
Abstract
The aim of this article was to explore whether expectant parents’ attitudes to termination or continuation of pregnancy, both in general and in case of fetal abnormality, are affected by previous experiences of miscarriage and whether attitudes change after ultrasound screening with normal findings. It was also of interest to investigate differences in attitudes in relation to age, parity and gender. A prospective one-year cohort study was carried out. Questionnaires were administered before and after the ultrasound examination. Analyses included 1258 women and 925 men. A comparison between the results pre- and post-ultrasound showed that after the ultrasound examination, there were significant changes towards a more positive attitude to give birth to a baby with an abnormality. Men were significantly more willing to terminate for a fetal abnormality and significantly less hesitant towards abortion in general than women. Women aged 35 years or older were significantly less willing to give birth to a baby with an abnormality and significantly more positive to termination for fetal abnormality than younger women. Parents showed understanding attitudes towards other parents’ decisions no matter what these were. We conclude that parents need individualized information and support in connection with prenatal diagnosis, due to parental hesitancy. Midwives play an important role in this.
Introduction
For many women and their partners an ultrasound examination is a part of normal pregnancy. A second trimester ultrasound is offered to all pregnant women as a general screening in Sweden, and it is normally performed around week 18 of pregnancy by a specially trained midwife. The purpose of the examination is for establishing fetal viability, dating, detecting the number of fetuses and identifying the location of the placenta. The examination also aims to diagnose certain malformations. If a malformation is detected, a doctor is consulted. Other ultrasound examinations, for example a combined ultrasound examination (for nuchal translucency) and biochemical markers (CUB), are also available, but health trusts differ in their routines. 1
It is generally midwives in antenatal care who inform parents about the screening program. If an abnormality is diagnosed, the parents have to decide whether or not they want to continue the pregnancy, and in Sweden abortion is a possible choice for women until the end of week 18 of pregnancy. After pregnancy week 18 the woman has to apply to The National Board of Health and Welfare for permission to terminate the pregnancy. Such authorization may be granted only if there are exceptional reasons for abortion. 2 Several studies have been published3–6 concerning parents’ decision-making processes when prenatal diagnosis has shown an adverse finding, but less is known about both parents’ pre-scan attitudes and their attitudes towards other people’s decisions. The Swedish National Council on Medical-Ethics (SMER) 7 states that women’s autonomy is limited by the framework established by society and that this framework should be based on an ethical analysis, continuing follow-up on fetal diagnosis and debate within society. Whether a screening program is perceived as discriminatory or not depends on how it is presented and implemented. 8 Another subject, discussed by De Jong et al. 8 is the importance of informed decisions. They claim that these issues rather than abortion rates ought to be taken as a measure of the success of prenatal screening programs.
Attitudes about whether to abort or to continue pregnancy can differ depending on the type and severity of the diagnosis.6,9–11 Leung et al. 9 showed that among 120 interviewed women, 90% would choose termination in case of chromosomal abnormalities but only 50% would choose termination for fetal abnormalities not associated with mental retardation. In a questionnaire study of parents-to-be who attended for nuchal translucency screening (NT), when presented with the scenario that the child’s intellectual ability would be affected, 49.8% would have the baby, only 6.2% chose the alternative ‘end the pregnancy’ and 41.6% chose ‘undecided’. 11 Studies have shown that religious beliefs are associated with negative attitudes to abortion9,12,13 and reluctance to undergo prenatal screening tests. 14 Garcia et al. 14 interviewed 59 pregnant women concerning ethical beliefs and decision-making after being confronted with a test offer. They showed that all the respondents agreed that ‘unconditional acceptance of children is the most praiseworthy approach’ but also that the right to life for the unborn child was context related, subordinate to the quality of life of the child and to the well-being of the family.
If a prenatal screening test has given an adverse diagnosis, the parents’ decision also depends on their perception of the quality of life of the child5,15 as well as legal and cultural factors.16,17 It was shown in a cross-sectional study 17 that pregnant women’s preferences for prenatal testing are related to their underlying attitudes about pregnancy loss and Down syndrome, rather than to their age, when measured in an unselected group before gestational week 20. Redlinger-Grosse et al. 12 have shown that parents appreciated non-directional information from health care professionals prior to their decision about continuation of pregnancy after their fetus was diagnosed with holoprosencephaly.
In some studies,10,18 women were found to have a more positive attitude to termination for fetal abnormality than their partners. Locock and Alexander 19 report that men’s feelings and status have sometimes been overlooked in the context of fetal screening, particularly when screening detects possible problems with the baby. Men’s role as a parent should be in focus but may sometimes come into conflict with other roles that have earlier been identified for partners, in the context of prenatal screening, for example ‘protectors/supporters’ or ‘bystanders’. 19
It has been shown that ultrasound increases maternal–fetal attachment when measured before and after the examination 20 and also that mothers’ and fathers’ experiences and reactions to ultrasound screening with normal findings are much the same. 21 Therefore, it is of interest to explore whether ultrasound also changes parents’ attitudes to continuation or termination of pregnancy in case of fetal abnormality.
Aim
The aim of this study was to explore whether expectant parents’ attitudes to termination or continuation of pregnancy, both in general and in case of fetal abnormality, were affected by previous experiences of miscarriage and whether attitudes change after ultrasound screening with normal findings. It was also of interest to investigate differences in attitudes in relation to age, parity and gender.
Methods
The material analyzed in this study included items from a questionnaire used in a one-year, prospective, observational cohort study of parents’ expectations, experiences and reactions to routine ultrasound examination, measured before and after the scan, in pregnancy week 18.
22
The items in the present study concerning parental attitudes about whether to terminate or to continue pregnancy in case of fetal abnormality have not previously been analyzed. There were eight items included in the analysis. They consisted of three statements which were posed both before and after a routine ultrasound examination and two statements which were posed only after ultrasound:
I can consider giving birth/becoming a parent to a child with an abnormality. I can consider terminating the pregnancy if the fetus has an abnormality, even if the abnormality is not lethal. I can understand others that continue with their pregnancy despite the fact they have been told that the baby has an abnormality.
I can understand others that have an abortion when the fetus has an abnormality, even if the abnormality is not lethal. I am doubtful about abortion in general.
Participants and procedures
The study took place during the period 10 February 2005 to 30 March 2006 and the first part of the questionnaire was sent to all parents booked for a second trimester ultrasound examination at a Swedish University hospital. The questionnaires, one for the women (n = 2982) and one for their partners (n = 2982), were sent to the woman’s address, together with the appointment time, about two weeks before the second trimester ultrasound examination. The woman was asked to give the other questionnaire to her partner. Written information and consent forms, for both parents, were included. A reminder was sent, if possible, within the time scale. The questionnaires could either be returned in a stamped addressed envelope or put in a locked mailbox at the Ultrasound Department. Pre-ultrasound scan replies were received from 2914 people (reply frequency women 57% and men 43%) but 62 respondents were later excluded, because of adverse findings at the examination, resulting in a total of 2852 pre-scan questionnaires. An analysis of some characteristics of the drop-outs has previously been performed. 22 A short anonymous questionnaire about drop-out was sent to all women (N = 260) who had not replied within a two-month period of the study. Of those, 55% (n = 144) replied. The most common reason for not answering the questionnaire was that it was considered to be too extensive, and 42% of the women had not given the questionnaire to their partners, partly explaining the lower reply frequency for men.
The second part of the questionnaire was mailed out, after the ultrasound examination, to all parents who had answered the first part (n = 2852), with the exclusion of those who had not had a normal scan result. Two reminders were sent. Of those who answered the pre-scan questionnaire, 30 more respondents were lost to follow-up (for example, because of miscarriage). The second questionnaire was answered by 77% of those who had answered the first: 1258 women and 925 men. The criteria for inclusion in analysis were that the respondents should have had normal ultrasound findings. For the analysis of the comparisons of the answers before and after ultrasound examination, an additional inclusion criterion was that the respondents should have answered both the pre- and the post-scan questionnaire.
Approval to undertake the study was obtained from the Regional Ethical Review Board in Lund.
Analysis
The Mann–Whitney U test has been used for comparing the responses from two independent groups: gender, age groups, parity and previous experience of miscarriage.
The cut-off for maternal age was chosen at 35 years as 25% of the mothers were 35 years or older. When comparing the answers before and after ultrasound, the sign test, which is a non-parametric test for changes in pairwise ordinal data, has been applied. The sign test compares the proportion of individuals who changed to a more positive answer with the proportion of individuals who changed to a more negative alternative. All statistical tests as well as the descriptive analysis have been performed using SPSS Statistics 18 for Windows (IBM Corporation, Somers, NY, USA).
Results
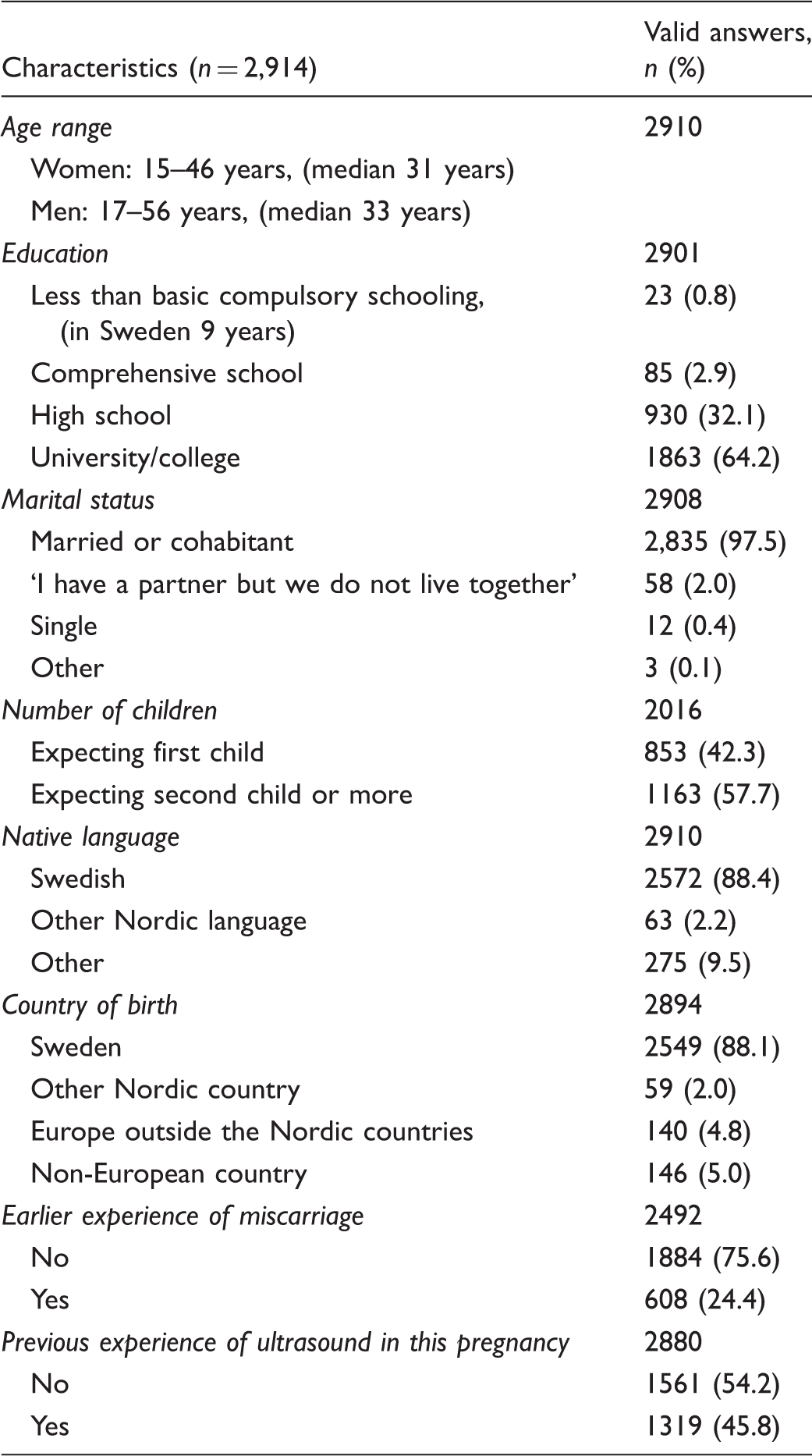
Characteristics of the respondents.
The parents’ attitudes
Measurement of changes in expectant parents’ attitudes to termination or continuation of pregnancy after the ultrasound examination using the non-parametric sign test. All three questions show statistically significant changes in attitudes in a direction which is more positive for the continuance of the pregnancy.
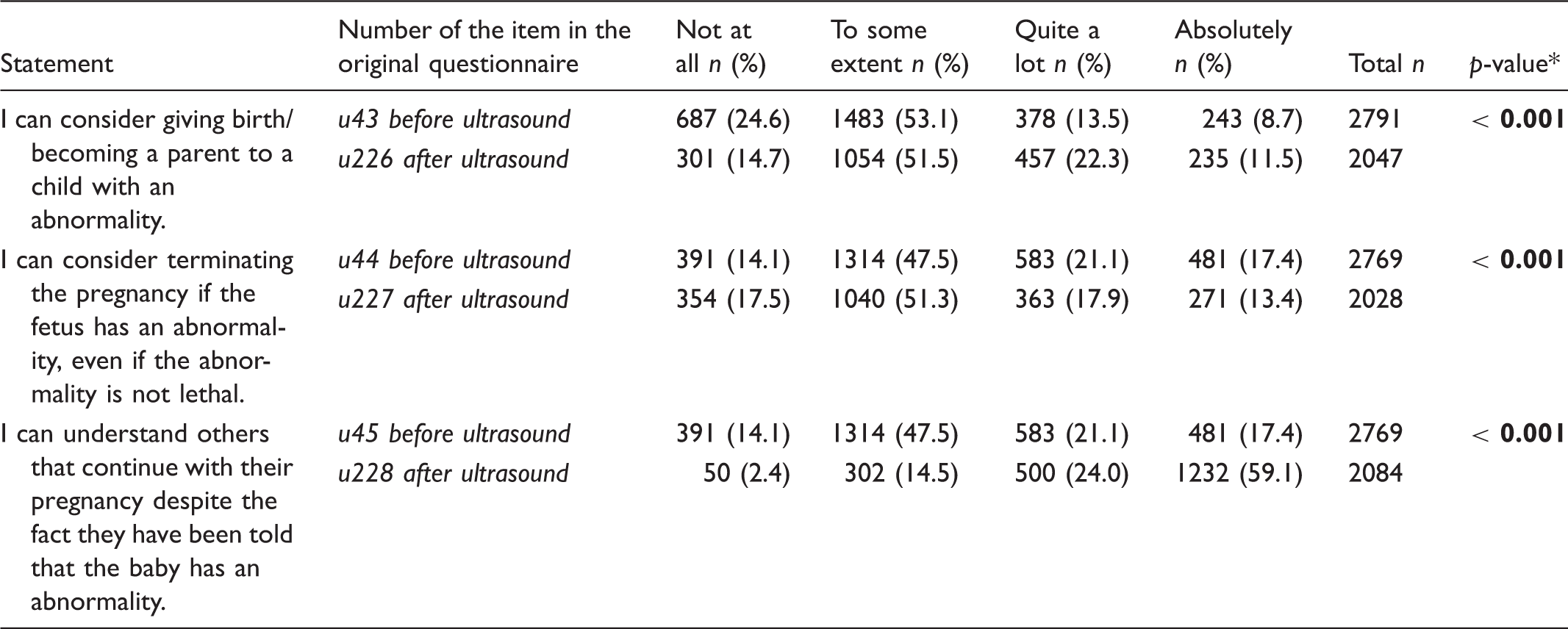
The statement ‘I can understand others that have an abortion when the fetus has an abnormality, even if the abnormality is not lethal’ was only posed after the ultrasound and showed that the majority 48.9% (n = 1380) answered ‘absolutely’ and 2.9% (n = 81) answered ‘not at all’.
Changes in attitudes after ultrasound
A comparison between the results pre- and post-ultrasound showed that there was significant change towards a more positive attitude to give birth to a child with an abnormality after the ultrasound examination (p < 0.001). A significant change was shown after the ultrasound towards a more positive attitude to other parents’ decisions to continue pregnancy in case of fetal abnormality (p < 0.001). There was also a significant change showing that the parents were less willing to terminate for fetal abnormality after the ultrasound examination than before (p < 0.001).
The results from the questions answered before the ultrasound showed that men were significantly more willing to terminate for a fetal abnormality (p < 0.001) and significantly less hesitant towards abortion in general than women (p < 0.001) (Figure 1). Men were also significantly less understanding towards other parents’ decisions to continue pregnancy in case of fetal abnormality (p < 0.001). No other statistical differences were shown between sexes (‘I can consider giving birth/becoming a parent to a child with an abnormality’ p = 0.503, ‘I can understand others that have an abortion when the fetus has an abnormality, even if the abnormality is not lethal’ p = 0.246).
Women’s and men’s attitudes to terminate or to continue pregnancy in case of fetal abnormality shown as percentages. Options for the answers were: 1 = not at all, 2 = to some extent, 3 = quite a lot, and 4 = absolutely.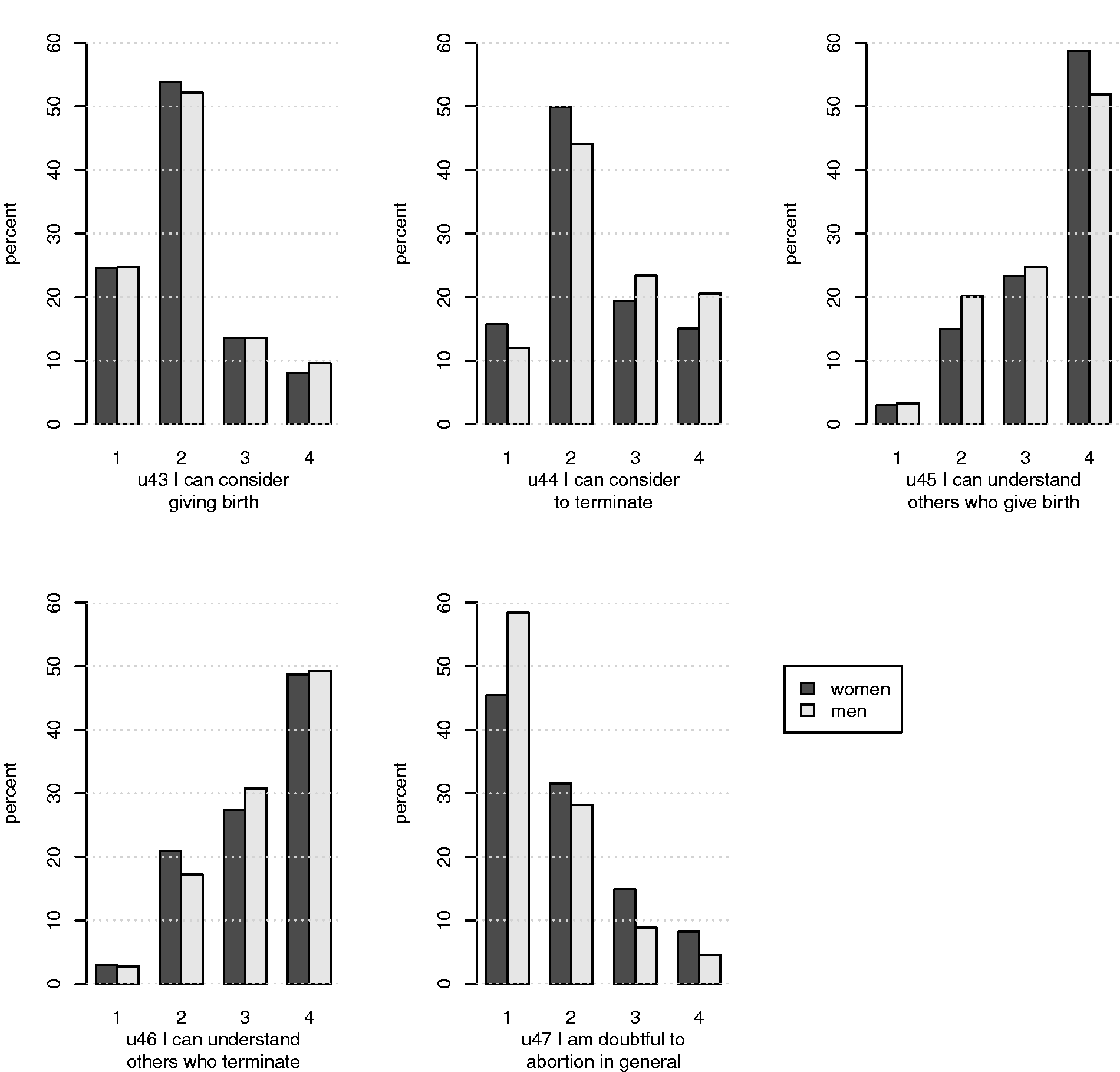
The attitudes of subgroups
Women aged 35 years or older were significantly less willing to give birth to a baby with an abnormality (p < 0.001) and significantly more positive to termination for fetal abnormality than younger women (p < 0.001) (Figure 2). There were no significant differences between women aged 35 years or older and younger women concerning attitudes towards other parents’ decisions (in case of continuing pregnancy p = 0.093, in case of termination p = 0.248), or concerning attitudes to abortion in general (p = 0.315).
Younger versus older women’s attitudes to abort or to continue in case of fetal abnormality shown as percentages. Options for the answers were: 1 = not at all, 2 = to some extent, 3 = quite a lot, and 4 = absolutely.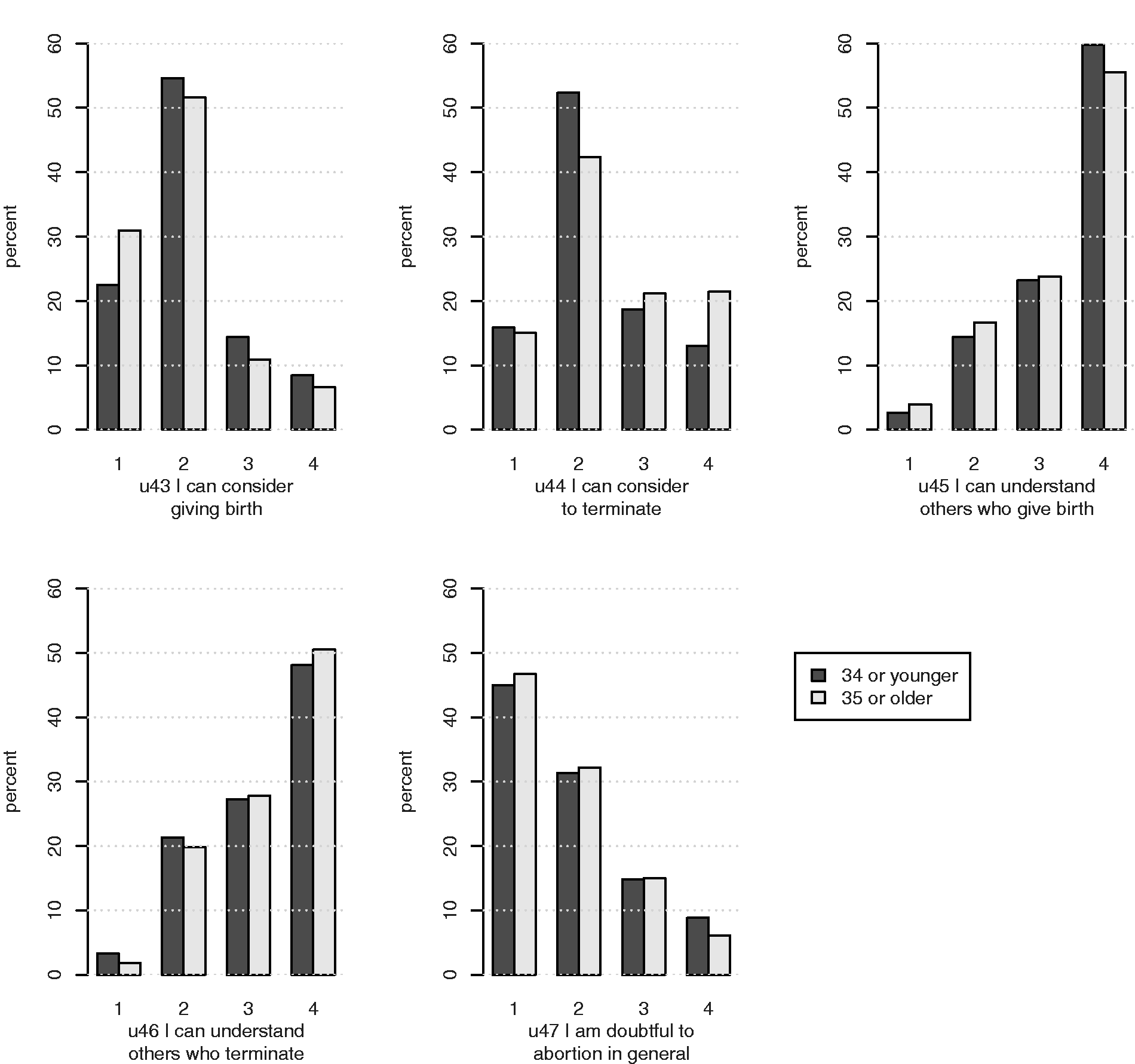
Parents who had previously had one or more children were significantly more doubtful to abortion in general than parents expecting their first child (p < 0.05). No other statistically significant differences in answers were demonstrated between first-time parents and parents who already had children. No significant differences in answers between respondents with previous experience of miscarriage (n = 593) and other parents were shown.
An analysis of the group lost to follow-up who had answered the pre-scan questionnaire but declined to answer the post-scan questionnaire, was performed concerning the questions regarding parents’ attitudes to termination or continuation of pregnancy. It showed that the group lost to follow-up were significantly less willing to give birth to a baby with an abnormality (p = 0.029). They were also significantly less understanding towards others’ decisions to continue pregnancy in case of fetal abnormality (p = 0.013) than those who answered both questionnaires. No significant difference was shown concerning attitude to termination if the fetus were to have an abnormality (p = 0.447).
Discussion
The results show that the participants were positive about the possibility to choose termination both in general and in the case of fetal abnormality, although most parents were hesitant and to some extent willing to consider both options: to continue the pregnancy or not. This is important knowledge for those who support couples in antenatal care.
In a study from the USA 11 participants, when asked before the NT examination, were more positive towards continuation of their pregnancy in case of abnormality than the Swedish parents in our study, although they all showed similar uncertainty. An explanation might be that these questions pose a very difficult decision, even before prenatal testing. This is an indication that parents need a great deal of support in cases of a fetal abnormality diagnosis as previously shown by Larsson et al.24,26 Asplin et al. 6 performed a questionnaire study with 99 women who had been diagnosed with a fetal malformation. Although these women needed information without prolonged delay, they also requested additional information before the final decision to continue the pregnancy or not. It has been shown in an interview study with 40 pregnant women that they preferred pre- and post-test counseling to be delivered by a midwife, 23 so this is an increasingly important midwifery issue. The finding that most parents were positive towards termination implies that parents value the ultrasound examination for the possibility of detection of fetal abnormality and the possibility to choose to terminate the pregnancy. In Sweden, however, parents have to seek for permission, in accordance with Swedish legislation, if the pregnancy has progressed further than 18 full weeks. 2 An additional possible explanation of the parents’ uncertainty might be that the severity of the abnormality was not clearly defined in the questions. The results might have been different if the malformations had been better defined, but it is known that the severity of the malformation is not always proportional to the parents’ initial reaction when the ultrasound finding is abnormal. 24 With some conditions it may be of medical advantage to know about the diagnosis before delivery in order to plan the necessary care, for example with heart malformations. 25 It can also be of psychological advantage for parents who may be given a prenatal consultation with a neonatologist 27 or other specialists.
The statistical differences in attitudes before and after ultrasound might be explained by the fact that the examination is an overwhelming experience for parents, especially when they see their fetus move, 21 and they are therefore are less likely to choose termination post-ultrasound. This result might also be due to the fact that all participants in the study had normal ultrasound findings. The result might have been different if parents with an adverse ultrasound diagnosis had been included, but it would have been unethical to send a general questionnaire to those parents. These parents have been included in other studies involving personal contact.24,26
Parents might find the decision more complex and difficult after a fetal malformation diagnosis than they imagined before the examination. However, Kimport et al. have shown that ultrasound viewing in the context of abortion did not affect women’s choice. 28
Couples may have completed the questionnaire together. This could lead to an underestimation of differences between men and women. It is not known what other factors, not related to the ultrasound examination, affected how the parents responded to the questions before and after the ultrasound examination. The characteristics of the study population are similar to those of another large Swedish study of pregnant women and can therefore probably be considered representative of the Swedish population. 29
Parents had very understanding attitudes towards other parents’ decisions, whatever these were. Similar results have been shown in an interview study with women who had undergone a legal abortion – their attitudes towards legal abortion in general were more positive than their attitudes towards their own abortion in particular. 30 The reasons for their negative attitudes towards their own abortion were the fears that that they might regret their abortion later in life and also the risk of infertility following an abortion. 30 Leung et al. 9 showed that among a group of women who had negative attitudes towards having a termination because of chromosomal anomalies, few stated that the option of abortion should not be available to other pregnant women. In our study men were more in favor of abortion than women. The statement ‘I am doubtful about abortion in general’ was only posed in the first part of the questionnaire but it would have been of interest to know their responses after the ultrasound as well, to explore whether their attitudes had changed.
An unanswered question is why the results showed statistical differences between sexes in some, but not in all items. In a Pakistani study from 2008, 10 women were more positive towards abortion in case of congenital syndromes than men, even considering that induced abortion is illegal in Pakistan. Alsulaiman and Hewison 18 came to the same conclusion in their study of a Saudi Arabian population. The differences could be due to cultural differences between countries. The Swedish National Association for Persons with Intellectual Disability (FUB) fears that both economical and practical support for the disabled may decrease if the number of children born with disabilities is reduced and the possibility of prenatal diagnosis and selective termination increases. 31 Therefore it is of interest to describe women’s and men’s attitudes towards other parents’ decisions in case of the detection of a fetal abnormality during pregnancy. Parents’ decisions are probably influenced by existing social structures, attitudes within the family itself and how health professionals act in connection to prenatal diagnosis.
Hickerton et al. performed in-depth interviews with parents whose fetus was diagnosed with a genetic disorder or had an increased risk result and who continued the pregnancy. 32 The study showed that parents felt that individual support was important in the context of prenatal diagnosis such as adequate information about the test and possible outcomes. Hickerton et al. also reflect on society and have reported that other people’s attitudes had an impact on parents who experienced a diagnosis of genetic abnormality. 32 Our study shows the positive result that expectant parents, mirroring society, are very understanding to other people’s decisions in these questions, no matter what those decisions might be. Since the material was collected in 2005/2006 attitudes may have changed, but it is likely that they have not changed much, since the ultrasound screening program is almost the same today. It would be of interest to study further what impact different screening programs have on parental preferences. Do parents in countries with a generous screening program have different attitudes in case of fetal abnormality than parents who are offered less extensive screening?
Conclusions
Women and men were positive about the possibility to choose abortion both in general and in case of fetal abnormality. It is important for care givers to consider that most parents were hesitant and to some extent willing to consider both hypothetical options: to terminate or to continue the pregnancy. Visualization of the baby affects parents’ attitudes, and gender and age can also have an implication for attitudes towards termination. Parents therefore always need individualized information and support in connection with prenatal diagnosis, and midwives play an important role in this.
Footnotes
Acknowledgements
The authors thank the participating parents, the ultrasound department, SSSH (Föreningen Södra Sveriges Sjuksköterskehem) for funding and Susann Ullén for statistical advice.
Funding
This research received funding from SSSH (Föreningen Södra Sveriges Sjuksköterskehem).
Conflict of interest
The authors declare that there is no conflict of interest.