
Abstract
While there is an abundance of research on the relationship between stigma and help-seeking attitudes among Asian Americans, few studies have examined how emotion and religious variables influence this relationship. Thus, using a moderated mediation model, we investigated how emotion regulation, emotion socialization, and religious coping might affect the relationship between close others’ stigma, self-stigma, and help-seeking among a sample of Asian American students (N = 105) from a Christian university. We predicted that (a) self-stigma would positively mediate the association between close others’ stigma and help-seeking attitudes, and (b) emotion regulation, emotion socialization, and religious coping would moderate this relationship. Mediation results showed that close others’ stigma was related to self-stigma, which in turn was associated with help-seeking attitudes. Moreover, this mediating relationship was moderated by religious coping (n = 70) but not emotion socialization or regulation; emotion regulation and help-seeking attitudes, however, were positively correlated. These findings highlight the influence of religious coping and emotion regulation strategies on views of counseling, and we reflect on some implications of these findings.
Some recent comparative studies found that Asian American college students experience more psychological distress compared with their non-Asian counterparts (Kalibatseva et al., 2020; M. R. Lee et al., 2006). Despite this reality, they also underutilize counseling services (e.g., Kearney et al., 2005) and express less favorable attitudes about professional help-seeking (Masuda & Boone, 2011). Therefore, researchers must continue to identify factors that might be associated with the help-seeking attitudes of Asian American college students, so that the broader mental health disparity of underutilization of mental health services might be addressed. As such, in this study, we examined a mediation model involving help-seeking attitudes as the outcome, and we explored moderators of this mediation model in a sample of Asian American college students.
Stigma and Help-Seeking Attitudes
Stigma is the unfavorable evaluation of people who have certain attributes that are looked down upon by society (Hinshaw, 2007). Prior literature has identified stigma as an important consideration for mental health service use among Asian Americans (e.g., Gee et al., 2020; Leong & Lau, 2001). For example, Gee et al. (2020) reported that Asian American college students demonstrated a higher level of family-related stigma of mental health compared with European American college students. It is not surprising, then, that stigma tends to be associated with less favorable help-seeking attitudes among Asian Americans (e.g., Masuda & Boone, 2011; Shea & Yeh, 2008; Ting & Hwang, 2009; Yee et al., 2020).
Recently, there has been an effort to differentiate between the sources of mental health stigma. In particular, perceptions of stigma from one’s close relationships (i.e., close others’ stigma) are important to consider, especially as a contrasting source of negative views compared with societal or public stigma (Vogel et al., 2009). Because Asian cultures tend to emphasize interpersonal connections, especially with family members (e.g., B. S. K. Kim et al., 2005), it is important to examine perceptions of how close social networks might feel about seeking psychological services. As such, this study examines close others’ stigma as a predictor of help-seeking attitudes.
Another stigma variable that is popular in the literature is self-stigma. Self-stigma refers to the tendency to internalize negative views from others about seeking professional mental health counseling (Vogel et al., 2006). There is research supporting the notion that self-stigma is a key predictor of help-seeking, Vogel et al. (2006) reported that it is associated with more unfavorable help-seeking attitudes, intent to seek professional counseling, and actual professional help-seeking behaviors. Therefore, this study examines self-stigma as a second type of stigma of mental health counseling and a correlate of help-seeking attitudes among Asian Americans.
In particular, stigma from external sources might serve as a precursor to internalized stigma. In support of this, Vogel et al. (2013) reported that public stigma predicted self-stigma after 3 months in a sample of U.S. college students; equally important was that the prediction’s reverse (self-stigma predicting public stigma after 3 months) was nonsignificant. In other words, these findings suggest that external sources of stigma come first and are followed by internal stigma.
Following this logic, researchers have examined mediating relations involving external sources of stigma (e.g., public or close others’ stigma) as a predictor, intrapersonal stigma (e.g., self-stigma) as a mediator, and help-seeking attitudes as an outcome (e.g., Allen et al., 2016; Ludwikowski et al., 2009; Mackenzie et al., 2019; Vogel et al., 2010), including in Asian (e.g., P. Y. Kim & Yon, 2019; E. J. Lee et al., 2014) and Asian American (e.g., Choi & Miller, 2014) samples. Notably, a recent, large meta-analytic study that included data from 54,793 people demonstrated that while both self-stigma and public stigma were significant predictors of help-seeking attitudes, public stigma was rendered nonsignificant when self-stigma was included in the predictive model (Yu et al., 2023). Given the strong empirical and theoretical arguments, it seems reasonable that our close others’ stigma variable would predict self-stigma, which in turn would predict help-seeking attitudes (see Figure 1).
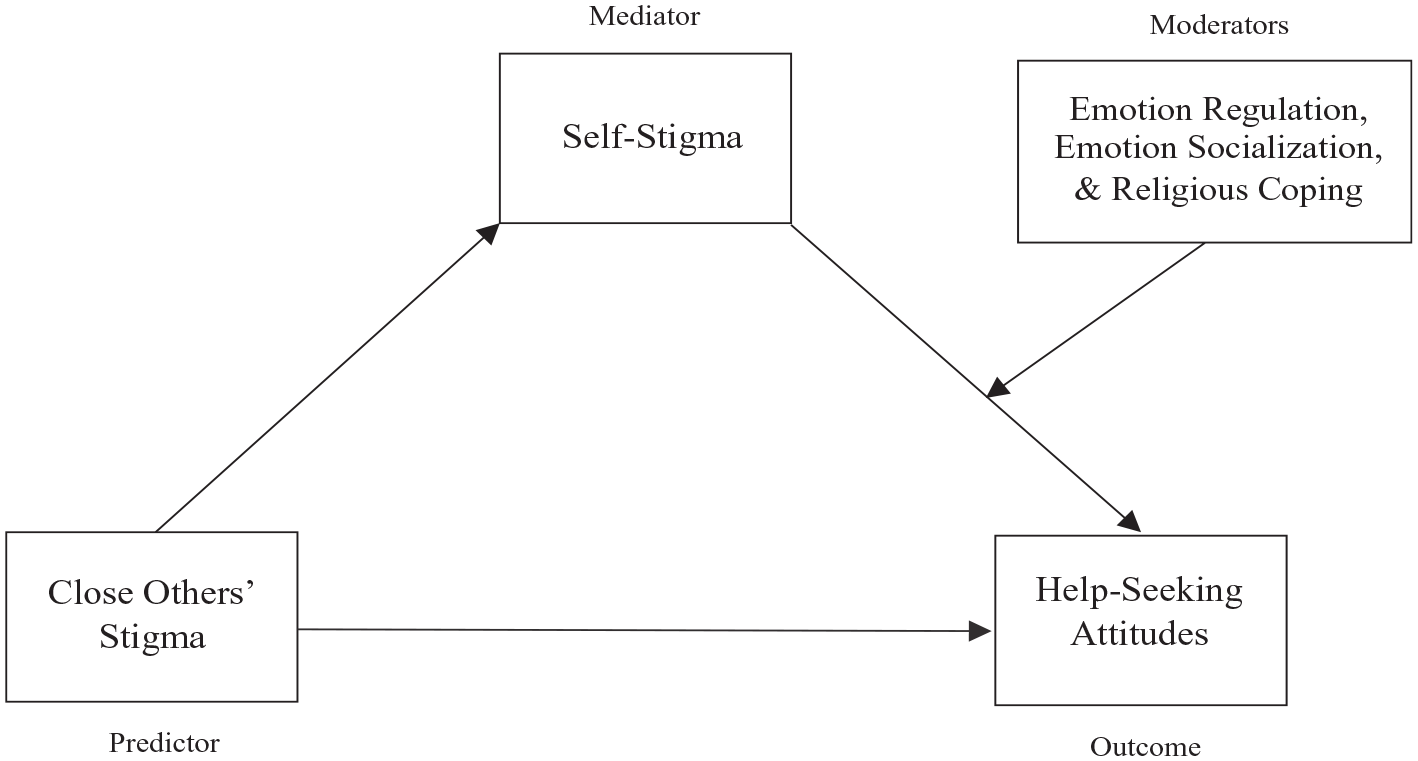
Hypothesized moderated mediation model: emotion regulation, emotion socialization, and religious coping as moderators.
However, given a few shortcomings of the empirical literature highlighting this mediation model among Asian American college students, we were motivated to replicate the current mediation model and extend it. First, the current literature tends to rely on a measure, ATSPPH-SF (Fischer & Farina, 1995), that has been critiqued for less-than-ideal psychometric characteristics (e.g., questionable content validity for some items, low reliabilities; see Hammer et al., 2018). For example, the studies cited earlier with Asian (P. Y. Kim & Yon, 2019; E. J. Lee et al., 2014) and Asian American samples (Choi & Miller, 2014) all used the ATSPPH-SF. In response to the shortcomings of the ATSPPH-SF, Hammer et al. (2018) developed a new measure of help-seeking attitudes named the Mental Help Seeking Attitudes Scale (MHSAS). In this study, we use the MHSAS to replicate the mediation models in the literature. Second, as a next step in extending the empirical literature, it is important to identify factors that might alter the mediation model. That is, if the empirical “story” is that stigma from others might be associated with help-seeking attitudes through self-stigma, are there additional stories to tell? For example, there might be compelling moderators of this mediation model that might aid the development of interventions. As such, in this study, we examined emotion regulation, emotion socialization, and religious coping as moderators.
Emotion Regulation and Socialization
Emotions are the processes of causally linked mental (i.e., appraisal, action tendency, subjective experience) and behavioral (i.e., physiological reactions, facial and vocal expression) elements (Reisenzein, 2007). While the expression of emotions can be influenced by several different factors, culturally specific values (and how they interact with core cultural ideas and practices) are especially influential in explaining emotions in the Asian American context. For example, members of Asian cultures tend to have an interdependent self-construal through which they view themselves in the context of their in-group. This influences which emotions Asian Americans view as socially acceptable to outwardly express. For example, “socially engaging” emotions, such as friendly feelings and guilt, promote social harmony and are encouraged in Asian contexts, whereas “socially disengaging” emotions, such as pride and anger, promote the expression of the individuals separate from their social contexts and are discouraged (Kitayama et al., 2000, 2006). Due to the emphasis on group solidarity and social harmony, behaviors that prioritize the group, like emotional self-control, are highly valued (B. S. K. Kim et al., 2005). Recent empirical studies suggest that, among Asian Americans, emotional self-control is a significant predictor of help-seeking attitudes (e.g., P. Y. Kim et al., 2016; P. Y. Kim & Kendall, 2015). Similarly, research shows that Asian Americans typically have different ways of coping with emotions; it is more common to rely on familial and social support (Yeh & Wang, 2000) or use disengagement (Lei & Pellitteri, 2017) as a coping strategy. Given these findings, it makes sense that Asian Americans may be less likely to seek help from professionals for emotion-related problems.
Given the significant association between emotion-related variables and help-seeking attitudes, we decided to explore two emotion-related variables in relation to Asian American stigma and help-seeking attitudes: emotion regulation and emotion socialization. Emotion regulation is the ability to control one’s emotional state; it includes the ability to modulate, evaluate, and monitor emotions through both explicit and implicit processes (Thompson, 1994). Emotion regulation has been associated with help-seeking attitudes among undergraduate psychology students such that emotion dysregulation is associated with more negative help-seeking attitudes (Limowski et al., 2023). Relatedly, low levels of emotional competence or the ability to identify, describe, understand, and manage emotions in an effective and non-defensive manner (Ciarrochi et al., 2002; Mayer et al., 2001) has been associated with a decreased likelihood of seeking help from both close networks and professionals (Ciarrochi et al., 2003). Both these findings suggest that the ability to identify, describe, and control emotions is crucial to help-seeking intentions. More specific to our study, in the Asian American context, various emotion variables have been found to be associated with help-seeking. For example, among Asian American college students, Lei and Pellitteri (2017) found that emotional intelligence (i.e., the ability to manage one’s own and others’ emotions) was a significant predictor of seeking family support for emotion-related problems. Based on these findings, it seems plausible that those who are effective in emotion regulation would be protected against the negative influence of self-stigma on help-seeking attitudes. As such, we examined emotion regulation as a moderator in the self-stigma and help-seeking attitudes association.
While emotion regulation and competence are very personal and internal processes, we posit that explicit emotional processes, such as emotion socialization, can play a role in the examined association as well. Emotion socialization refers to the indirect and direct ways external, environmental factors (e.g., parents or caregivers) shape one’s experience and expression of emotion (Klimes-Dougan et al., 2007). A child’s first and most influential message(s) about which emotions are socially acceptable to exhibit and how to express emotions typically come from their parent(s) or caregiver(s) (i.e., parental emotion socialization; Halberstadt, 1991). For example, emotion coaching practices, or those that validate emotional expression, teach emotion labeling, and support emotion coping, indicate to a child that specific emotions are acceptable to express. Emotion dismissing practices, or those that ignore and minimize emotions, indicate to a child that specific emotions are undesirable and harmful and, thus, should be avoided (Gottman et al., 1997). More specific to our study, research suggests that cultural differences influence the larger behavioral cultural norms and expectations that are transmitted from parents or caregivers to their children, and this is evident by which emotion socialization practices are prevalent across cultures. Compared with White parents, Asian American parents are more likely to emphasize emotional moderation (Tsai et al., 2002), more likely to use an “emotion-criticizing style” (i.e., emphasize emotions as a ramification of social interactions and to teach the child a lesson about emotional norms expectations; Wang, 2001), and less likely to encourage emotional expressivity (Zahn-Waxler et al., 1996). While no studies, to our knowledge, examine the relationship between emotion socialization and help-seeking, various emotion variables have been found to be associated with help-seeking (i.e., emotional openness, Komiya et al., 2000; emotional competence, Ciarrochi et al., 2003; emotional intelligence, Lei & Pellitteri, 2017). Given this, we seek to further explore the possible relationship between parental emotion socialization and help-seeking attitudes.
For both emotion socialization and emotion regulation, we were interested specifically in how these variables might interact with self-stigma to predict help-seeking attitudes. We reasoned that more effective regulation and socialization experiences would protect against the negative influence of self-stigma on help-seeking attitudes. This is because, even while self-stigma levels might be high, strong emotion regulation abilities may provide individuals with effective emotion coping skills that will allow them to recognize the effectiveness of professional help-seeking. In line with this argument, emotional competence has been associated with help-seeking intentions for suicidal thoughts among college students (Ward-Ciesielski et al., 2019), and Ward-Ciesielski and colleagues (2019) suggest that this is due to increased access and utilization of various emotional coping strategies. Ciarrochi and Deane (2001) also found that college students who feel less skilled at managing their emotions are less willing to seek help from both professional and nonprofessional sources. Similarly, we posit that if children experience positive emotion socialization (i.e., emotion coaching) growing up, they will likely have higher levels of emotional awareness and understanding of their emotional experiences. In other words, because emotional expression was openly modeled for these individuals, we posit that they will view professional help-seeking as a positive and effective emotional outlet for experiencing both negative and positive emotions. Therefore, we argue that with these heightened levels of emotional awareness, individuals with positive emotion socialization experiences can overcome any internalized stigma they may otherwise hold toward professional help-seeking. That is, their experiences of emotion socialization serve as a protective factor against self-stigma because they have seen these methods of emotion regulation work effectively before.
Religious Coping
Given that this study was conducted on a Christian liberal arts campus with majority (but not exclusively) Christian students, we decided to explore the role of religious coping in relation to stigma and help-seeking attitudes among Asian American college students. Religious coping can be understood as the utilization of sacred or spiritual resources for coping with stressful life situations (Pargament et al., 2000). A popular conceptualization of religious coping includes both positive elements (i.e., positive religious coping), such as the reliance on spiritual communities and reframing of stressors from a spiritual perspective, and negative elements (i.e., negative religious coping) such as the focus on punishment and attribution of circumstances to demonic forces (Pargament et al., 2011). In this study, given our emphasis on protective factors against stigma’s influence on help-seeking attitudes, we explored the role of positive religious coping only. Specifically, we investigated whether the use of positive religious coping might alter the empirical relation between the self or internalized stigma of help-seeking and attitudes toward seeking psychological help among Christian Asian American college students.
On one hand, the argument could be made that the utilization of religious coping can lead to less favorable professional help-seeking outcomes. Although we are unaware of any studies that examine religious coping and help-seeking attitudes in Asian American samples, prior studies with related religiosity variables, or other non-White samples, provide some insight. For example, religious coping was associated with less likelihood of having utilized professional counseling in a sample of Black Americans (Avent Harris et al., 2021). Similarly, in a qualitative study, Catholic secular priests reported increased stigma and hesitation about seeking psychological help stemming from their religiosity (Pietkiewicz & Bachryj, 2016). Finally, the literature on spiritual bypass—the idea that religious individuals might “use their religious or spiritual beliefs, values, and practices to keep from dealing with threatening personal issues” (Fox et al., 2020, p. 179)—suggests that such an approach can be related to unfavorable help-seeking attitudes (Fox et al., 2020). As such, it seems plausible that for Asian American Christians who tend to use religious coping as a way to handle stressors, the idea of seeking psychotherapy might be viewed less favorably. Extending this to a moderation argument, it is also plausible that those with a high level of religious coping might be even more prone to experiencing the negative influence of internalized stigma of mental health counseling on their help-seeking attitudes.
On the other hand, one could also argue that religiosity and related constructs could lead to a more accepting attitude toward professional counseling, even in the face of self-stigma. For example, in a qualitative study, Mayers et al. (2007) noted that participants who sought professional therapy viewed the process as compatible with their spiritual lives and as a way of fortifying their faith. This recent perspective of compatibility between the Christian faith and professional counseling is consistent with the larger societal movement in the United States to destigmatize mental health in Christian communities, as illustrated by a recent Christianity Today article on how one can make sense of antidepressants from a Christian perspective (K. Lee, 2023). Moreover, in the Asian American Christian community, there has been a concerted effort to discuss mental health more openly, with the ultimate goal of destigmatizing mental illness and seeking treatment for it (e.g., see Asian American Christian Collaborative’s [n.d.] efforts). As such, those who rely on God to cope with psychological distress might also view counseling as a meaningful process, a way to strengthen their spiritual health, and a God-given intervention to alleviate emotional and mental suffering. Extending this to the moderation argument, it is feasible that those who engage in higher levels of religious coping might also be protected against the deleterious influence of self-stigma on help-seeking attitudes; that is, they might express more favorable help-seeking attitudes because of spiritual or religious factors, despite the fact that they might have some internalized stigma about the process of seeking professional help.
In sum, we explored religious coping as a moderator in our study. Specifically, we explored whether religious coping would moderate the mediation model specified earlier by moderating the inverse relation between self-stigma and help-seeking attitudes. We did not specify the nature of moderation (suppression or amplification) given the possibility that it could go either way.
Hypotheses
Method
Participants
Participants were 105 self-identified Asian American undergraduate students (Mage = 20.26, SD = 2.92; 74 females, 25 males, five non-binary/other, one missing) from a Christian university located in the Pacific Northwest region of the United States. Participants were allowed to self-report one or more ethnicity; the ethnicities recorded were Filipina/o (n = 35), Chinese from mainland China (n = 19), Japanese (n = 16), Korean (n = 13), Vietnamese (n = 11), Hong Kongese/Hong Konger/Chinese from Hong Kong (n = 8), Indian (n = 7), Cambodian (n = 5), Taiwanese/Chinese from Taiwan (n = 5), Indonesian (n = 1), Laotian (n = 1), Malaysian (n = 1), and Other (n = 11). The majority of participants were born in the United States (n = 85), and on average, participants reported living in the United States for 18.00 (SD = 5.10) years. The majority of participants also reported being second generation (born in the United States; parents immigrated to the United States; n = 58), but participants also reported being third generation (born in the United States; parents born in the United States; n = 18), 1.5 generation (foreign-born but raised primarily in the United States [immigrated at age 12 or younger]; n = 11), fourth generation of higher (born in the United States; parents, grandparents [or more] born in the United States; n = 10), and first generation (foreign-born and immigrated to the United States; n = 8). Participants reported the following religions: Protestant Christian (n = 41), Catholic Christian (n = 29), no religion (n = 14), Buddhist (n = 5), Muslim (n = 3), Hindu (n = 1), and Other (n = 11). Participants were also asked the highest level of school completed and reported the following educational levels: some college but no degree (n = 41), high school diploma or general educational development (GED) (n = 33), Associate’s degree (n = 25), Bachelor’s degree (n = 5), and Master’s degree (n = 1). Finally, 65 participants reported that they had not previously received mental health counseling while 40 participants reported that they had.
In addition to the general demographic variables, participants were asked demographic variables relating to their upbringing. Participants reported that an average of 2.10 (SD = 0.73) parental figure(s) or caregiver(s) were present growing up. Participants were then asked to select the type of parental figure(s) that were present when growing up; if participants grew up with three or more parental figures, they were instructed to choose the two that played the most influential role in their emotional development. When asked about the parental figure(s) or caregiver(s) that were present when growing up, the majority of participants reported growing up with a mother and father figure (n = 95); participants also reported growing up with a mother figure only (n = 8), a father figure only (n = 1), and two mother figures (n = 1).
Recruitment and Procedures
Participants were recruited via email with a list, provided by the Registrar’s office, of all Asian American students enrolled at the current institution. From the email announcement, students who wished to participate clicked on a link that took them to the online Qualtrics survey. The online survey consisted of demographic questions and study measures. For participation in this study, participants were entered into a drawing for a single prize of a $250 Amazon gift card. All participants were treated according to the ethical standards of the American Psychological Association.
A total of 135 individuals accessed our survey. Of these participants, 22 participants who left one or more of the study measures entirely blank were removed. In addition, seven participants were deleted for not answering the question “Please select the type of parental figure(s) present growing up” as instructed. Finally, one participant who did not identify as Asian American was removed. In the final data set, only three cases had missing data; two cases had one item missing, and one case had two items missing. Little’s (1988) test was nonsignificant, χ2 = 352.44, p = .999, suggesting that the data were missing completely at random. After these data cleaning procedures, the final data set included 105 participants. All participants provided consent through the online questionnaire to participate in this study.
Measures
Close others’ stigma
The Perception of Stigmatization by Others for Seeking Help (Vogel et al., 2009) was created to measure how the stigma associated with seeking professional mental health treatment may be reflected in social interactions with others. The measure includes five items that reflect various types of social reactions others could have (e.g., behavioral, emotional, cognitive) to participants seeking psychological help. Participants read the statement, “Imagine you had a problem that needed to be treated by a mental health professional. If you sought mental health services, to what degree do you believe that the people you interact with would _____.” before answering each item on a 5-point scale (1 = not at all, 5 = a great deal). Higher scores indicated greater perceived stigmatization from one’s social network. Example items include “React negatively to you” and “See you as seriously disturbed” (Vogel et al., 2009). Vogel et al. (2009) found this measure to have adequate reliability (e.g., test–retest reliability of .82) and concurrent validity (e.g., association with three different stigma measures). Our study yielded an internal consistency score of α = .89.
Self-stigma
The Self-Stigma of Seeking Help (Vogel et al., 2006) is a measure used to assess internalized stigma associated with seeking professional help. Participants were asked to rate their agreement with statements regarding the implications of seeking professional help on a 5-point scale (1 = strongly disagree, 5 = strongly agree). Higher scores indicate greater self-stigma. An example item includes “Seeking psychological help would make me feel less intelligent” (Vogel et al., 2006). This measure was found to have good construct (e.g., positive association with public stigma) and criterion (e.g., negative association with benefits of disclosing emotional problems with therapists) validity (Vogel et al., 2006). In addition, Vogel et al. (2006) also found adequate reliability with reliability coefficients ranging from .89 to .91. This measure demonstrated good internal consistency in the current study, α = .86.
Help-seeking attitudes
The Mental Help Seeking Attitudes Scale (MHSAS; Hammer et al., 2018) assesses one’s attitudes toward mental health services. This scale includes nine items that participants rate on a bipolar semantic differential scale from −3 to 3, with 0 indicating “undecided,” but for research purposes, the scores are translated to a scale of 1 to 7 (Hammer et al., 2018). Higher scores indicate more positive attitudes toward help-seeking. Participants read the statement, “If I had a mental health concern, seeking help from a mental health professional would be. . .” before responding to each item. Sample items include “effective-ineffective” and “healing-hurting” (Hammer et al., 2018). The MHSAS has demonstrated good internal consistency, convergent validity, and test–retest reliability among a sample of community-dwelling adults (Hammer et al., 2018). The internal consistency of this measure for the current sample was good, α = .95.
Emotion socialization
The Emotions as a Child–Youth Report (EAC; Magai & O’Neal, 1997) is a measure that assesses an individual’s perception of their parents’ emotion socialization practices for various emotions. Guo et al. (2017) psychometrically revised this measure to include supportive and unresponsive emotion socialization strategies; in the current study, we used the supportive strategies items only (seven items) and focused on the emotions of sadness and anger. Participants were asked to recall a time when they were angry or sad and then rate the likelihood that their parent(s) or caregiver(s) would respond in a certain way (i.e., use a socialization strategy). Participants responded on a 5-point scale (1 = never, 5 = very often) with higher scores indicating greater use of each socialization strategy for the emotion being measured. An example item includes “When I was angry/sad, my parent asked me what made me angry/sad” (Magai & O’Neal, 1997). This measure has been found to have acceptable convergent validity (e.g., association with parent–child connectedness) and test–retest reliability (e.g., correlations ranging from .54 to .83 for sadness and .57 to .82 for anger) among an adolescent and adult sample (Guo et al., 2017). For our analysis, we decided to average across the sadness and anger items, and across the parent(s) or caregiver(s), resulting in a total score. As such, because of the way we scored the emotion socialization variable, it did not make sense to compute the internal consistency of the total score, and therefore, we do not report it here.
Emotion regulation
To measure emotion regulation, the current study utilized the Lack of Emotional Awareness subscale of the Difficulties in Emotion Regulation Scale (Gratz & Roemer, 2004). This subscale has five items and is designed to measure awareness and understanding of emotions. Participants were asked to indicate how often each item applied to them on a 5-point scale with 1 being never and 5 being almost always. Higher scores indicate greater access to emotion regulation strategies. Although the original Gratz and Roemer (2004) article recoded scores so that higher scores indicated greater emotion dysregulation, for the purposes of our study, we decided to use the original, straight-coded scale so that high scores indicate more positive emotion regulation. In addition, as the subscale we used was all positively worded and in the same direction, we did not recode participants’ answers. A sample item includes “When I am upset, I acknowledge my emotions” (Gratz & Roemer, 2004). Gratz and Roemer (2004) report good internal consistency, good test–retest reliability, and adequate convergent and predictive validity. In this study, this measure demonstrated good internal consistency, α = .83.
Religious coping
The Brief RCOPE (Pargament et al., 2011) assesses one’s utilization of spiritual or religious resources. We set up our Qualtrics survey so that only those who identified as Christian (n = 70) were given the Brief RCOPE. The scale includes seven items (1 = not at all, 4 = a great deal) that consist of positive religious coping and seven items that make up negative religious coping; in our study, we used the positive religious coping scale only, with higher scores indicating more tendency to rely upon the utilization of reliance and trust of the sacred for coping. The Brief RCOPE has demonstrated good psychometric properties (Pargament et al., 2011), and it has been used with Asian American samples (e.g., P. Y. Kim et al., 2015). Internal consistency of the Brief RCOPE for this study was good, α = .94.
Results
Preliminary analysis
Table 1 displays the bivariate correlations between the study variables. The variables significantly correlated with the outcome variable of help-seeking attitudes were close others’ stigma (r = –.23, p = .017), self-stigma (r = –.42, p < .001), and emotion regulation (r = .37, p < .001).
Correlations and Descriptives for the Study Variables.
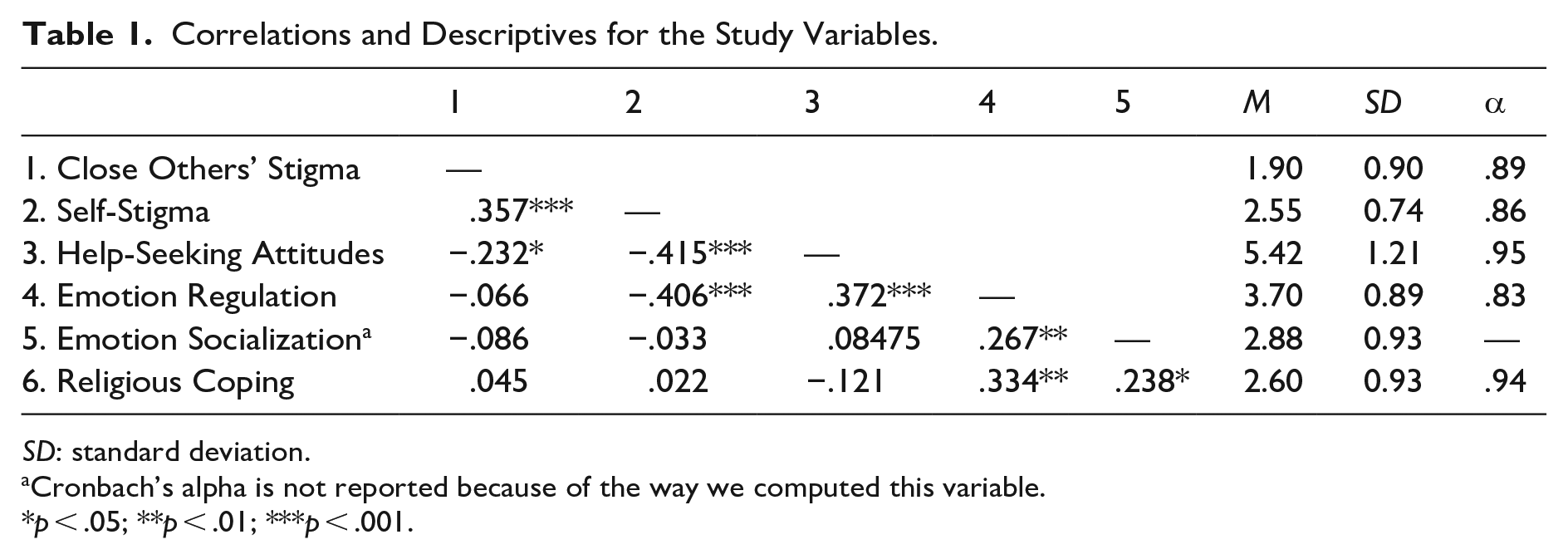
SD: standard deviation.
Cronbach’s alpha is not reported because of the way we computed this variable.
p < .05; **p < .01; ***p < .001.
Simple mediation analysis
Next, we tested our mediation prediction using the PROCESS macro (Hayes, 2013) in SPSS v. 28, which provided 95% bias-correlated (BC) confidence intervals (CIs) for the indirect effect based on 5,000 resamples. We hypothesized that self-stigma would mediate the relationship between close others’ stigma and help-seeking attitudes. Specifically, we predicted that close others’ stigma would positively predict self-stigma, which, in turn, would negatively predict help-seeking attitudes. Counseling experience was included as a covariate in this model. Results indicated that the indirect effect of close others’ stigma on help-seeking attitudes through self-stigma was statistically significant (b = –.205; BC 95% CI = [–.380, –.073]). Specifically, close others’ stigma was a positive and significant predictor of self-stigma (b = .290, t = 4.00, p = .0001), and self-stigma was a significant and inverse predictor of positive help-seeking attitudes (b = –.708, t = –4.32, p < .001). Therefore, the mediation model of close others’ stigma predicting help-seeking attitudes through self-stigma was found significant in this study.
Moderated mediation analyses
After establishing that the mediation model (close others’ stigma → self-stigma → help-seeking attitudes) was statistically significant, we conducted three moderated mediation analyses (i.e., conditional indirect effects) to test whether the indirect effect would vary according to levels of emotion regulation, emotion socialization, and religious coping. Specifically, we tested the conditional indirect effect in which each moderator moderated the b path (mediator to outcome variable, or self-stigma → help-seeking attitudes) in the mediation model using PROCESS in SPSS v. 28, which is Model 14 in Hayes (2013). We used bootstrapping with 5,000 resamples to estimate our confidence intervals. To determine whether there was as significant moderated mediation, we examined the significance of the index of moderated mediation provided by PROCESS, which represents the linear relationship between the moderator and the indirect effect; this was determined to be statistically significant if the bootstrapped confidence interval did not include a 0 (Hayes, 2013).
Difficulties in emotion regulation as a moderator
We examined whether difficulties in emotion regulation (moderator) might interact with self-stigma (mediator) to predict help-seeking attitudes (outcome variable) in the mediation model. The results revealed that the index of moderated mediation for difficulties in emotion regulation was not statistically significant, as its CI [−0.18, 0.10] contained a 0 (index = –.02). Emotion regulation was not a significant moderator of the others-stigma → self-stigma → help-seeking attitudes relationship.
Emotion socialization as a moderator
We examined whether difficulties in emotion socialization (moderator) might interact with self-stigma (mediator) to predict help-seeking attitudes (outcome variable) in the mediation model. The results revealed that the index of moderated mediation for emotion socialization was not statistically significant, as its CI [−0.19, 0.04] contained a 0 (index = –.05). Therefore, we concluded that emotion socialization was not a significant moderator of the others-stigma → self-stigma → help-seeking attitudes relationship.
Religious coping as a moderator
Finally, we examined whether religious coping (moderator) might interact with self-stigma (mediator) to predict help-seeking attitudes (outcome variable) in the mediation model. Because the RCOPE (Pargament et al., 2011) was only administered to self-identifying Christians, the sample size for this moderated mediation analysis included 70 participants. Table 2 displays the moderated mediation results associated with religious coping. As expected, the simple mediation pattern reported earlier on the whole sample (N = 105) was replicated in the moderated mediation results: Others’ stigma was a significant predictor of self-stigma (b = 0.33, t = 3.63, p = .001) and self-stigma significantly predicted help-seeking attitudes (b = −0.86, t = –4.07, p < .001).
Regression Results for Conditional Indirect Effect: Close Others’ Stigma → Self-Stigma → Help-Seeking Attitudes. Moderator: Religious Coping (N = 70). a

SE: standard error; SD: standard deviation; CI: confidence interval.
Previous experience with counseling coded: 0 = no; 1 = yes.
N = 70 to include only Christian participants who completed the RCOPE.
Next, we examined whether religious coping moderated this simple mediation model (i.e., conditional indirect effect); specifically, we were interested in how religious coping might interact with the mediator (self-stigma) to predict the outcome variable (help-seeking attitudes) in the mediation model. The index of moderated mediation of 0.17 was statistically significant, as its CI did not contain a zero [0.01, 0.40]. The indirect effects at three different levels of religious coping (−1SD, M, and +1SD) revealed that at both −1SD (b = −0.44 [−0.76, −0.17]) and M (b = −0.28 [−0.52, −0.09]) of the moderator, the indirect effects were statistically significant. However, at +1SD, the indirect effect was rendered non-significant, b = −0.12 [−0.42, 0.13].
The same trend was found when examining the association between the interaction term Self-Stigma × Religious Coping and help-seeking attitudes, and we display this interaction effect in Figure 1. At low (−1SD; b = −1.35, t = –4.76, p < .001) and medium (M; b = −0.86, t = −4.07, p = .0001) levels of religious coping, the mediator–outcome association was statistically significant, but at high (+1SD; b = −0.37, t = −1.39, p = .17) levels of religious coping, the association was rendered nonsignificant. In sum, the results suggested that religious coping is a significant moderator of the others-stigma → self-stigma → help-seeking attitudes associations, and the specific mechanism for the moderation involves the weakening of the inverse relation between self-stigma and help-seeking attitudes in the mediation model.
Discussion
This study was an empirical examination of Asian American students’ perception of stigma from close others (close others’ stigma), internalized stigma, and help-seeking attitudes. In addition, emotion regulation, emotion socialization, and religious coping were examined as moderators of the mediating relation. Our findings revealed that (a) the hypothesized mediation model (close others’ stigma → self-stigma → help-seeking attitudes) was statistically significant, and (b) for Christian students, religious coping was a significant moderator of the mediation model. Although emotion regulation and emotion socialization were nonsignificant moderators, emotion regulation was a significant predictor of help-seeking attitudes.
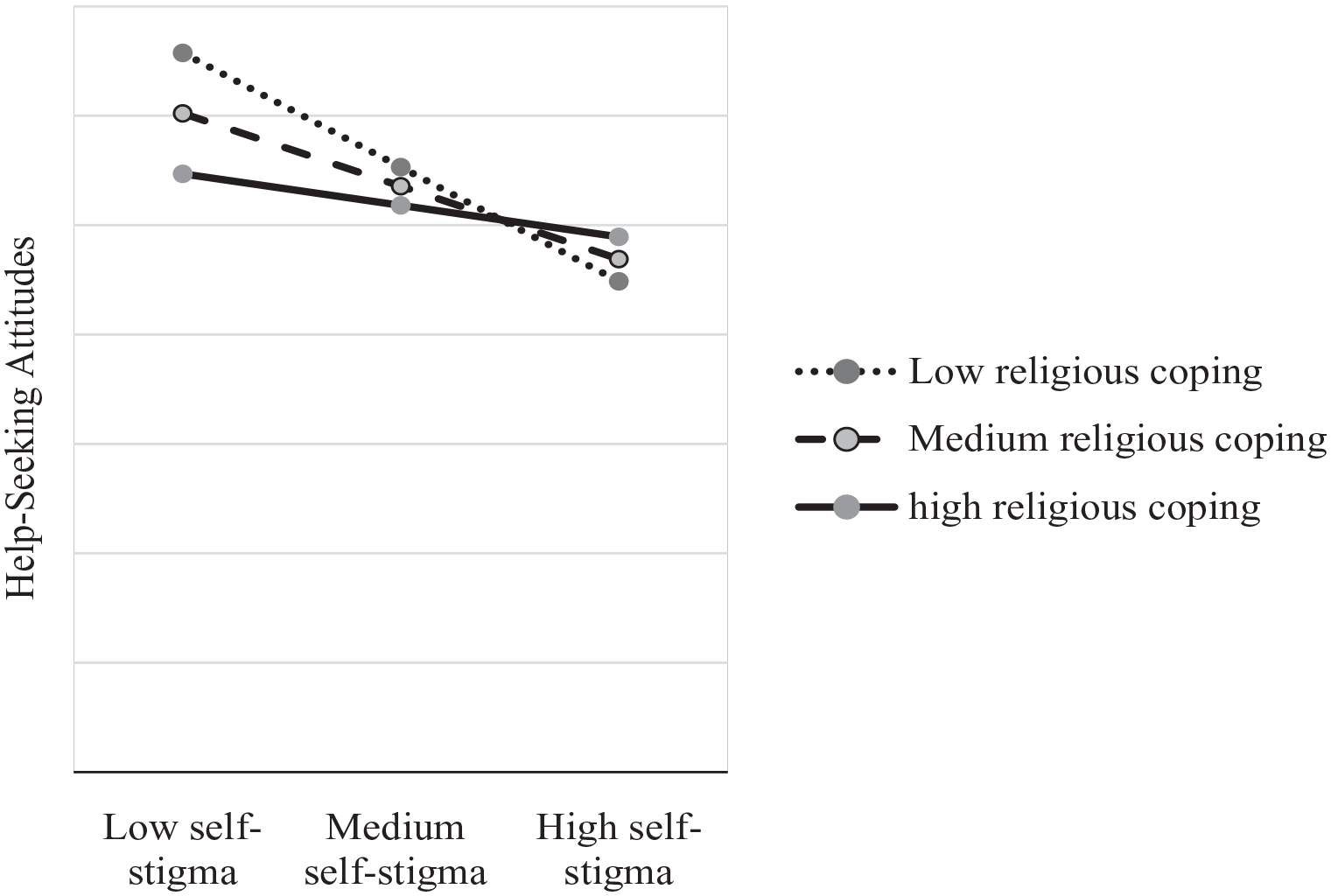
Self-Stigma × Religious Coping predicting help-seeking attitudes.
Explanation of findings
Consistent with prior empirical studies (e.g., Choi & Miller, 2014; P. Y. Kim & Yon, 2019; E. J. Lee et al., 2014), our study found that, among Asian American college students, stigma perceived from close relationships is influential in shaping both internal stigma and attitudes toward seeking psychological help. For Asian American college students who might be affected by cultural values that place a strong emphasis on collectivism and conforming to norms (B. S. K. Kim et al., 2005), opinions about help-seeking held by close relationships might be especially influential in help-seeking decisions (P. Y. Kim & Park, 2009). Although our finding of this indirect effect is a replication of prior associations, our study also contributes to the literature by using a measure with better psychometric properties (MHSAS; Hammer et al., 2018) compared with what has been the norm in the Asian and Asian American psychological help-seeking literature (ATSPPH-SF; Fischer & Farina, 1995). We encourage future researchers to continue to replicate and extend Asian American help-seeking attitudes literature using measures such as the MHSAS.
We also found that religious coping significantly moderated the mediation model for Christian participants, such that the relationship between self-stigma and help-seeking attitudes was altered based on positive religious coping. This finding is partially consistent with prior literature that has argued for the facilitative role of religion on help-seeking processes (e.g., Mayers et al., 2007) but inconsistent with those that suggest that religion might be associated with less help-seeking (e.g., Avent Harris et al., 2021). What is notable in our finding is that the facilitative role of religious coping on help-seeking attitudes is complex; at lower levels of self-stigma, religious coping does not seem to be as impactful on help-seeking attitudes, compared with higher levels of self-stigma (see Figure 1) where religious coping seems most protective. More broadly, for those who have a higher level of negative perception of self when seeking psychological help, more intensive religious coping might lead to more favorable attitudes toward seeking help, compared with those with the same level of negative self-stigma but with less religious coping. That is, it is not the absence of self-stigma of counseling but rather the presence of religious coping that can be most beneficial for help-seeking. As such, this suggests some interesting implications for how intervention and prevention programs might be designed. However, the effect of religious coping on help-seeking found in this study is specific to Christianity. Although religious coping among religions outside of Christianity may have similar effects on help-seeking, generalizations of these findings to other religions should be made cautiously as religious coping practices of other religions were not examined in this study.
Contrary to our hypotheses, emotion regulation and emotion socialization were not significant moderators of the mediation model. These findings are inconsistent with the literature that suggests that “positive” emotion socialization experiences and high levels of emotional awareness may provide individuals with a large repertoire of coping skills (Ward-Ciesielski et al., 2019), which we reasoned might allow them to “push” past internalized stigma and view help-seeking more favorably. We did find, however, that emotion regulation directly and significantly predicted favorable help-seeking attitudes. This relationship makes sense given the prior literature demonstrating that adolescents with low levels of emotional awareness (Ciarrochi et al., 2002) and emotional competence (Ciarrochi et al., 2003) displayed the lowest intentions to seek help. More specific to Asian American samples, emotion-related variables like emotional self-control (P. Y. Kim et al., 2016; P. Y. Kim & Kendall, 2015) and emotional intelligence (Lei & Pellitteri, 2017) have demonstrated important relations to stigma and help-seeking attitudes. At the same time, although these studies examined help-seeking intentions and related emotional variables among Asian Americans, they did not examine emotion regulation specifically. Thus, our findings add to the current literature by showing that emotion regulation is associated with help-seeking attitudes among Asian Americans. Taken together, it is evident that the role of emotion in stigma and mental health counseling attitudes among Asian Americans is complex and needs to be unpacked further.
Implications
Our religious coping findings suggest some possible implications for both prevention and intervention efforts among Christian Asian American college students. In particular, our study implies that being attuned to the religious coping tendencies of Christian Asian American students might be a fruitful emphasis in accurately gauging beliefs and attitudes around mental health counseling. This might be especially true for Asian American students who are trying to make sense of stigma—both external and internal stigma—toward seeking psychological services; that is, encouraging Asian American students to draw strength from their Christian religion might be especially effective in increasing favorable views of mental health counseling, especially if done as a counter to heightened levels of stigma of counseling. More broadly, our study suggests that religion can facilitate the attractiveness of seeking professional psychological help and that the Christian faith can and should be compatible with the notion of seeking professional counseling. To increase counseling center utilization, counselors conducting outreach with Asian American students should explore intentional ways to incorporate Christian beliefs to help make mental health counseling more compelling. However, this should be done with caution for non-Christian Asian Americans, as it cannot be assumed that religious coping will have the same positive effects among non-Christians as it did with Christian Asian Americans in this study. Similarly, our findings on the direct relationship between emotion regulation and help-seeking suggest the importance of emotional literacy and education, especially among Asian Americans. Higher education institutions, and university counseling centers more specifically, should endeavor to provide education on emotional awareness and adaptive emotion regulation strategies. This could include disseminating how-to information on recognizing emotional experiences and managing emotions effectively and accurately. Not only will this allow students to recognize dysfunctional emotional experiences, but it will increase their positive help-seeking attitudes and potentially increase the utilization of college campus counseling centers. We recognize that this last implication assumes that emotion regulation leads to help-seeking attitudes, but we also acknowledge the possibility that help-seeking can increase emotion regulation.
Limitations and future directions
There were several methodological and theoretical limitations of our study. First, as mentioned above, neither causality nor directionality can be established given the cross-sectional design of the study. Along the same lines, we recognize that the quantitative nature of this study can only provide an overview of the study’s variables, and the correlations between them, rather than a complex understanding of religious, emotional, and help-seeking experiences that qualitative data could have produced. In the future, studies should utilize alternative research designs, including qualitative designs, to capture the depth of how religious coping might shape Asian American help-seeking. Second, this study utilized self-report measures to quantify emotion socialization that required participants to recall retrospective information from childhood. Thus, participant responses may be subject to memory and reporting biases that may influence the validity of their responses. In addition, when calculating total emotion socialization (EAC) scores, the current study averages across (a) sadness and anger items and (b) parental figure(s) or caregiver(s) items. This scoring approach may lack psychometric support as it prevented us from reporting an index of reliability for this measure. Future studies should employ strategies to reduce reporting bias, such as also obtaining parent or caregiver reports, and reporting separate scores for both emotions and parental figures. Third, although the sample was in many ways representative of the institution where data collection took place (i.e., Christian, college students, East Asian, female), the experiences and attitudes of the participants in this study should be generalized with caution. Future studies should seek to intentionally recruit a diverse Asian or Asian American sample on dimensions of Asian ethnicity, acculturation and enculturation, gender, religion, and age in order to examine how one’s complex and intersecting identities may influence their help-seeking experiences. Fourth, our study focused on only one aspect of religiosity—religious coping—when there are many other dimensions to consider. While religious coping can be described as an important functional aspect of religion, there are also dispositional or intrapersonal aspects of religion that should be captured when examining religiosity (Tsang & McCullough, 2003). Relatedly, this study did not examine negative religious coping (Pargament et al., 2011), which is also relevant, especially in the context of difficult experiences (e.g., see P. Y. Kim et al., 2015). In addition, religious coping was only measured among Christian participants in this study; readers should not assume that religious coping functions in the same way across other religions. We encourage future researchers to consider a fuller conceptualization of religiosity in relation to help-seeking attitudes of Asian Americans, especially among those of other faiths. Finally, it is possible that our method of assessing for close others’ stigma—asking participants to think about “people you interact with,” without specifying the specific relationship(s)—resulted in participants keeping in mind very different types of relationships when providing the responses to the Perceptions of Stigmatization by Others for Seeking Help scale (PSOSH; Vogel et al., 2009). There are empirical examples of the PSOSH being used to ask about specific types of people (e.g., “unit leaders/command,” Blais et al., 2023; a parental figure, Surapaneni et al., 2022) and their stigmatizing attitudes toward seeking professional help. This type of specificity might be especially promising to elucidate the different levels of stigma and their roles among Christian Asian Americans, depending on who is stigmatizing.
Conclusion
We examined the moderating role of emotion regulation, emotion socialization, and religious coping on the association between close others’ stigma and help-seeking attitudes through self-stigma among Asian American undergraduate students. Religious coping strengthened the indirect effect of others’ stigma on help-seeking attitudes through self-stigma, suggesting that religion may play an important role in the formation of attitudes toward pursuing mental health treatment. Although the direct relationship between emotion regulation and help-seeking attitudes was positive and significant, emotion regulation and emotion socialization did not moderate the proposed mediation model. These findings suggest that emotion variables have a complex role in help-seeking attitudes; however, more research is needed to more specifically clarify how emotions interact with stigma to influence help-seeking. We are hopeful that these findings add to the current literature that examines how Asian Americans experience stigma and professional help-seeking.
Footnotes
Authors’ Note
This article is based on the first author’s independent research project completed under the guidance of the second author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.