
Abstract
Introduction:
Hepatitis B virus is a viral infection which can cause both acute and chronic liver disease. Predominately, this virus transmitted through the mother-to-child route. It is an endemic disease in low-resource setting countries like Ethiopia.
Objective:
Therefore, this study was used to assess magnitude and associated factors of hepatitis B surface antigen among pregnant mothers, who had antenatal care in Attat Hospital.
Method:
The cross-sectional study was conducted from 1 September 2019 to 30 January 2020. The data were collected from serological testing in laboratory and interview in antenatal care on 422 pregnant mothers. The data were entered into Epi Data version 3.1 and exported to SPSS version 24.0 for further analysis. Variables on bivariate analysis at p < 0.25 were taken to multivariate analysis. A p value of less than 0.05 on multivariate analysis was considered significant.
Result:
From 438 total samples, 422 respondents were participated and the mean age of the participants was 25.4 years (standard deviation ± 4.85). Magnitude of hepatitis B surface antigen was 10.9% (95% confidence interval: 8.3, 14.0). Respondents whose occupation was in government or self-employed were 67% (adjusted odds ratio = 0.33, 95% confidence interval: 0.12, 0.91) and whose number of gravidity was 3 and below were 79% (adjusted odds ratio = 0.21, 95% confidence interval: 0.04, 0.68) less likely to have hepatitis B surface antigen. Respondents who respond that hepatitis B surface antigen has cured were 1.52 times (adjusted odds ratio = 1.52, 95% confidence interval: 1.7, 9.4) more likely to have hepatitis B surface antigen. Respondents who answered hepatitis B surface antigen has vaccine were 57% (adjusted odds ratio = 0.43, 95% confidence interval: 0.05, 0.75) less likely to have hepatitis B surface antigen.
Conclusion:
Magnitude of hepatitis B surface antigen among mothers who were on antenatal care in Attat Hospital was high compared to other studies. Being employed in government or self-employed, gravida 3 and below, those who think that the disease has vaccine and those who think hepatitis B surface antigen was curable were statistically significant factors. Health promotion should be an important recommendation to be done by the hospital.
Introduction
Hepatitis B virus (HBV) is thought to be the main etiological agent for chronic liver disease (CLD) worldwide caused by a double-stranded DNA.1–4 HBV infections can cause both acute and CLD, including cirrhosis and hepatocellular carcinoma (HCC).5,6The hepatitis B surface antigen (HBsAg) is the serologic hallmark of HBV infection, while the soluble extractable protein, the hepatitis e antigen (HBeAg), is a marker for the highly infectious state. 7
HBV accounts about 50%–80% of HCC cases worldwide. 8 More than 780,000 people die per year as a result of HBV-related liver diseases including chronic hepatitis, cirrhosis and HCC, making HBV infection the 10th leading cause of death globally.9,10
In Nigeria, HBV is endemic and it has been estimated that 10%–12% of the total population are chronic carriers.11,10Countries of sub-Saharan Africa have a high endemicity, and more than 50 million people are chronic carriers of the HBV.12,13 In endemic areas, however, most individuals are infected by vertical transmission or in early after birth.10,14
HBV is predominately transmitted through mother-to-child transmission (MTCT).12,15 Chronic HBV infection during delivery occurs in approximately 90% of infants who are HBsAg-positive mothers. 16 When pregnant mothers are infected with HBV, there is a 10%–20% chance of transmitting the virus to their neonates. 17 Magnitude of HBV among pregnant women worldwide is approximately 5%, ranging from 0.6% in low-endemic regions to >20% in high-endemic areas in the Far East and Africa. 16
Apart from its significant magnitude, liver disease contributes to approximately 12% of the hospital admissions and 31% of the mortality in Ethiopian Hospitals. 18 In Ethiopia, a lack of information is the leading factor to have HBsAg among pregnant mothers.5,19
Being urban dwellers, young age and unemployment were the common factors affecting HBsAg.10,14 Educational status, having history of surgery, dental procedure, ear piercing, abortion and tattooing were other factors affecting HBsAg. 16
However, routine antenatal screening and intervention strategies are not yet practiced in Ethiopia. 1 Even if Ethiopia rolled out childhood immunization against HBV in 2007, vaccine is delivered in a pentavalent form as part of Expanded Program on Immunization (EPI) of newborns. 18
However, primary (vaccines and post-exposure prophylaxis) and secondary prevention of HBV transmission by appropriate sexual and sanitary practices is not yet optimal in Ethiopia. A measure for early detection (serological, molecular) and treatment of infected pregnant women is not a practice. This study aimed to determine the magnitude of HBsAg and associated factors among mothers following antenatal care (ANC) in Attat Hospital.
Methods and materials
Study setting, design and period
Attat Hospital is a primary hospital located in Guraghe zone, Cheha woreda, 175 km south from Addis Ababa. The hospital ANC clinic gives routine antenatal screening services such as: HIV, hemoglobin, blood group, rapid plasma reagin (RPR) and urinalysis (glucose, protein, infection) tests for more than 15 pregnant women per day. Institution-based cross-sectional study was conducted among pregnant mothers attending antenatal Clinic. The study was conducted from 1 September 2019 to 30 January 2020.
Population
The source populations were all pregnant mothers who had ANC contact in the hospital. All pregnant mothers who had ANC contact were included, and those who have severe illness during data collection were excluded.
Data collection methods and procedures
The data for the study were collected from serological testing in laboratory, and interviewer-administered questionnaires were used in antenatal follow-up clinic. The interview parts of the questionnaire were done by two professional midwives and two medical laboratory technicians after having received a clear direction and signed agreement form. Pregnant woman were contacted in the hospital waiting room for mothers who have ANC checkup. Mothers who had interviewed in ANC were marked as interviewed on their laboratory request for the serum HBsAg test, and their result was recorded as positive or negative accordingly with their ANC registration number. At the end of the day, the questionnaire in ANC and result in laboratory were compiled.
Sampling
Sample size was determined using single population proportion formula by considering the 95% confidence level; since there were no similar studies in the similar setup, the p value of 0.05 was used, and on adding 15% non-response rate, the final sample size will be 438. Systematic random sampling method was used to select participants, and the average number of patient flow before 1 year of the data collection was 450. From this average number, the total number of expected clients in the 5 months of data collection period was 2250 which gives an interval value of 5.
Laboratory investigation and procedures
After obtaining oral and written informed consent, 5 mL of venous blood was collected in plane tubes under aseptic conditions from the peripheral vein by data collector. These tubes were labeled with their ANC registration number and processed at the time of collection. The blood samples taken from the individuals were centrifuged at 3000 r/min (RPM) for at least 20 min at room temperature, and the serum was separated.
All the serum samples were tested for HBsAg by using rapid HBsAg test kit following standard operating procedures; samples reactive for HBsAg were confirmed by the same method. Samples tested twice positive were considered positive. A study participant who is positive for HBsAg was referred to the attending physician for further evaluation.
The one-step HBsAg test strip (serum or plasma) was a qualitative lateral flow immune chromatographic assay for the detection of HBsAg in the serum or plasma. The membrane was precoated with anti HBsAg antibodies on the test line region of the strip. During testing, the serum of plasma specimen reacts with the particles coated with anti-HBsAg antibody. The mixture migrates upward in the membrane chromatography by capillary action to react with anti-HBsAg antibodies on the membrane and generate line. The presence of this colored line in the test region indicates a positive result, while its absence of a negative result. To serve as procedural control, a colored line always appears in the control line region indicating that proper volume of specimen has been added and membrane wicking has occurred.
Data quality control
The validity and completeness of the data were checked by the principal investigator daily at the end of data collection. One-day training was given to the interviewer and laboratory technician on methods and consensus of data collection method. The performance of the rapid HBsAg test kit was evaluated using known positive and negative control obtained from the rapid HBsAg test kit. Furthermore, formation of colored band to the control (C) line acts as a procedural control and serves to valid the results. Blood samples were collected aseptically from pregnant mothers and properly labeled by the patient identification number. The specimens were collected by trained laboratory personnel. The samples were centrifuged; the serum was evaluated and separated appropriately and stored until transported to the laboratory.
The reagent and test method were assessed with a known positive and negative control materials. The standard laboratory procedures were followed, and the result was checked by the supervisors.
Variables
HBsAg was the dependent variable, and socio-demographic characteristics (age, marital status, occupation, educational status, number of gravidity), information about HBsAg (heard about hepatitis; heard about HBV; is hepatitis B viral? can HBV affect any age group?; heard about symptoms of HBV; is it curable?; is it self-restricted?; is vaccination available?; may you get HBV; your reaction if you have HBV; with whom you talk to if you are positive?; how much is the diagnosis cost?; what will be your worries if you are positive?; when you will go to facilities if you have symptoms?; have you got vaccination?; do you ask for new syringe before use?; do you ask for screening of blood to be transfused?; if you are positive, would you go for further investigation?; would you avoid meeting if you are positive?; have you ever participated in health education?) and transmission of HBsAg (transmitted by unsterile tools, transmitted by contamination, transmitted by unsterile blades, transmitted by intercourse, MTCT) were the independent variables.
Data analysis
Data were checked manually for completeness. Then, the data were cleaned and stored for consistency after entering into Epi Data version 3.1 software. For further analysis, the data were exported to statistical package for social sciences version 24.0 software. Descriptive statistics were carried out. Bivariate and multivariate analysis was used to see the effect of independent variables over HBsAg. Variables which were significant on bivariate analysis at the p value less than 0.25 were taken to multivariate analysis. The fitness of model was checked by the Hosmer and Lemeshow test. In multivariate analysis, the p value of less than 0.05 and 95% confidence level was used as a cutoff point for presence of association. Finally, results were compiled and presented using tables, graphs, charts and texts.
Result
Socio-demographic characteristics of the respondent
In this study, from 438 total sample sizes, 422 respondents were participated with a 96.35% response rate. The mean age of the respondents was 25.4 years with a standard deviation of 4.85. Most of the respondents were married, and more than half of the respondents were self-employed (Table 1).
Socio-demographic characteristics of respondents for HBsAg and its associated factors among mothers following antenatal care in Attat Hospital, April 2020 (N = 420).

HBsAg: hepatitis B surface antigen.
Information about HBsAg
From the total respondents, 301 (71.3%) respondents’ response was HBV is curable. In addition to this, about 46 (10.9%) of them answered that it was self-restricted (Table 2)
Information about HBsAg and its associated factors among mothers following antenatal care in Attat Hospital, April 2020 (N = 420).

HBsAg: hepatitis B surface antigen; HBV: hepatitis B virus.
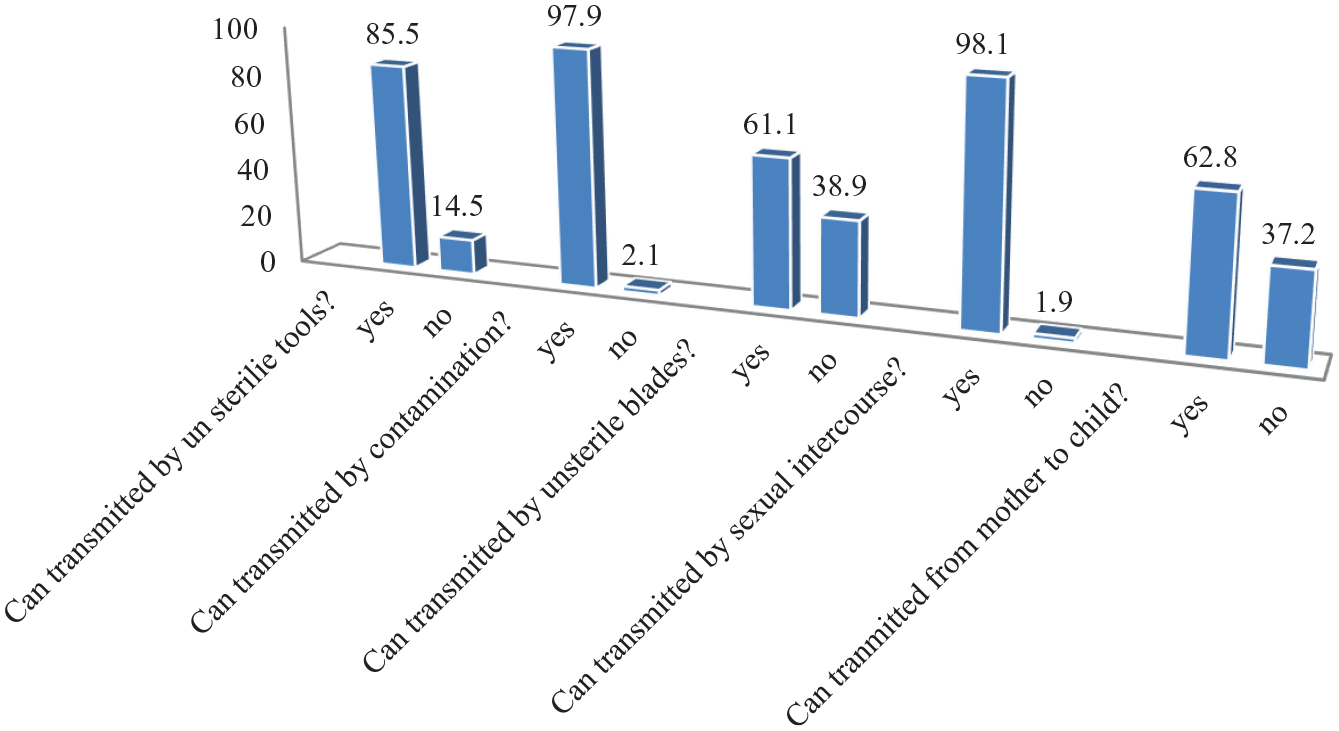
Participants’ response about the transmission of HBsAg
From the respondents, 164 (38.9%) of them respond that unsterile blade cannot transmit HBsAg. Similarly 157 (37.2%) of the respondents answer HBsAg cannot be transmitted from mother to child (Figure 1). From the total test results, 46 (10.9%) of them were positive for HBsAg test (Figure 2).
Information about transmission of HBsAg and its associated factors among mothers following antenatal care in Attat Hospital, April 2020 (N = 420).

Laboratory results of HBsAg and its associated factors among mothers following antenatal care in Attat Hospital, April 2020 (N = 420).
Factors associated with HBsAg
In bivariate analysis Occupation, number of gravidity, heard about HBsAg, heard about transmission, hear about cause of HBsAg, Measure taken for symptoms, is HBsAg curable, is HBsAg self-restricted, is vaccination available for HBsAg, have chance to get HBsAg, participated in health education program and actions if there are symptoms were included. From this only occupation, number of gravidity, did it have cure and is vaccination available were stay statistically significant in multivariate analysis (Table 3).
HBsAg and its associated factors among mothers following antenatal care in Attat Hospital, April 2020 (N = 420).

HBsAg: hepatitis B surface antigen; COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio. *p ≤ 0.05.
Bold values are significant variables with p value less than or equal to 0.05.
Respondents whose occupation was in government or self-employed were 67% (adjusted odds ratio (AOR) = 0.33, 95% confidence interval (CI): 0.12, 0.91) less likely to have HBsAg compared to those who were housewife or not employed. Respondents whose number of gravidity was 3 and below were 79% (AOR = 0.21, 95% CI: 0.04, 0.68) less likely to have HBsAg compared to those whose gravidity was 4 and above. Respondents who respond that HBsAg has cure were 1.52 times (AOR = 1.52, 95% CI: 1.7, 9.4) more likely to have HBsAg test compared those who respond that it does not have cure. Respondents who answered HBsAg has vaccine were 57% (AOR = 0.43, 95% CI: 0.05, 0.75) less likely to have HBsAg compared to those who answered it does not have vaccine (Table 3).
Discussion
Magnitude of positive HBsAg test among mothers following ANC in Attat Hospital was 46 (10.9%) (95% CI: 8.3, 14.0) which is higher than a study in the Gojjam zone 7.5%, 5 Yirgalem hospital 7.2%, 1 Dawuro zone 3.5%, 4 Adis Abeba 6.0%, 18 in Nigeria 6.78%, 7 in Mali 8% 12 and in southern 7.8%. 20 The magnitude of this result was similar to that in studies in Nigeria and Uganda.8,21 In summary, global magnitude of HBsAg is clustered as high (⩾8%), intermediate (2%–7%) and low (<2%). 22 Thus, the result of this study belongs to the high magnitude category. This difference might be due to inadequate information as stated by the result of this study. Other reason for this higher magnitude might be location of the study area which is remote.
Respondents whose occupation was in government or self-employed were less likely to have HBsAg compared to those who were housewife or not employed. Similarly, a study in Gojjam zone state’s housewives has higher risks, 5 and recent meta-analysis shows that income has impact on HBsAg. 23 Possible reason for this might be exposing factors may decrease when there is source of income.
Respondents whose numbers of gravidity were 3 and below were less likely to have HBsAg compared to those whose gravidity was 4 and above. A study in southern Ethiopia also shows that higher gravidity was risky for HBsAg, 3 and another study in Germany shows similar impact of being higher gravidas. 24 This might be due to decrease in exposure either during delivery or during termination of the pregnancy when most of the deliveries were at home and also when hospital setup was not safe enough when the number of gravidity was lower.
Respondents who respond that HBsAg has cure were more likely to have HBsAg test compared those who respond it does not have cure. Similar to a study in northern Tigray, 2 a study in different hospitals of Ethiopia states mothers in ANC have low awareness about HBsAg. 25 This might be because more than half (54.7) of mothers have never been participated in health education and most of them were housewives who have limited source of information.
Respondents who answered HBsAg has vaccine were less likely to have HBsAg compared to those who answered it does not have vaccine, which is similar to a study conducted in Yirgalem. 5 This might be because those who know that it has vaccination were better understanding to prevent the disease.
Strength and limitation of the study
Each patient participated in this study had laboratory investigation with either positive or negative result. This could provide an exact characteristic of the outcome variable.
Participants who had found to be positive for HBsAg were linked to follow-up as special case, considering hepatitis B immune globulin and hepatitis B vaccine for their neonate.
Data collectors were professionals who were on their routine activities in the study area which could substantially reduce errors on sampling and measurements.
Univariate, bivariate and multivariate analyses were used to see statistically significant effect of independent variable over the outcome variable.
Nature of the study design employed could not appreciate cause-and-effect relationship.
Since enzyme-linked immunosorbent assay (ELISA) was not routinely available in the study area, false-negative values of the rapid diagnostic tests result might deflate the prevalence of HBsAg.
Conclusion
Magnitude of HBsAg among mothers who were on ANC follow-up in Attat Hospital was high compared to other studies. Being employed in government or self-employed, gravida 3 and below and those who think that the disease has vaccine were less likely to have HBsAg, whereas those who think that the disease was curable were more likely to have HBsAg. Therefore,
Since the magnitude of HBsAg was high, the test should be routine so that neonates from positive mothers need to receive immunoglobulin and vaccination by the hospital;
Mothers who have no regular job need to be addressed by woreda and zonal health office, woreda and zonal administration office and other non-governmental organizations working on women’s empowerment.
Footnotes
Acknowledgements
My subjects, mothers who have antenatal care follow-up, who have been included in this study; this research report cannot be a plan if you are not here, many thanks dear mothers and live long. Mr Tewodros Tesfa never needs to be missed from this section for his important comments.
Author contributions
All authors have substantial contributions to conception, study design, acquisition of data, analysis and interpretation of data. H.D. has drafted and Y.F.G., H.D., M.M.G. and T.M.B. have critically reviewed the article. All authors have agreed on the journal to which the article will be submitted. They have reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication and any significant changes introduced at the proofing stage. Y.F.G. agrees to take responsibility and be accountable for the contents of the article.
Data sharing
Dataset supporting this study can be accessed discussing with the corresponding author. Since the data have confidential participant results, it could be available upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Haromaya University research review board with a review ID of 29/2012.
Ethical clearance
Permission was obtained from Gurage zone health office and Attat Hospital medical director office. Confidentiality and anonymity were ensured, and participants were informed that their participation was voluntary. The results were recorded with patients’ identification number, to avoid errors in the results of the test, repeatedly checked before reporting. The laboratory results were given to the hospital and to each pregnant woman.
Informed consent
Written and verbal informed consent was obtained from all subjects before the study.