
Abstract
Objective
To identify organizational barriers to and facilitators for female surgeons' career progression.
Design
Systematic review of qualitative and quantitative studies relating to organizational barriers to and facilitators for female Surgeons' career progression. After the quality assessment of the peer-reviewed journal articles, twelve articles were selected for full review. Thematic analysis was used to identify key themes in these selected articles.
Setting
The studies solely focused on organizational factors linked to female physicians' career progression in surgical specialties.
Partcipants
Female surgeons.
Main outcome measures
Organizational barriers and facilitators
Results
Twelve peer-reviewed journal articles were included in the study which focused on barriers to female surgeons' career progression, ways of facilitating female surgeons' career progression, and female surgeons' job satisfaction.
Conclusion
The major organisational factors contributing to the lack of career progression for female surgeons are (1) organizational culture which promotes rigid career structure that is inclined to support male surgeons than female surgeons and also male domination in which male surgeons feel superior to female surgeons (2) work family conflict whereby women feel that they have to make a family sacrifice by being women; they experience the difficulty in securing a work-life balance in the masculine career structure in surgical specialties. This implies that policy makers and healthcare organizations need to pay significant attention to organizational facilitators for female surgeons' career progression such as flexible career pathways and work patterns, a variety of different viable career progressions, more family-friendly working conditions, and the promotion of female mentors and role models in surgical specialties to support female surgeons in dealing with the organizational barriers in the male-dominated organizational culture and the lifestyle issues as well.
Keywords
Introduction
The percentage of women among medical students has been growing recently in both developed and developing countries, and the number of women in medicine has increased quite rapidly worldwide.1–3 However, women generally remain seriously under-represented in the field of surgery. For example, the proportion of women surgeons associated with the UK National Health Service was just 6.5%. 4 Such under-representation can impact on female patients’ satisfaction with the services they receive, as research shows that gender preference with regard to doctors is more prevalent among female patients than that among male patients. 5 For instance, women find female doctors more desirable for breast, cervical and colorectal screenings, because the procedures feel less embarrassing when women do not have to expose their body to a physician of the opposite gender. 6
Indeed, the number of women entering the field of surgery has risen due to the positive efforts made by medical schools, medical councils and healthcare providers. 7 Nevertheless, many women leave surgery before developing their career. The number of female physicians who change their specialty in the course of training is the highest in surgery. 2 Several researchers have argued that female doctors’ lifestyle preferences are the primary cause of this under-representation. They contended that women are more likely to choose a balance between work and personal life and often do not attach the same importance as men do to achieving a high income or a prestigious position.1,8
However, other researchers have strongly argued that there are persistent organisational barriers such as a female-unfriendly work environment which includes all-hours work and on-call duties and culture of gender discrimination in surgery and that such barriers create a ‘glass ceiling’ that prevents female doctors from rising beyond a certain level in the surgery hierarchy.9–12
As a result, some female surgeons shift to non-surgical specialties, such as general medicine and paediatrics, which do not seem to have the inconvenient obligations that come with life as a surgeon.12,13 This implies that examining organisational barriers to female career progression in surgery is a significant research area, although there has been very little research reported on this.
Consequently, we conducted a systematic review to identify organisational barriers and facilitators for female surgeons attempting to progress in their careers.
Methods
This study systematically identified, critically appraised, summarised and synthesised qualitative and quantitative studies relating to organisational barriers to and facilitators for female surgeons’ career progression.
We conducted a systematic literature search using different electronic databases including Google Scholar, CINAHL Plus, Medline, PubMed, Science Direct, ScienceDirect, Emerald Management and Wiley Online Library. These databases were searched using various combinations of the key terms included ‘women physicians’, ‘female doctors’, ‘surgeon’, ‘obstacle’, ‘barrier’, ‘gender-based discrimination’, ‘glass ceiling’, ‘work-life balance’, ‘part-time’, ‘family’, ‘children’, ‘career’, ‘satisfaction’, ‘surgical specialty’, ‘general surgeon’ and ‘obstetrics and gynecology’, and Boolean logic using ‘AND, OR’ was used to refine a number of articles. We adapted the Preferred Reporting Items for Systemic Reviews and Meta-Analysis when conducting this search
14
and identified 284 articles after title screening and excluding duplicates. Following a screening of the abstracts, 49 articles were selected by the first author for full text reading (Figure 1).
Preferred Reporting Items for Systemic Reviews and Meta-Analysis flow chart.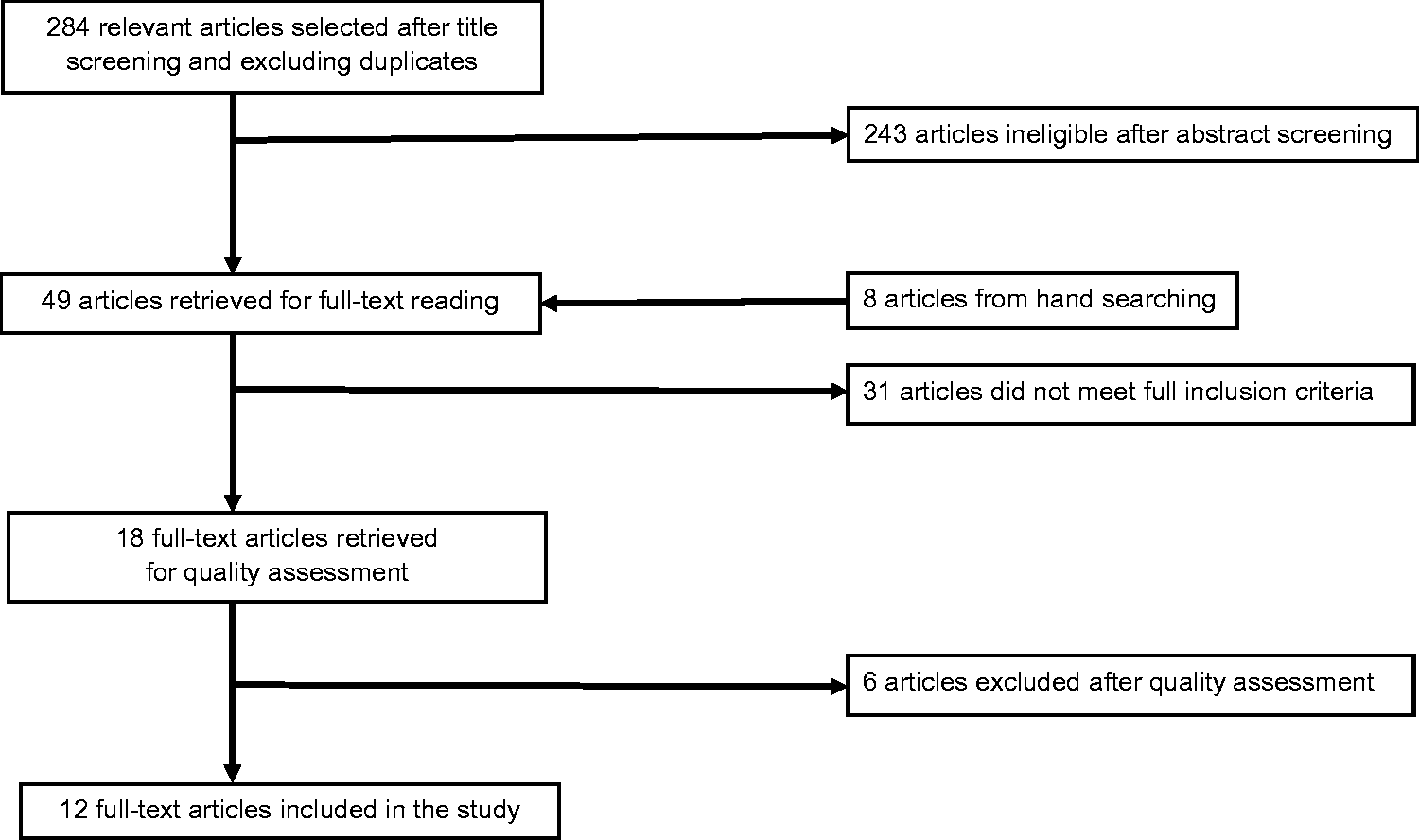
From the retrieved 49 articles, we identified studies which met the following inclusion criteria: (1) peer-reviewed English-language journals published in the last 10 years; and (2) studies solely focused on organisational factors linked to female physicians’ career progression in surgical specialties such as general surgery, academic surgery, paediatric surgery, plastic surgery, and obstetrics and gynaecology. The exclusion criteria were: (1) studies not focused on organisational factors linked to female physicians’ career progression in surgical specialties; (2) studies focused on male physicians/doctors and female doctors working in non-surgical specialties; (3) studies not published in English; and (4) studies published before the year 2005 in order to indicate the ongoing debate in the research area.
Using the above criteria, the both authors selected 18 articles for quality assessment. These articles were assessed using an appraisal checklist by Kuper et al. 15 The tool consists of six key questions, each question was categorised ‘yes’, ‘unclear’ or ‘no’. If one question was assessed as ‘yes’, it was counted as 1 point. If all questions were assessed as ‘yes’, the total quality score for a study was a maximum of 6 points. If the question was assessed as ‘unclear’ or ‘no’ it was counted as 0. Consequently, after the quality assessment, we deselected six articles because it was difficult to transfer the results of the studies reported in the papers to the setting of our study. 15 All of these deselected studies have quality scores lower than 5 and some of them have very low quality scores (e.g. 1, 2). As a result, including the results of these deselected articles in our analysis would not change the final outcomes of our systematic review significantly. The 12 articles selected for full review have quality scores of −5.
We extracted study details from each article and summarised them using a standardised data extraction form in order to reduce errors and minimise bias. Both authors participated in data extraction. The first author extracted all the studies included in the review. The second author extracted a random sample of 50% to assess the reliability. Any discrepancies were discussed by both authors and resolved by consensus.
A data extraction form by Bettany-Saltikov 16 was used as a data registry and as a guide for identification of the experience from female surgeons’ perspective. Details of the author, year of publication, purpose of the study, study design, setting, population, exposure and outcomes were included in the data extraction form. Study design was categorised as quantitative or qualitative, but the original study sometimes mixed both methods. Study population was only selected to the specialties relevant to the review. Data were categorised into organisational barriers and facilitators within the career progression. Every outcome was also categorised using sub-themes.
Thematic analysis was used to identify key themes from the selected articles. We began with repeated reading of data extracted from the papers. This process helped us to identify recurrence themes related to organisational barriers to and facilitators for women's career progression in surgery. From these themes, we iteratively developed final themes that helped us to examine the phenomena we studied. 17
Both authors participated in thematic analysis. The first author independently developed themes and discussed them with the second author. Through this discussion more themes began to emerge and some initial themes were abandoned. This iterative process was repeated until the final themes were able to sufficiently identify and explain organisational barriers to and facilitators for female surgeons’ career progression. Any discrepancies were discussed by both authors and resolved by consensus.
Results
Twelve peer-reviewed journal articles were included in the study. Two studies focused on barriers to career progression,18,19 one investigated ways of facilitating career progression 20 and two explored both subjects.21,22 Six studies focused on job satisfaction; among these, three studies also suggested barriers22–24 and two discussed facilitators for career advancement.25,26 The remaining two studies in this category described the reason why female surgeons experienced or did not experience job satisfaction.27,28 Five studies were conducted in the United Kingdom, six in the United States and one in Canada. Five studies were quantitative, three were qualitative and four used mixed methods.
Summary of articles reviewed.

Organisational barriers to career progression
Organisational culture
The organisational culture focuses on the values, beliefs and expectations that organisational members come to share. As a result, the organisational culture influences behaviour patterns of professionals who work in healthcare organisations. 30 It has been argued that organisational culture is one of the key barriers which form the ‘glass ceiling’ that hinder women’s career progression. 31
Organisational culture as organisational barrier.
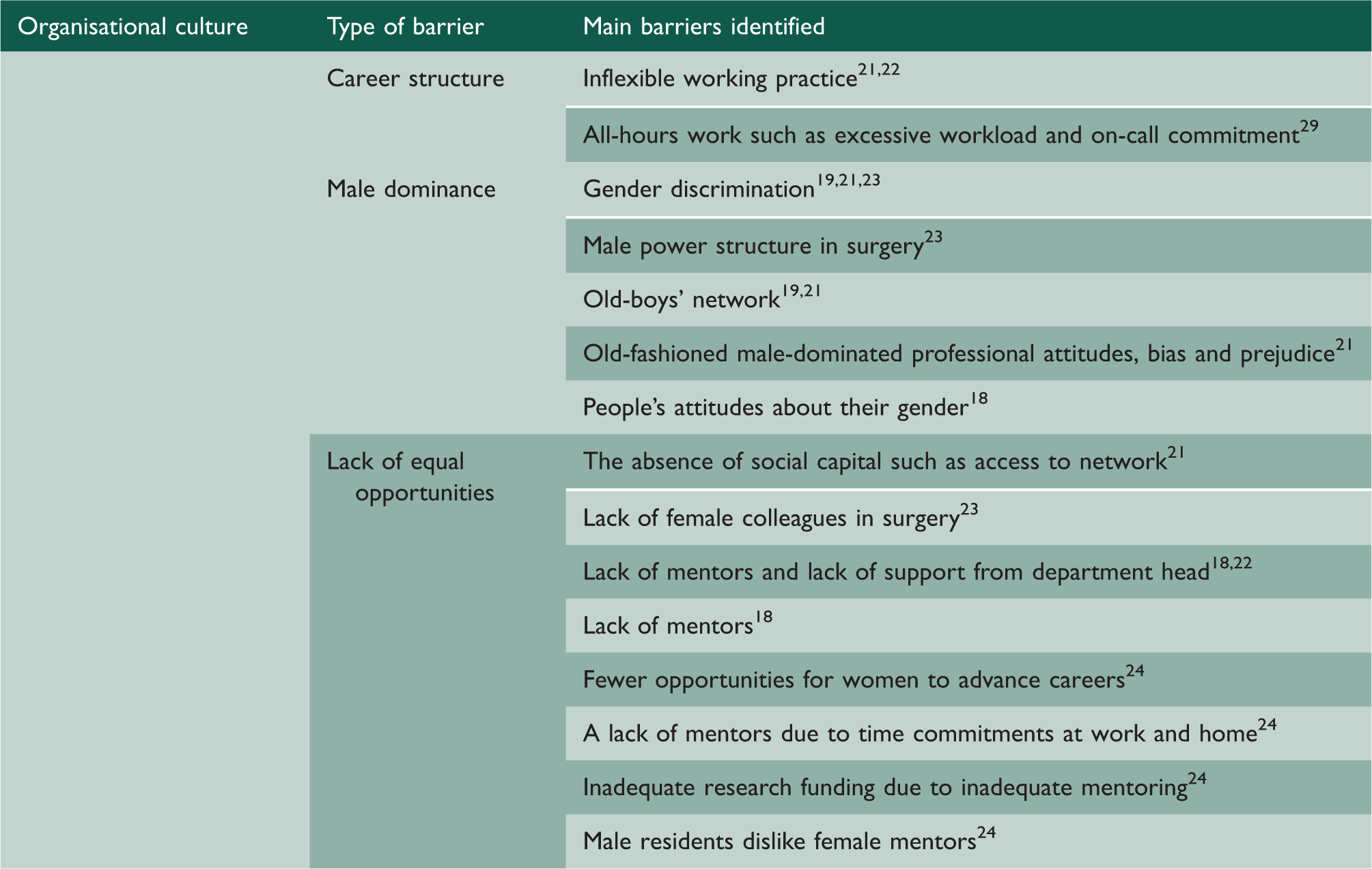
In our review, two studies found that rigidity of career structure requirements, such as all hours work, insufficient research time, and inflexible work practices, presented a barrier hindering career progression.21,22 One 40-year-old female doctor noted that it would be difficult to alter the current career structure in surgery: ‘You can’t have part-time trainees in surgery, you just can’t! It’s a 24 hour job’. 29
Four studies in the review indicated the impact of male dominance in surgical specialties. Female surgeons reported having encountered gender discrimination in the form of being treated differently; receiving negative comments about their gender; 18 and experiencing demeaning remarks, abusive behaviour, or bullying. 23 Studies revealed experiences of old-fashioned male professional attitudes, the ongoing prevalence of bias and prejudice in traditionally masculine fields, 21 and a sense of entitlement that allows men to feel superior to women. 23 Therefore, females felt excluded from the dominant culture in surgery departments, and negative male attitudes and consequent exclusion from the ‘old-boy network’ inhibited the career aspirations of female surgeons.18,19 For example, a cardiac surgeon at a university hospital stated that she stumbled blocks every steps of the way, and the same biases she encountered still exist today. 23 This implies that those who indicated the existence of gender discrimination believed that men and women did not have equal opportunities for career progression in the surgical field. 21
Furthermore, five studies in our review indicated that the absence of forms of social capital, such as access to social networks and collegial support, constituted a barrier to females’ career progression.21,23 In particular, a lack of female mentors and a lack of support from department heads were cited as causing females to have fewer opportunities for career advancement than their male peers.18,22 For instance, one woman seeking to become the chair of a surgical department stated ‘Being a chair requires political tact and connection to a network of supporters … Women don’t often have the chance to show their political skills and lack the network of supporters their male colleagues have.’ 23 Additionally, female surgeons claimed that few female mentors were available due to their time commitments at work and home and that male residents disliked female mentors. Consequently, female surgeons indicated that this inadequate mentoring negatively affected their pursuit of research funding. 23 According to Longo and Straehley, 23 one reason why young female doctors are not encouraged to pursue careers in surgery is that they lack a mentor during their formative years.
Work–family conflict
Work–family conflict refers to the impact of personal lives in the workplace. Work–family conflict has been explained as a form of inter-role conflict in which role pressures from the work and family domains are mutually incompatible. In other words, work–family conflict arises when family responsibilities hamper work activities. 32
Work–family conflict as organisational barriers and reasons of dissatisfaction with job.
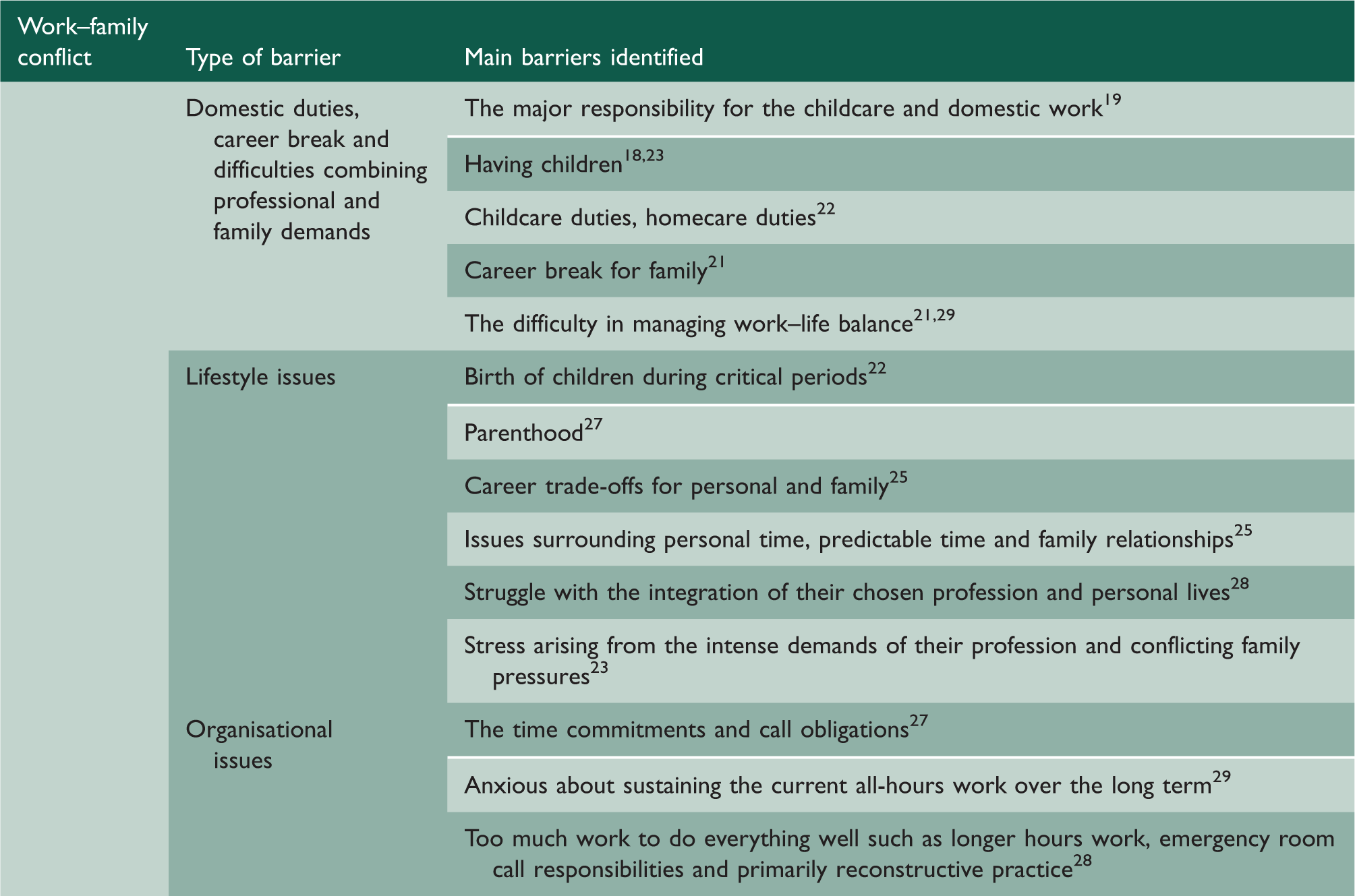
One study found that all female participants were responsible for the majority of housework and childcare, 19 and female doctors expressed the view that having children and domestic duties were barriers to their professional development.18,22 For example, an assistant professor and director of a university surgical residency programme had to forgo the tenure track because of the difficulty in meeting both the work requirements and family commitments. She stated that having two children in a two-year period had clearly affected her academic and clinical productivity, illustrating how family concerns slowed the progress of married women’s careers. 23
Most female doctors believed that having a family would harm their careers because the masculine-oriented career structure poses a major problem for working women who also have caregiving responsibilities. One cardiac surgeon insisted ‘Women are not treated equally. We cannot have children during training. The strong women finish, but it is difficult and involves great sacrifice.’ 23
On the other hand, most women in surgical specialties were satisfied with their specialty choice and their careers. For instance, female colorectal surgeons were happy with the clinical cases they saw 24 and 80% of female general surgeons were satisfied with their career choice. 26 However, most female surgeons had experienced significant stress arising from the intense demands of their profession and conflicting family pressures. 23 For example, Streu et al. 28 reported that female plastic surgeons felt that they had too much work to do and that they struggled with time management of both career and personal responsibilities. This view resonates in several studies (Table 3). Nevertheless, female surgeons enjoyed their jobs, but they were not satisfied with their work–life balance because of the lifestyle sacrifices they must make. A middle-aged female surgeon confessed, ‘I am working really hard now but I cannot possible carry on like this for much longer. I come at 8 in the morning and always leave late. I will always work evenings and weekends.’ 29
Organisational facilitators of a successful career progression
Professional support
Organisational facilitators.
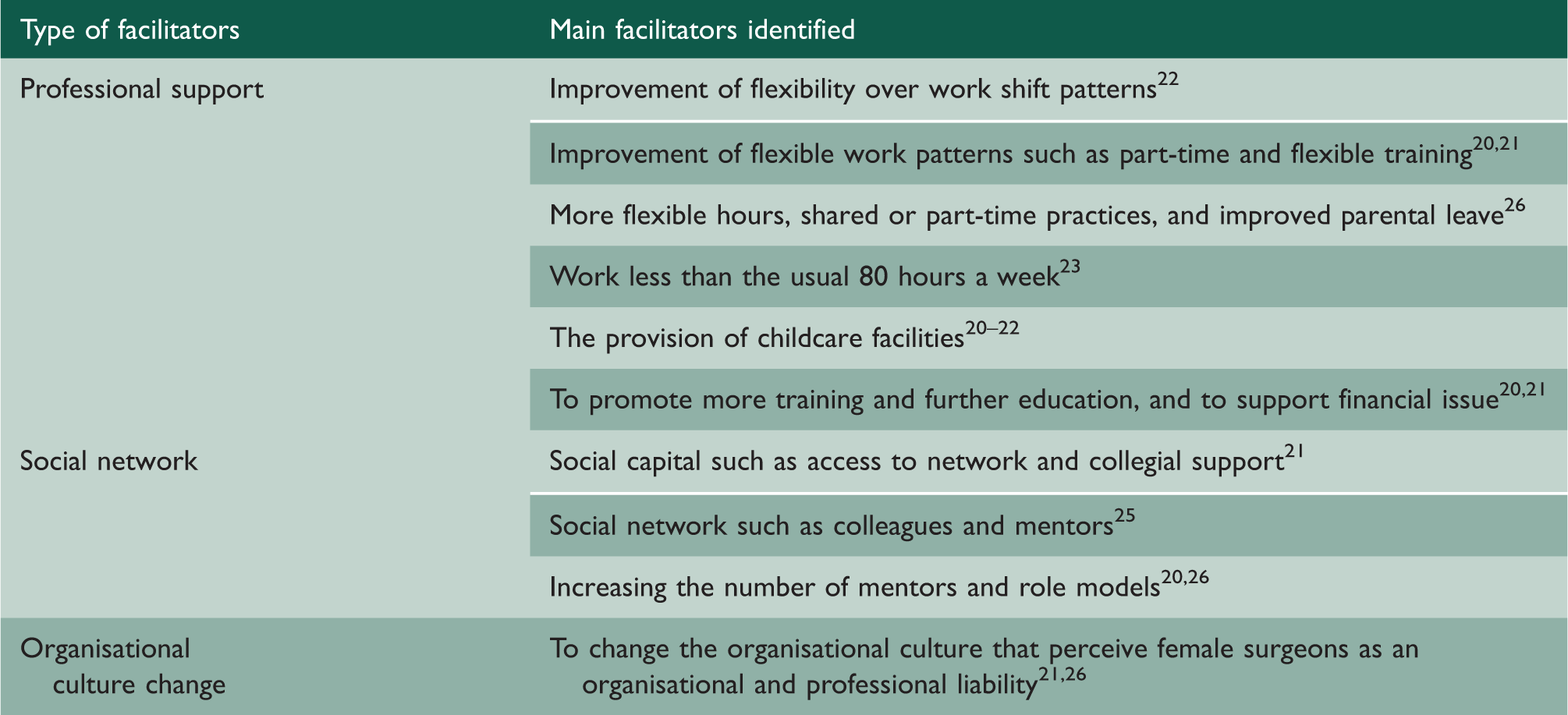
Furthermore, Smith et al. 22 reported that greater flexibility with regard to work shifts was a factor enhancing female paediatric surgeons’ career progression. Hence, the promotion of flexible career structures would keep well-trained female surgeons in the field and would help to attract new candidates. Availability of childcare facilities,20,21,26 promotion of additional training and further education, and adequate financial support20,21 were also identified as important forms of professional support.
Social networks
Social networks were cited as a key to women’s career success in three studies (Table 4). Professional networks, collegial support and mentors are important to developing a successful surgical career, because social networks enable women in male-dominated specialties to share their knowledge and expertise. 25 In particular, mentors can provide social support and appropriate information, and can serve as valuable role models for young doctors.25,26
Organisational culture change
Two studies recommended efforts to change problematic aspects of the organisational culture in surgery. Female general surgeons in studies propose to change the attitudes typical of traditionally male-dominated organisational culture.21,26 For example, many women were discouraged to pursue a surgical specialty at medical school partly because of views held by surgeons that women and surgery do not mix. 21 Some female surgeons suggested changing the organisational culture that stereotypes female doctors as an organisational and professional liability because female surgeons struggle to cope with excessive pressure to ‘do everything’ 21 (Table 4).
Discussion
This systematic review found considerable evidence of organisational barriers that hinder the career progress of female surgeons. It demonstrated that the major factors contributing to the lack of career progression for female surgeons are: (1) an organisational culture which promotes rigid career structure that is inclined to support male surgeons than female surgeons and male domination in which male surgeons feel superior to female surgeons; and (2) work–family conflict whereby women feel that they have to make a family sacrifice by being women and mothers, and the difficulty in securing a work–life balance in the masculine career structure. In addition, many women believed that it is difficult to achieve a work–life balance in higher positions and higher positions lead to more stressful work. 21 Thereby, women frequently do not want to progress in their careers, because they believe that they have to give up their personal life in order to occupy higher positions. As a consequence, these beliefs prevent women from pursuing their careers.
Despite these challenges, most female surgeons are satisfied with their specialty choice and career. They report that they would choose a career in surgery again if they could start over, 27 and they think that surgery is a good career for women. 25 Medical students tend to assume that female surgeons do not enjoy their jobs because of the long work hours and high job demands, but in this instance there is a significant gap between perceptions and reality. Interestingly, female surgeons with families are also satisfied with their jobs, but they have sacrificed their personal lives to pursue professional careers, to the extent that they feel dissatisfied with their ability to parent.25,27 Additionally, female surgeons, whether married or single, are displeased with some of the obligations associated with surgery careers, such as heavy time commitments and on-call duties.25,27 Female surgeons’ job satisfaction is strongly associated with their work–life balance, because they want to work relatively ‘normal’ hours. 1
This implies that healthcare organisations need to pay significant attention to organisational facilitators for female surgeons’ career progression. First, flexible career pathways and work patterns are recommended to retain female surgeons and attract more female medical students. Healthcare organisations need to arrange and implement a variety of different viable career progressions. 34 Second, establishing more family-friendly work conditions to fit domestic responsibilities, especially the provision of adequate childcare facilities, would enable a more satisfactory balance between work and family for all female doctors, not only surgeons.20,35 Third, the promotion of female mentors and role models is suggested to support female surgeons in dealing with their organisational and lifestyle issues. Increasing availability of mentors and role models would contribute to expanding the number of female medical students entering surgical specialties, 7 and the eventual development of richer social networks resulting from the increasing number of female surgeons would further enhance females’ careers.21,25,26 Ultimately, the greater presence of female surgeons would produce meaningful change in the currently male-dominated organisational culture, so that female surgeons would no longer believe that they are restricted by a glass ceiling. At that point, women would have greater opportunities to advance into leadership positions or to achieve the balance that they prefer between productive professional work and their personal lifestyles.
Conclusion
This systematic review has identified and synthesised the main perceived organisational barriers to and facilitators for female surgeons attempting to achieve a successful career progression. The findings described here may be useful for policy-makers and healthcare organisations as they seek to create new career structures for female surgeons and to make the work environment better suited for women.
Nevertheless, the study has some limitation; the studies included in this review lack details about doctors’ personal work patterns, such as whether they were employed part-time or full-time or their personal family contexts. More investigation of the implications of part-time work and other family-friendly work conditions is needed. For instance, Barnett and Gareis 36 found that reducing work hours had increased life satisfaction among married female physicians with children, but Crompton and Lyonette 19 observed that part-time work can be counterproductive to careers by limiting opportunities for promotion to higher positions. 19 Consequently, further research needs to examine the advantages or disadvantages of flexible work patterns, such as part-time employment and job sharing for female surgeons’ career progression.