
Abstract
Novel psychoactive substances (NPSs) present a significant challenge to healthcare professionals working in Scotland. An area that has not previously been researched is student nurses’ feelings of knowledge and confidence in relation to NPS. This study aimed to provide data on this topic. An evidence-based presentation on NPS was produced. Five undergraduate mental health nursing students at a Scottish university were recruited as participants. They completed identical quantitative questionnaires assessing perceived levels of knowledge and confidence surrounding NPS pre- and postwatching the presentation. A focus group followed where the participants were asked how their perceived levels related to feelings of competence. The results showed that participants valued knowledge on clinical vigilance and awareness (CVA) over other themes measured, with it appearing to act as a lens by which to understand NPS-related phenomena observed in practice. These findings are explored in relation to the concepts of the theory–practice gap and the null curriculum. The author argues that knowledge pertaining to CVA may play a crucial role in helping to resolve the theory–practice gap in the context of NPS by facilitating nursing student understanding of the relative salience of knowledge and skills developed in other clinical contexts to this area of working, with this also acting as a vehicle by which NPS-relevant knowledge may be transferred from its place in the null and hidden curricula to that of the explicit curriculum. CVA is also considered alongside Rhodes and Lancaster's concept of evidence making and Race's idea of emergent causality, with the author arguing that CVA may help facilitate student nurses’ orientation toward attitudes consistent with the former and avoid problematization (in the Foucauldian sense) of relevant service users aligning to the latter.
Keywords
Introduction
The use of novel psychoactive substances (NPSs) in Scotland has been a notable public health concern for almost a decade (Scottish Government, 2016). Some evidence initially suggested that UK government legislation introduced in response to the emerging NPS phenomenon during the previous decade had achieved some success in countering its rise. For example, the introduction of Temporary Class Drug Orders in 2011 was found to have obstructed importation and distribution of several NPS, resulting in a temporary reduction in the number of patients being treated for acute toxicity from their consumption in Scotland (Pettie et al., 2018). Any success of such measures has proved to be short lived, however, as attested to by recent drug-related death (DRD) figures for Scotland. In 2020, of the record high 1,339 DRDs in the country, 872 (65.1%) had NPS as an implicated factor (National Records of Scotland, 2021). While subsequent DRD rates have reduced, NPS remain a contributory factor for a substantial proportion, with formally controlled benzodiazepines having involvement in 550 (46.9%) of 1,172 deaths in the latest available annual figures for 2023 (National Records of Scotland, 2024a). By far, the most common category of NPS implicated in recent Scottish DRDs are novel or “street” benzodiazepines such as etizolam (McAuley et al., 2022) and bromazolam (McAuley et al., 2023), with these being a contributory factor in 572 (48.8%) of the DRDs in 2023, as opposed to the 218 (18.6%) where prescribable benzodiazepines such as diazepam were implicated (National records of Scotland, 2024a).
Motivations for NPS use vary hugely according to popular individual drugs’ objective or subjective effect, availability or legal status among other factors, and these may evolve over time. The recent history of the synthetic cannabinoid receptor agonists (SCRAs) serves as an excellent case in point to help demonstrate this. SCRAs were originally developed in the 1960s as part of efforts to devise drugs that matched tetrahydrocannabinol's (the primary psychoactive in herbal cannabis) analgesic and anti-inflammatory properties though which did not exhibit the latter's psychoactive effects, with many developed SCRAs ultimately failing in this latter goal (Chung et al., 2021). In 2008, the SCRA JWH-018 was detected in herbal smoking preparations marketed in mainland Europe (European Monitoring Centre for Drugs and Drug Addiction, 2009). For some time after this point, this compound and a plethora of other SCRAs grew in popularity—especially among young people—with potency, licit status, perceptions of them being “safe” drugs, and wide availability cited as being explanatory factors in motivations for use (Fattore & Fratta, 2011). However, unlike THC—which acts as only a partial agonist of CB1 and CB2 receptors (Chung et al., 2021) —SCRAs very often are high or full agonists of the former (Darke et al., 2021) and in many cases also highly affinitive with the latter receptors (Wiley et al., 2017), which is theorized to account for SCRAs’ far more pronounced physical (Sachdev et al., 2019) and mental health (Hobbs et al., 2018) complications in adverse experiences of consumption than are generally seen after natural cannabis use. In the United Kingdom, SCRAs became criminalized in 2009 (Dargan et al., 2011), with this being “reinforced” (as it were) by the later 2016 Psychoactive Substances Act (PSA; Alexandrescu, 2020). Although this may have resulted in lower rates of use among younger people generally, it did not prevent SCRAs from finding a niche within two specific populations in the United Kingdom—people experiencing homelessness (Coombs et al., 2024) and those incarcerated within the criminal justice system (Grace et al., 2020). Indeed, qualitative research indicates that the enactment of the PSA served as a driver for increased use and harms from SCRAs among the UK's homeless population (Ralphs et al., 2021).
In these two populations, motivations for use differ in some regards to those noted for young people by Fattore and Fratta (2011). The author would typify additional motivations in the former groups as being more “functional” in nature, with nondetectability in drug testing and escape from the reality of the populations’ two respective situations being common to both (Gray et al., 2021; Ralphs et al., 2017), as well as relief from physical and psychological pain in the case of the homeless population (Coombs et al., 2024). In Scotland, SCRA use rates appear to have declined drastically in the general population subsequent to the introduction of the PSA while—simultaneously—dramatically increasing among its incarcerated people (Norman et al., 2020) to the point where its use is now postulated to be almost exclusive to those within the prison system of the country (Norman et al., 2021).
Alexandrescu and Spicer (2023) utilize the transition of SCRAs from the licit/gray market to illicit/black market sphere in the United Kingdom and subsequent uptake of them in the specified communities to illustrate what they characterize as the “stigma-vulnerability nexus.” Essentially, this is the argument that both stigma and vulnerability are highly correlated in contemporary political discourse on drugs, though that legislative measures to protect those categorized as vulnerable (in this case, enactment of the PSA to safeguard young people) may in fact inadvertently serve to deepen stigmatization of those already deemed as “other” or “abnormal” in society (so, the UK's homeless and incarcerated populations), even if the latter are—at least superficially—acknowledged to belong to the former category within said discourses (Alexandrescu & Spicer, 2023). Even if the entrenchment of stigmatization of some groups over others is taken out of the equation, the policy discourse and resultant legislative action in relation to NPS can still be viewed as troubling. Brown and Wincup (2020) discuss the development of the “vulnerable subject” within English legislative drug policy, noting that—as a whole—young people, the homeless and incarcerated populations in the context of NPS use generally are framed as vulnerable, though that such casting can simultaneously see increased criminal justice measures in relation to them. Ultimately, Brown and Wincup (2020) summarize that the conception of such groups as “special,” vulnerable populations in this manner inevitably contributes to their further stigmatization, casting them as subjects who necessitate coercive action to direct them toward the “straight and narrow path.” Although not specific to NPS per se, the current author notes at this juncture that a tension between the Westminster (i.e., United Kingdom as a whole) and Scottish governments as to the focus and direction of drug policy has existed for some time. Both health and justice policy are devolved to the Scottish government. However, under the Misuse of Drugs Act 1971—which applies to the entirety of the United Kingdom—policy relating to drugs are considered primarily as a criminal justice matter, changes to which are reserved to the Westminster government (Nicholls et al., 2022). The Scottish government has appealed to Westminster in this regard on several occasions, requesting leeway to pursue strategies more aligned to public health than the currently directive, criminal justice approaches in relation to drug policy, inclusive of decriminalization (Scottish Government, 2023), and the implementation of low-threshold treatment protocols such as safe consumption rooms (House of Commons Scottish Affairs Committee, 2019). Of the two examples mentioned, only the latter application has been successful and then only very recently (Scottish Government, 2025).
Evidence regarding the mental health impacts of NPS in the Scottish context is scarce. However, the limited extant literature suggests a negative association. One recent qualitative study of men incarcerated in Scottish prisons found that the interviewed sample felt that there was direct link between the use of SCRAs and increased psychiatric symptoms such as paranoia and aggression in their cohorts (Deuchar & Densley, 2024). A less contemporaneous audit of discharge letters from psychiatric services at one Edinburgh hospital found that although cases where NPS was identified as a factor in presentation only accounted for 6.6%, the NPS-using cohort was significantly more likely to display thought disorder and paranoia than their non-NPS using peers (Bennett et al., 2017).
Research regarding UK clinicians’ self-perceived levels of confidence and knowledge of treatment of NPS-related health conditions is limited. However, the extant body of work pertaining to this topic consistently suggests that UK-based healthcare workers feel underconfident and lacking in both knowledge and competence in NPS misuse treatment generally, as well as in comparison to orthodox substances of abuse (Guirguis et al., 2015; Owie et al., 2017; Ramos et al., 2020; Solomon & Guirguis, 2024; Wood et al., 2016). This is of particular concern in the context of nurses, given their instrumental role in both the identification and early management of adverse drug reactions initiated through NPS consumption (Addison et al., 2018; Brewer & Collins, 2014).
One hitherto unexplored area in the literature is self-perceived knowledge and confidence of preregistration nurses in relation to NPS. The overarching objective of the current research was to address this deficit in data pertaining to undergraduate nursing students’ preparedness for practice in this area. Using a mixed methodological approach, participants’ feelings of knowledge and confidence in relation to the treatment of NPS harms to health prior to and postdelivery of a specifically tailored educational resource were gathered, with the intention of helping to direct and inform future resources of a similar nature. Due to the exploratory nature of the research area, a small sample of participants for which a relatively high volume of qualitative data could be gathered was preferred, with ancillary quantitative data from the same sample gathered for triangulation purposes.
Methodology
The research was divided into two distinct, consecutive streams. The first of these consisted of secondary research for the formulation of an educational resource that would later form an integral part of the subsequent primary research stream. The overall procedure followed is presented in brief in Figure 1, before expansions on each procedure element are offered.
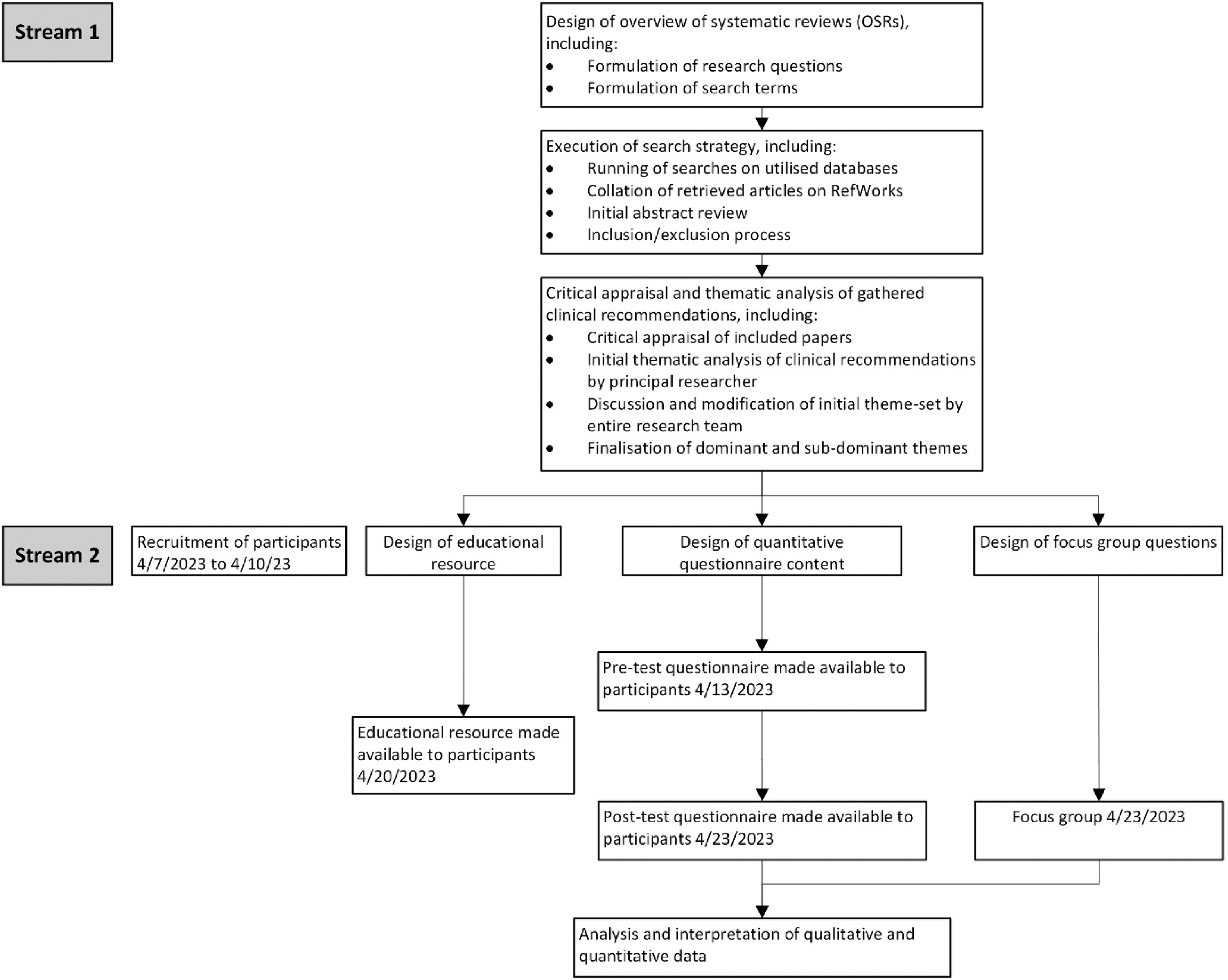
Overall Study Procedure.
The first stage of the research was a series of overviews of systematic reviews, which were performed to provide an evidence base by which to inform the educational resource employed in the research stream. Four overviews of systematic reviews were performed, with each aligning to one of four generalized categories of NPS suggested by Tracy et al. (2017)—stimulants, SCRAs, hallucinogens, and depressants. However, due to the high crossover between results for stimulants and hallucinogens—for example, many novel phenethylamines can share characteristics of both categories (Schifano et al., 2023)—these were ultimately treated as a single entity, with results combined.
Upon completion of the above, a thematic analysis of clinical recommendations across all selected articles was performed. Four dominant themes ultimately emerged: clinical vigilance and awareness (CVA), psychosocial interventions, management of physical symptoms, and management of psychiatric symptoms. Collated clinical recommendations were then used to inform the content of an educational resource that was distributed to participants at the appropriate stage of the research. Prior to and after viewing the resource, participants completed identical questionnaires designed to measure their self-perceived feelings of knowledge and confidence in relation to each theme. Finally, an online focus group using a semistructured format was held to gather qualitative data from participants. Ethics approval for this stream of the study was sought and approved by the Abertay University's Research Ethics Committee, with this being gained on April 4, 2023, ethics approval reference number: EMS7178. Participants provided written informed consent prior to their involvement.
Participants were recruited from students enrolled on Abertay University's BSc (Honours) in mental health nursing degree at the time of the research. Sample size was chosen in large part due to considerations for the focus group element of the primary research. Literature on optimal participant numbers for online focus groups disagrees, varying from four to six members (Lobe, 2017) to five to 10 (Hennink, 2014). Ultimately, a sample of five participants was sought and obtained from a total of six respondents, with the first five respondents being selected.
Results and Findings
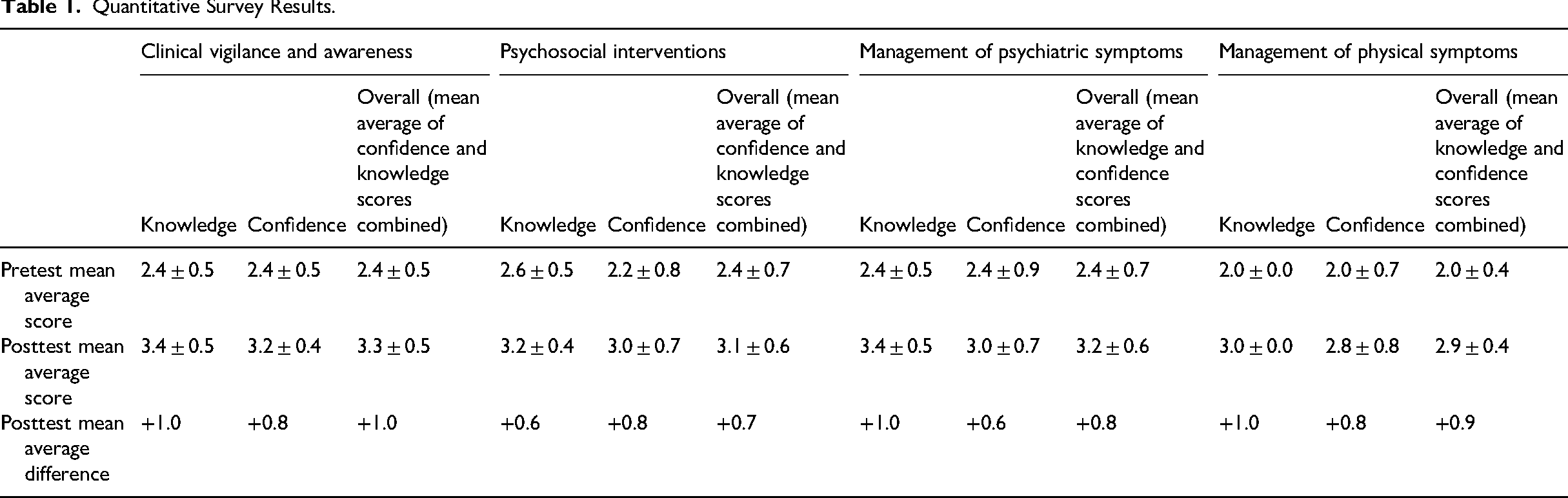
Due to the small sample size, quantitative data gathered from the pre- and-posttest questionnaires were primarily used for triangulation of focus group data, with independent interpretation of it considered too underpowered to be meaningful. However, Table 1 presents the relevant results of the quantitative portion of the study, and complete results and analysis of them can be found in the original thesis from which this article has been developed (Lindsay, 2024).
Quantitative Survey Results.
Primacy was instead given to thematic analysis of qualitative of data from the focus groups. For this, an inductive analysis method suggested by Braun and Clarke (2006) was followed. This consisted of data familiarization; generation of initial codes; and location, review, and definition of themes, with all stages being performed independently by all three members of the research team before final discussion and agreement was made. Ultimately, five dominant themes (value of CVA, holistic treatment of patients, confidence in other professionals’ knowledge of NPS, and NPS-specific competence and educational needs in relation to NPS) were identified. Of these, all but holistic treatment of patients proved of relevance to data triangulation and subsequent analysis, with an exploration of primary data from the remaining relevant dominant and their subdominant themes presented below.
Qualitative Themes
Value of CVA in Relation to NPS
CVA was found to be a theme of great importance to the participants: What we should be looking at – and what I found really useful – was the clinical vigilance. Just asking about assessments and making time to ask the question about whether they're using any of these substances. (Participant 4) The clinical vigilance is something that I think was really… that was probably the most important part to me, and something that I think that everyone would gain something from learning. (Participant 1) I wasn't aware that it was also things like fentanyl and things that we actually are administering. And I was thinking of it more as- yeah – things that are being created and sold on the internet or these kinds of things. (Participant 2) I think I didn't realise the groups of people so much who it could affect and what the effect could be on a person as much. I think I had the belief that it's like “it's a legal high, it's not that important. It's not that disruptive.” But I've definitely changed my view on that. (Participant 3) I think even last placement in forensics, I remember somebody's history. It was said that they took drugs that we're more used to hearing or seeing about and novel psychoactive substances. And then, after watching that presentation, it's like we really need to actually define what those are, because actually they're all going to have really different effects. (Participant 2) The thing about having more confidence is to make sure those questions are asked, those questions to really explore more in depth. The [patient] history is really important. (Participant 4) I think I would feel more confident in actually questioning… well, everyone now. Like let's say … whether it was like nursing staff, I would feel like way more confident in being like “Okay, you're saying they’re NPS, but like what is it? Like, do we need to do a further assessment?” (Participant 1) Realistically, if I see that phrase [NPS] coming up, if I'm on placement, you know, be like “Do we know what the substances are?” Kinda, “What's going on with that?” (Participant 2) At this stage in my nursing career, I would feel a bit anxious about being this newly qualified that comes in and just goes, “well, what about this? What about that?” But I suppose that's our role to really shake it up a little bit. (Participant 4)
Participant 4 articulated concerns over established health professionals’ competence and knowledge on NPS-related issues generally: I would be worried that maybe staff that haven’t had this sort of training or perhaps staff that are coming towards more, the end of their career and they're not as interested in gaining new skills because they're quite happy with the skills they've got already. I would lack confidence in them actually being able to identify and make these inquiries about the patients. Although – I did mention the fentanyl patches, that they can be burnt or chewed – here in placement. And they said, “Yes, but the patches have got a really low therapeutic dose.” (Participant 4) Coming back to what [PARTICIPANT 1] just said, I would be interested in… in the prison settings aspect of it, because the Mental Health Act really isn't used fully within prison settings. So, I would be quite interested to see what they would do – because I know spice is a big problem in prison settings – what they do with people who are obviously going through really bad mental health rather than carting them off into segregation. I'd like to see how they dealt with that. (Participant 3) [O]bviously, if someone's coming in at that crisis point – until you can get them down to a level where you can fully assess them – It's kinda keeping them safe and that in the meantime. And I think I've definitely seen some bad practice surrounding that on placements and wards that I've been in before. And I don't think that's based on the staff themselves. I think it's based on not being educated in what the best practice actually is. (Participant 1) I've just got a post in addictions. And I’m, like… so it's definitely good to have this as a starting point and to be able to find out more about it. Because a lot of the time, it's kinda more generalised in drug and alcohol. (Participant 1)
NPS-Specific Competence
Participants proposed that NPS-specific competence could be increased primarily through direct working with people who use NPS (PWUNPS). This was considered alongside increased professional confidence, was held as bearing similar import as working with established professionals, and was associated by participants as increasing likelihood of improved health outcomes for PWUNPS. Having that team perspective is going to give you a better outcome for that person as well – and involving them in it [their NPS related care-planning] – as well. (Participant 1) I would just echo what everybody else has been saying in relation to that [competence]. I think it would take a lot of experience dealing with patients to slowly build your confidence up. Or perhaps in a certain area, where you see the same thing happen time and time again. (Participant 5)
Educational Needs in Relation to NPS
Some discussion pertaining to outstanding educational needs on NPS focused on the lack of NPS-related content at university curricular level and from other sources: Yeah, considering that we’re based in Dundee, it's quite interesting that we don't get a lot on NPS or as much substance misuse as I thought we would at uni. Considering the levels of it actually in Dundee. So that PowerPoint is quite interesting in the fact that it's definitely furthered my education of them, which I'm quite surprised the uni doesn't do? Or they might do in third-year, don't know? (Participant 3) Yeah. We did touch on it more in third year. We've just done. A workshop that was a few hours about addictions, but not specifically on NPS or anything like that. (Participant 1) Yeah, I would agree with what you're saying. My learning on the subject mostly comes from other courses or just general knowledge gained from the media. So I don't think it's something that's really, as we say… we talk about people having addictions and I think we have this image. And unfortunately, I would actually say that some of the slides and presentations that we get, maybe we use the typical stereotypical sort of “needle and spoon”. All these sort of pictures. That is, we have this idea of addictions just being like the typical, stereotypical images. (Participant 4) I think just having experience with NPS as well – overall – within placements, because some of the placements we've had… really this is probably my first time in placement experience in somebody that does have an issue but NPS. Whereas any other ones, I've never had an experience of it. I also think having practical experience of it and speaking to nurses who have experience or medics as well is highly important – pharmacists, etc. – just to build on this knowledge as well. So I think placement for me is a big one, getting more placements suited to that. (Participant 3) [L]iterally on the placement I'm on at the moment … this week we've had a change from pharmacy, which – this is [NHS health board in Scotland] – where certain medications such as pregabalin are now treated as locked cupboard. I mean, obviously the supply – the storage – is always locked, but they are now classed as “attractive medications”, and … because they have been subject to going missing from the hospital environment. So they're not controlled drugs. However, they are subject to new controls within the practice environment. So that ties in effectively to what we've been looking at with this presentation. (Participant 4) [W]hat would be nice is to get some lived experience voices in there, because that's obviously – this [the presentation] is very much a knowledge … almost like a knowledge dump. But there's no real comment on how it would be to go through that recovery process. Or perhaps even not necessarily somebody who's experienced it themselves, but perhaps families who are looking at what has gone wrong for their loved one and how that can impact on them. So I think that would be interesting point to bring in. (Participant 4) I think definitely what [PARTICIPANT 4] was saying, the lived experience or service user's experience could be an interesting thing to bring in – just, yeah – because if you're reading about a drug and its impacts, it's all very abstract unless you've actually experienced it. (Participant 2) I think that lived experience is something that is quite important for myself to hear as well. But I do understand the barriers, and a lot of people may be resistant to actually talking about it, chatting about it, because of stigma, etc. That could be quite a difficult one to conquer. Or they might downplay what's going on because they don't want to see it as a problem. So again, I see that as an issue, but I do feel life experience is one of the most valuable feedback forms you can have. (Participant 5)
Triangulation of Datasets and Analysis
One finding from the quantitative data was that CVA overall (in other words, inclusive of both knowledge and confidence scores) was the measure in which the participants rated themselves most highly in if standard deviation was factored for, with mean average for this being 2.4 ± 0.5. From this, an expectation could reasonably be held that this would prove to be the area in which participants had the lowest score increase posttest. However, such an expectation was not ultimately borne out at the posttest phase, where it was found that participants’ mean average for this measure had increased by 0.9, which was the joint highest posttest increase alongside the management of physical symptoms, and with this latter measure having the lowest mean average score during pretest (2.0 ± 0.4).
In triangulating this quantitative data surrounding CVA with qualitative data concerning it in the focus group, tentative evidence emerges that participants may have overestimated their knowledge and confidence in relation to CVA at baseline, with this hypothesis also helping to direct interpretation as to how participants consider CVA in their development as healthcare professionals.
During focus group conversations, participants appeared to value newly gained knowledge on CVA as a mechanism by which to prompt new, more informed reflection of both prior and anticipated clinical practice experiences. One specific finding that may seem paradoxical when initially contemplated is that participants’ seemed to regard established healthcare professionals’ level of knowledge and competence (either as individuals or in the context of their being representatives of organizational/professional cultures that do not give due prominence to NPS-related health matters) in NPS-specific healthcare either negatively or with uncertainty while also holding the belief that competence—in reference to NPS treatment specifically—could be developed directly through practicing as part of experienced healthcare teams.
Resolution to this paradox may be provided through return to the idea that participants held possession of a relatively advanced level of CVA to be a framework through which to interpret observed practice. CVA-related competence may implicitly have been more directly relatable to knowledge alone—as opposed to practicable skills—than in it is in other themes that were measured. In these other themes, the inverse may be true, with increased competence instead tacitly being viewed as built primarily through practice of specific skills during hands-on clinical practice. An important aspect of many skills relevant to the current discourse is that they are not NPS specific, having wide utility within the fields of substance misuse, physical, or mental health nursing. This implies that competence in such skills (and therefore treatment of NPS-related health issues) can still be usefully developed in nursing students through working alongside experienced professionals who practice them, regardless of said professionals’ level of CVA.
This working model is given some further credence from other quantitative data. While perceived confidence considered independently improved by a mean average of 0.8 at posttest for the three themes that held the joint highest increase for this measure—CVA, psychosocial interventions, and physical management—CVA held the lowest standard deviation at 0.4 versus the 0.7 observed in the other two themes. This variance is perhaps explained if one considers that—due to their having differences in life, work and professional experience, skillsets, professional interests, and innate ability—participants will have almost inevitably displayed less even levels of confidence in themes they more definitively associated to practical skillsets, having more varied levels of experience in the observation and delivery of these. If—as postulated above—CVA was held to be unique among the themes by participants (due to competence in relation to it being perceived as more attainable through increased knowledge alone), then confidence may reasonably be expected to increase more uniformly across participants for it.
Data concerning self-perceived knowledge score increases also offer tentative support for the hypothesis, given that standard deviations for these proved lower than comparative ones for confidence in all themes other than CVA. This offers the possible argument that while knowledge concerning all themes is considered as relatively attainable through material such as the educational resource utilized in the study, translation of it into competence (expressed through self-perceived confidence) is less attainable, as this is more contingent on hands-on experience of the delivery of aligned practical skills, with the sole exception to this being seen in CVA.
Discussion
Before proceeding to the central arguments of this Discussion section, it is germane of the author to briefly outline how the theme of CVA identified during the thematic analysis of clinical recommendations was considered by the research team, as this will add necessary clarity to later arguments.
Recommendations were categorized under CVA if they could usefully direct nurse decision-making processes for health issues stemming from PWUNPS use of NPS though did not advise directly on specific minutiae of care in the way that other themes did. The research team's operational definition of awareness aligned largely to the more specific concept of situational awareness, which consists of conscious “knowledge about a given situation's elements and circumstances” (Feller et al., 2023). Therefore, recommendations that served to endow the practitioner with such knowledge within NPS-specific clinical situations were included in this category. Vigilance as a term in nursing is often associated with the professional's anticipation of the possibility for and monitoring of threats to patient health (Ajri-Khameslou et al., 2021; Vahidi et al., 2019). While vigilance's salience to this theme overall may seem somewhat intangible, the authors note that the specific term “clinical vigilance and awareness” is widely utilized within medical literature (Chen et al., 2024; Pothapregada et al., 2016; Sackey et al., 2018; Wijburg et al., 2021) though without a specific definition of it offered. The research team chose to adopt this term for the current research, holding a tacit understanding that vigilance can often be said to be of little value without appropriate awareness, and with the former alerting, the clinician to the possibility that the latter is to be employed.
The author suggests at this early juncture that such an understanding has strong resonance with the concept of evidence-making (as opposed to evidence based) interventions as defined in the work of Rhodes and Lancaster (2019), and that much primary data from the current study strengthens this assertion.
Framing interventions from an evidence-making perspective emphasizes them as ontological practices, where the ways that performance of them are enacted are considered along with the formal evidence bases from which they were developed and alongside localized social and cultural milieus, thus facilitating more nuanced and better-informed engagement with service users, according to said contexts (Rhodes & Lancaster, 2019). A case study to illustrate why such an approach is necessary offered by Rhodes and Lancaster (2019) builds on a previous work by Rhodes that discussed how methadone as a treatment protocol was considered by service user and other stakeholder communities in contrast to what was initially intended by policymakers in Kenya (Rhodes, 2018). Methadone was implemented in Kenya primarily to inhibit the transmission of HIV through drug injecting (Rhodes et al., 2015), something that Rhodes and Lancaster (2019) notes as aligning with evidence-based practice for methadone as a therapeutic agent. However, in practice, methadone was translated from this intended interpretation to ones varying from a representation of hope for a normal life to a potentially harmful object that warranted suspicion by PWUNPS (Rhodes, 2018). For Rhodes and Lancaster (2019), examples such as this highlight the need for situated forms of standardization, “wherein intervention experiments in practice are not polarized toward the extremes of [evidence-based medicine] universalism against individualized concern but fall somewhere in the middle ground” (Rhodes & Lancaster, 2019).
Qualitative data from the focus group of the current study are suggestive of some implicit understanding of this by participants. For the author, Participant 4's commentary in relation to the labeling of stored medications such as pregabalin as “attractive medications” is particularly emblematic of this in relation to NPS. Not only did this emphasize the value of increased knowledge of CVA to the participant's understanding of NPS’ potential import in practice environments but also a burgeoning comprehension as to how framing of what constituted viable drugs of misuse differed from clinician/clinical bodies and PWUNPS, with—in an evidence-based framing of practice—the former perspective having to be reactive to the latter. The author notes here that earlier, clinician-devised definitions of NPS quickly became obsolete in light of rapidly evolving NPS contexts and the drugs that were utilized in their attendant drug cultures, and contrasts Peacock et al.'s (2019) classification of NPS as substances that were “originally designed alternatives as legal alternatives to … controlled substances” with the later contribution of the National Records of Scotland (2024b) that they are “the kinds substances that people have, in recent years, begun to use for intoxicating purposes.” In the former definition, legal status and NPS’ relative position to controlled, orthodox psychoactives is stressed, whereas in the latter a more agile understanding of NPS as a phenomenon—free from such earlier delimitations—is given. Instead, only that they are of late being utilized within drug cultures is given prominence. Although conjectural, the author posits that such a radical change in emphasis (in the Scottish context at the very least) must to some degree be a reaction to drugs previously considered as primarily belonging to the domain of the “clinical sphere” being retranslated to objects of unanticipated alternative meanings and value within relevant drug cultures, with the gabapentinoids representing a highly a salient example of this in Scotland (Torrance et al., 2020). Similar tensions between clinician/policymaker and PWUNPS meanings of NPS have been noted by Pickering and Greenwood (2019) who—in their study of Scottish NPS-using people—found that themes of continuity as much as of disruption dominated participant discourses and that the term NPS itself held so little value to them as to be near meaningless.
A further framework through which the research team considered the study's data was the theory–practice gap. One formulation of this concept initially promulgated by Allmark (1995) and expanded upon by Greenway et al. (2019) conceptualizes the phenomenon as partially consisting of the following interrelated attributes: lack of correlation between learning from practice and formal education, theoretical knowledge failing to be mirrored in observed practice, and theory being regarded as irrelevant to practice. Taken alone, this understanding was not found by the research team to align well with all findings of the study discussed above. However, Hatlevik (2012) suggests a model in which the theory–practice gap is resolved by coherence (internal harmonization between practice and theory) being realized primarily via the practitioner's reflection on theoretical knowledge, with reflection on practice being an ancillary component to this. Under an evidence-based approach to designing educational resources on NPS for nurses and other clinicians, it is conceivable that all four themes that were identified during the thematic analysis of clinical recommendations may have held comparable value to participants. Instead, the author holds that the fact that only CVA was specified by participants as being of particularly high value in the qualitative data (with quantitative data also attesting to this) makes sense to both evidence based and the preferable evidence-making approach.
Due to the CVA theme's position as a lens through which to prompt reflection on observed practice, it aligns well to Hatlevik's (2012) model, which centralizes reflection as the mechanism to enact closure of the theory–practice gap. As discussed earlier within the findings section of this article, self-perceived competence in CVA was theorized by the research team to be more readily attainable due to the substance of it skewing more toward the “theory end” of the theory–practice continuum. If considered under the frame of Hatlevik's (2012) work, CVA should therefore readily act as a vehicle for reflection and—ultimately—coherence between theory and practice. To return briefly to Greenway et al. (2019)'s formulation, prior to the aforementioned attributes of the theory–practice gap are three antecedents: evidence-based practice, ritualistic practice, and teaching and acquisition of nursing skills. In the case of educational themes other than CVA, these remain more sensitive to the theory–practice gap. However, this is not through the previously discussed attributes but in potential deficits at the antecedent stage or—more specifically—in ritualistic practice and acquisition of nursing skills. The practical skills associated with non-CVA themes are generalizable to non-NPS contexts. Therefore, while the attributional aspect of Greenway et al. (2019)'s model is irrelevant to the NPS-specific context directly—through theoretical knowledge here having no competing counterpart in the field of practice—these themes remain more prone to being subject to the theory–practice gap through the practical skillsets they share with non-NPS contexts, with the latter contexts acting as the channels through which theory–practice gap attributes can manifest.
However, if the awareness within CVA concerns “knowledge about a given situation's elements and circumstances” (Feller et al., 2023) and such circumstances and elements are to be considered as inclusive of the lived realities of PWUNPS and their own relationships with NPS within localized contexts, then it can also act as a lens for reflection by which the more “[e]mergent and adaptive” (Lancaster et al., 2020) practice of evidence making can occur in learners. As previously noted, uncertainty as to evidence-based practice is in itself a potential antecedent of the theory–practice gap (Greenway et al., 2019). It is important to reemphasize here that evidence making does not seek to entirely devalue the use of clinically researched evidence bases but to seek parity of regard for other informant knowledge bases to practice (Rhodes & Lancaster, 2019). As corroborated by much of the qualitative data included in the current article's results section, content concerning CVA increased participant confidence to ask questions and encouraged them to avail themselves of a more systemic understanding of NPS-related healthcare interactions—that is, the “given situations” of Feller et al. (2023) —in a manner that remains consistent with the valuing of evidence bases. In other words, it encouraged a mode of understanding compatible with evidence making, in that it is one that embraces being emergent and encouraging of adaptation of approach to localized and/or individualized situations.
Further, these same features align such a mode well to Connolly's (2004) idea of emergent causality as interpreted by Race (2014). Race (2014) emphasizes the avoidance of simplistic understandings of how service user communities and (in the case study they primarily utilize in relation to their argument—though which they ultimately extend to other forms of policymaking, including healthcare) criminal justice/law enforcement interact upon one another in relation to drug-taking practices and norms of the former, with Race characterizing these as dominated by facile, overly linear “cause and effect” discourses within the literature. Instead, Race (2014) borrows the concept of emergent causality to propose that actions by each set of actors (as well as nonhuman factors) in such interactions are far less predictable and unidimensional in nature. As much discourse in the current article attests to, NPS as a phenomenon is a highly complex issue, wherein what is to be understood by the term it is employed is—necessarily—mercurial and reactive to emergent PWUNPS practices. It is perhaps unsurprising then that Duke (2020) applies Race's (2014) conceptualization to the issue of problematization of NPS within the English prison system, utilizing it to critique reductive narratives within policy documents that serve to narrow the issue to a simplistic, largely service user inculpating set of causative factors. The author proposes that being attendant to the multiplicity of ways in which such emergent causalities can occur in relation to NPS-related events is essential to all professionals whose work intersects with PUWNPS, from researchers and drug scholars to frontline healthcare workers such as nurses. In the case of the latter, increased CVA in the current study seemed to increase participant anticipation for the need to not only apply more formal, clinical assessments and similar instruments (amongst other “clinically vigilant” measures) as necessary: “do we need to do a further assessment?” (Participant 1); “Do we know what the substances are?” (Participant 2), but to be an active actor within the situation, engaging with PWUNPS so as to factor in their experiences, motivations and personal understandings of NPS into tailored treatment: “make sure those questions are asked, those questions to really explore more in depth. The [patient] history is really important” (Participant 4); “they [PWUNPS] might downplay what's going on because they don't want to see it as a problem” (Participant 5), aligning to a form of awareness congruent with both evidence making and emergent causality as described.
Further evidence on the theory–practice gap suggests that experience of it by student nurses may in part be precipitated by observing dehumanization of the patient by established professionals (Martínez-Linares et al., 2019) and that successful addressment of the gap may include addition of a greater amount of educational content that considers relevant patient culture and characteristics, inclusive of lived experience input (Singh et al., 2024). While this latter point aligns well with the line of argument followed in the current article to this point, data concerning healthcare professionals’ attitudes toward PWUNPS specifically is lacking (although what does exist will be analyzed later), making comment on this specific aspect difficult. However, some participant discourse from the current study was at least suggestive that health professionals that they had worked with could be dismissive of PWUNPS strategies as they related to NPS consumption practices: “I did mention the fentanyl patches, that they can be burnt or chewed … And they said, “Yes, but the patches have got a really low therapeutic dose”” (Participant 4). While this is not evocative of stigma on the part of healthcare workers in a cursory reading, it is strongly indicative of assumptions that clinician “owned”/produced knowledges are superior to those that arise from PWUNPS experience. Although this specific example cannot be said to truly align with evidence-based understandings of knowledge and practice ownership—given that the health professional's assertion here is entirely incorrect (Giorgetti et al., 2017)—it is illustrative of an attitude that understanding of PWUNPS contexts or perspectives are of negligible value to the clinician and their practice. The US's National Academies of Sciences, Engineering and Medicine (2016) typify stigmatization of PWUD as being enacted or held in the form of attitudes, beliefs, or organizational/systemic structures (among others possible elements). Albeit scant overall, the extant recent data concerning UK health professionals’ perceptions of PWUNPS are not strongly suggestive of direct attitudinal stigmatization of service users on the part of health professionals (Ralphs & Gray, 2018; Solomon et al., 2023; Solomon & Guirguis, 2024). However, what is revealed in the work of Ralphs and Gray (2018)—which gathered views from both care providers and PWUNPS—is perceived stigmatization at structural level within health services of some PWUNPS communities or populations, mostly manifesting as the absence of services tailored to their specific needs. Further, Solomon et al.'s (2023) findings—focused solely on health professional perspectives—revealed a prevailing viewpoint that a lack of training based on evidence-based frameworks of knowledge precipitated feelings of underconfidence within them. To affirm, the author does not contest the legitimacy of such feelings. Clinical training produced from formally gained evidence bases is of course necessary. However, Solomon et al.'s (2023) results—regarded alongside previous research concerning health care professionals’ (HCPs) confidence in relation to NPS treatment (Guirguis et al., 2015; Owie et al., 2017; Ramos et al., 2020; Wood et al., 2016)—points to either an overarching hesitancy among HCPs to contemplate an evidence-making form of intervention production or even a lack of comprehension of it as a possibility.
As attested to by participant discourse in the current research, NPS's position within undergraduate-level educational curricula is essentially nonexistent, with this being matched by the author finding a complete absence of it as a topic within the literature. Satterfield et al. (2022) discuss the “hidden curriculum” as it applies to the field of substance misuse healthcare education. Broadly, this term refers to the norms, values, and attitudes held by established professionals and perceived by learners outside of formal curricular structures within medical education, most commonly associated with clinical practice as a learning environment (Mulder et al., 2019). As it pertains to substance misuse disorder education in the health professions, Satterfield et al. (2022) cite Avery et al. (2017) and Werder et al. (2022) in typifying the hidden curriculum as inclusive of stigmatization and depersonalization of relevant patient groups within the context. During their subsequent model formulation for the improvement of substance misuse educational curricula—which contains a particular focus on addressing the potential negative influence of the hidden curriculum—Satterfield et al. (2022) suggest inclusion of lived experience and localized, community input as desirable measures, relating the latter in particular as a direct counter to stigmatization. This aspect of said model echoes not only with the previously mentioned association between patient dehumanization and the theory–practice gap as intimated by Martínez-Linares et al. (2019), but with themes from the current study's findings concerning the desirability of lived experience content as well as Rhodes and Lancaster's (2019) concept of evidence making. However—as already discussed—there was content in participant discourse that suggested an absence or only rudimentary understanding of NPS from either evidence-based or evidence-making perspectives seen among health professionals on practice placements. This—when considered in conjunction with participant expressions concerning lack of educational resources—suggests that NPS-focused healthcare education may be better aligned to a concept distinct from the hidden curriculum, that of the “null curriculum.”
The term null curriculum refers to an absence of education on a given topic within curricula, with failure of its addressment through either the explicit, implicit, or previously discussed hidden curricular modes (Eisner, 1994). Within this framework, “explicit curricula” refers to formalized educational content made publicly available by educational institutions (Flinders et al., 1986), while “implicit” or “informal” denotes that which may broadly align to the former though is transferred interpersonally via student/educator exchanges and is therefore subject to some deviation or variance from it (Rothlind et al., 2020). More properly then, location of NPS education's position within the described scheme of curricula may be informed through further reference to an argument posited originally in the analysis portion of this article. Namely, the relatively unique position of the theme of CVA and its relationships to other themes is explored in the study. Much learning concerning treatment of NPS-related health conditions is in fact disseminated to nursing students. However, this is overwhelmingly through the implicit curricular mode, and—even then—due to the serendipitous fact that many practical skills germane to NPS-relevant treatment are common to substance misuse and/or nursing contexts in the widest possible sense. As Satterfield et al. (2022) attest to in their discourse on substance misuse healthcare education, this tacit alignment to that remit may in itself leave NPS healthcare education overall open to the potentially malignant vagaries of the hidden curriculum.
The author closes this discussion by returning to Race's (2014) interpretation of emergent causality. Within the same article Race (2014) also invites the reader to consider drug contexts/events from a “topological” perspective, that is, “a relational understanding of the construction and permutation of space, time, objects and events” in which the observer is themselves an inherent part of said topology. This—as well as Race's (2014) argument regarding emergent causality overall—finds strong parallels in Springer and Clinton's (2015) call to view nursing knowledge from a Foucauldian perspective, asking of practitioners that they “[d]escribe complex systems of distinct and multiple elements, events and identities that deny synthesis and foundational truths” while emphasizing Foucault's insistence that the self cannot be separated from such systems. The previously recalled works of Brown and Wincup (2020), Duke (2020), and Alexandrescu and Spicer (2023) all infer that NPS have been problematized in UK-contextual policy discourses of them, where problematization is considered from Foucault's theorization of the concept, wherein “issues, experiences, phenomena, and populations get constituted as ‘things’ in need of regulation or intervention” (Houborg et al., 2020) and in which the “problematized” must be thought of as inherently distinct from “problematizer.” To briefly resume the theme of what is meant by the term NPS, Measham and Newcombe (2016) argue that legislator-dominated constructions of it have their greatest import to those actors themselves, as well as the producers of NPS. Although not framed as such explicitly, Measham and Newcombe (2016)'s discourse somewhat echoes the findings of Pickering and Greenwood (2019), in that both emphasize that the legal status (and hence a key component in such constructions) of NPS is often poorly understood or is rarely a motivating factor in PWUNPS's decision making in relation to acquisition of them. For the author, this is particularly emblematic of the current disconnect between evidence based and the possibility of evidence-making approaches in relation to NPS and healthcare treatment of conditions arising from their use. Student nurse education on NPS that centralizes CVA over other themes may serve to help bridge this gap, as well as any theory–practice gap that emerges from consideration of NPS as a pedagogical subject. The “vigilance” aspect of CVA has importance. However, the awareness it fosters appears to be inclusive of the student's realization of their own, other practitioners’ and PWUNPS's relative positions “in relation to [the] complex systems of distinct and multiple elements, events and identities” (Springer & Clinton, 2015) that are inherent to NPS-relevant contexts, lending it greater comparative value. Finally, without the modifying presence in explicit curricula of CVA-focused NPS-specific education—which as this study suggest, may act as a catalyst toward student understanding the shared commonalities of said practical skills across the aforementioned contexts—NPS education in nursing is ultimately left to the black hole of the null curriculum.
Conclusion
The current study has provided tentative evidence that the theme of CVA is highly valued by nursing students within NPS-specific education, appearing to act as something of a vehicle toward reflection by which they can interpret the relative salience of any knowledge, practiced skills and placement experience to NPS-related treatment. Confidence in the theme appears more readily attainable than others examined, with this perhaps being accounted for by it skewing more toward the “theory end” of the theory–practice continuum.
Much of the discussion of this article explored the theme of the theory–practice gap as it applied to the current study's results, finding that increased knowledge of CVA aligned well to Hatlevik's (2012) concept of coherence between theory and practice as it allows for the necessary reflection to achieve this. Other themes were suggested as being more prone to the mechanisms of the theory–practice gap. This was not via the attributional aspects suggested by Greenway et al. (2019) but rather by virtue of possible antecedents suggested by those authors, due to such themes having no viable rival theoretical schema offered by established professionals while simultaneously being more reliant on achieving competence through gaining proficiency in practical skillsets that share commonalities across broader healthcare remits.
Further discussion then related CVA (as considered by the author) to Rhodes and Lancaster's (2019) concept of evidence making. Here, the awareness aspect of the former was emphasized as allowing clinician sensitivity to PWUNPS's understandings and personalized/localized meanings of NPS to be fostered in a manner consistent with the aims of evidence making which are—again, broadly—to inform practice from both formal evidence bases as well more situated, grassroots sources of knowledge (Rhodes & Lancaster, 2019). Similarly, some alignment was found with Race's (2014) idea of emergent causality, which urges professionals involved in drug user community facing roles to be cognizant of their active role in drug-related events, in which cause and effect cannot be clearly delineated. Again, CVA's awareness of the type described in relation to evidence making was proposed as a catalyst for such a mode of thinking, with the author drawing attention to contemporary discourse on nursing asking that its practitioners hold a more Foucauldian understanding of their position within systems to assert this (Springer & Clinton, 2015). Without doing so, they become in danger of contributing to the problem–problematizer dichotomy (Houborg et al., 2020) that dominates much policy and subsequent protocol related to NPS to date (Duke, 2020). Not only should avoidance of this be considered a worthy ambition for nursing more globally, but also—in the Scottish context—aligns well with the Scottish government's ambition for a “wholesale culture change” in drug policy that embeds acknowledgement of service user perspectives (Scottish Government, 2023).
Previous researchers of the NPS phenomenon have asked of policymakers that they facilitate education of it “in its widest and original sense,” from both top-down and grassroots positions (Zamengo et al., 2019). While the inconstant nature of the NPS landscape may explain healthcare educational bodies’ reluctance to engage in this endeavor in part, it does not excuse it. Shafi et al. (2020) urge clinicians to be cognizant of the fact that much within their current skill and knowledge bases relevant to substance misuse practice broadly (as well as management of symptoms) in their most general sense is highly applicable to a narrower, NPS-focused remit. The current author noted early in the Discussion section of this article that—although widely employed in the literature—the phrase CVA remains without a standardized definition, either in substance use contexts or more widely. Therefore, they propose that this absence presents an opportunity to give the term meaning in relation to NPS-related healthcare. If nurse undergraduate (and other health professional) education on NPS is truly to take its “widest and original” form and avoid effective exclusion to the null or hidden curricula, then it must be inclusive of relevant service user perspectives in the manner demanded in evidence-making approaches and must marry the clinical awareness of PWUNPS's understandings and knowledge on relevant drugs with the clinical vigilance—gained primarily from more traditional evidence bases and which originally related to more orthodox drugs—that may still usefully inform nursing practice, in the manner suggested by Shafi et al. (2020).
Limitations
The author acknowledges that the current study is subject to several limitations. The first of these relates to the small participant sample size used. This does greatly restrict the reliability, reproducibility, and statistical significance of its results and findings, particularly in relation to its quantitative data (Andrade, 2020). However, a mixed-method approach to the research was pursued, given its exploratory nature in relation to a vastly underresearched area of study. Within such methodologies, quality is open to being falsely conflated with rigor, when only the latter can be objectively exhibited (Harrison et al., 2020), especially given that the qualitative element of the current research was considered as “dominant” to the quantitative and that a reduced sample size is generally recommended in mixed-method research where this holds true (Venkatesh et al., 2016). This decision is given further partial justification in light of the thematic analysis strategy that was employed in the qualitative analysis, as—when using this as a protocol—larger sample sizes are not necessitated unless data saturation is sought (Fugard & Potts, 2015).
The second limitation relates to the author's relationship to the participants. The author/principal researcher is a member of teaching staff at the university at which all participants were studying at the time of the research. This does open the study to accusations of bias, as well as to social desirability influencing participants’ discourse. Although the study cannot be truly considered as aligning to the field of action research, it was hugely instrumental in its design, given said research philosophy's focus on solving problems related to reflexivity and positionality (Gibbs et al., 2017). That participants’ involvement was entirely voluntary, that they had full freedom to withdraw from the study at any time and the ultimate anonymization of their collected data were clearly emphasized to them in consent to participate forms, with the furnishing of such information considered crucial to action research (Cohen et al., 2017). Action research prioritizes the conscious avoidance of any coercive measures (Banegas & Villacañas de Castro, 2015)—that there would be no tangible reward or preferential treatment in relation to their involvement was also made clear to participants, and the author was not involved in any assessment grading of participants at the time (or close to the time) of the research. In the spirit of transparency and full disclosure, the author did later send two articles of interest on the subject of substance misuse nursing to one participant and advised two others in relation to substance misuse-related elective practice placements they were considering, all at their spontaneous request. However, this is far from unusual in the author's role, and they do this routinely for many students at the institution in question. Moreover, to return to the theme of action research, a particular strand of this—participatory action research—stresses empowerment and democratization of research procedures to the benefit of involved participants (Cohen et al., 2017), wherein empowerment of the same is explicitly tied to maximization of their own ability to research and increase their knowledge (LeCompte, 2015), and the aforementioned actions by the author can be considered as being conducive to this.
Footnotes
Acknowledgements
The author gives huge to thanks to Jude Kelly, Mhairi Thurtson, and Anne Savage (all of Abertay University) as their supervisors during the Masters by Research project from which this article is based. Their patience, insight and encouragement throughout made its completion possible. They also thank Seb Monteaux, Noelle McDougall, and Alison Elliot (again—all of Abertay University) for the invaluable advice and support they gave during the writing of this article.
Ethical Approval and Informed Consent Statements
The Research Ethics Review Committee at Abertay University approved our focus group and quantitative questionnaires (Approval: EMS7178) on April 4, 2023. Respondents gave written consent for review and signature before starting both. All participants provided digital, written consent for their anonymized data gathered during the research to be used in all subsequent publications.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets forming the primary research component of this article are publicly available from the Abertay University repository, can be accessed using the following DOI: ![]() , and with the dataset record being named Data for: Exploring mental health nursing student competence and confidence in treating NPS-related health issues in the United Kingdom.
, and with the dataset record being named Data for: Exploring mental health nursing student competence and confidence in treating NPS-related health issues in the United Kingdom.