
Abstract
Objective
To determine if applying change analysis to the narrative reports made by reviewers of hospital deaths increases the utility of this information in the systematic analysis of patient harm.
Design
Qualitative analysis of causes and contributory factors underlying patient harm in 52 case narratives linked to preventable deaths derived from a retrospective case record review of 1000 deaths in acute National Health Service Trusts in 2009.
Participants
52 preventable hospital deaths.
Setting
England.
Main outcome measures
The nature of problems in care and contributory factors underlying avoidable deaths in hospital.
Results
The change analysis approach enabled explicit characterisation of multiple problems in care, both across the admission and also at the boundary between primary and secondary care, and illuminated how these problems accumulate to cause harm. It demonstrated links between problems and underlying contributory factors and highlighted other threats to quality of care such as standards of end of life management. The method was straightforward to apply to multiple records and achieved good inter-rater reliability.
Conclusion
Analysis of case narratives using change analysis provided a richer picture of healthcare-related harm than the traditional approach, unpacking the nature of the problems, particularly by delineating omissions from acts of commission, thus facilitating more tailored responses to patient harm.
Introduction
Over the last decade, there has been a movement towards developing a more systematic understanding of causes of hospital mortality as part of a range of approaches that can be used to identify preventable harm, and so focus improvement efforts. 1 Mortality has been the focus of attention of clinicians, the public and politicians following the well-publicised investigations at Bristol Royal Infirmary and Mid Staffordshire National Health Service (NHS) Foundation Trust, both prompted by standardised hospital death rates found to be outside the expected range.2,3 The Modernisation Agency, 4 and subsequently the NHS Institute for Innovation and Improvement, 5 drawing upon the work of the US Institute for Healthcare Improvement, 6 have advocated the use of retrospective case record review (RCRR) for this purpose. The approach is also recommended by NHS national safety campaigns in both England and Wales.7,8
RCRR can either be explicit (whereby healthcare professionals assess the quality of processes of care using a set of predetermined criteria) or implicit, allowing clinicians to make judgements using their knowledge and experience. Enhancements to the latter, such as the use of a structured review form and formal training, have been introduced over time in an effort to increase its reliability. Within the research sphere, RCRR, both implicit and explicit, has usually been orientated towards quantitative analyses of the prevalence of patient harm, and its underlying causes or the percentage of patients in which a particular process was satisfactorily undertaken. However, it has been recognised that preventable deaths are often a consequence of the interplay between factors and that omissions in care play an important role especially in frail elderly patients whose defences against such insults are not as robust as those of younger, fitter patients. 9 Although the traditional RCRR method does involve delineating the nature of adverse events and contributory factors, usually captured as lists, this may not capture the complexity of how harm arises. Approaches that can capture the complexity of threats to patient safety can augment traditional RCRR.
RCRR has benefitted from the introduction of methods of incident analysis, derived from James Reason’s organisational accident model, and this can highlight both the chains of small events at the clinician/patient interface and wider organisational factors.10–12 These approaches involve in-depth analysis of patient harm and aim to discover root causes. Such tools might be usefully applied to the narrative reports made by reviewers of hospital deaths to increase the utility of this information in the systematic analysis of patient harm.
A large RCRR of 1000 deaths in acute hospitals has recently been conducted to provide a robust estimate of the proportion of preventable deaths in England. This has provided the opportunity to test the use of narrative reports and what they might contribute to traditional case record review.
Method
Details of an RCRR of 1000 hospital deaths in 2009 in 10 randomly selected acute hospitals have been described elsewhere. 13 The method was based on previous similar studies.14–18 The reviews were undertaken by 17 recently retired physicians, all of whom had extensive experience as generalists, supported by training and expert reviewer advice. For each case, in addition to a structured set of questions, reviewers were asked to provide a brief narrative account (up to one A4 page) of the circumstances.
The narrative accounts from the 52 deaths judged preventable were transcribed from the review form. Of the range of root cause analysis tools available for qualitative analysis of causes and contributory factors underlying harm, we chose ‘change analysis’ as the most suitable tool. The approach enabled specification and categorisation of problems in care within the narratives using a constant comparison approach between theoretical ‘problem free’ care and what actually happened in practice. The categories were based on those developed by Woloshynowych et al. 19 In addition, the Contributory Factor Classification Framework (developed by Charles Vincent and colleagues) was used to categorise contributory factors into nine major groups: patient, staff, task, communication, equipment, work environment, organisational, education and training, and team. Underlying subcategories were also used. 12
The method was applied to five cases by two independent reviewers (HH and FH). They then discussed any discrepancies in their findings and made adjustments to the process before all 52 cases were reviewed by HH. One-third of cases were also reviewed by FH to test inter-rater reliability. Reviewers agreed on problems in care in 71% of cases (Kappa coefficient = 0.64 indicating substantial agreement) and on contributory factors in 64% (Kappa coefficient = 0.56 indicating moderate agreement).
The problems in care and contributory factors coded under each of the categories and subcategories were summed to give an indication of relative distributions.
Results
Identifying multiple problems in care
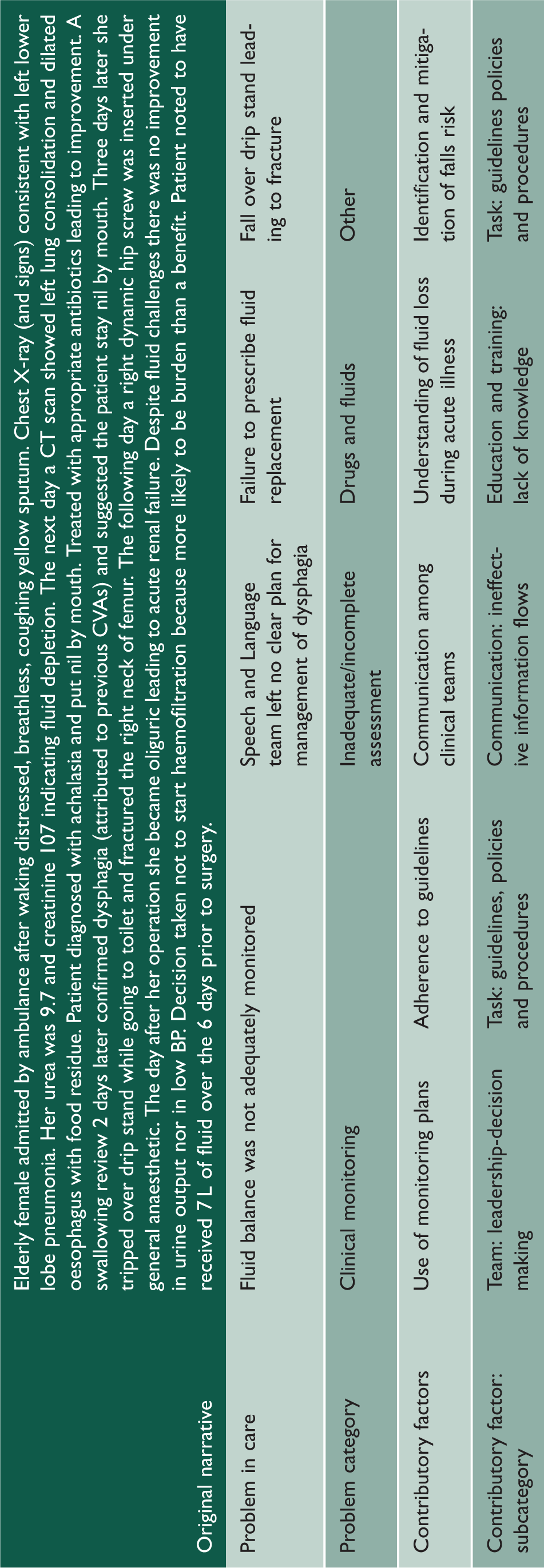
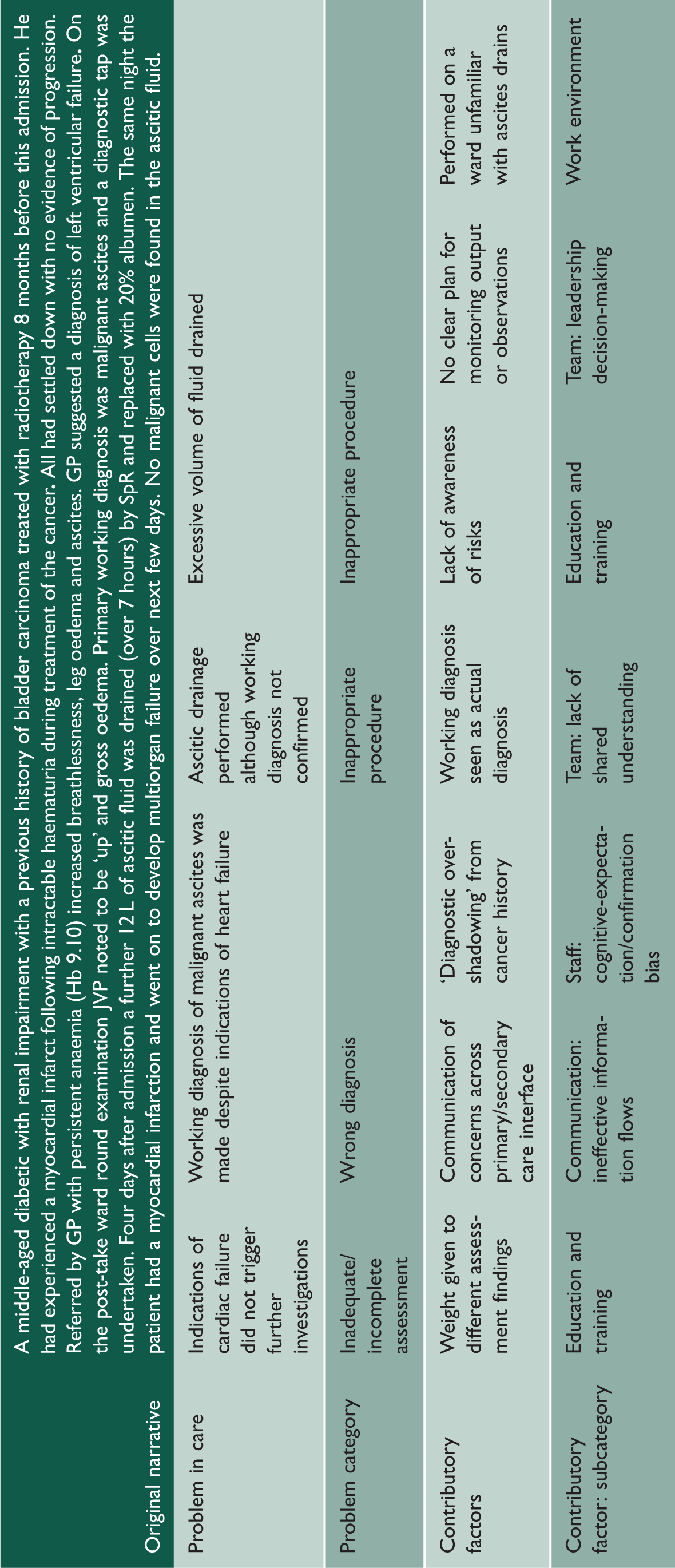
Using the process of change analysis enabled multiple problems in care that cluster in broad categories to be identified, thus defining the nature of the problem more precisely, particularly delineating omissions from acts of commission.
Case 1.
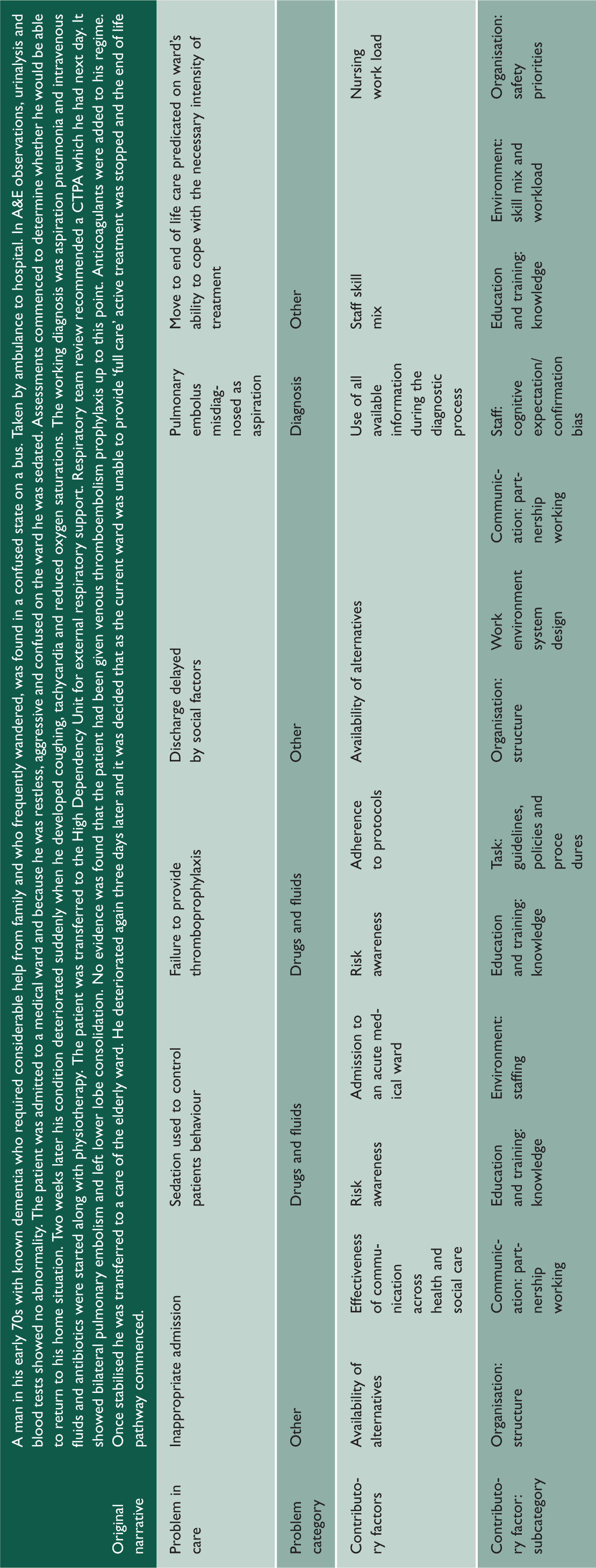
Identifying problems in care across the admission
Case 2.
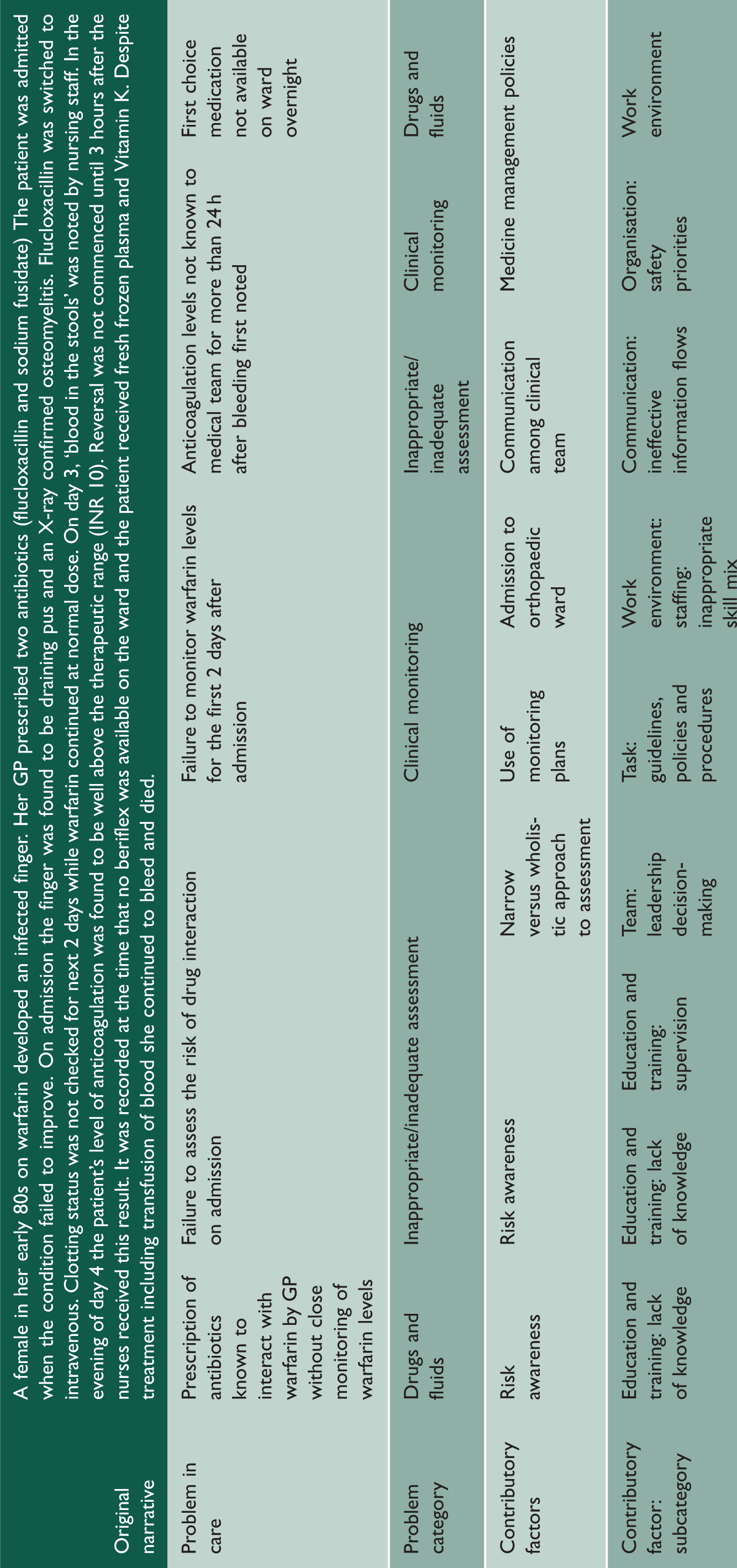
Case 3.
Nature of problems in care and contributory factors
Analysing the narrative accounts led to an average of three (range, 1–8) problems in care associated with preventable death per case being identified with over 70% of these being related to omissions in care. Figure 1 shows how the distribution of problem subcategories differed between medical and surgical patients. For instance, issues with laboratory tests accounted for a larger proportion of clinical monitoring problems in medical patients than surgical patients, while drug omissions formed a larger proportion of drug and fluid problems in surgical than in medical patients.
Pie charts showing the distribution of problem in care subtypes across medical and surgical preventable deaths.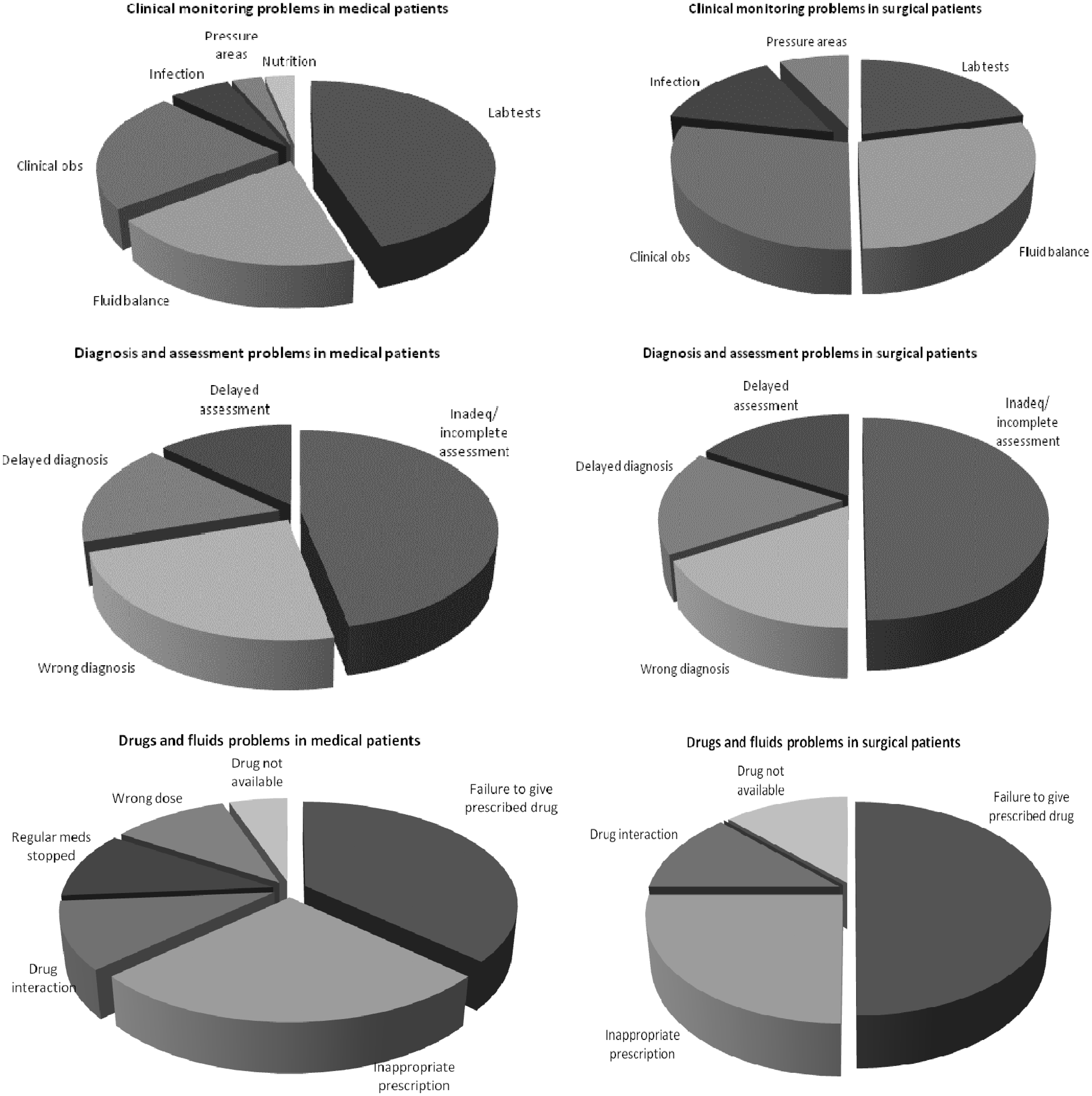
An average of five (range, 1–10) contributory factors were identified per patient (Figure 2) with subtypes differing across the different problem categories.
Pie charts showing the distribution of contributory factors across different categories of problems in care.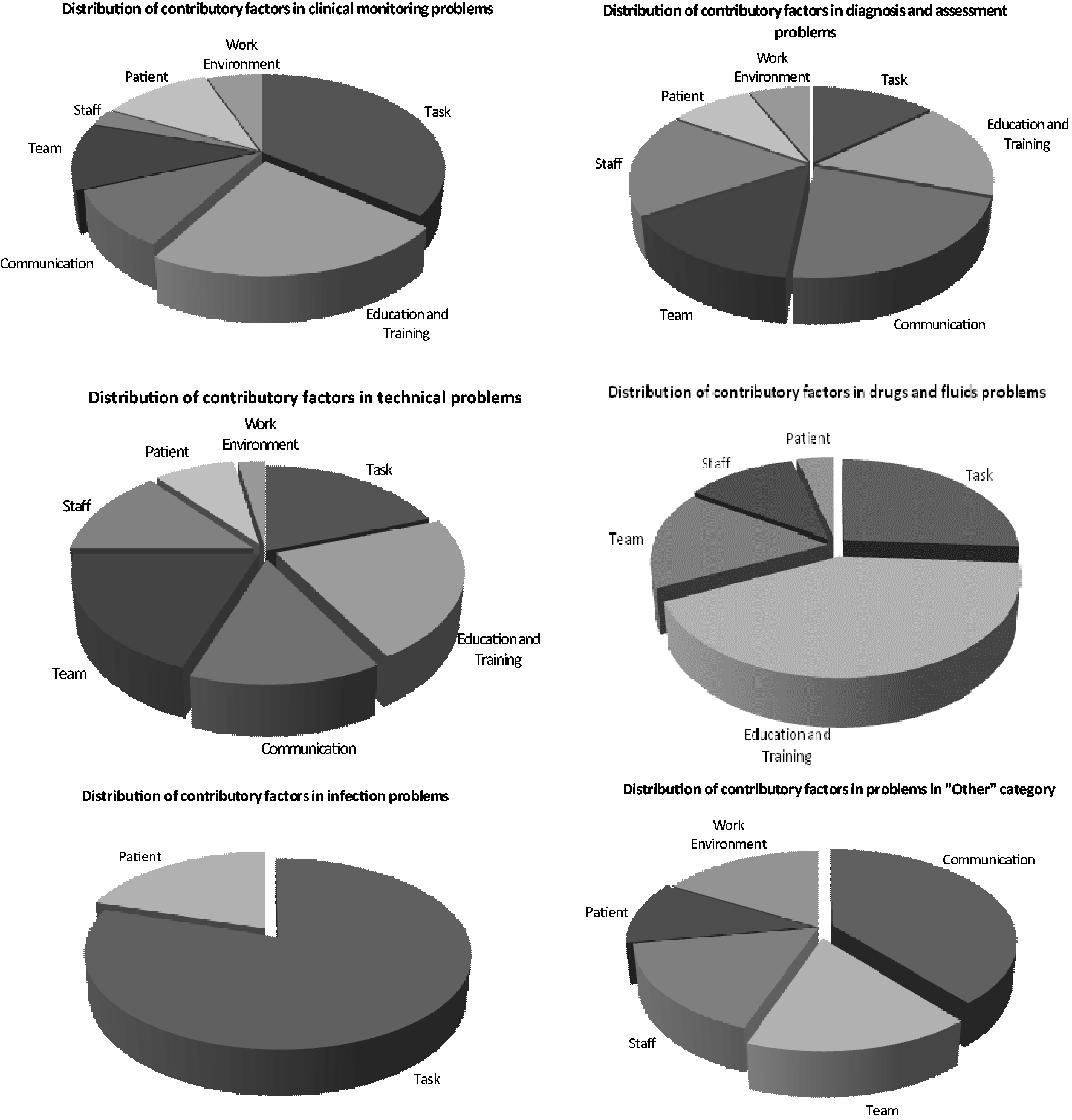
Discussion
Principal findings and interpretation
Change analysis, a tool developed for root cause analysis, was used to mine case narratives from previous case record-based mortality review to provide a richer picture of the nature of harm associated with preventable deaths than traditional RCRR approaches. The approach was feasible for use on the relatively short narratives that accompany mortality reviews and was time efficient (15–20 min per case). It was sufficiently robust in identifying problems and contributory factors, with good inter-rater reliability.
Change analysis identified multiple components underlying single problems, the balance between acts of omission and commission and the interplay between contributory factors. The nature of harm generation across the admission and at the interface between healthcare providers could be gauged. The collation of findings from the analysis can be used to demonstrate how distributions of problems and their contributory factors vary across different patient groups.
We found that problems generated when processes of care go wrong accumulated across admissions. Most commonly, problems related to clinical monitoring, to assessment and diagnosis, and to drugs and fluid problems combined and led to preventable deaths. Contributory factors shed light on the issues underlying these problems in care and varied in distribution according to problem subcategories.
Strengths and limitations
Examining the narratives of deaths judged to be preventable allowed a deeper understanding of the nature of problems in care underlying such deaths and was particularly good at identifying multiple omissions across the care pathway. There are, however, three potential limitations. First, the narratives were short, ranging from one paragraph to one sheet of A4. Missing details are likely to have led to a failure to identify some problems and their contributory factors. Even with the availability of the full admission record, it is unlikely that retrospective review can find the full spectrum of hospital-related patient harm.
Second, clinicians are more likely to record clinical details than factors related to organisational policies and processes; therefore, reviews of records are more likely to identify clinical–technical aspects of care, especially those related to human error, rather than system-wide issues.20,21 For the same reasons, contributory factors are often not explicitly recorded and factors such as a lack of knowledge have to be inferred from the nature of the problem itself. And third, we knew we were reviewing narratives of patients who had experienced a preventable death and such hindsight bias may have led us to identifying problems, even if the evidence for these was scant.
Implications and conclusions
As the majority of patients who die in acute hospitals are elderly and frail with multiple co-morbidities, hospital death reviews provide a window on how well healthcare is delivered to those with complex conditions. Their care tests the safety of hospital systems, with fragmented and poorly coordinated care increasing the opportunity for omissions and ensuing harm, especially in those with fragile health states. 3 Our findings confirm those from previous large RCRR studies, both in the predominance of omissions as a major factor in serious harm and the nature of the problems in care underpinning preventable deaths.15,18,22 Our findings are also consistent with the work of James Reason, who showed how system-level factors such as poor communication, team work or task design enable problems at the patient–clinician interface to occur.
Mortality reviews can highlight key areas of risk thus allowing more focused targeting of actions to reduce these risks. Such reviews, based on retrospective review of medical records are increasingly used as a quality and safety improvement tool in NHS hospitals. Some hospitals in England are reviewing all deaths, while others are using samples derived in a variety of ways. As increasing proportions of deaths undergo review, it is important to consider how to maximise the potential for learning. Categorisation of problems using traditional RCRR does not provide a sufficiently precise picture of the nature of the problems within in any given category, how these problems link together and how they are associated with specific contributory factors. While useful for monitoring trends over time, the information generated has limited value for understanding the complex nature of harm evolution and the influence of multiple interacting contributory factors. Although root cause analysis was developed for this purpose, such an in-depth multidisciplinary approach is not feasible for assessing large numbers of cases.
Applying change analysis to case narratives identifies the scope of problems in care and their linked contributory factors across the admission, offering the opportunity to identify high-risk areas and better targeting of appropriate interventions. Drawing as precise a picture as possible of the nature of harm makes mortality review a powerful tool for improving quality, especially if this information can be efficiently gathered across multiple cases. Further research will be required to determine the acceptability of this approach among NHS staff undertaking mortality reviews and to determine the impact of the analyses on quality and safety improvement. Given that problems in care span initial assessment through to complex treatment, resulting improvements have the potential to provide safer environments for all patients.