
Abstract
Objective
The history of treatments for fistula-in-ano can be traced back to ancient times. Current treatment of transphincteric fistulae is controversial, with many options available. We reviewed the history of treatment using cutting setons and present our series of transphincteric fistulae in the light of the series in the literature.
Design
Literature review and case series.
Setting
Hospital based coloproctology service
Participants
140 consecutive patients presenting with fistula-in-ano were included.
Main Outcome Measures
The literature pertaining to treatment of transphincteric fistula was reviewed, along with the outcome of various treatment methods for this condition. Data were collected for 140 consecutive patients presenting with fistula- in-ano were assessed for fistula healing, recurrence and complications.
Results
A total of 140 consecutive patients with fistula-in-ano were identified, of which 111 were cryptoglandular (79.3%). Eighty-one of these 111 were transphincteric (73.0%). At a median follow-up of 35 months (range, 2–83 months), 70 transphincteric fistulae had healed (86.4%), 10 were still undergoing treatment (12.3%) and one patient was lost to follow-up prior to treatment (1.2%). Two patients in this group required a stoma (2.5%), six patients developed recurrence (7.4%); three ‘true’ recurrences (3.7%). One (1.2%) developed a chronic fissure. There were no reported cases of incontinence.
Conclusions
The management of transphincteric fistula-in-ano is complex and controversial, for which no clear surgical procedure has gained acceptance as the gold standard. This study demonstrates that transphincteric fistulae can be successfully treated using cutting setons. A high healing rate (86.4%), low recurrence rate (7.4%) and a low complication rate (3.7%) are shown, which compares favourably with published rates over a long follow-up.
Introduction
Fistula-in-ano is a challenging pathology where treatment attempts have been traced back to the days of Hippocrates (Figure 1).
1
The pathophysiology is still not completely understood and can be complicated further by a variety of other underlying pathological conditions, or through the surgeon embarking on an inappropriate course of treatment.
Hippocrates (460–370 BC). Image credit: Public domain.
Today, the most widely accepted classification system of fistulae is based on the work done by Sir Alan Parks leading to the accepted modified Parks classification (Figure 2)
2
in defining fistula anatomy. In the absence of an underlying condition such as Crohn’s disease or malignancy, most ‘idiopathic’ fistulae are thought to arise from sepsis in the intersphincteric glands as hypothesised by Parks,
3
and are commonly described as ‘cryptoglandular’ in origin.
Diagram of Parks classification of fistula-in-ano image taken from Parks 1976.
2
Type A Intersphincteric, Type B Transphincteric, Type C Suprasphincteric, Type D Extrasphincteric.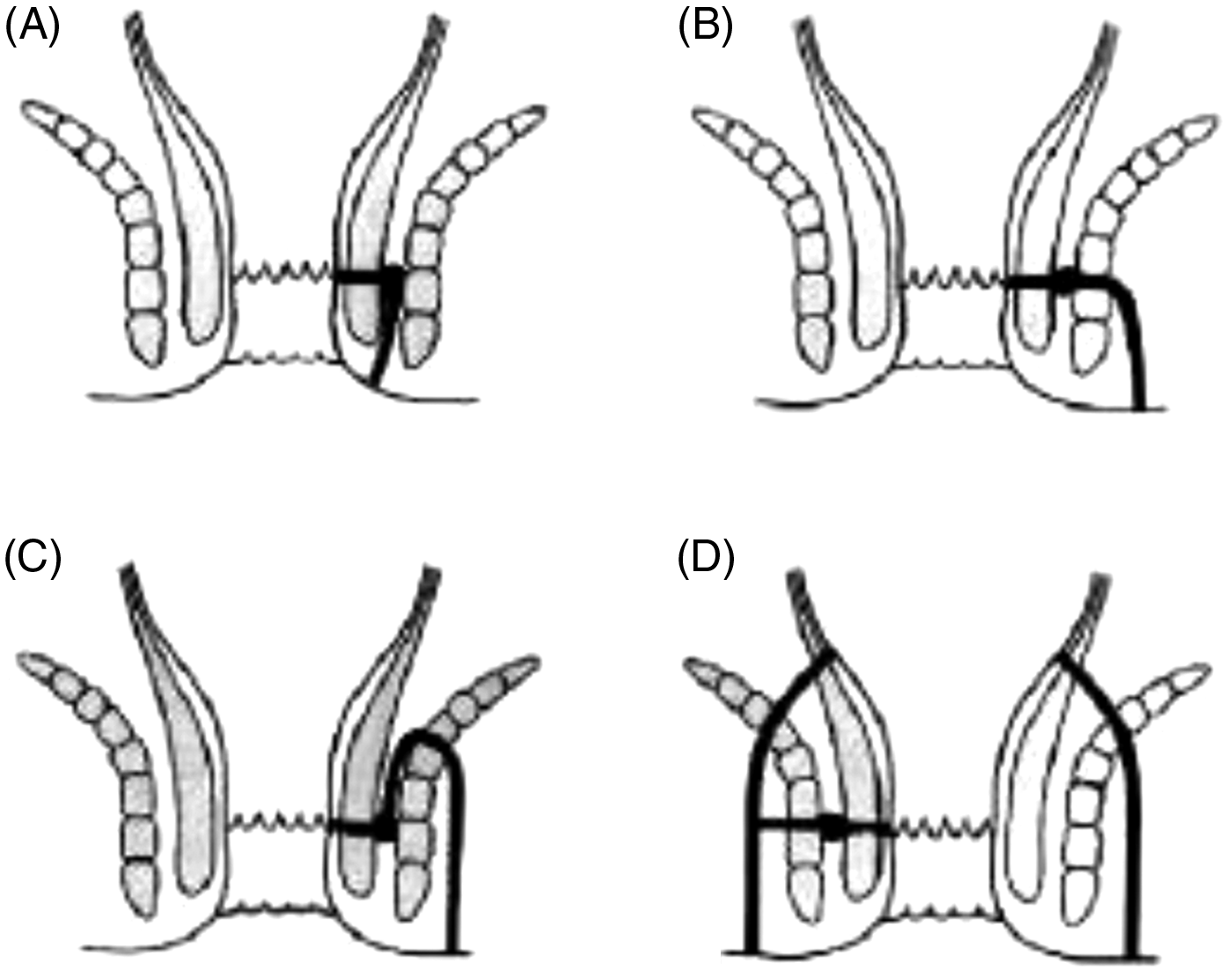
Transphincteric fistulae, which cross the external sphincter, are more challenging to treat. This is due to the need to balance eradication of the fistula with continence preservation.
History documents a wide range of treatments that have been undertaken over the years in an attempt to treat this problem, with no one particular treatment accepted as a gold standard. 4 The documented history of fistula management with cutting setons initially started with Hippocrates, 1 who inserted horsehair with lint into the fistula and, which was periodically tightened.
The Middle Eastern physician Albucasais (936–1013 AD) (Figure 3)
5
as well as the medieval physician John of Ardene (1307–1392 AD) (Figure 4) practised a variety of methods to treat fistulae. Patience was the cornerstone of their treatment; however, they found that their patients often wanted a quick fix to their ailments. The Treaties of Fistulae texts written by Ardene describe seton use for complex fistulae.
5
Today the material may be different
6
but the principle is the same.
‘Abu al-Qasim Khalaf ibn al-Abbas Al-i‘: Known in the West as ‘Albucasis’ (936–1013 AD). Image credit: Peter Paul Rubens/Public Domain. John of Ardene (1307–1392 AD). Image credit: Treatises of fistula in ano, haemorrhoids and clysters 5/public domain.

In 1835, Fredrick Salmon (Figure 5) opened ‘The Infirmary for the Relief of the Poor Afflicted with Fistula and Other Diseases of the Rectum’ following the successful treatment of Charles Dickens. The fistula infirmary became popular and by 1854 the infirmary site was relocated and re-named ‘St Mark’s Hospital for Fistula and other diseases of the Rectum’.
7
Fredrick Salmon (1796–1868 AD). Image credit: George Brown/Public domain.
Sir Lockhart-Mummery summarised the difficulties that surgeons encountered in treating anal fistulae when he said ‘Probably, more surgical reputations have been damaged by the unsuccessful treatment of fistula than by excision of the rectum or gastroenterostomy’ and later went on to state ‘The bad results of laparotomy are generally buried with flowers, while fistulae go about the world exhibiting the unsuccessful results of the treatment’.8,9
More recently, options for treating transphincteric fistulae have included anal advancement flaps, 10 fistula plugs,11,12 fibrin glue and collagen glue. 13 More recently, the Ligation of Intersphincteric Fistula Tract procedure,14,15 and stem cell injections 16 have been introduced.
Proponents of the advancement flap have argued that it produces superior results, resulting in fewer procedures required to treat the condition.17,18 However, it has also been counter argued that it demands more complicated skills and is associated with greater pain, bleeding and potentially more severe complications for the patient. 19
Fistula plugs have been introduced and a UK-based randomised controlled trial FIAT-500 is currently underway comparing the SURGIS® AFP™ anal fistula plugs 20 to alternative fistula treatment of the surgeons’ choice. Current data do not seem to demonstrate any higher efficacy of fistula plug to that of conventional treatment options.20–24
The Ligation of Intersphincteric Fistula Tractprocedure 25 and Modified Ligation of Intersphincteric Fistula Tract 26 Procedure have produced promising results from early studies and will need more long-term evaluation.
The desired outcomes following surgery to treat fistula-in-ano are threefold; the first aim is to get rid of the fistula, second to preserve sphincter function and the third is to prevent recurrence. Published results vary with respect to success of treatment, recurrence, technique used, patient cohort and length of follow-up.6,12–15,17–19 Prognosis is also affected by the complexity of the fistula and any secondary underlying disease that can affect fistula healing. However, treatment is considered successful and complete when the patient is free from fistula, has maintained continence and the fistula does not recur.
Methods
Patients presenting with fistula-in-ano were studied over an 11-year period within two health boards in South East Wales. Data were collected both retrospectively and prospectively during the study period.
Demographic data, fistula anatomy, investigations, treatment course, complications and subsequent follow-up were recorded. Cryptoglandular transphincteric fistulae were included and non-cryptoglandular and non-transphincteric fistulae were excluded from further analysis.
Outcome measures assessed healing, recurrence and complications. All patients were asked about continence to flatus and faeces and to report any soiling when attending clinic and at each subsequent day case visit. A subset of patients was formally continence scored using the Cleveland Clinic Faecal Incontinence Severity Index. 27
All procedures were carried out under general anaesthetic as day case Examination Under Anaesthetics (EUAs), where number 1 nylon cutting seton was hand tied in place. The anoderm from the external opening to the internal opening or dentate line, whichever was lower, was removed along with a Salmon back cut when necessary. This reduced the pain associated with tight seton placement across the sensate epithelium and allowed improved drainage at the external opening, respectively. The suture was subsequently changed and tightened, if necessary, on a six- to eight-week basis, following a re-examination under anaesthetic.
When final EUA demonstrated no residual fistula or sepsis following extrusion or removal of the seton, patients were followed up in clinic at approximately eight weeks to confirm healing.
Results
The series comprised 140 patients presenting with fistula-in-ano, of these 84 were male (60%) and 56 were female (40%). Men presented at a mean age of 44.3 years (range, 17–79 years) and women presented at a mean age of 41.9 years (range, 17–71years). The majority, 111 (79.3%), presented with cryptoglandular fistulae-in-ano. Twenty-nine patients were excluded from further analysis (20.7%); of these 21 (15.0%) were excluded due to a significant underlying pathology, e.g. Crohn’s disease and eight (5.7%) were excluded due to the patient records being unobtainable.
Number of fistulae, aetiology, mean age of presentation and classification of fistulae in series.
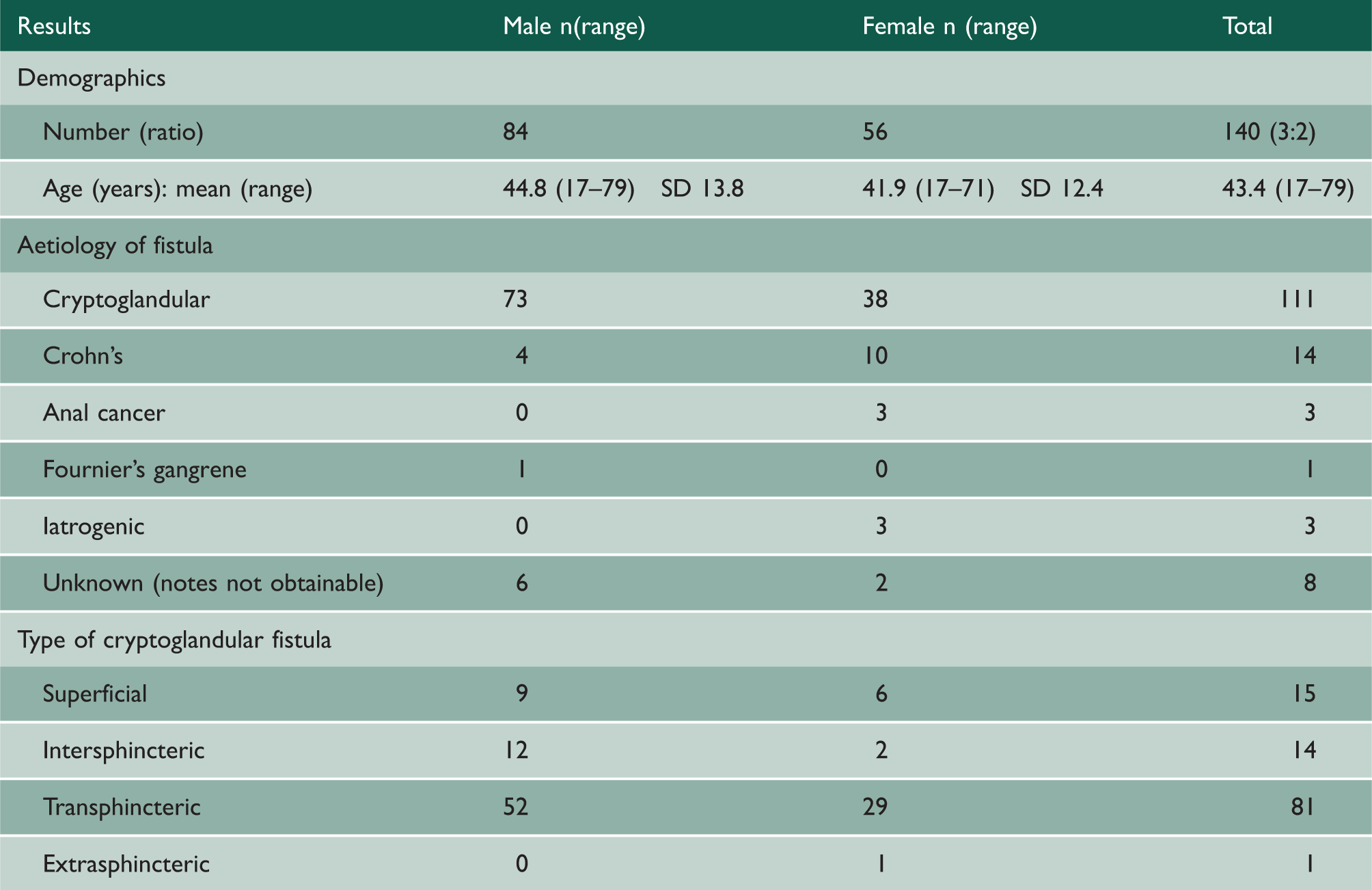
Of the 81 patients with transphincteric fistulae, 29 (35.8%) were women and 52 (64.2%) were men. Seven patients had two fistulae, of which three had two transphincteric fistulae. The remaining four had one transphincteric fistula plus one of either a superficial or intersphincteric fistula.
Magnetic resonance imaging was done in 30 patients (37.0%) during the management of their transphincteric fistula. No patient with cryptoglandular transphincteric fistula underwent endoanal ultrasound.
At the time of writing, 70 of the 81 patients (86.4%) had healed, 10 patients (12.3%) had a seton in situ and were still undergoing treatment and one patient (1.2%) was lost to follow-up prior to receiving treatment (Figure 6). The median number of procedures was four (range, 1–17). Median follow-up time was 35 months (range, 2–83 months) after the fistula had healed.
Number of fistulae healed, number of patients with a seton in situ and number lost to follow-up.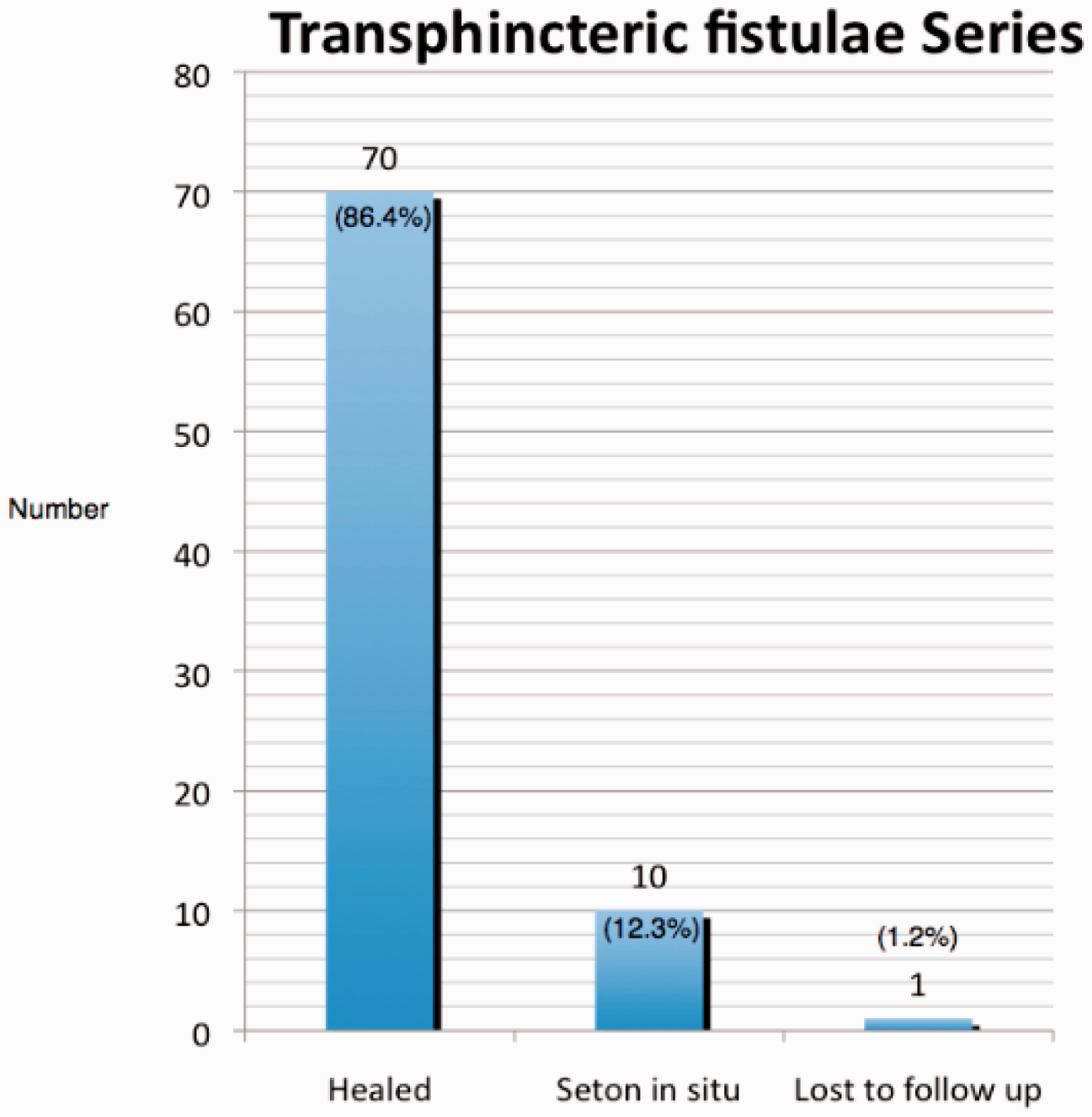
Six patients (7.4%) developed recurrence; three ‘true’ recurrences (3.7%) and three ‘de novo’ fistulae (3.7%). Two (2.5%) patients required a stoma in an attempt to treat their sepsis; one had multiple co-morbidities including poorly controlled diabetes and a high body mass index and the other suffered with severe alcohol dependency. Both of these presented with large transphincteric fistulae and both were poorly compliant with scheduled procedure appointments. One patient (1.2%) developed a chronic fissure post treatment, as a result of a non-healing wound at the 6 o’clock site of the original fistula.
No patient reported a worsening of continence at any clinic or day surgery visit. Eleven patients (13.8%) completed the Cleveland faecal incontinence severity index. 27 Of these, one patient reported an improvement in their continence from preoperative Cleveland Incontinence Score of 3 to Cleveland Incontinence Score 0. One patient reported occasional incontinence of flatus (Cleveland Incontinence Score 1) both pre- and post-procedures. No patient has re-presented with incontinence at hospitals in either of the two South East Wales health boards.
Six (7.4%) patients required one or more of their EUAs at an interval of less than six weeks. This was due to either dislodgement of the previous seton or due to anal pain.
Discussion
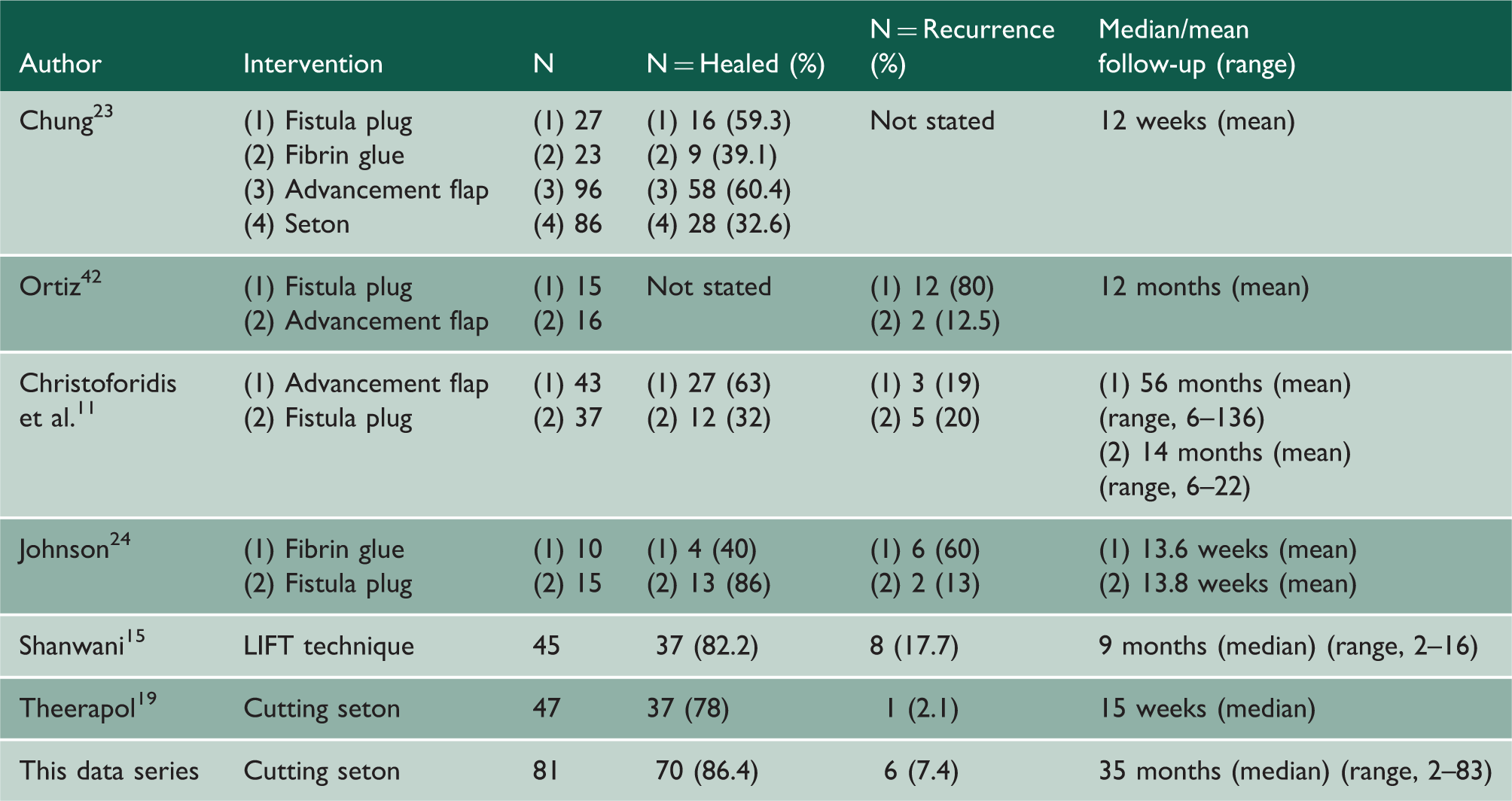
Comparison of series against recent series treating fistulae through a variety of treatment modalities comparing healing rate, recurrence rate and follow-up time.
In line with all these other series, the height of the fistula has not been presented as a separate entity in this report; however, the fact that a seton was inserted into the transphincteric fistula of 81 patients indicates that at the time of first EUA the operating surgeon did not have confidence that any of them were low enough to lay open without risk of incontinence.
Although treatment by cutting seton is a very old method of fistula management and in many centres has been superseded by more modern techniques, this case series suggests that transphincteric anal fistulae can be treated successfully by cutting setons alone. This causes minimal disruption to the pelvic anatomy and preserves continence. The technique fulfils the objectives in anal fistulae management; it defines the anatomy, drains sepsis, eradicates the fistulous track and preserves continence and sphincter integrity. 29 When compared to literature data30,31 this study compares favourably in terms of healing (86.4%) to rates quoted for cutting setons as well as other techniques used in management (Table 2).
A significant duration of follow-up was achieved with a median 35 months (range, 2–83). This is an important aspect in assessing long-term outcome and success of treatment in terms of fistula recurrence and patients re-presenting to the hospital suffering from complications from fistula procedures. Many studies are noted for their relatively short follow-up time following treatment of fistulae and are unable to assess long-term outcome post-surgery. One study was identified as having comparable follow-up times when looking both at advancement flaps and fistula plugs 11 (Table 2).
Several papers suggest that seton use causes a functional defect leading patients to develop changes to continence, particularly to flatus, 32 with some quoted figures greater than 60%. 33 It has also been theorised that defects in the internal sphincter contribute significantly to incontinence to either faeces or flatus.34,35 There is an argument that division of the internal sphincter and eradication of sepsis in the intersphincteric space are important in the treatment of perianal sepsis. 36 However, internal sphincterotomy is not without its own risks, and avoidance of primary internal sphincterotomy may prevent deterioration of continence.37,38 Therefore, for this reason the internal sphincter was not routinely divided, but if a few lower fibres of internal sphincter were still present inside the cutting seton at the time of final EUA, then they were divided with the final skin bridge to remove the seton. We were unable to formally continence score all patients with the Cleveland Incontinence Scoring System, but were able to follow up all patients in clinic and record continence issues in the clinical notes. No patient in this series reported a worsening of continence. This care around sphincter preservation may have contributed to a greater number of EUAs being required, in order to avoid the risk of incontinence.
The large number of EUAs for some patients also reflects the referral practice in this series. Several patients were referred after multiple EUAs, abscess drainages and other attempted treatments in other hospitals. In a few patients the seton fell out unintentionally and thus caused a slight delay in their treatment progression.
The choice of material for the cutting seton was influenced by several considerations. Training at St Marks Hospital where 1-nylon was regularly used provided the initial impetus. Many other materials have also been described. Steel wire 39 is not available in these health boards. Polyfilament, e.g. silk, 40 carries a potentially higher infection risk. Rubber, sialastic sloops or bands 41 have been used by the authors, but mainly as loose setons in acute sepsis or in semi-permanent setons in complex Crohn’s/radiotherapy fistulae. The latter materials have more ‘elasticity’ and so a constant ‘cutting’ action is less predictable than with 1-nylon.
One downside of the use of cutting setons is the cost of repeated EUAs. Although change of seton can be done as an outpatient (office) procedure, many patients find this uncomfortable and prefer general anaesthetic (particularly in a free at the point of use service such as the National Health Service). Commonly used alternative strategies include the fistula plug, which currently have a list price of approximately £580. However, fistula plug use has declined over the last two to three years as surgeons see an increasing number of treatment failures and recurrences. The currently favoured option, the Ligation of Intersphincteric Fistula Tract procedure, also has the potential advantage of a single procedure, without the additional cost of a plug. However, follow-up is only short-term and its long-term success is yet to be determined.14,15
The ideal treatment for transphincteric fistulae would be for a one-off intervention without the attendant costs of repeated procedures. Although some cases series in the literature do contain costings for individual procedures such as the fistula plug, it is difficult to do a formal health economic assessment due to the relatively short follow-up. Although we have not performed a formal health economic assessment ourselves, it is important to consider the relatively low recurrence rate at a median of 35 months.
Conclusions
The ideal surgery for transphincteric fistulae-in-ano management is still not known. Newer advances in technologies have added to the debate and allowed surgeons to explore if indeed, a holy grail to fistula-in-ano management can indeed ever be found. It is a challenging condition, which is likely to continue to plague us.
This relatively large series demonstrates that transphincteric fistulae can be successfully treated by the ancient method of cutting setons. It shows a high healing rate (86.4%), a low recurrence rate (7.4%) and a low complication rate (3.7%) and compares favourably with more modern techniques in the literature (Table 2).