
Abstract
People with depression are reluctant to seek professional help, with estimates indicating that over half of people with major depression in the community do not consult a health professional [1–3]. According to recent research, this reluctance is most evident with respect to help-seeking from mental health professionals [2,4,5]. Help-seeking from professionals may be influenced by stigmatizing beliefs. Some research has found that stigma is a barrier to professional help-seeking for depression [6–8], whereas other research has concluded that stigma does not have a significant impact [5,9,10]. Such contradictory findings may be due in part to the complexity of the concept of stigma, the resulting differences in the way in which it is measured and the relevance of these measures to the help-seeking context. Two forms of stigma –self stigma and perceived stigma –are believed to be important in the context of help-seeking.
Self stigma is said to exist when people have negative attitudes about themselves as a result of internalizing stigmatizing ideas held by society [11]. For example, people may perceive depression as being due to a weak personality. Such stigmatizing views may impact on help-seeking because sufferers do not wish to show their ‘weaknesses’ to others. Similarly, it is known that people who believe depression to be under personal control are less likely to endorse help-seeking for themselves [12].
Perceived stigma refers to the belief that other people hold stigmatizing ideas. Depressed people may believe that others will view and respond negatively to them if they seek help. Sufferers may be concerned about responses of the professionals from whom they seek help, the responses of other people who are aware of the helpseeking, or both. The influence of others' views seems to play a crucial role in help-seeking, with recommendations from significant others an important factor for those who have sought professional help [13,14]. Accordingly, it might be expected that help-seeking will be inhibited if other members of the community are perceived to hold negative attitudes to help-seeking.
The aims of this paper were to investigate: the likelihood of people seeking various sources of professional help for depression; community attitudes to help-seeking for depression and their beliefs about the attitudes of others; and the role of stigma in affecting the likelihood of seeking help.
Method
Participants
Seven thousand questionnaires were sent to a random selection of residents in an electorate in New South Wales, Australia. There were 1312 respondents (response rate of 19%), ranging in age from 18 to 89 years (M=50.9), comprising 496 men and 796 women. Fifty-eight per cent had completed 6 years of secondary schooling and an additional 23% held a bachelor's degree. Fifty-five per cent had personally experienced depression.
Instruments
The questionnaire included a vignette of a person, ‘John’ who met the DSM-IV minimum criteria for major depression. The vignette described John's symptoms and behaviours and included a diagnosis of depression. Respondents were asked for their attitudes in relation to the vignette.
Help-seeking intention (five items). Respondents were asked to indicate on a five-point scale ranging from ‘extremely likely’ to ‘extremely unlikely’, how likely they would be to seek help from each of five professional sources (general practitioner, counsellor, psychologist, psychiatrist and complementary practitioner) if they were depressed like John.
Self stigma (five items). Respondents were asked to indicate on a five-point scale ranging from ‘strongly agree’ to ‘strongly disagree’ how likely they would be ‘to feel embarrassed’ if they went to see each of five professional sources if they were depressed like John.
Perceived stigma (15 items). These items sought to identify respondents' views about the beliefs of health professionals and others toward help-seeking. Respondents were asked to indicate on a fivepoint scale whether they would be worried that they would be regarded in a condescending way by each of these five professional sources; whether they would be afraid they would be regarded as unbalanced or neurotic by each source; and whether they would worry that other people would think less of them for seeing a [health professional] for depression. The three relevant items were summed to form a measure of perceived stigma associated with help-seeking from each professional source.
Depressive symptoms. Current depressive symptoms were measured using the PRIME-MD PHQ-9 (Primary Care Evaluation of Mental Disorders Patient Health Questionnaire) [15], which asks about the experienced frequency of symptoms matching the DSM-IV criteria for major depression [16] over the previous 2weeks.
Personal experience of depression. Respondents were asked if they had personally experienced depression.
Demographics. Gender, age and education level of respondents were requested.
Analyses
Statistical analysis was carried out using SPSS 12.0. Pearson correlation coefficients were conducted and all reported associations above 0.08 were significant at the p<.01 level. A series of logistic regressions was run to determine the impact of stigmatizing beliefs on the likelihood of help-seeking from specific sources. The outcome variable of help-seeking likelihood from each source was dichotomized so that being ‘extremely likely’ or ‘likely’ to seek help were coded as 0 and being ‘extremely unlikely’, ‘unlikely’ or ‘not sure’ were coded as 1. Education was coded with less than a year 12 education as the reference category, and compared to year 12 and bachelor degree education.
Results
Help-seeking intention
The likelihood of seeking help varied according to the specific helpsource: general practitioners (GPs) (73%; 95% confidence interval (CI) 70–75%), counsellors (50%; 95% CI=46–52%), psychologists (40%; 95% CI=37–42%), psychiatrists (34%; 95% CI=31–36%) and complementary practitioners (37%; 95% CI=35–40%). Moderate to high correlations between the likelihood of seeking help from a counsellor and psychologist (r=0.68, 95% CI=0.65–0.71), counsellor and psychiatrist (r=0.55, 95% CI=0.51–0.59) and psychologist and psychiatrist (r=0.78, 95% CI=0.76–0.80) suggest that attitudes toward mental health professionals are shared to some degree. The association of help-seeking from a GP with that from a counsellor was lower (r=0.37, 95% CI=0.32–0.41), psychologist (r=0.40, 95% CI=0.35–0.45) and psychiatrist (r=0.40, 95% CI=0.36–0.45). The correlation between help-seeking from a complementary practitioner and other professionals were: GP (r=0.22, 95% CI=0.16–0.27), counsellor (r=0.38, 95% CI=0.34–0.43), psychologist (r=0.32, 95% CI=0.27–0.37) and psychiatrist (r=0.28, 95% CI=0.22–0.33). These suggest a general inclination toward help-seeking from professionals, but also some distinction in views toward mental health professionals compared to other help-sources.
Self stigma
Self stigma varied according to the source of help, with greater embarrassment associated with seeing mental health professionals, especially psychiatrists. Forty-four per cent (95% CI=41–47%) of respondents said they would feel embarrassed to see a psychiatrist. Figures for the others sources were: psychologist (38%; 95% CI=35–41%), counsellor (34%; 95% CI=32–37%), complementary practitioner (32%; 95% CI=29–35%) and GP (29%; 95% CI=26–31%).
Perceived stigma
Expectations of negative responses from professional help-sources were also evident in a substantial minority of respondents, with some differences found between the sources. The greatest condescension was expected from GPs (20%; 95% CI=18–23%) followed by psychiatrists (17%; 95% CI=15–19%), complementary practitioners (17%; 95% CI=15–19%), psychologists (16%; 95% CI=14–18%) and counsellors (16%; 95% CI=14–18%). A similar pattern emerged regarding beliefs that professionals would think them unbalanced or neurotic, with the greatest stigma expected from GPs (18%; 95% CI=16–20%), complementary practitioners (16%; 95% CI=14–18%), psychiatrists (15%; 95% CI=13–17%), psychologists (14%; 95% CI=2–16%) and counsellors (14%; 95% CI=12–15%).
Many respondents saw seeking professional help as risking stigma from other people. Forty-six per cent (95% CI=43–48%) of respondents believed others would think less of them for seeing a psychiatrist, psychologist (39%; 95% CI=36–41%), counsellor (32%; 95% CI=29–34%), complementary practitioner (27%; 95% CI=24–29%) and GP (21%; 95% CI=18–23%).
Effect of stigma on help-seeking
The initial unadjusted logistic regression model showed that perceived stigma and self stigma were significant predictors of helpseeking likelihood from each source. The other predictor variables were entered as a block, and subsequently, the variables of exposure to depression and current depressive symptoms were removed, as they were not significant predictors. The final model is shown in Table 1.
Odds ratios and significance levels for the associations of sociodemographic and attitudinal measures with likelihood of help-seeking from professional sources
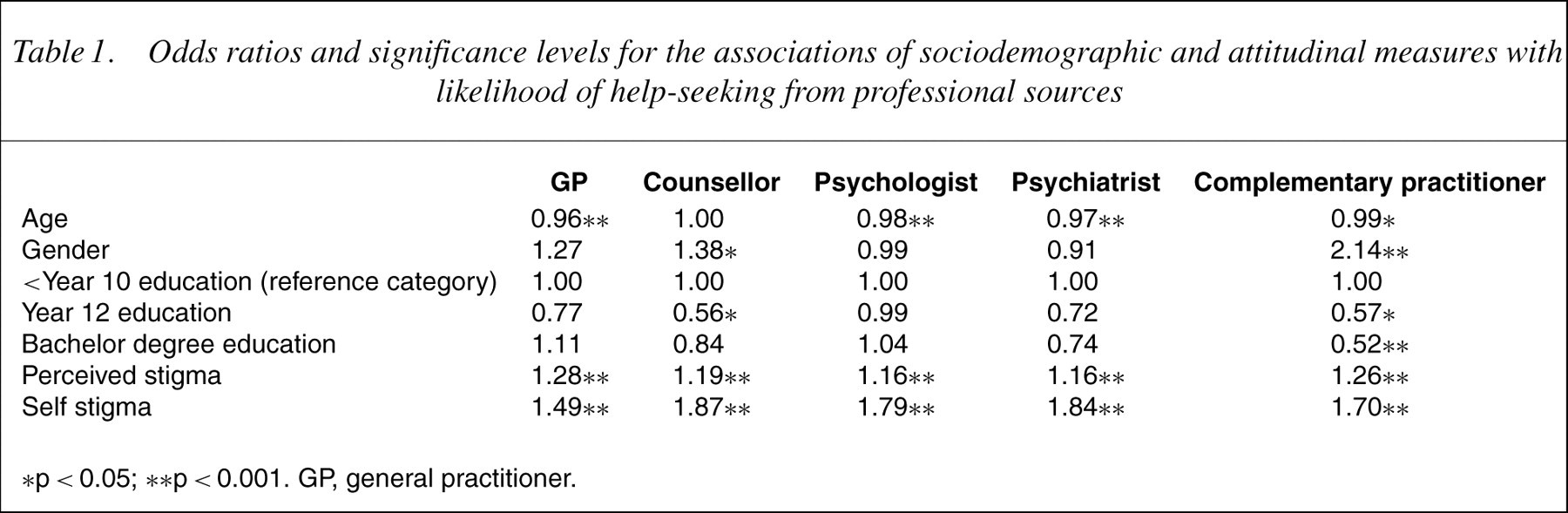
∗p <0.05; ∗∗p <0.001. GP, general practitioner.
Younger people reported being less likely than older people to seek help from every professional source except counsellors. Men were less likely than women to seek help from counsellors and complementary practitioners. People with a year 12 education were less likely than people of lower and higher educational levels to seek help from counsellors, and people with higher education levels were less likely to seek help from complementary practitioners. Both greater perceived stigma and self stigma reduced the likelihood of seeking help from all sources.
Discussion
This study found that self stigma and perceived stigma about help-seeking for depression is common and that both types of stigma reduce the likelihood of help-seeking from any professional source. The inhibitory effect of self-stigmatizing views was particularly strong. There is evidence that personal attitudes are more important than the disapproval of others in predicting intentions to seek help from ‘mental health professionals’ [17]. This study is consistent with such a conclusion, but extends previous findings by showing that the effect of self stigma on help-seeking exists for a wide range of helpsources including GPs, counsellors, psychologists, psychiatrists and complementary practitioners. Additionally, concerns that other people will respond negatively were also found to impact on help-seeking likelihood, so there is clearly a need to promote positive societal attitudes as well as improve self-attitudes.
Even though people felt least embarrassment and expected least stigma from others about help-seeking from GPs, some concerns were still evident. These stigmatizing beliefs are especially problematic because GPs may be the only feasible source of help in terms of cost and access [18,19]. Unwillingness to consult a GP may also prove a barrier to obtaining help from mental health specialists because of the existingmedical referral process in Australia. In such circumstances, people may not obtain professional help of any kind.
We should not be complacent about the relativewillingness of people to consult GPs because it is common for depressed people to present with somatic rather than psychological complaints [18] which can lead to incorrect diagnosis [20,21]. Additionally, GPs may lack the training, skills or time to detect and manage depression appropriately [18,22]. Therefore, it is important that people are comfortable about disclosing depression and consulting a mental health professional if necessary.
The differential sociodemographic findings may point to the need for awareness campaigns to be framed differently for various demographic groups. Of particular concern is the apparent reluctance of young people to seek professional help, a finding consistent with young people's preference to seek help from friends [23], which warrants further investigation and targeting of young people.
Some caution is needed in drawing conclusions because: help-seeking intention is not a perfect predictor of actual help-seeking behaviour; it cannot be assumed that people do hold the views they are perceived to hold; and voluntary participation restricts generalizability. Further research of a longitudinal nature is recommended and would also resolve the dilemma of causal direction. Irrespective, this study provides valuable insight into community beliefs about source-specific help-seeking for depression.