
Abstract
Jejunal diverticulosis is a rare disease which normally presents for the first time with acute complications, often requiring surgical intervention. The diverticulae are acquired, occurring more commonly after middle age, but their aetiology is unclear. We discuss this condition in the context of four cases which presented to our hospital as emergencies over a five year period: small bowel obstruction, gastrointestinal haemorrhage, small bowel volvulus, and visceral perforation. Our aim is to encourage clinicians to include jejunal diverticular disease as a differential diagnosis in patients with abdominal symptoms.
Keywords
Introductory statement
Jejunal diverticulosis is a rare disorder often identified when complications arise, illustrated by the four cases described here.
Case descriptions
Case 1: small bowel obstruction
An 84 year old man presented with a 3 day history of worsening abdominal pain with distension. He had a history of gastric volvulus, hiatus hernia, oesophageal stricture and Parkinson's Disease but was active and independent. On this admission, contrast-enhanced computed tomography (CT) reported small bowel obstruction with a transition point at the mid to distal jejunum. An emergency laparotomy was performed which identified multiple jejunal diverticulae approximately 25 mm in diameter with a strangulated ischaemic segment (Figure 1). Approximately 50 cm of diseased jejunum was resected 15 cm distal to the duodeno-jejunal flexure and the healthy ends were anastomosed. Post-operatively, the patient initially received parenteral nutrition due to a prolonged ileus but restarted oral feeding after 9 days and was discharged home.

Case 1: Jejunal diverticulosis at laparotomy for small bowel obstruction showing multiple diverticulae including a distal ischaemic segment.
Case 2: gastrointestinal haemorrhage
A 55 year old male presented to the Emergency Department with a 3 day history of persistent melaena and haematemesis. He had been taking non-steroidal anti-inflammatory drugs (NSAIDs) for chronic elbow pain. Abdominal examination was unremarkable and his vital signs were stable apart from a mild tachycardia. Initial blood tests showed a raised white cell count (WCC) 18 × 109/L and a haemoglobin (Hb) of 77 g/L, falling to 63 g/L, initiating transfusion. An emergency endoscopy showed erosive duodenitis but no active bleeding. Further melaena, hypotension and haemoglobin drop (108 to 77 × 109/L) led to a bleeding point being identified by CT angiography in the proximal jejunum (Figure 2) so he was transferred to the operating room. An on-table endoscopy revealed fresh blood in the duodenum but no obvious bleeding point. As the patient was unstable, an emergency laparotomy was performed which identified a large jejunal diverticulum 50cm distal to the duodeno-jejunal flexure full of haematoma. An intra-operative endoscopy via a jejunal enterotomy found no other active bleeding point, so a 50cm segment of jejunal diverticulosis was resected with primary anastomosis. The patient's haemoglobin remained stable, he passed normal stool after 24 h and was discharged home. Histology described thin-walled blood vessels at the apex of a jejunal diverticulum as the likely source of bleeding.

Case 2: CT angiogram showing blush of contrast in jejunum (arrowed) as likely site of intestinal haemorrhage.
Case 3: jejunal volvulus
A 70 year old man presented as an emergency with a 3 day history of vomiting, constipation, bloating, leg cramps, and weakness. Previous similar vomiting attacks had been diagnosed as gastro-oesophageal reflux disease (GORD) so he had been prescribed a proton pump inhibitor. An MRI small bowel study later reported a “lax small bowel mesentery probably causing intermittent small bowel volvulus”. On this admission, he had a raised white cell count (WCC 25.3 × 109/L), an acute kidney injury (eGFR 14), and a lactic acidosis (lactate 5.7 mmol/L) which partially resolved (to 2.1 mmol/L) with fluid resuscitation. Non-contrast computed tomography revealed a small bowel volvulus with multiple small areas of pneumoperitoneum in the right upper quadrant, suggesting visceral perforation. The patient underwent an emergency laparoscopy, adhesiolysis and de-rotation of the volvulus, but as found no evidence of perforation so resection was not performed. Three weeks later he was admitted with similar symptoms and a CT with contrast suggested small bowel ischaemia. At laparotomy, there was a recurrent jejunal volvulus containing a large jejunal diverticulum (Figure 3). This time 120 cm of affected small bowel from 60 cm distal to the duodeno-jejunal flexure was resected with primary anastomosis. The patient's post-operative recovery was uneventful and he was discharged home. The histology of the resected specimen showed a granulomatous reaction to foreign material in the jejunal diverticulum but the nature of the material could not be identified.

Case 3: Small bowel volvulus containing large jejunal diverticulum.
Case 4: jejunal perforation
A 79 year old man was admitted as an emergency with a 4 day history of abdominal pain, fever, loose stools and one episode of vomiting. In the Emergency Department, he had a fever of 38°C, a tachycardia of 106 bpm and blood pressure of 116/80mmHg. Inflammatory markers were raised (WCC 14.9 × 109, CRP 335 mg/L), and total bilirubin was raised at 73 micromol/L. The patient was initially diagnosed with cholangitis and given antibiotics, but CT showed thickening of the mid jejunum, with a localised collection, presumed to be a sealed perforation as there was no pneumoperitoneum. As the patient was clinically stable, he was maintained on antibiotic therapy under observation until he was fit for discharge. The patient continued to experience intermittent abdominal symptoms, so an MRI small bowel study was performed, which suggested intussusception due to mid-jejunal diverticular disease. An diagnostic laparoscopy subsequently identified a jejunal diverticulum constricted by an adhesional band and wrapped in omentum suggestive of a previous local perforation (Figure 4). Resection of the affected jejunum with primary anastomosis was performed and the patient recovered.
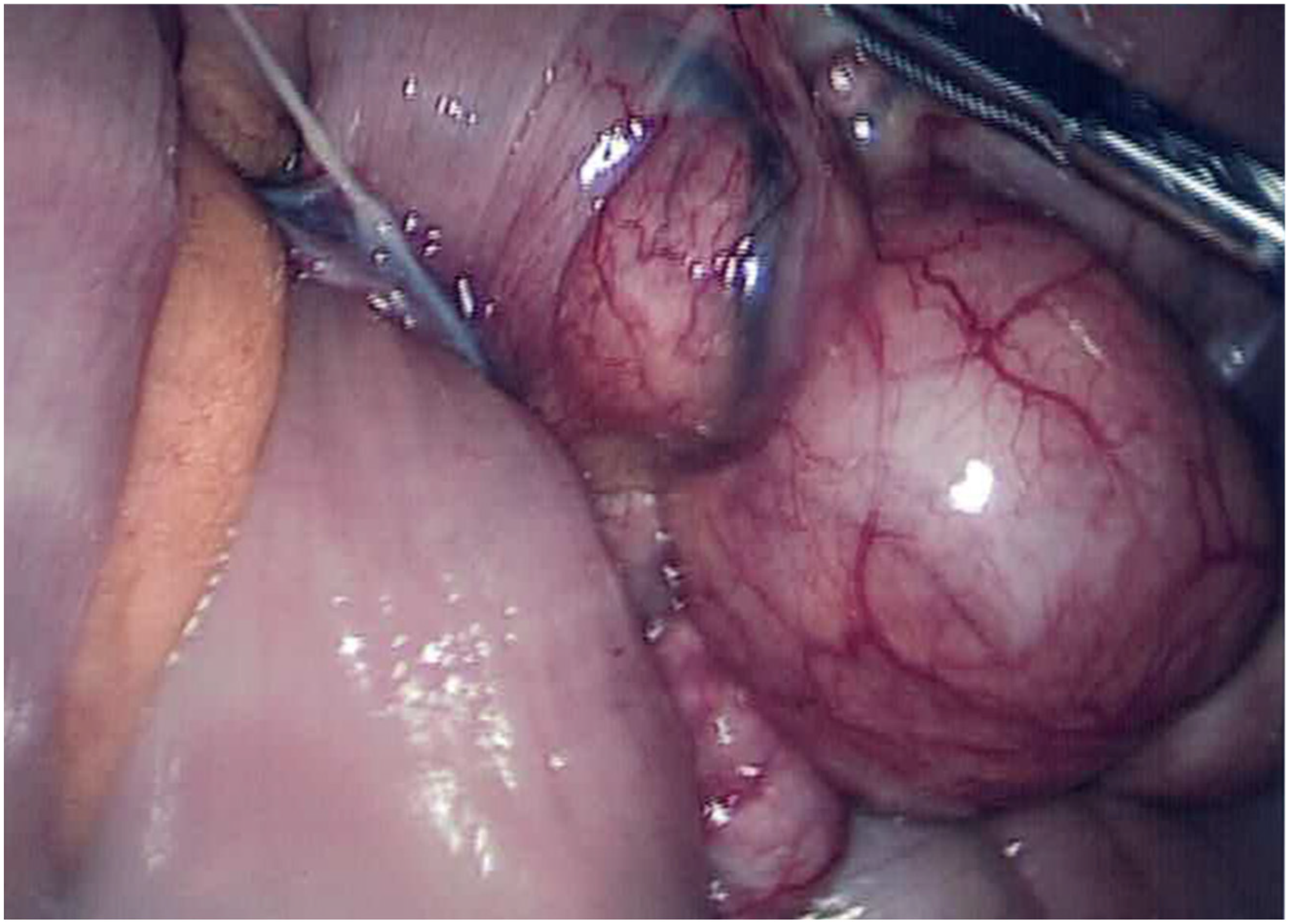
Case 4: Laparoscopic view of band adhesion adjacent to a jejunal diverticulum.
Discussion
Diverticulae of the jejunum and ileum have a reported incidence of 0.5–2.3% 1 with a male predominance as in the cases described here. Jejunal diverticulosis may be found incidentally, but is often identified due to complications. 2 In many cases, there is a history of diffuse abdominal pain, excessive flatulence, bloating or reduced appetite. When jejunal diverticulosis causes symptoms, it is often misdiagnosed, as the interpretation of jejunal diverticulae on standard cross-sectional imaging is challenging and can lead to a delay in diagnosis. 3 Surgical resection of the diseased segment is recommended for treating complications of jejunal diverticulosis, as most patients recover well. 4
The cases described here show different aspects of the pathophysiology of this condition. The diverticulae are pathologically pseudodiverticulae, as they are herniated areas of the mucosal and submucosal layer. 5 Unlike a Meckel's diverticulum, an embryonic remnant, acquired jejunal diverticulosis tends to occur on the mesenteric border of the jejunum and tends to occur as multiple defects. They are thought to be pulsion herniations caused by raised intraluminal pressure or inherent tissue disorders, 6 but there is no evidence that the jejunum is particularly subject to significant pulsion forces, except perhaps in cases of chronic subacute obstruction, so the aetiology remains unknown. The points of weakness may be associated with areas where blood vessels enter the intestinal wall and therefore are associated with sites of haemorrhage. 7 Our case presenting with acute gastrointestinal haemorrhage may have arisen from a weakened blood vessel at the site of jejunal herniation, increasing the risk of rupture. This case presented with life-threatening haemorrhage, but diagnosis and treatment was delayed due to the challenges of identifying jejunal bleeding. The CT angiography here played a crucial role in the decision to proceed to emergency surgery. Unlike diverticulae of the large bowel, jejunal diverticulae tend to be significantly larger than their colonic counterparts. Conceivably, the unbalanced weight of these large diverticulae could lead to jejunal volvulus, 8 as seen in the third case presented here. It is interesting that the histology of the resected specimen showed a granulomatous reaction to foreign material. This may indicate previous inflammation from impacted intra-luminal contents, such as small bones.
Symptomatic jejunal diverticulosis usually presents in the elderly population, as with most of the cases described here. Many patients have a history of non-specific symptoms, such as pain, nausea, vomiting, bloating, diarrhoea or flatulence before they are diagnosed due to complications. 9 In our first case, a combination of previous gastro-oesophageal surgery and jejunal diverticulitis is likely to have generated a band adhesion, eventually strangulating the distal jejunum. In hindsight, the patient's background of non-specific abdominal symptoms that had been attributed to his hiatus hernia may instead have been due to his long segment of jejunal diverticulosis. In a similar way, the fourth case presented here developed strangulation and then perforation of a jejunal diverticulum. He was initially diagnosed with ascending cholangitis, misinterpreting the signs of small bowel perforation. As this local perforation was rapidly sealed by omental wrapping, his acute symptoms partially resolved but further imaging and ongoing obstructive symptoms prompted exploration by laparoscopy and established the correct pathology. Perforation has also been known to cause fistulation 10 but we have not encountered this particular complication.
Diagnosing jejunal diverticulosis remains a challenge, as the common investigations for non-specific gastrointestinal symptoms such as gastroscopy, colonoscopy and computed tomography (CT) rarely detect this pathology. 11 Double-balloon enteroscopy may have a role, especially in gastrointestinal bleeding. 12 Imaging modalities recommended in the literature include small bowel oral contrast studies and MRI enteroclysis. 3 As CT is unreliable, it has been suggested that the role of CT in these cases is to rule out other diagnoses, rather than confirm jejunal diverticulosis. Our cases support the idea that, despite imaging, the exact pathology associated with jejunal diverticulosis may only be confirmed by direct visualisation of the affected segment of the bowel during laparoscopic or open surgery.
In conclusion, while diverticular disease of the jejunum is rare, an awareness of the condition is important, as acute complications often require emergency surgery and some, such as acute haemorrhage, can be life threatening. While conservative management may work temporarily, we would recommend surgical management of complicated or symptomatic jejunal diverticulosis with resection and primary anastomosis, either electively or in the acute setting.
Footnotes
Statement of authors
The authors declare no conflicts of interest. Written permission to publish was obtained from patients, to whom we are extremely grateful. No funding or sponsorship was obtained.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.