felt a loss of control which was (partially) regained during their F3s. The final theme was the impact of taking time out upon return to training (for those participants who had completed their F3 year). When doctors returned to NHS posts they brought valuable experience.
Conclusions
This study provides evidence to support the important ongoing initiatives from Health Education England and other postgraduate bodies, exploring approaches to further engage, retain and support the junior doctor workforce.
Keywords
Introduction
Modernising Medical Careers 1 set out the current UK medical training pathway, envisaging that doctors would move seamlessly between foundation years (F1 and F2) and specialty training. There has been a steady decline in the number of doctors doing so, from 83% in 2010 2 to 42.6% in 2017. 3 The year following F2, away from the UK training pathway, is informally termed an ‘F3’ year. There is a growing cohort of doctors taking one, or even more (‘F4’), year(s) out of training.
There is limited qualitative research relating to reasons why UK junior doctors take time out of training. Lambert et al. 4 conducted a cross-sectional questionnaire survey, aimed at establishing why doctors consider working abroad. The sampling frame was all UK doctors who graduated in 2008 and in 2012, with 5291 respondents. The authors undertook qualitative content analysis of themes arising in selected white space responses. Common themes were: (a) gaining experience abroad; (b) a perception that things are better abroad; (c) the NHS culture/state/politics; and (d) training/job opportunities. This limited study was based upon two questions posed among a larger national survey.
Spooner et al. 5 published a mixed-methods study, using a quantitative cross-sectional survey (816 respondents) alongside a qualitative semantic thematic analysis 6 of 20 interviews. The study only explored how the new junior doctor contract effected career decisions. The sampling frame was all F2 doctors in England in a given year. They found that the new junior doctor contract had made 20% of doctors uncertain about their career choices and found doctors felt under-valued within the NHS and society.
Lachish et al. 7 conducted a cross-sectional survey in 2016, of 2324 F1 doctors to establish the association between perceived institutional support and intentions to work in the UK. They found that lower levels of support led to doctors being less likely to intend to stay in the UK. This study focused only on one particular possible cause of why doctors were leaving UK training programmes.
There is a paucity of qualitative literature exploring the complex motivations behind junior doctors taking an F3 year. A targeted study is therefore required to systematically explore the emergence of an F3 generation of doctors. The primary aim of this study is to explore the reasons why F2 doctors are choosing to take a year out of training. The secondary aim is to understand the experience of taking an F3 year and the impact of this on re-entering training.
Method
This is an exploratory qualitative cross-sectional study using content analysis of in-depth interviews. Full ethical approval was sought and approved from Brighton and Sussex Medical School Research Governance and Ethics Committee (ER/BSMS697/1).
Participants
Participants were doctors who started their F3 year in August 2015 (Group A), August 2016 (Group B) or August 2017 (Group C). There were five participants per group (total n = 15). This enabled data sufficiency, where additional interviews would not add further insight. 8 Doctors were interviewed at three different stages relative to their F3 year (all interviews conducted between October 2017 and January 2018). Group C were interviewed during their F3 year. Group B had recently completed their F3 year and were either taking an F4 year or had returned to training. Group A had either started an F5 year or had returned to training.
Doctors were eligible if they had completed their foundation training in a single foundation school and had not immediately progressed to specialty training. There were 438 eligible doctors for Group A, 465 eligible for Group B and 443 eligible for Group C. All eligible doctors were invited to participate via personal longstanding email addresses held by the foundation school. Where more than five participants volunteered for a given group, individuals were selected using purposive sampling to ensure that participant demographics (ethnicity and gender) reflected national data. 9 All participants provided written informed consent.
Data collection
The in-depth interviews (one per participant) were conducted face-to-face or via Skype. A semi-structured topic guide was used (see online Supplementary material). The interviews encouraged participants to talk about their experience without interruption. This enabled the participant to control the content, rather than the agenda being imposed by the researcher. 10 An in-depth approach was used to explore the individuals’ lived experience of the decision to take time out of specialty training. Interviews were audio-recorded on a digital handheld device or Ecamm Skype call recorder and lasted on average of 34 min (range 28–47 min). Each pseudoanonymised audio file was transcribed by a professional transcription service (Voicescript). Transcripts were checked against audio-recordings to ensure data quality.
Data interpretation
Content analysis 11 was used to distill the themes which exemplified the totality of the experience of the three groups. The content analysis coding was performed by three research team members (CRi, JM, CRa), reducing subjectivity. 12 Process tracing was further applied for theory-testing, to test alternative explanatory hypotheses.13,14 The research members discussed resulting themes and mutual agreement was reached. Exemplar quotations are provided along with year the participant started their F3 and participant identifier.1–5
Results
There were 24 eligible respondents. Of those selected, nine were female and six were male (for each group three female, two male). The last participant interviewed (Group C, female) was later found ineligible, resulting in 14 interviews. The average age of participants was 30 (range 27–35). Participants represented 13 different medical schools and were predominantly white British (10/14). Three of the interviews were conducted face-to-face and 11 by Skype.
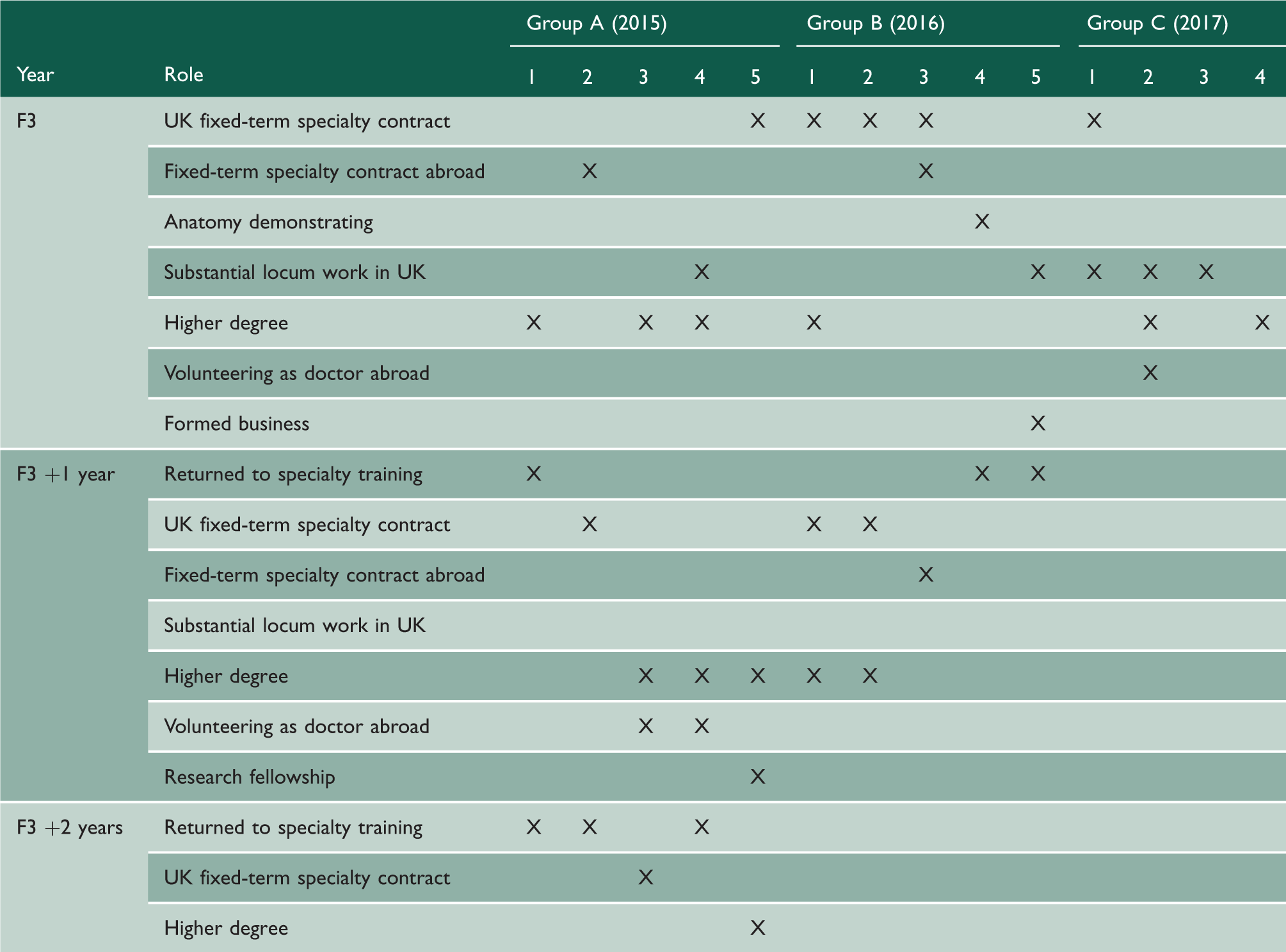
Summary of roles taken during F3 year and beyond.
Comments from participants reflected the scale of junior doctors taking time out. Most participants reported their decision to embark on an F3 year was validated by their peers and friends who were similarly taking time out, finding this ‘reassuring’ (2015;1). One participant noted ‘I would have been an odd one out, if I’d gone [straight] into training’ (2016;1). Participants who started their F3 in 2015 appear to have felt less certain and more anxious about their decision initially, with one reflecting ‘my peers were sort of nervous for me, was this a good idea?’(2015;4).
There were four predominant themes arising across all three groups regarding the decision to take time out of training. First, participants describe exhaustion and stress resulting in a need for a break. Second, participants required more time to decide and prepare for specialty applications. Third, participants felt a loss of control which was (partially) regained during F3 years. The final theme was the impact on return to training (for those participants who had completed their F3 year at the time of interview).
Alleviating stress and exhaustion
Participants reflected upon their experiences of foundation training prior to taking time out. Many felt that they were put in situations where they were out of their depth (particularly when on-call). Issues surrounding workload were compounded by staff shortages. Participants reported feeling unsupported by senior colleagues. One participant (2016;3) recalled days at work where she did not have time to eat or use the bathroom. Another (2017;1) reported that staff shortages meant she was unable to attend compulsory teaching. Meanwhile, one (2017;2) was put under pressure to work beyond 13-h days due to staff sickness. There were more reports of issues relating to staffing levels and lower levels of support in Group C (2017). While all participants had a strong desire to do their best for patients, one reflected with regret that he became resentful of patients due to work overload (2015;4). Others described feeling they were fighting an uphill battle: You couldn’t do a good job. And we are all people that aspire for the best … the fight you were having everyday just to scrape through, and you’re constantly providing inadequate care to people that you really want the best for. (2015;4)
The general morale appeared low, both within participants and their colleagues. There was a sense that junior doctors feel undervalued and under-appreciated. Participants described being treated ‘like a ward mule’ (2015;2) or feeling used for ‘service provision’ (2017;2). However, many participants did enjoy aspects of foundation training, especially where they were given specific learning opportunities.
A number of participants were warned against the concept of taking time out of training by consultants and family members, adding further stress during foundation years. One participant reported being told ‘it would be career suicide’ (2015;4). However, for other participants, consultants and supervisors were in support. The participants who most recently embarked upon their F3 year (Group C) reported higher levels of senior backing, linking this to increasing numbers of trainees taking F3s (2017;3).
The reported stress and exhaustion was partially alleviated during participants’ time out of training. Taking F3s enabled them to recuperate, look after themselves (including sleeping and exercising more) and regain energy.
Participants additionally reflected upon the stress and energy levels of their peers who had not taken time out. Many reported these colleagues were exhausted, one describing them as ‘pretty miserable’ (2015;4). Some participants reported that their peers wished they had taken an F3 (2016;2) and were planning to take time out at a later stage, for example after core medical training or GP training. One participants reported that senior colleagues including consultants have said: ‘if we could do it, we would do’ (2017;2).
Specialty indecision
A second major factor in participants’ decision to leave surrounded making specialty applications. While applications occur roughly six months into the F2 year, many felt that they were not then ready to decide which specialty to apply for. Some participants felt they had inadequate experience in given specialties to decide which to pursue. This is illustrated by one participant (2016;3): I didn’t apply for specialty training that early on in F2 because I didn’t know what to apply for. So that was probably the main reason why I took an F3 in itself. I just wanted a bit of time out from that overwhelming, busy feeling. And to, you know, readjust and think, okay, is this what I like, is this what I want to do? (2015;2) Applying for specialty training takes quite a lot of time and energy doesn’t it? Like you have to compile a portfolio, you have to practice for interviews and how are you meant to do that with your crazy 1A job [highest banded junior doctor job with greatest contracted work hours], I don’t know? (2017;4)
Losing and reclaiming control
Participants felt a loss of control across a broad range of factors during foundation years, including physical location and rotas. Participants also expressed great difficulties in arranging study leave or annual leave, feeling ‘controlled by rota coordinators’ (2016;5). This was echoed by one of the study participants, who remarked, ‘you sort of leave me with your vulnerable patients every day but yet you don’t trust me to organise my leave’ (2015;4).
Multiple individuals described a sense of being trapped on a conveyor belt of education from school, through medical school and onto postgraduate training. One described his feelings towards this as ‘training ladder fatigue’ (2016;4). The participants interviewed indicated they would be working for the NHS into their 60 s and 70 s, but many described sensing there was ‘no rush’ to get to Consultant level. Instead, participants wanted to take the opportunity to take a step back, as ‘they just can’t face climbing another ladder’ (2017;1).
There was also a sense of loss of autonomy, with participants feeling a sense of self-sacrifice (2015;4) and ‘helplessness’ (2017;4). One (2015;1) even described Feeling like some greater power is in control of your life the whole way through.
The loss of control was further exacerbated among many by a perception of being required to ‘jump through hoops’. This related specifically to the ePortfolio, with multiple participants describing this as time-consuming ‘box ticking’ exercises.
In contrast, taking an F3 enabled the ultimate regain of autonomy as there was no specification over what needed to be done during this time out of training. Participants were able to do things of personal importance and to tailor roles to their own learning. Participants valued the flexibility (2015;5), freedom (2016;5) and ‘ability to personalise training’ (2015;4) afforded by a year out. One participant aptly summarised this: The [F3] years that me and my friends and colleagues took were so different in terms of what they actually looked like … that's the first time in almost a decade that you have the ability to do that. (2015;1) a step off the treadmill I suppose, because that’s the thing, you can still work on your CV and you’re still a better applicant and you lose nothing … ‘cause that year is a more enjoyable, fulfilling year for you as a human being.
Return to training after the F3 year
Among the 10 participants who were interviewed more than one year after completing their F2 (Groups A and B), seven took F4 years while only three had re-entered specialty training straight after their F3 (Table 1). During this time, of the seven who took F4 years, three did fixed-term specialty contracts in the UK and another in Australia. Five of the participants did higher degrees, one as part of a research fellowship. A further two participants volunteered as doctors abroad during their F4 years. Of the five participants interviewed more than two years after completing F2 (Group A), two went on to take an F5, while two started specialty training at that point, and the final participant entered into their second year of specialty training. During the F5 years, one participant did a further fixed-term specialty contract in the UK and the remaining doctor was completing his PhD.
A number of participants applied for specialty training during their F3 year but turned down training post offers and continued to take time out of training. Two participants did so due to unfavourable locations away from partners or family (2016;1; 2016;2). Another participant (2015;3) reported being offered his ‘130th choice’ training post. This participant went on to create his own out of programme training, as he felt this provided him with increased control and ability to tailor his learning, aiming to obtain alternative competencies. One participant (2015;4) applying for specialty training during their F3 year described this as ‘sort of practice … I didn’t take that job and did the interview again in F4, and got my first choice’.
It appeared there were barriers to applying for training while taking an F3 year in Australia. One participant was put off applying due to the logistics of flying home for face-to-face interviews (2015;2). Another participant did not apply for specialty training during her F3 year because her year-long contract in Australia started in January (overlapping with two academic years in the UK), so ‘it kind of just naturally run into an F4’ (2016;3). Aside from those in Australia, participants reported minimal barriers in returning to training, one reporting ‘psychological rather than specific logistical [barriers]’ (2015;1). Some reported that consultants considered them to be desirable specialty candidates, with one participant remarking that his time out of training conducting research on Mount Everest (2015;5) is ‘all [interviewers] want to talk about’.
Participants described feeling more mature and confident, alongside offering greater clinical and life experience. Participants felt that time out of training helped them in obtaining skills which are required to be good doctors, for example in dealing with immense suffering within palliative care (2015;4) or the range of knowledge required of GPs (2017;3). Another was able to apply the artificial intelligence expertise he had gained during his F3 year during his clinical radiology training (2016;5). Participants felt more positive and ‘in a much happier space mentally’ (2015;1) upon return to training. They also described feeling ‘more refreshed’ (2016;4) and ‘full of energy’ (2015;4).
When asked what participants would advise younger generations of doctors, all reported encouraging others to take time out of training as a valuable experience that has enriched their early career as a doctor. Some cautioned that doctors must ensure they are doing something productive (2016;3) and others warned of problems with taking longer periods out of training (2016;5). A number felt that they were not given adequate formal support in deciding to take an F3 year, with one participant suggesting that mentorship from near-peers would have been helpful (2015;2).
Discussion
The flow of junior doctors has become more unpredictable in recent years, with 57.4% currently not following the intended career path. 3 This represents a major problem for workforce planning, particularly in light of a recent report by the General Medical Council indicating that doctors are at their limits and that stress is causing many doctors to ‘consider future options that would reduce or end their clinical practice’. 15 Findings of the General Medical Council report on the state of medical education and practice in the UK reflect those of this study, highlighting burnout and poor mental health among junior doctors, lack of support and deterioration in work-life balance. 15 This study identified a number of factors underlying doctors’ decisions to take time out of training.
Participants in our study reported high stress levels and feeling over-worked within their foundation years, which is supported by other research. The 2017 GMC National Training survey found that 25% of doctors in training felt short of sleep on a daily or weekly basis and 40% rated work intensity as ‘heavy’ or ‘very heavy’. 16 A Dutch study 17 concluded that 21% of residents (out of 2115) fulfilled the criteria for moderate to severe burnout. A large UK questionnaire survey (6220 participants) 18 identified excessive hours and lack of time for reflection among junior doctors. Furthermore, this study found doctors commonly expressed concern regarding the balance between service provision, training and education.
The present study indicates that doctors feel a pervasive sense of loss of control. This was previously highlighted in 2012 by a King’s Fund report which concludes (p17), ‘[The NHS] employs some of the brightest people in the country, then disempowers … them’. 19 The perceived loss of autonomy causes particular distress among doctors, who typically highly value being in control, with loss resulting in deterioration in physical and mental wellbeing. 20
Our study also indicates doctors did not feel ready to make specialty decisions during their F2 year. Tooke predicted an increase in the number of doctors not going straight into specialty training in 2008. 21 ‘The Tooke Review’ concluded that the 2005 Modernising Medical Careers training programme was ‘unlikely to … offer appropriate flexibility to trainees … It risks creating another “lost tribe”’ 21 (p4). Tooke went on to recommend that the existing pathway should be abolished, in place of a more flexible and transferable training stem system. The 2013 Shape of Training Review 22 later recommended broader training, outcome-based programmes and flexible work patterns which may alleviate this. These suggested changes were not apparent to the doctors in this study.
The majority of our participants re-entered training within three years of taking time out. This reflects findings from Goldacre et al. who found that the majority of British medical graduates do end up practicing in the NHS in the long term. 23 There appeared to be more barriers to returning to training following taking time out of training abroad. Sharma et al. found that of the 1.4% of UK graduates who are practicing abroad in New Zealand, only 30% originally intended to stay, but ultimately 89% planned to permanently emigrate, in part due to better lifestyle and disillusionment with the NHS. 24
This study highlights the broad range of additional relevant skills and diverse experiences that can be obtained during years outside of training. Participants embarked upon a range of formal qualifications during their time out, ranging from specialty membership exams to a PhD. A Higher Education Academy 25 systematic review identified that career progression should involve enhancing and empowering the learner to take control of their own career. Our participants who re-entered UK training returned with broader portfolios of experience, which enhanced competitiveness in a way similar to those who take time out at later stages during specialty training programmes. 26
There are a number of limitations to this study. There is a risk of recall bias, as participants are retrospectively recounting experiences and decision processes. Their responses may be altered through knowledge that their answers will be recorded and scrutinised, risking observer bias and the Hawthorne effect. 27 However, this qualitative study focuses on transferability and does not seek to make generalisable claims.
Conclusions
This study explores the reasons why doctors take time out of training. The findings raise questions about the future of run through training and timing of making specialty choices. This study provides evidence to support the important ongoing initiatives from Health Education England28,29 and other postgraduate bodies, exploring approaches to further engage, retain and support the junior doctor workforce.
Supplemental Material
Supplemental material for Why are UK junior doctors taking time out of training and what are their experiences? An qualitative study
Supplemental Material for Why are UK junior doctors taking time out of training and what are their experiences? An qualitative study by Chantelle Rizan, Julia Montgomery, Charlotte Ramage, Jan Welch and Graeme Dewhurst in Journal of the Royal Society of Medicine
Footnotes
Declarations
Competing Interests
None declared.
Funding
This research was funded by Health Education England Kent Surrey and Sussex.
Ethics approval
Full ethical approval was sought and approved from Brighton and Sussex Medical School Research Governance and Ethics Committee (ER/BSMS697/1).
Guarantor
JM.
Contributorship
GD and JW both conceived the research. CRi led the planning of the research, acquisition, analysis and interpretation and drafting of the manuscript. JM and CRa were also involved in the design of the research alongside data analysis, interpretation and drafting of the manuscript. In addition, JM is the guarantor, accepting responsibility for the work and conduct of the study, as Principal Investigator. All authors were involved in drafting the article and have approved the final version. All agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgements
None.
Provenance
Not commissioned; peer-reviewed by Emily Ward and Julie Morris.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.