
Abstract
Objectives
To investigate doctors’ intentions to raise a patient safety concern by applying the socio-psychological model ‘Theory of Planned Behaviour’.
Design
Qualitative semi-structured focus groups and interviews.
Setting
Training venues across England (North West, South East and South West).
Participants
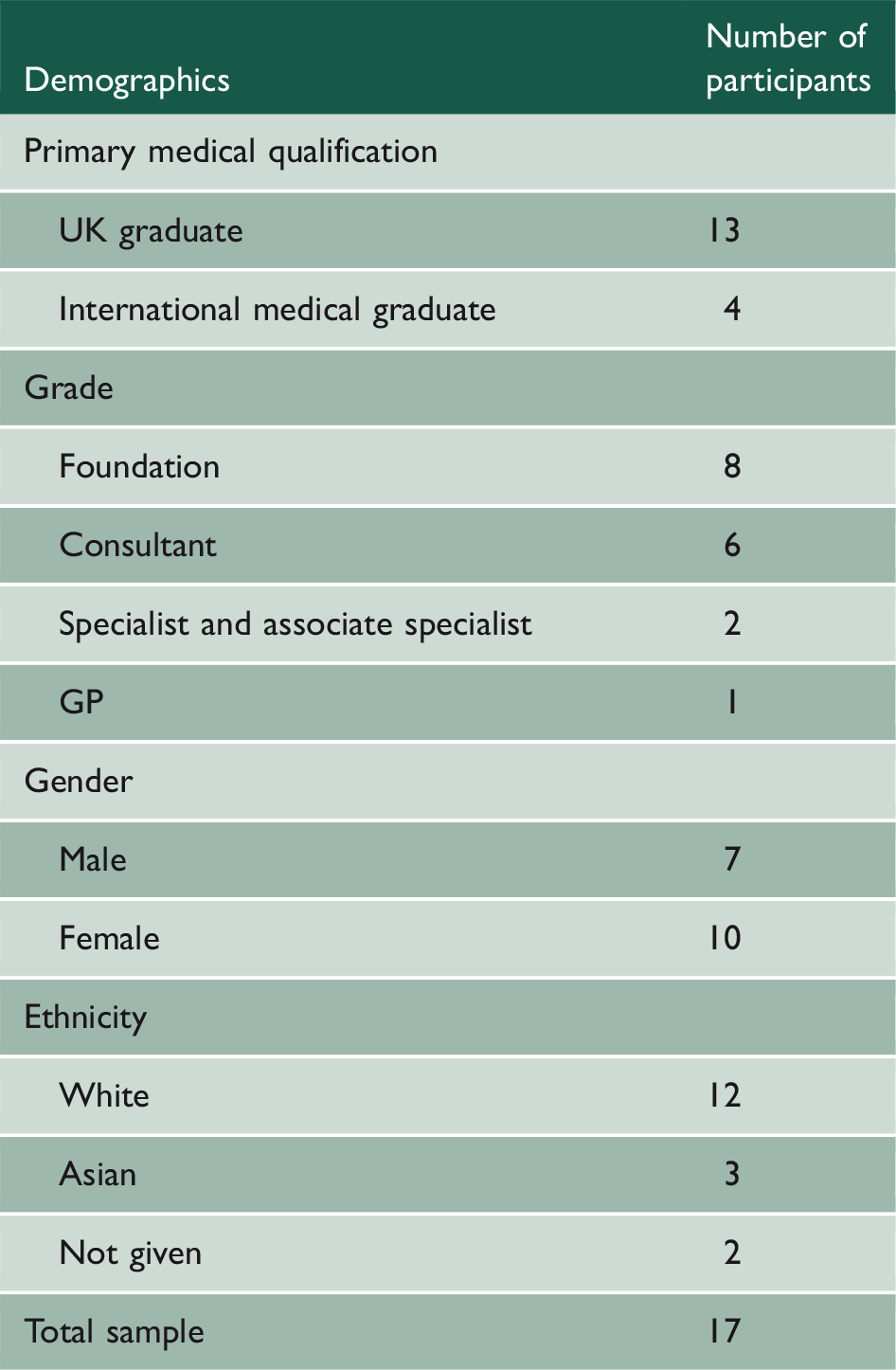
Sampling was purposeful to include doctors from differing backgrounds and grades.
Main outcome measures
Perceptions of raising a patient safety concern.
Results
While raising a concern was considered an appropriate professional behaviour, there were multiple barriers to raising a concern, which could be explained by the Theory of Planned Behaviour. Negative attitudes operated due to a fear of the consequences, such as becoming professionally isolated. Disapproval for raising a concern was encountered at an interpersonal and organisational level. Organisational constraints of workload and culture significantly undermined the raising of a concern. Responses about concerns were often side-lined or not taken seriously, leading to demotivation to report. This was reinforced by high-profile cases in the media and the negative treatment of whistle-blowers. While regulator guidance acted as an enabler to justify raising a concern, doctors felt disempowered to raise a concern about people in positions of greater power, and ceased to report concerns due to a perceived lack of action about concerns raised previously.
Conclusions
Intentions to raise a concern were complex and highly contextual. The Theory of Planned Behaviour is a useful model to aid understanding of the factors which influence the decision to raise a concern. Results point to implications for policymakers, including the need to publicise positive stories of whistle-blowers and providing greater support to doctors.
Keywords
Introduction
Given that ‘to err is human’, 1 doctors and other healthcare workers in clinical settings do experience mistakes which pose substantial risks to patient safety.2,3 The burden of harm from preventable problems in healthcare is substantial 2 and patient safety is a global concern as healthcare organisations struggle to deliver safe care. In the UK, doctors have a professional duty to raise and act if they have a concern about patient safety. 4 Understanding the factors that influence doctors raising a patient safety issue, such as their attitudes towards raising a concern, and the degree to which these influence safety behaviours, is critical to improving patient safety. 5
Few studies have proposed a comprehensive theoretical framework to explain patient safety behaviours.6,7 The Theory of Planned Behaviour
8
(Figure 1) is one of the most widely used psychological theories and has been shown to have successful prior use in explaining the behaviour of healthcare workers, including adherence to clinical guidelines,
9
and has been proposed as a useful framework to help understand lapses in professionalism among medical students.
10
The Theory of Planned Behaviour is an appropriate theory for explaining behaviours that are under volitional control, and studies have shown that healthcare professionals have volitional control over reporting a patient safety concern.11–16
The Theory of Planned Behaviour.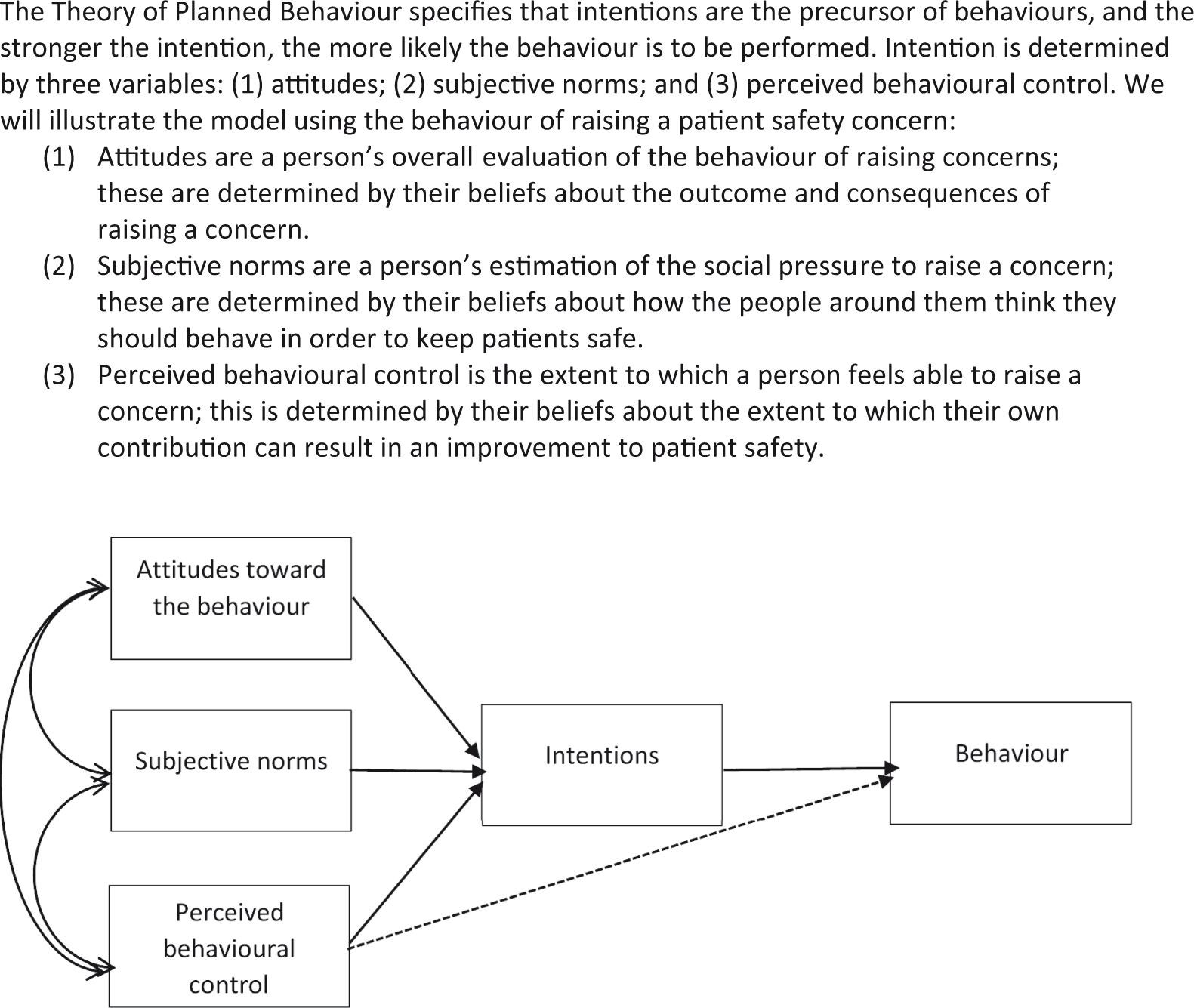
In this study, we investigate the factors that facilitate and hinder raising a concern using qualitative methods by applying the theoretical framework provided by the Theory of Planned Behaviour. This is important because to date the majority of research has been atheoretical
6
and where the Theory of Planned Behaviour has been applied it has been mainly for quantitative studies, where responses are captured using questionnaires around areas of interest determined by the researcher, meaning important factors may have been missed. Furthermore this study intends to understand raising a concern from a broader perspective than merely incident reporting. The majority of studies thus far have focused on Incident reporting-events in which harm has occurred – rather than the broader issue of concerns – experiences of, and worries about, a broad range of factors that might pose a risk to patient safety, such as poor systems, lack of staffing and resources, or poor teamwork.
17
(p. 251)
Method
Design and sampling
The study received ethical approval from UCL ethics committee (5490/001). The interview schedule was semi-structured and developed based on guidelines for research using the Theory of Planned Behaviour. 18 Questions were deliberately broad and open-ended to allow participants to discuss areas important to them and thus were not confined to specific types of raising concerns (e.g. voluntary incident reporting). Data were collected via interviews and focus groups, and occurred in training venues, hospitals and GP practices across England (North West, South East and South West).
Participant demographics (n = 17).
Analysis
Audio recordings were transcribed verbatim and analysed using thematic analysis. 19 Analysis was primarily deductive, guided by the Theory of Planned Behaviour; however, the team also approached the data inductively (with meaning flowing from the data) and were open to themes occurring which were not accounted for by the Theory of Planned Behaviour. An iterative approach, sensitised by theory, informed the categorisation and coding of transcripts. The initial coding framework was developed by two researchers (AR - health psychologist, RV - linguist) based on analysing two transcripts. Each researcher coded the same two transcripts and discussion about these was used to devise the first iteration of the coding framework. Thereafter, a further transcript was coded using the framework, and due to little disagreement the final coding framework was agreed. The remaining transcripts were coded using QSR NVIVO 11© 20 and the researchers met regularly to ensure consistency.
Results
Summary
Thematic analysis revealed four overarching themes in line with the variables of the Theory of Planned Behaviour. The first theme addresses attitudes towards raising a concern, which describes participants’ fears about the consequences of raising a concern on both themselves and others. The second theme, subjective norms, illustrates pressures from organisational norms which inhibit the disclosure of a concern and the negative influence of the treatment of whistle-blowers. The third theme, perceived behavioural control, illustrates how doctors often felt disempowered to raise a concern if the person who was the subject of the concern had greater authority and as a result of lack of feedback from previous concerns raised. The fourth theme concerns behavioural intentions, which identified that the course of action depended upon a doctors’ grade, with foundation doctors more likely to turn to their supervisor as opposed to regulator guidance.
Quotes have been anonymised with identifiers as follows: Ethnicity/Grade/Primary Medical Qualification and abbreviations used for specialist and associate specialist (SAS), UK medical graduate (UKMG) and international medical graduate (IMG).
Theme 1: Attitudes towards raising a concern
Two sub-themes:
Fear of negative consequences for themselves
Fear of negative consequences for the doctor who is the subject of the concern
Fear of negative consequences for themselves:
While the general sentiment was that most doctors approve of raising concerns as a behaviour, raising a concern in practice was not as straightforward as regulator guidance suggests. There were perceived negative consequences for the doctor raising a concern, who might then become isolated and be labelled ‘difficult’. Even if you are following the [regulator] guidance, what you may find is that you become an isolated practitioner, an isolated clinician at that point. (White British/Consultant/UKMG) And difficult colleague. (White British/Consultant/UKMG) The guidance is simple, the process isn’t … It’s not black and white and it’s not that easy, you are dealing with humans. (Asian/Consultant/IMG) You know, they are friends, they are colleagues … (White/SAS/IMG) The fact that there’s [regulator] guidance out there is not going to be the thing that decides me … I am going to do it because my internal, moral and ethical code says I have to do this for patient safety, I would be there thinking, okay, how dangerous do I think it is for patient safety, because it’s going to be a pretty miserable journey for me, I am not expecting people to be very supportive. (White British/Consultant/UKMG)
Doctors were not just concerned about themselves, but also about the impact on the doctor subject to investigation. Participants were empathic to the personal situation of the doctor and the likely damaging consequences for their career, financial and social circumstances. The other thing is the financial aspect, but if you think somebody has got a problem dealing with a job, due to drug dependency or something, so I have known people, families, so meaning dependent kids, for example partner, they have to pay, they lose everything basically, not just socially... Because then you feel guilty about you know, interfering with their family, their kids’ education, their partner’s lives, their own lives. (White/SAS/IMG) And I have serious concerns about the time frames. Justice delayed is justice denied, and so obviously it’s very very stressful for doctors to be put under the microscope in a potentially quite threatening and confrontational way that might even remove their livelihood, or more, see them in jail, and then be exposed to that process over a period, not only of months, but of years generally. (White/SAS/IMG) It’s one of the taboos in our society, the doctors can be ill and malfunction. (White/SAS/IMG) There were seven suicides in the last year within the M25 [motorway encircling London], all are able experienced doctors, that didn’t come on the news at all, isn’t it. But at the same time if a dog is run over … breaking news. So this is how doctors are valued. And in this day and age, alcoholism or drug addiction is considered a disease, and [well-known celebrity]…that is being praised, [well-known celebrity], he is addicted to painkillers, so he is being praised for being honest and coming out. But I have got a GP who is three years sober, back into practice and everything … Still in the clutches of GMC [General Medical Council],
b
can’t prescribe Codeine, and he is asking, a common man can get eight 500 Codeine off the counter, but I bloody can’t prescribe Codeine, what is this. (Asian/Consultant/IMG)
Theme 2: Subjective norms
Two sub-themes:
Pressure of organisational norms inhibit the disclosure of a concern
Negative treatment of whistle-blowers
Pressure of organisational norms inhibits the disclosure of a concern:
Organisational influences were important when considering raising a concern, both internal from within their NHS Trust and from external organisations such as regulatory bodies. In terms of their NHS Trust, the culture of the organisation was crucial in determining whether a risk to patient safety was raised, with some participants expressing that while colleagues would agree in principle that raising a safety concern was appropriate, the reality of raising a concern in practice was frequently met with disapproval from a number of groups, including management, other health professionals and administrators: Other colleagues will give lip service and agree that this is a risk or this is unacceptable, but then when you actually say … this needs to be flagged to senior, to management as a risk … and then even if they kind of agree with you on principle, they sort of say, oh, do you really think … there seems to be a certain amount of other people step back a little bit I would say right across [the organisation]. I would say a large part of professionals, and also medical colleagues, and also administrators, so yes, the lot really. (White British/Consultant/UKMG) Management would say, patient safety is our first concern, please speak up if you have any issues. They would absolutely advocate you follow [regulator] guidance and that, but then the practicalities of okay, well in which case, please cancel these clinics, please employ two extra doctors, please sack this doctor because they can’t communicate, those are the steps that then don’t happen because everyone goes, wooah, can’t do that, we have got a waiting list of 24 weeks and the [statutory health body] aren’t paying us. (White British/Consultant/UKMG) What’s it going to do to our outcomes? (White British/Consultant/UKMG) The CQC [Care Quality Commission
c
] are about to come back, we can’t say that one of our lead surgeons is a bully and needs to be expelled from the Trust, la la la. (White British/Consultant/UKMG) And it’s often due, because of the paperwork, you know like what we said, what’s going to come after that, I am going to be the bad books, even if I haven’t done officially anything bad, it’s a lot of red tape, a lot of paperwork, a lot of headache. (White/SAS/IMG) And somebody has got to take ownership of that and people don’t want that happening. (White British/Consultant/UKMG) [In appraisal] you will pick up the person who is spewing out lots of [incident reports] and is involved with lots of clinical incidents, but just as dangerous actually, is perhaps the person who is not doing anything, not reacting to what they are seeing. (White British/Consultant/UKMG)
Negative treatment of whistle-blowers:
Another important factor was the treatment of doctors who had raised a concern. For doctors in training, the Chris Day
d
case was particularly pertinent. As the following quote from a Foundation doctor illustrates, the case evoked fear that they themselves will not be protected for whistleblowing and this uncertainty caused ambivalence towards raising concerns: I guess the Chris Day case … that is quite frightening... one week we hear that whistleblowing – we’re supposed to do it. And then we get another the next week; it’s like: oh, but you’re not actually defended if you do do it. (White British/Foundation/UKMG) I think as long as you have got a situation where a trainee raising issues losing their training number and has to go to a high court to get it back, you are unlikely to change the culture and the fear about doing this. We have, as a medical profession, just alienated an entire generation of trainees to doing the right thing, because the one person that they saw do the right thing got horribly penalised and has had a miserable three years. (White/Consultant/UKMG) I don’t see whistle-blowers held up as this doctor is amazing, look what they did, they have saved lives, they have changed this hospital for the better. (White British/Consultant/UKMG) One of the best outcomes is to be able to continue to work, really isn’t it, raising the concern and still being able to carry on with your job. (White British/Consultant/UKMG) If you’re lucky, you can work in the same place, but if you are unlucky you have to move Trusts or nation. (White British/Consultant/UKMG)
Theme 3: Perceived behavioural control
Two sub-themes:
Regulator guidance can act as an enabler to raise a concern
Ability to raise a concern is dependent on the power of the doctor whom is the subject of the concern
It’s there; you can say, I have to do this because our guidelines say … essentially tells me I have to do this... you know, it’s definitely not a personal thing; you can see why I’m doing it; it’s on this guideline here. So it is very useful in that respect. (White British/Foundation/UKMG)
Given the negative repercussions for the doctor raising the concern, having the support and approval of colleagues was an important factor in the decision to take action. The extent to which a doctor felt able to raise a concern was determined by their role within the organisation and whether the person they were concerned about held a position of power. It depends on the type of concern … because there’s a consensus among the team that actually there was an individual on another team that were perhaps causing some risk to patients, that would be more straightforward, but if it wasn’t something that would be generally supported, or if the person you were concerned about wielded a lot of influence, that could be quite challenging. So it’s very situational dependent I think. (White British/Consultant/UKMG) In terms of our behaviour at large and the powers that be, and who wants politically I think to have a chastised Responsible Officer would look very bad, so I don’t think it would go anywhere. (White/GP/UKMG) Maybe one of our supervisors … just purely because they’re responsible for your assessment in some way, shape or form as well. So to raise a concern against somebody who’s then going to be grading you in about a month’s time or so seems a bit … there’s something not quite right about that. (White British/Foundation/UKMG) If someone’s going to be signing you off in a month’s time and you need it, then you may be more hesitant to just jump straight in. (White British/Foundation/UKMG)
Doctors spoke of having raised concerns through the hospital system, which had then been ignored. As a result, they did not believe that their actions could result in an improvement to patient safety, and so ceased to raise them: I think you need ten times the good news stories than you need the bad news stories, so if you want me to put in a [incident report], I need to get feedback about that, I need to feel as if something I am doing is actually making a difference because otherwise you do it for as long as you can and then you burn out, and that’s proven time and time again. (White British/Consultant/UKMG)
Behavioural intention
In terms of participants’ intention to raise a concern, Foundation doctors considered regulator guidance on raising a concern would have greater relevance when they were further on in their career and instead they would consult with their supervisor. It’s probably easier at this stage, isn’t it, because if you have a concern then you would just speak to like your kind of career and education supervisor whereas maybe you would need more and guidance later on in your career and you don’t have seniors anymore to ask for help. (White British/Foundation/UKMG) If we had a systems problem within our department, you have now got a cohort of like-minded people who have had the same training who would be able to voice more strongly, actually, you know, this is a line in the sand and the GMC say this, so we are going to, and then you are four rather than one, so it’s a lot less intimidating isn’t it? So it’s quite good, it’s quite good for a networking of like-minded similarly trained individuals. (White British/Consultant/UKMG)
Discussion
Principal findings
Intentions to raise a concern were conceptualised according to the three variables of the Theory of Planned Behaviour, postulated to influence the strength of doctors’ behavioural intentions to raise a patient safety concern: attitude; subjective norms; and perceived behavioural control.
Doctors’ attitudes toward raising a concern were multifaceted. Raising a concern was considered an appropriate professional behaviour particularly for patient safety issues. However, doctors expressed trepidation about actually raising concerns, suggesting a mismatch between the idea of raising a concern and the reality. Negative attitudes toward raising a concern were dominant. This was due to fear of negative consequences both for the doctor subject to investigation and for themselves, with ramifications for damaging relationships with colleagues; such fears for the implications on relationships have been found elsewhere.21,22
Social norms were a powerful influence, particularly at an interpersonal and organisational level, which often acted to inhibit the disclosure of a concern. Organisational constraints of workload, resources and culture were a major influence and acted to significantly undermine doctors raising concerns. There appeared to be an implicit understanding among some participants that the organisational culture was one where incidents were not actioned or even acknowledged, and thus behaviours such as incident reporting were considered pointless. Organisational issues and a culture of blame have been discovered elsewhere as negatively impacting on reporting. 23 High profile cases in the media, such as the Chris Day case, 24 where whistle-blowers received adverse treatment were reported as influential obstacles to raising concerns, as identified in another recent study. 23
Regarding participants’ perceived behavioural control participants reported that lack of feedback led to demotivation to report, identified as a barrier in previous research. 23 While regulator guidance could be used to justify raising a concern, how able participants felt to raise a concern depended on whether their colleagues approved, and on the individual in question; it was acknowledged that raising a concern against someone with greater power would be more challenging. Power dynamics have been recognised as an important factor in the decision to speak up22,25 and foundation doctors talked about potential conflicts of interest if they had a concern regarding their supervisor.
Meaning of the study: possible explanations and implications for clinicians and policymakers
The results suggest there would have to be a significant risk to patient safety for a doctor to raise a concern. These barriers can be classified according to the Theory of Planned Behaviour, and at three further levels: individual; interpersonal; and organisational. Barriers need to be addressed at each level, which can also be conceptualised using variables from the Theory of Planned Behaviour (included in brackets below):
Professional guidance, such as the General Medical Council’s ‘Raising and acting on concerns about patient safety’, which applies to all doctors, including trainees, acknowledges some of these barriers: You may be reluctant to report a concern for a number of reasons. For example, because you fear that nothing will be done or that raising your concern may cause problems for colleagues; have a negative effect on working relationships; have a negative effect on your career; or result in a complaint about you.
4,5
(pp. 7–8)
There are ongoing efforts to address some of these barriers since the publication of the Francis Report into the failings of care at Mid Staffordshire NHS Trust, 26 and more recently the ‘Freedom to Speak Up’ review into whistleblowing, 27 which highlighted many remain fearful of raising a concern, with those whom have raised concerns reporting victimisation, bullying and disciplinary action. Reforms designed to protect whistleblowers include the introduction of ‘Freedom to Speak Up Guardians’, 28 a dedicated person in each NHS Trust, whose role is to lead culture change and to whom staff can speak to confidentially. There has also been a reduction in timescales for doctors undergoing fitness to practice investigations 29 and helplines exist for doctors who feel unable to raise concerns at a local level, provided by the General Medical Council, NHS and the Care Quality Comission. However, significant challenges remain. While the dispute between Health Education England, the organisation with whom trainees hold their training contract, and the trainee Dr Chris Day resulted in trainees being able to claim legal protection for whistleblowing, as the findings here illustrate, the lengthy legal fight did little to reassure trainees that they would be protected if they raised a concern. Thus while reforms indicate progress is being made, reluctance to raise concerns persists, posing a continued risk to patient safety. There remains substantial work in fostering a culture where doctors feel able, and supported, to raise a safety concern without fear of negative repercussions.
Strengths and weaknesses of the study
A significant strength of the study is that the design and analysis is informed by the Theory of Planned Behaviour. To the authors’ knowledge, this is the first qualitative study to utilise the Theory of Planned Behaviour to examine the factors that influence doctors’ intentions to raise patient safety concerns. Theoretical models are valuable because they provide a mechanism for identifying the factors that influence behaviour and form the basis of developing interventions which can be systematically evaluated to examine what works, for whom and how.6,30 This study is important because it demonstrates the Theory of Planned Behaviour can be applied to aid our understanding of the factors influencing the decision to raise a patient safety concern, highlighting the importance of doctors’ perceptions of control to raise a concern, and organisational norms. The value of applying the Theory of Planned Behaviour to this particular topic lies in the model’s ability to understand and predict behaviour. The theory is one of the most widely applied theoretical models, with a systematic review demonstrating the Theory of Planned Behaviour can predict intention and behaviour in healthcare professionals. 31 The results of this study are being used as the basis for a Theory of Planned Behaviour questionnaire study with a larger sample of doctors (N = <300) to investigate intentions to raise a concern (in progress). This will further enable our understanding of the factors affecting doctors’ intentions to raise concerns, which can guide intervention development.
Regarding reflexivity, the research team consisted of both clinicians and researchers from varied backgrounds in general practice, health psychology, linguistics and medical education. Data were collected by all team members, and the team met repeatedly throughout the analysis to ensure the development of a shared understanding of the meaning of the data. We feel this is a particularly strength of the study as we were able to bring our own disciplinary insights into the interpretation of the data.
While the doctors were from a variety of career stages and backgrounds, the sample size was small. This was not considered problematic because we utilised the model of information power 32 to guide our sample size. This outlines that a study with a narrow aim, specific sample, supported by an established theory with strong dialogue with participants which focuses on cases, as opposed to cross cases, requires a smaller number of participants to obtain necessary insight. It is not proposed that the findings are generalisable to all doctors within the UK; however, they provide sufficiently rich data to fulfil the research aim of assessing the utility of the theory of planned behaviour to understand doctor’s intentions to report a patient safety concern.
Participants may have been influenced by social desirability bias due to the sensitive nature of the topics. The data were collected immediately at the end of a regulator-run training programme and thus they may have felt pressure to answer in terms of ‘best practice’ and been reluctant to give honest answers. To minimise this possibility, we emphasised throughout the data collection that the researchers were independent and anonymity would be protected.
Conclusion
The study illustrates that the theoretical framework of the Theory of Planned Behaviour has utility in understanding the factors that influence intentions to raise a patient safety concern. The results can be of benefit to the doctors of the future by improving the environment of raising concerns if relevant organisations such as the Department of Health, NHS Trusts, Care Quality Commission, British Medical Association, Medical Royal Colleges and the General Medical Council work together to address the individual, interpersonal and organisational barriers described.