
Abstract
Objective
To ask those most affected by continuing professional development for senior doctors – patients, other professional groups and doctors themselves – what it needs to encompass.
Design
The nominal group technique.
Participants
Six groups of between seven and nine members (n = 49). Separate groups were held for nurses and therapists (n = 9), patient representatives (n = 8), medical directors (n = 8), consultants (n = 8) and medical trainees (n = 7). An additional group consisted of ‘Darzi Fellows’ (n = 9), trainee doctors who were undertaking a leadership fellowship.
Setting
Groups were held at the Royal Society of Medicine in London.
Main outcome measures
Priorities for the content of continuing professional development for senior hospital doctors, ranked in order of importance. Themes derived from analysis of group discussions.
Results
We present the ranked priorities of different groups for what should be included in continuing professional development for senior hospital doctors. Analysis of group discussions identified the following three themes: developing and supporting the system of care; changes in the way medicine is practised; and personal wellbeing and caring for colleagues.
Conclusions
The implication of our findings for providers of continuing professional development is to consider the balance of content. Doctors and other healthcare professionals need to keep up with scientific advances and technical developments. But in addition, they need to be adept at working with the system changes required for translation of research into practice, the development of new ways of working, and for the organisational changes that underpin continual quality and safety improvement.
Introduction
Throughout their career, doctors must continue to develop expertise and become proficient in the sometimes very rapidly changing technologies in their specialty. They must also keep up to date with advances in care more generally and with developments in associated fields. In contemporary care settings, doctors are increasingly expected to work in teams, be involved in management, and design services in collaboration with patients. 1 Clinical leadership has been found to play a crucial role in quality improvement, both within organisations and in wider systems of care. 2 Moreover, against the backdrop of unprecedented financial pressures on the National Health Service, fostering a culture of compassionate care requires that doctors nurture their own, and their colleagues’, health and wellbeing. 3 These changes in the context and practice of medicine have been incorporated into new understandings of what it means to be a doctor, for example, the Royal College of Physicians has redefined medical professionalism for the 21st century as ‘multiple commitments – to the patient, to fellow professionals and to the institution or system within which healthcare is provided.’ 4
In order to meet these challenges, continuing professional development must evolve. In this study, we asked those most affected by continuing professional development for senior hospital doctors – patients, other professional groups and doctors themselves – what it needs to encompass. We used the nominal group technique 3 to ask ‘what should be in continuing professional development for senior hospital doctors?’ Our aim was to initiate and inform discussion, debate and development of future continuing professional development for senior hospital doctors.
Methods
The nominal group technique 5 is a form of focus group that allows a wide range of ideas on a subject to be expressed and collated with a view to establishing consensus and identifying priorities. Unlike conventional ‘brainstorming’ sessions, in the early stages, the participants work in the presence of one another but do not interact. Therefore, the group is ‘nominal’ in the sense of being a group in name only. The benefit of the nominal group technique is its ability to foster creativity. A broader range of ideas are generated, and participants feel less inhibited than in other approaches as the technique prevents a single idea, or a charismatic personality, dominating discussion. The technique is also orientated to prioritising and ranking ideas so that information is gleaned on the relative importance of different ideas to individuals and groups.
Group composition
Six groups of between seven and nine members (n = 49) were held between February and June 2016. Separate groups were held for nurses and therapists (n = 9), patient representatives (n = 8), medical directors (n = 8), consultants (n = 8) and medical trainees (n = 7). One group consisted of ‘Darzi Fellows’ (n = 9), trainee doctors who were undertaking a clinical leadership fellowship (Darzi Fellowship). Members of the medical trainee group were in the specialist registrar grade. Clinical participants came from different hospitals in England and from a range of specialties including general medicine, surgery, psychiatry, obstetrics and gynaecology, anaesthetics, general practice and public health. Participants were recruited from databases held by the Royal Society of Medicine and through organisations that coordinate patient involvement in health research. FM emailed an invitation to participate in the study, and places were allocated on a ‘first come first served’ basis.
Procedure
We adopted a slightly modified form of the technique as follows:
Step 1. Welcome and introduction. Participants were offered refreshments and welcomed to the meeting and introduced to other participants and to the research team. The question for nominal group was displayed on a PowerPoint slide, together with a description of the procedure and ‘rules’ for the session. We asked a single question – ‘what should be in consultant continuing professional development?’.
Step 2. Silent generation of ideas. Participants were given 15 min to list as many responses to the question as possible. Silence was enforced during this stage, if necessary, by the facilitator requesting that participants who have finished the task do not distract others still working.
Step 3. ‘Round Robin’ listing of ideas on a flip chart. At the end of 15 min, the facilitator asked each participant, one at a time, to share one item from their list. The facilitator wrote the item on a flip chart in the exact words used by the participant. The focus during this stage was on listing ideas, without discussion. Participants were asked to omit ideas that had previously been given, if they were identical, but invited to contribute a variation on a theme. Participants could ‘hitch hike’ on other people’s ideas by adding additional items to their lists that had been inspired by something another participant had said. This process continued until all participants had exhausted their individual lists. The average number of ideas generated during this phase was 70 (range 56–97).
Step 4. Discussion of ideas on the flip chart. After all ideas were recorded on the flip chart, the facilitator led a discussion of the ideas now in front of the group in writing. The purpose of the discussion was to clarify, elaborate or illustrate the ideas in order to generate additional qualitative data. This was descriptive, rather than analytical, in that there was no attempt to collapse ideas into categories.
Step 5. Ranking priorities. In the final stage, participants were asked to list, in order of importance, their own individual top 10 priorities for consultant continuing professional development and to submit these anonymously to the facilitator. Participants were then thanked for their time, given information about the next stage of analysis and offered closing refreshments. Each group lasted for approximately 2 h.
Analysis and generation of a group ranking
Top 10 ranking of different groups.
Results
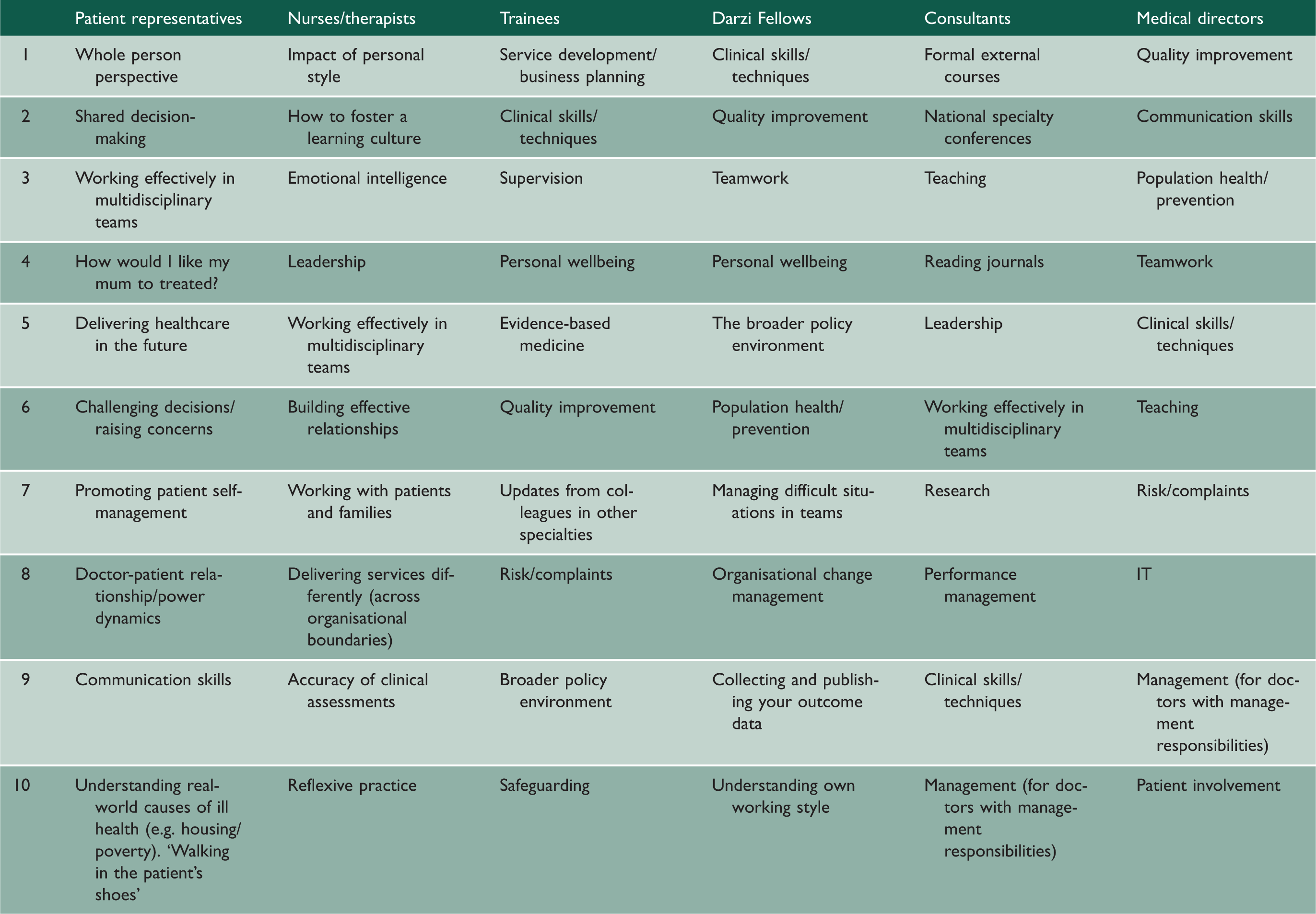
The ranking of the different groups are given in Table 1. Analysis of the full lists of ideas and group discussion identified the following three themes: (1) developing and supporting the system of care; (2) changes in the way medicine is practised; and (3) personal wellbeing and caring for colleagues.
Developing and supporting the system of care
While updates and training in clinical skills and techniques remained important to the doctors in our study, the suggestions from the medical groups reflected the additional roles that make up a career as a consultant, especially teaching and management. It was clear during the group sessions involving doctors that they felt a sense of responsibility that extended beyond direct patient care to the wider healthcare system. A priority for participants in the medical groups was not just providing care but improving it. And many showed an interest in developing services that were better suited to present and future healthcare needs. At the same time, participants were cognizant of the challenging financial and policy environment, often requesting to have training in business planning, designing appropriate metrics, and in collecting and publishing outcome data to meet demands to demonstrate effectiveness and cost control.
Changes in the way medicine is practised
The responses from all groups reflect changes in the way medicine is practised. For example, respondents wanted to learn more about working, and learning, in multidisciplinary teams. During the nurse and therapist group discussion, it was suggested that this should include deferring to other forms of expertise and knowing when to ask for help. A priority for the patient group was for consultant continuing professional development to support ‘shared decision-making’. Nurses listed ‘working with patients and families’ and medical directors listed ‘patient involvement’. Another feature of the contemporary context of practice that was highly rated for inclusion in consultant continuing professional development was risk and complaints. This was a priority for both medical directors and trainees. The patient group listed as one of their priorities learning how to raise concerns and challenge decisions if necessary.
Personal wellbeing and supporting colleagues
‘Personal wellbeing’ was included in the top 10 rankings for trainees and Darzi Fellows, and all groups talked about the importance of doctors’ own wellbeing and their ability to look after themselves. Alongside a managerial concern for learning ‘how to do performance management’, there were also expressions of a professional concern with helping colleagues in difficulty.
Differences between groups
There were some important differences between groups. Patients wanted consultant continuing professional development to engender a whole-person perspective. They also suggested that consultant continuing professional development should include providing kind, compassionate and respectful care, captured in the question ‘how would I like my mum to be treated?’ While a number of groups talked about the importance of prevention and population health in the abstract, the patient group talked about understanding the causes of ill health in terms of the lived experience of patients or as they called it: `walking in the patient's shoes'. Priorities for nurses and therapists included hospital consultants understanding the ‘impact of their personal style’ and developing ‘emotional intelligence’. Other highly rated elements of consultant continuing professional development from this group were knowing ‘how to foster a learning culture’ and ‘reflexive practice’.
Discussion
Statement of principal findings
We present the ranked priorities for the content of continuing professional development for senior doctors, of different groups directly affected by continuing professional development. Drawing on the ranked priorities, the full list of suggestions generated by participants, and group discussion, we identified the following themes: developing and supporting the system of care; addressing changes in the way medicine is practised, and personal wellbeing and supporting colleagues.
Strengths and weaknesses of the study
The value of our research is in asking a range of groups directly affected by continuing professional development, including patients, what should be in consultant continuing professional development. We know of no other similar research. We used a qualitative design and a non-probabilistic sample as our aim was to explore the topic with different groups, identify the needs of staff, reveal the priorities of our participants and draw together and discuss themes, rather than establish a statistical representation of phenomena. 6 A limitation of our study is that the sample did not include any specialty or associate specialist doctors, who may face barriers accessing continuing professional development. 7
Interpretation of findings in context of wider literature
The highest ranking element for medical directors was quality improvement. Recent research has highlighted the important role played by medical directors in quality improvement. 2 A study of organisations with highly developed approaches to quality improvement found that board-level clinical leaders brought in-depth knowledge and understanding of quality issues and provided the board with meaningful analyses of data. In high performing organisations, medical directors, in particular, appear to contribute important translation work using knowledge and skills drawn from their medical training or from dedicated training in quality improvement.
The doctors who participated in our study expressed a responsibility for the wider system of care. However, in most cases, this was in addition to existing responsibilities, to the patient, and to update technical skills, suggesting an increase in job demands on doctors. Empirical research has found that doctors with management roles may be isolated ‘lone wolves’ and lack organizational support. 8 It is therefore important for doctors to receive appropriate training and support for additional roles.
Implications for practice, policy and research
The implication of our research, for the providers of continuing professional development, is to consider the balance of the content of continuing professional development. Doctors and other healthcare professionals need to keep up with scientific advances and technical developments. But, in addition, they need to be adept at working with the system changes required for translation of research into practice; the development of new ways of working and for the organisational changes that underpin continual quality and safety improvement. Often the types of content outlined as important by our groups are included in short-term, stand-alone ’Leadership’ or ‘Management’ courses. Perhaps if this type of content was a regular and frequent component of doctors continuing professional development, this would reflect the contemporary experiences and needs of senior doctors, particularly in relation to the management roles held by doctors, and quality improvement. Our findings also support the development and use of innovative learning formats, especially learning from patients and with, and from, other members of the healthcare team. Future research should evaluate the introduction of new forms of continuing professional development from the perspective of staff and patients.
All groups in our study, including patient representatives, and nurses and therapists, identified doctors’ own wellbeing and their ability to look after themselves as an important area for continuing professional development. Work-related stress among doctors is a long-standing issue. 9 The desire to see support for doctors’ wellbeing among study participants aligns with increasing international recognition of the importance of fostering high-quality care through identifying and supporting doctors who are at risk of burnout.10,11 The most effective approach to preventing burnout combines individual interventions with organisation and system-level interventions. 12 As doctors take more responsibility for the wider system, the wider system must take more responsibility for the health and wellbeing of doctors.