
Abstract
The purpose of this study is to examine gender differences in quality of life (QoL) and symptomatology in fibromyalgia (FM) patients. A total of 20 men (48.0 ± 8.0 years) and 78 women (49.8 ± 7.2 years) with FM participated in the study (age range 31-63 years). Health-related QoL and FM impact were assessed by means of the Spanish versions of the Short-Form-36 Health Survey (SF36) and the Fibromyalgia Impact Questionnaire (FIQ), respectively. Comparisons in QoL were performed using one-way analysis of covariance adjusted by age and body mass index (BMI), and comparisons in FIQ dimensions were performed using Mann-Whitney test. Overall FM impact, as measured by FIQ-total score (p = .01) and FIQ-physical impairment (p = .02) was higher in men, whereas women presented higher values of FIQ-fatigue and FIQ-morning tiredness (p = .04) and less SF36-vitality (p = .02). Therefore, women appear to feel more fatigue, whereas men present higher FM overall impact. Due to the small number of men included in this study and the consequent small statistical power, these results should be taken as preliminary. Higher powered studies are warranted to further address gender differences in FM in order to design more successful treatments.
Introduction
Fibromyalgia (FM) is a disease characterized by the concurrent existence of chronic, widespread musculoskeletal pain and multiple sites of tenderness (Wolfe et al., 1990). FM symptomatology greatly differs among patients but commonly includes pain, morning stiffness, fatigue, nonrestorative sleep, and concentration and memory difficulties (Wilson, Robinson, & Turk, 2009; Wolfe et al., 1990). Therefore, FM has an enormous impact on patients’ health-related quality of life (QoL; Gormsen, Rosenberg, Bach, & Jensen, 2010; Verbunt, Pernot, & Smeets, 2008).
In Spain, the prevalence of FM is ~2.4% (Mas, Carmona, Valverde, & Ribas, 2008) and is dramatically more common in women than in men (~95% vs. ~5%, respectively; Mas et al., 2008). Studies on male FM patients are scarce, and information regarding differences in QoL and in FM symptoms between men and women with FM seems to be controversial and inconclusive. Some studies have observed that women with FM have more tender points (and hurt all over), total number of symptoms, and irritable bowel syndrome than men with FM (Buskila, Neumann, Alhoashle, & Abu-Shakra, 2000; Yunus, 2001; Yunus, Celiker, & Aldag, 2004; Yunus, Inanici, Aldag, & Mangold, 2000). It has also been stated that men have a worse perception of their health, a higher percentage of psychiatric history and current mental illness, decreased physical function, lower QoL, and more impact of the disease (Buskila et al., 2000; Ruiz Perez et al., 2007). In contrast, Lange, Karpinski, Krohn-Grimberghe, & Petermann (2010) observed no gender differences in pain measures, but they identified that men had more positive levels in psychological measures and coping strategies than women. More recently, Häuser et al. (2011) reported no relevant gender differences in the clinical picture of FM and concluded that the assumption of well-established gender differences could not be supported. The inconsistent results on gender differences in the clinical manifestations of the FM are difficult to explain (Hauser et al., 2011), and more studies are needed. Despite more studies having been focused on FM features and treatment in men in the past years (Aparicio et al., 2010; Carbonell-Baeza et al., 2011), they are still scarce.
To better understand FM disease, we believe that it is of interest to know the symptomatology and physical and psychological characteristics of the different groups of patients. Gender differences would require different gender-specific interventions. In fact, in the past years, an effort has been made to better classify FM patients, to identify subgroups with unique clinical characteristics, and to pinpoint therapeutic interventions (Buskila, 2009; de Souza et al., 2009; Turk, Okifuji, Sinclair, & Starz, 1998). There is, thus, a need to examine if women and men have different characteristics and manifestations of the FM in order to adapt the treatment and monitoring of the disease accordingly.
The present study aimed to examine the differences in QoL and FM symptomatology between male and female FM patients.
Method
Study Sample
We recruited 20 men aged 48.0 ± 8.0 years (range: 31-63 years) from a local association of FM patients from Granada (Spain) who were diagnosed with FM by a rheumatologist and met the American College of Rheumatology criteria for FM (Wolfe et al., 1990). To compare them with aged-matched (49.8 ± 7.2 years) women having the same characteristics, we contacted a total of 79 female FM patients. During this process, exclusion criteria included having other rheumatic diseases and/or severe somatic or psychiatric disorders, such as cancer, severe coronary disease, or schizophrenia. All the participants were informed about the study’s aims and methodology and were made to sign a written informed consent to participate. All patients were assessed by the same researchers to reduce interexaminer error. The study was reviewed and approved by the Ethics Committee of the “Hospital Virgen de las Nieves” (Granada, Spain).
Material and Procedures
Height (in centimeters) was measured using a stadiometer (Seca 22, Hamburg, Germany), and weight (in kilograms) and body fat (%) were measured by means of an eight-polar tactile-electrode impedanciometer (InBody 720, Biospace, Seoul, Korea). The validity of this impedanciometer has been reported elsewhere (Malavolti et al., 2003; Sartorio et al., 2005). Body mass index (BMI) was calculated as weight (in kilograms) divided by height (in meters) squared and categorized using international criteria.
The Spanish version of the Short Form-36 Health Survey (SF36; Alonso, Prieto, & Anto, 1995) was used to assess QoL. The SF36 is a measure of health status that is frequently used to assess QoL. This questionnaire is composed of 36 items that include questions about both physical and mental health. It assesses eight subscales: physical functioning, physical role, bodily pain, general health, vitality, social functioning, emotional role, mental health, and general health. Each subscale score is standardized (range: 0-100), where 0 indicates the worst possible health status and 100 the best possible health status. In the analysis of reliability as the stability of such a questionnaire, correlation coefficients between the test and retest were between .58 for the SF36-emotional role subscale and .99 for the SF36-physical role subscale. Internal consistency showed an alpha coefficient between .78 for the SF36-vitality subscale and .96 for the SF36-physical role subscale (Alonso et al., 1995).
The Spanish version of the Fibromyalgia Impact Questionnaire (FIQ; Rivera & Gonzalez, 2004) was used to assess the FM-related symptoms. FIQ assesses the components of health status that are believed to be the most affected by FM. It is composed of 10 subscales: physical impairment, overall well-being, work missed, and seven items (subscales) of a visual analog scale (VAS) marked in 1-cm increments, on which the patient rates the work difficulty, pain, fatigue, morning tiredness, stiffness, anxiety, and depression (Bennett, 2005). All the subscales ranged from 0 to 10, where high scores indicated a higher negative impact and/or a greater severity of symptoms. A total score may be obtained after normalization of some subscales and summing the subscales. The FIQ total score ranges from 0 to 100, and a higher score indicates a greater impact of the disease. In the analysis of reliability as the stability of such a questionnaire, correlation coefficients between the test and retest were between .58 for VAS-anxiety and .83 for work-missed days. Internal consistency showed an alpha coefficient of .82 for the total items of the FIQ; α = .79 for the eight items, without the two items concerning work, and α = .86 for the nine subitems of the physical impairment (Rivera & Gonzalez, 2004).
Statistical analysis
The distribution of the variables was examined. The FIQ variables showed a nonnormal distribution, whereas the anthropometric and QoL variables showed an acceptable normal distribution. Consequently, comparisons in QoL were performed using one-way analysis of covariance (ANCOVA) adjusted by age and BMI because high BMI has been associated with worse QoL (Yunus, Arslan, & Aldag, 2002). Comparisons between genders in FIQ dimensions were performed using exact Mann-Whitney test. Standardized effect size statistics were estimated in all the comparisons. We used Cohen’s d and its exact confidence interval for QoL variables (parametric). For FIQ variables (nonparametric) we used the probabilistic index P(XA > XB), which is the probability that the response X of a patient from Group A (e.g., male FM patients) is higher than the one for a randomly chosen patient from Group B (e.g., female FM patients; Acion, Peterson, Temple, & Arndt, 2006). All analyses were performed using the Statistical Package for Social Sciences (SPSS, version 17.0 for Windows; SPSS, Chicago, IL), and the level of significance was set at p < .05. The exact confidence intervals for Cohen’s d were obtained by means of the noncentrality parameter of the noncentral Student’s distribution using Wolfram-Mathematica 8.0 (Zou, 2007).
Results
Anthropometric and body composition characteristics of the study sample for men and women with FM are presented in Table 1. Comparisons in QoL and FM impact between men and women with FM are shown in Table 2. Women with FM had lower SF36-vitality (p < .05) than men with FM. Mean FIQ total score and physical impairment were higher (worse) for male than for female FM patients (p < .05), whereas female patients presented higher FIQ-fatigue and morning tiredness (p < .05).
Physical Characteristics of the Study Sample for Men and Women With Fibromyalgia
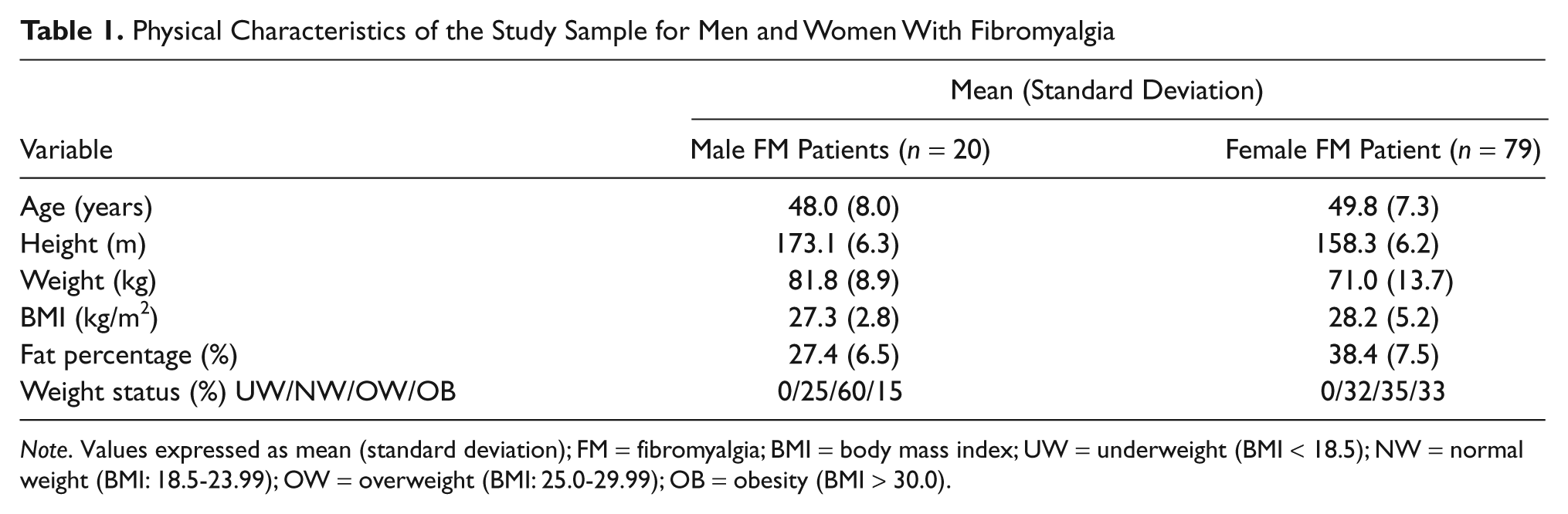
Note. Values expressed as mean (standard deviation); FM = fibromyalgia; BMI = body mass index; UW = underweight (BMI < 18.5); NW = normal weight (BMI: 18.5-23.99); OW = overweight (BMI: 25.0-29.99); OB = obesity (BMI > 30.0).
Health-Related Quality of Life and Fibromyalgia Impact of the Study Sample
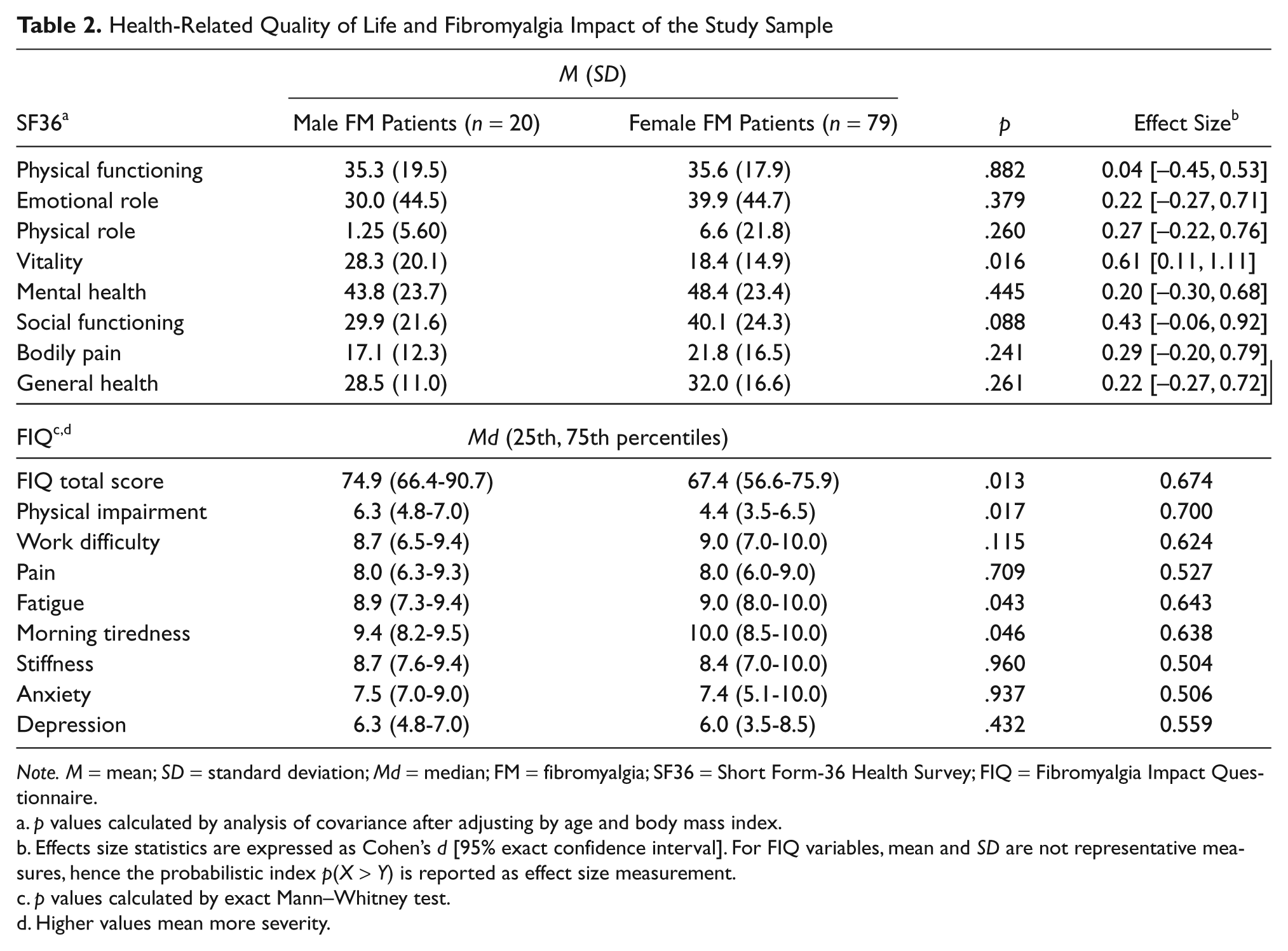
Note. M = mean; SD = standard deviation; Md = median; FM = fibromyalgia; SF36 = Short Form-36 Health Survey; FIQ = Fibromyalgia Impact Questionnaire.
p values calculated by analysis of covariance after adjusting by age and body mass index.
Effects size statistics are expressed as Cohen’s d [95% exact confidence interval]. For FIQ variables, mean and SD are not representative measures, hence the probabilistic index p(X > Y) is reported as effect size measurement.
p values calculated by exact Mann–Whitney test.
Higher values mean more severity.
Discussion
The vast majority of previous studies have been conducted on female FM patients. Very little is known about male FM patients and about gender differences in QoL and FM symptomatology. From a clinical point of view, it is of interest to examine the symptomatology and QoL differences between male and female FM patients in order to adapt the treatment and monitoring of the disease accordingly. We observed that overall FM impact and physical impairment were lower in women than in men with FM, whereas female FM patients showed higher fatigue and lower vitality.
In agreement with the study by Buskila et al. (2000), we did not observe important differences between the genders in QoL, as assessed by SF36, except for a slightly worse physical role and vitality in the female patients group, whereas they reported a worse emotional role in men. Note that other studies have reported a worse QoL in men with FM (Buskila et al., 2000; Ruiz Perez et al., 2007)
In our study, FM impacts measured by FIQ-total score were significantly higher in male than in female FM patients, which concurs with other studies (Buskila et al., 2000; Ramirez-Maestre, Lopez Martinez, & Zarazaga, 2004; Ruiz Perez et al., 2007; Yunus et al., 2004).
Despite the general agreement regarding the global severity of the disease, we have reported a notable controversy respecting the fatigue experienced by females and males with FM. Our findings concur with those of Yunus et al. (2000). They observed higher levels of fatigue and morning tiredness in the female FM group. However, other studies observed higher levels of fatigue in men (Buskila et al., 2000) or failed to find gender differences (Ruiz Perez et al., 2007; Yunus et al., 2004).
One similar Spanish study (Ruiz Perez et al., 2007) analyzed gender differences in sociodemographic, clinical, psychosocial, and health care characteristics in FM patients, and it observed that sociodemographic characteristics were similar in both men and women. However, men with FM had a worse perception of their health, a higher percentage of psychiatric history and current mental illness, and a greater impact of the disease. In contrast, Lange et al. (2010) observed no gender differences in pain measures, but they reported differences regarding psychological measures and coping strategies. Women reported more psychological strains and used more adaptive coping strategies on the scales “cognitive restructuring”, “perceived self-competence”, “mental diversion,” and “counterbalancing activities” than men. The authors concluded that women need more treatment for psychological aspects, and men need assistance in pain management.
Nevertheless, concerning pain perception, gender differences appear to be low or inexistent. Except for the higher pain perception observed by Buskila et al. (2000), most of the studies developed in FM patients, including ours, have not reported marked gender differences (Yunus et al., 2000; Yunus et al., 2004). In fact, in the study by Danneker, Knoll, and Robinson (2008), the authors examined the gender differences in ratings and effects of recalled and experimentally induced muscle pain in two substudies. In Study 1, participants completed a questionnaire about recalled muscle pain. In Study 2, participants described muscle pain from an exercise stimulus over 3 days by telephone. The authors concluded that there is an absence of meaningful sex differences in muscle pain ratings.
Finally, in a recent study by Häuser et al. (2011) conducted on a large sample of 885 women and 138 men, the authors observed that women reported a longer duration of chronic widespread pain and time since FM diagnosis and men had a higher tender point count. However, there were no gender differences in age, family status, number of pain sites, or somatic and depressive symptoms. They concluded that their data did not support the thesis by Yunus and colleagues (Yunus, 2001; Yunus et al., 2000; Yunus et al., 2004) that gender differences in the clinical features of FM are well established.
Several limitations of this study need to be mentioned. First, the major limitation of the present study is that, because of the extremely low prevalence of FM in men, the male sample size recruited was low and consequently it is difficult to generalize the findings. The associations observed presented a low to medium effect size. More studies looking at sex differences in FM patients with larger sample sizes are warranted. Second, our participants were volunteers, which could have affected the representativeness of the study sample. Third, individually tailored medication used for FM symptomatology, which unfortunately was not registered, might have potentially affected the study findings. Fourth, similar studies should be conducted with adequate representation of populations with no pain, mild and/or localized pain, as well as chronic widespread pain. There is evidence that regional pain syndromes are common in both genders; but with “spectrum” effects due to many differences between occupational and many other probably relevant factors, males and females still lead different lives between and within genders.
In conclusion, overall FM impact and physical impairment were higher in men, whereas women had higher levels of fatigue and lower vitality. We can conclude that women feel more fatigue, whereas men present higher FM global impact and worse physical impairment. Because of to the small number of men included in this study and the consequent small statistical power, these results should be taken as preliminary. In addition to the gender differences indicated, other gender differences could have been undetected due to the lack of power. Higher powered studies will further address gender differences in FM to design more successful treatments.
Footnotes
Acknowledgements
The authors are grateful to all the participants for their collaboration. We also thank all the AGRAFIM (FM association from Granada, Spain) members involved in the fieldwork for their efforts and great enthusiasm.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was in part financially supported by grants from the Spanish Ministry of Education (AP-2006-03676 and EX-2008-0641) and the Ministry of Science and Innovation (BES-2009-013442, and RYC-2010-05957).