
Abstract
Introduction
In light of North America's persisting drug toxicity crisis, alternative drug policy approaches such as decriminalization, legalization, regulation, and safer supply have increasingly come to the forefront of drug policy discourse. The views of people who use drugs toward drug policy and drug law reform in the Canadian context are essential, yet largely missing from the conversation. The aim of this study was to capture the opinions, ideas, and attitudes of people who use drugs toward Canadian drug laws and potential future alternatives.
Methods
This paper was developed as part of the Canadian Drug Laws Project, a cross-jurisdictional qualitative study conducted in British Columbia, Canada between July and September 2020. The qualitative data are from 24 semi-structured interviews with a diverse sample of people who use illegal drugs. Interviews were recorded, transcribed, coded, and analyzed thematically by the research team.
Results
Two main themes and corresponding sub-themes are presented: (1) The experience of stigma as a consequence of criminalization; (2) The perceived benefits of drug law reform. Participants spoke in-depth about their experiences living within a criminalized drug policy context and offered suggestions for new pathways forward. Their perspectives illuminate how Canada's drug laws may shape public attitudes toward people who use drugs and the consequent manifestations of structural, social, and self-stigma experienced by people who use drugs.
Conclusion
Participants openly and profoundly believed that current drug laws produced and propagated the public attitudes and structural inequities experienced by people who use drugs in Canada. This matters, not only because our findings highlight the fact that people who use drugs experience stigma in tangible and clearly impactful ways, but it also suggests that the criminlilization of drugs shapes the experience of structural, social, and self stigma. Finally, participants believed that efforts to destigmatize people who use drugs would be ineffectual without the enactment of more robust forms of drug law reform such as the decriminalization of illegal drugs.
Introduction
In Canada, and elsewhere around the world, the primary approach to addressing drug use and drug possession has been through punitive drug laws, prohibition, and policing. Yet, this draconian approach has failed to produce any substantive reduction in the number of people who use drugs (World Drug Report, 2021) and aggressive policing tactics are well documented to exacerbate the multiplicity of social, health, legal, and environmental issues experienced by people who use drugs (Cooper et al., 2005; Jensen et al., 2004; Nelson, 2018; Sarang et al., 2010). Since 2016, while people who use drugs have continued to be criminalized in Canada, 34,355 people have died from opioid-related overdoses—more than all major causes of accidental death combined (Fischer, 2023; Government of Canada, 2023). The inadequacy of a solely policing response opened the door for the introduction of low-cost public health responses centered on harm reduction (Hyshka et al., 2017 ; Wild et al., 2017) 1 . Despite these innovations, in recent years, academic, public health, community activist groups, and even some branches of law enforcement (Canadian Association of Police Chiefs, 2020; Zimonjic, 2020), have called for more robust policy reform such as the decriminalization of illegal drugs and the implementation of wide-reaching safe supply programs (Bonn et al., 2020; CAPUD, 2019; Ivsins et al., 2020).
The involvement of people with lived or living experience of drug use as a valued resource in democratic drug policy processes is increasingly recognized within research as critical to the success (e.g., applicability, accessibility, relevance) of drug policy reforms (Madden et al., 2021). While the majority of such studies have explored the perspectives of people who use drugs in relation to cannabis regulation (Hathaway et al., 2011; Osborne & Fogel, 2017), some researchers have recently begun to examine people who use drugs’ policy preferences toward the regulation of criminalized drugs (Greer & Ritter, 2019; Greer & Ritter, 2020). This study contributes to a small body of research on views of people who use drugs toward drug law reform and is the first of which to focus specifically on decriminalization in the Canadian context.
With this gap and the evolving context in mind, our qualitative study captures the opinions, ideas, and attitudes of people who use drugs to elucidate their views on the impacts of criminalization and potential drug liberalization policies. Building on the work of stigma theorists such as Fraser et al. (2017) and Seear et al. (2017), who employ a poststructuralist lens to understand how stigma is both performative and produced, our paper adopts a critical realist approach to our data and analysis. More specifically, in analyzing the experiences of participants, we suggest that public attitudes toward people who use drugs may be in part produced by Canada's criminal drug laws and explore what consequences the resulting stigma has on the lives of people who use drugs. Based on our findings, we recommend that to truly combat structural, social and self stigma, alternatives to criminalization and a move toward the liberalization of drug policies (e.g., decriminalization, legalization, regulation, and safer supply) should be considered.
Defining Drug Laws and Criminalization
In this paper, we take up drug laws and criminalization as two independent ideas. At the time of data collection, the personal possession of illegal substances (i.e., “simple possession”) was a criminal offence across all provinces and jurisdictions under the Canadian Drugs and Substances Act (CDSA, 1996). This Act specifies the current legal framework for drugs as well as the mandated punishments. When referring to Canadian drug laws, we mean the policies that legally mandate threats of punishment delineated for the possession of illegal substances through this Act. Possession of illegal substances is the focus here as it is this section of the CDSA which criminalizes the largest swathe of people who use drugs and is the primary section being contested presently in drug policy discourse in Canada. It is only this section of the CDSA that has been the focus of pilot proposals for reform such as decriminalization as a public health intervention in British Columbia (BC). Alternatively, the term criminalization refers to a multitude of social processes, including the enforcement of criminal laws, everyday law enforcement, and the threat or use of state power (e.g., police apprehension, exclusionary public policy), that transform people and acts (e.g., drug possession) into criminals and crimes, respectively.
Litterature Review
Harms of Criminalization
In recent years, Canada's drug laws and mechanisms of criminalization have been called into question given the evidence of harm created (Boyd et al., 2016). Criminalization is increasingly recognized as a critical structural determinant of health that worsens health and social outcomes for people who use drugs (Greer et al., 2022; Selfridge et al., 2020). A large body of evidence suggests that the policing of drugs has a compounding effect on a multitude of the harms experienced by people who use drugs (Baker et al., 2020 ; DeBeck et al., 2017; Sarang et al., 2010; Werb et al., 2008). For example, studies show that police presence in drug markets results in rushed injections and increased overdose risk (Beletsky et al., 2014; Gaines et al., 2015; Hayashi et al., 2013; Miller et al., 2008; Small et al., 2006; Werb et al., 2008). Policing also discourages people who use drugs from carrying or using harm reduction equipment (Beletsky et al., 2014; Small et al., 2006) and accessing health and harm reduction services, including needle and syringe programs, overdose prevention sites (Bardwell et al., 2019; Collins et al., 2019; Watson et al., 2021), as well as opioid agonist therapy (Philbin & Zhang, 2010), and HIV and Hepititis C medication (Mimiaga et al., 2010). Research from Toronto, Canada has documented police both apprehending individuals and destroying harm reduction equipment in the vicinity of these health and harm reduction services (Watson et al., 2021).
Finally, the over-policing of people who use drugs has been shown to drive feelings of distrust between communities of people who use drugs and the police, reinforcing structural inequalities and reducing the perception of people who use drugs that police assistance is appropriately commissioned for their community as much as it is for the wider public (Kammersgaard et al., 2021; Scher, 2020; Selfridge et al., 2020). Criminal drug laws also structurally produce an unregulated and illegal drug market where it is impossible to control drug toxicity and where marginalized people who use drugs are often pushed to procure illegal substances from dangerous and often unpredictable environments (Jacques & Allen, 2015; Werb et al., 2011). Criminalization, policing, and fear of arrest are also barriers to people seeking emergency medical services during overdose events (Latimore & Bergstein, 2017; Moallef et al., 2021; Selfridge et al., 2020). In spite of Canada's Good Samaritan Drug Overdose Act (2017), intended to protect people who witness people using drugs from drug charges when calling for emergency serivces at the scene of an overdose, evidence suggests that awareness and understanding of this Act varies greatly amongst police officers and people who use drugs in BC (Mehta et al., 2021; Xavier et al., 2021, 2022). This means despite legal reform, people who use drugs still may not call emergency medical services due to the threat of both police apprehension and police prescence at the scene of a drug overdose. Furthermore, studies show the stigma associated with drug use—is a direct factor limiting people's willingness and ability to access health services and contributes to people using drugs alone, which in turn leads to higher rates of overdose deaths (Corrigan & Nieweglowski, 2018; Hatzenbuehler & Link, 2014).
Stigma Theory and Drug Use
In his seminal 1963 essay “Stigma: Notes on the management of spoiled identity,” sociologist Erving Goffman defined stigma as “arising when an individual, because of some attribute, is disqualified from full social acceptance” (p.9). As many subsequent analyses have pointed out however, Goffman's influential conceptualization of stigma as individual experiences of “deviance” from societal norms obscures the political histories and production of the marks of stigma; it is a decidedly “apolitical” account of stigma that lacks an analysis of social power (Cavan, 2014; Scambler, 2009, 2018; Tyler, 2018; Tyler & Slater, 2018). Goffman's significant influence in sociology and public health has led both stigma research and anti-stigma interventions to focus heavily on adjusting individual attitudes of “stigmatizers” and helping the “stigmatized” to endure their exclusion with less harmful outcomes. This stands in contrast to an approach centered on understanding the political, historical and structural roots of stigmatization or empowering collective resistance to challenge those who drive stigma production or benefit from its divisive impacts (Fraser et al., 2017; Friedman et al., 2021; Tyler & Slater, 2018; Tyler, 2018; 2020).
Importantly, stigma scholars have built upon Goffman's work by adding to the mechanisms and contexts in which stigma develops. Link & Phelan (2014) explain that to understand stigma we must understand the power structures within society. Laws function as one device within these political systems and power structures. More specifically, stigma is produced by those who have the power to define the rules and apply sanctions for violating them. As targets of this process, people who are stigmatized are defined not by their actions but by their labelled identity in accord with the oversimplified, undesirable social characteristics ascribed to them (Livingston, 2013). This process ultimately leads to the perceived legitimization of discrimination and the loss of political status for the stigmatized group (Friedman et al., 2021).
More recently Fraser and colleagues have theorized stigma at a much broader societal or even cultural scale and as a performative process that helps delineate between legitimate subjects, deserving of care and concern and those who are deemed illegitimate, underserving, and stigmatized. They highlight this perfomative process by elaborating on how the experiences of stigma (both felt and enacted) in a variety of settings (eg., healthcare, workplace, family) lead to people who use drugs avoiding those contexts. This in turn “produces” their invisibility in those contexts and reinforces the stigmatizing conception that people who use drugs do not deserve health care, cannot manage stable employment, and so on. While their interpretation speaks clearly to the political role of institutional and political arrangments such as drug laws, the authors specifically call for a societal reconceptualization of “addiction”—one which would work to dethrone the widely held belief that substance use is antithetical to the “good,” liberal, self-governing, rational subject who is therefore deserving of care. This conceptualization of stigma has been further elaborated by Seear and colleagues (2017) who outline an approach to interrogating the potential of laws pertaining to alcohol and other drug (AOD) use to “perform” stigma toward people who use drugs.
In the analysis we present below, we adopt a critical realist ontological framework (Bhasker & Hartwig, 2015) to examine how our participants (i.e., people who use illegal drugs and experience criminalization under Canadian prohibition policies) experience and interpret the connection between the criminalization of their substance use and the production of stigma at various levels. Like Seear and colleagues (2017) we too focus on the under-examined phenomenon of the law itself as a producer of stigma, in addition to considering participant experiences with law enforcement (e.g., police interactions, see also Greer et al., 2022; Selfridge et al., 2020). Like Fraser and colleagues (2017), we critically examine participants accounts of substance use-related stigma but do so in direct relation to their understandings of how the criminalization of drugs contributes to and may even “produce” the varieties of stigma experiences they report.
Structural, Social, and Self Stigma
Amongst the numerous “types” of stigma that organize modern stigma theories, the most common include stigma at the level of the structural, the social, and the self. Within the context of drug use and drug dependency literature, scholars (Friedman et al., 2022; Livingston, 2013; Nieweglowski et al., 2018) have explored how stigma is related to the criminalization of illegal substances.
Livingston (2020) defines structural stigma as “the rules, policies, and procedures of social institutions that arbitrarily restrict the rights and opportunities of people [living with substance use issues]” (p4). Structural stigma encompasses the systematic devaluation of people who use drugs through policies that reflect and facilitate their social exclusion. Connected to the experience of structural stigma, social stigma in relation to drug use refers to negative connotations associated with people who use drugs (Santos da Silviera et al., 2018). Contemporary characterizations of drug-related social stigma are fundamentally associated with the neoliberal belief that people who use drugs are “weak, antisocial, selfish, lazy and people who value pleasure” (Santos da Silviera et al., 2018, p.19) and that they are both dangerous and to blame for their condition (Lloyd, 2013). Finally, self-stigma manifests when people who use drugs come to internalize negative beliefs and stereotypes about themselves that are transmitted to them through the societal messages of exclusion communicated by both social and structural stigma (Nieweglowski et al., 2018). This phenomenon of internalization applies most significantly to those who experience social marginalization because of their drug use (Corrigan et al., 2017; Matthew et al., 2017). A recent systematic review by Hammerlund and colleagues (2018) further reveals that self-stigma has been widely found to deter people who use drugs from accessing formal health care due to feelings of shame, specifically the fear of revealing their substance use to both their immediate social networks and health care practitioners.
Whilst the lived experience of self-stigma and the pervasive nature of social stigma in relation to drug use is well-documented (Hammarlund et al., 2018; Matthews et al., 2017) there is surprisingly little research on the connection between stigma toward people who use drugs, criminal drug laws and the potential alleviating effect of drug liberalization policies. More importantly, only a limited body of research has begun to offer concrete solutions for reducing, addressing or resisting the structural, social and self-stigma experienced by people who use drugs (Friedman et al., 2021; Gao et al., 2020; Livingston et al., 2012; Livingston, 2021a; McGinty & Barry, 2020). This study addresses this important gap within drug policy research by examining the perspectives of people who use drugs who interpret and describe how drug laws shape the moral associations, stereotypes and wider beliefs about people who use drugs and how these views are continually cemented into reality.
Recent Drug-Policy Reforms in British Columbia
In Canada, most substances (e.g., heroin, cocaine, methamphetamine, etc.) remain illegal and their possession and trafficking remain a criminal act under the Canadian Controlled Drugs and Substances Act. However, in 2018, cannabis became a legally regulated substance under the Cannabis Act. More recently in 2021, some Canadian jurisdictions, including Vancouver, Toronto and the Province of BC, applied to Health Canada for an exemption from the CDSA, which would essentially decriminalize certain drugs. Thus far, only BC has been approved for this exemption, with the decriminalization of possession of certain illegal drugs in amounts totaling less than 2.5 grams coming into effect as of January 31, 2023. In a news release, Carolyn Bennett, Federal Minister of Mental Health and Addictions stated that “eliminating criminal penalties for those carrying small amounts of illicit drugs for personal use will reduce stigma and harm and provide another tool for BC to end the overdose crisis.” (BC Government News, 2022). BC's Minister of Mental Health and Addictions also asserted that: “By decriminalizing people who use drugs, we will break down the stigma that stops people from accessing life-saving support and services” (BC Government News, 2022). While these political figures mention the potential role of legislative reform to impact stigma, we contend that theorizations of the relation between drug (de)criminalization and stigma remain relatively under-researched, unclear, and context-dependent. Official statements such as these assuming a direct correlation between decriminalization and destigmatization fail to explain how the details of decriminalization (What kind? To what extent? What model?) might produce a specific stigma reduction effect (What kinds? For whom? How is it manifested?). The current study and data collection took place before this reform was proposed or enacted; however, this described setting contextualizes the experiences and opinions of our participants.
Methodology
The Canadian Drug Laws project was a cross-jurisdictional qualitative study conducted in BC, Canada, to gather perspectives on current drug laws and alternatives from people who use drugs themselves. This paper uses the qualitative data collected from interviews with 24 people who use drugs between July and September 2020. The criteria for participation were: 1) people aged 18 years or older, 2) people who used illegal drugs in the past 12 months, 3) people who were interested in discussing drug policies and experiences with police, 4) people who had access to a telephone (for the interview). We used a combination of purposive, snowball, and convenience sampling to recruit participants to maximize the breadth and depth of data generated while reducing selection bias by reaching hidden or hard-to-reach people who may not have otherwise heard about the study (Valerio et al., 2016). Snowball sampling included asking participants if they were interested in sharing the study information with others who met the inclusion criteria. The purposive sampling was informed through the concurrent data analysis to identify “information-rich” cases and characteristics and/or experiences (Becker et al., 2012). For example, initially, we only interviewed people residing in BC; however, in the later stages of sampling, we were curious if views and experiences were considerably different outside of the province and therefore also interviewed people from outside BC (n = 8). To recruit participants, we shared a recruitment flier through known networks of people who use drugs. The flier was also posted on social media and shared through several drug user networks social media accounts. Recruitment continued until we saw saturation in the information collected and were confident in the richness and depth of data. This occurred at 21 interviews, after which we conducted an additional three interviews. Interested participants made contact through the study email or phone number. Each interested participant received options to schedule an interview time and received a consent form to review before the interview. They were also given the option to have the consent form read to them verbally via telephone. Each participant received an honorarium of $30CAD. This study was granted ethical approval by Simon Fraser University Research Ethics Board.
Due to the COVID-19 pandemic and physical distancing observances present at the time of participant recruitment and data collection, all interviews were conducted over the phone. A semi-structured interview question guide was drafted collaboratively by the initial research team (AG,JF,NZ). We then consulted with people who use drugs from a provincial drug user network who provided feedback on the relevance, applicability, and appropriateness of the language and questions asked. Following these consultations, we piloted the interview guide with three people who use drugs from this network to test the questions and refine the instrument to ensure rich and relevant information was collected.
For the current study, our analysis focused on responses to questions relating to two main topic areas: 1) views on drug laws and alternatives and 2) the policing of drugs. To achieve both breadth of coverage across these two topic areas, as well as the depth of coverage within each, the questions posed were deliberately open-ended, for example: Can you tell me your opinion about drug laws here in Canada?; What are your thoughts on decriminalization?; Has the criminalization of drugs impacted your life in any way? If yes, how so?. To expand on the participants’ responses, probing questions were also asked. We also asked about basic demographics such as self-identified age, gender, ethnicity, and housing status. The sample included ten men, eleven women, two people who were gender non-conforming or genderqueer and one participant for whom gender information was not available. Sixteen participants self-identified as White, five as Indigenous or Metis, one as Black, and two as Eastern European. Twenty-two participants were in stable housing with two being in unstable or precarious housing. Ages ranged from 22 years to 63 years.
The interviewers (NZ & JF) discussed ideas and findings regularly throughout data collection which resulted in subsequent revisions to the question guide to elicit deeper responses related to our research aims. Transcripts were imported into NVivo version 12 to organize the data. As a means of ensuring participant anonymity, all identifying information was removed. A preliminary coding framework was collaboratively developed (AG, AB, NZ & JF), guided by both “in vivo” concepts (born from the language and terms used by the participants of our study) and “a priori” concepts (adopted from the relevant literature pertaining to the study) (Ritchie & Spencer, 1994). The coding framework was applied by two of the researchers in NVivo to organize the data (NZ & JF). The first author (BS) further refined the coding based on our study aims and analyzed the data within the broad category of “drug laws,” which included 18 sub-codes.
We conducted a thematic analysis (Braun & Clarke, 2006), commencing with a process of familiarization with the data, whereby members of the analysis team read, re-read, and reacted to a subset of transcripts while also making notes about analytic ideas (Braun & Clarke, 2021). We then collectively developed a multi-level coding framework to work systematically through the data, identifying relevant and meaningful information related to our research questions, as well as new and interesting concepts inductively. Coding was an iterative and rigorous process of reviewing transcripts, discussing, and refining that continued until all the data were organized under the final coding framework. Themes were based on important patterns of meaning across the data (Braun & Clarke, 2021). In line with thematic analysis, themes were refined and synthesized as we developed the findings and theme headings, and further synthesized throughout the writing process as we developed a coherent set of findings. Theme development was both deductive and inductive in that we were interested in certain topics, such as views on drug laws, but also were open to new and unexpected ideas related to this and other topics throughout the course of our data collection and analysis. As an example, people who use drugs unexpectedly spoke about the impact of drug laws on their ability to access adequate housing. During the coding and analysis process, it became clear that the various mechanisms and expressions of stigma: self, social, and structural were clearly impactful in the lives of people who use drugs and widely believed to be propagated through drug laws.
To promote the most accurate portrayal of our participants’ experiences, the themes, as well as the analysis and interpretation of our findings were discussed extensively by the researcher team throughout the course of both data collection and analysis (Brownlie, 2011). We also brought the findings back to people who use drugs—one researcher (JF) presented a preliminary report of the findings to both the Canadian Association of People Who Use Drugs and the Peer Engagement and Evaluation Project to gain insight into the relevance and validity of our findings. To further promote confidentiality and the anonymity of participants, identifying information, such as name, location, housing status and extent of interaction with the criminal justice system are excluded from this article and are not tied to individual quotes.
Findings
In this study, we were interested in the ideas, experiences, and recommendations expressed by people who use drugs concerning Canada's current criminal drug laws and alternatives. Below we present two main themes and several related subthemes that speak to participants’ views and experiences related to drug laws and drug law reform: 1) The experience of stigma as a consequence of criminalization; 2) The perceived benefits of decriminalization (see Table 1).
Themes and subthemes related to People Who Use Drugs’ views toward criminalization and drug law reform.
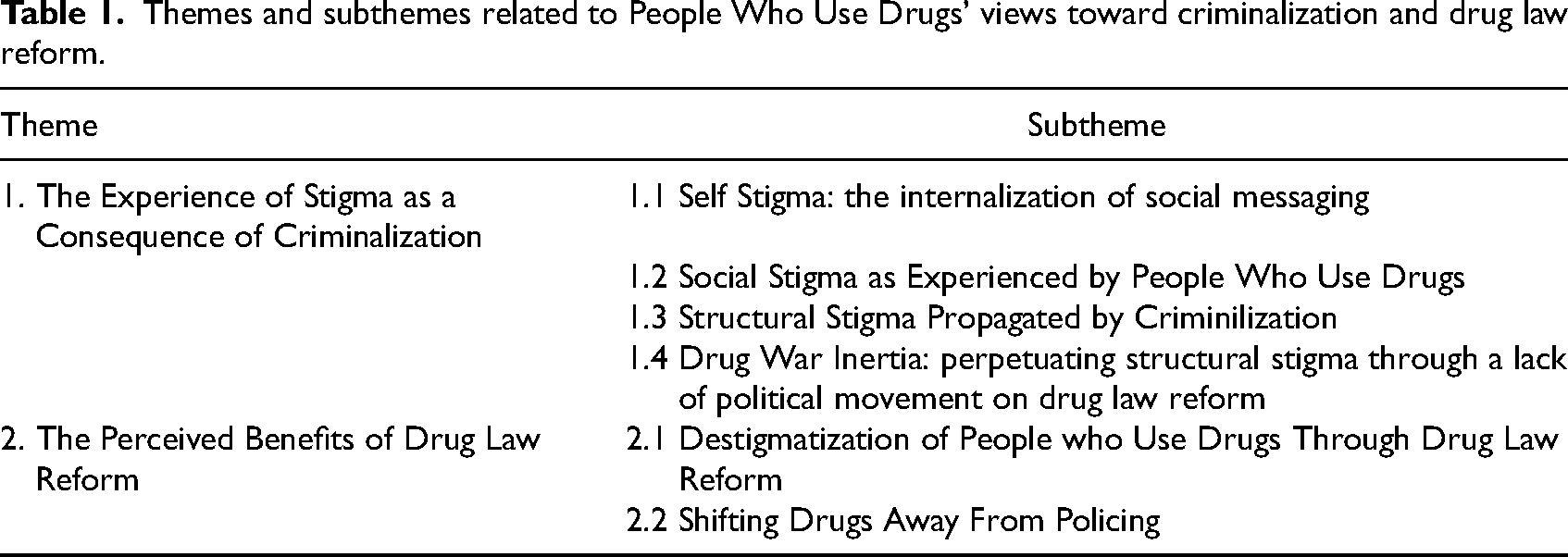
The Experience of Stigma as a Consequence of Criminalization
Participants shared a range of views toward Canada's drug laws, including diverse experiences related to law enforcement and/or criminal charges related to drug possession and/or trafficking. One idea that we did not ask about specifically, yet came up across all interviews, was that stigma was an inevitable consequence of drug criminalization—a clear symbolic message to the public about the value of people who use drugs in society: “…they’re just stigmatizing – the laws.” (Caucasian, Gender non-conforming, 33 years old). For our participants, drug laws themselves sent a clear message to them and the public that materialized in terms of moralized judgements of drugs and people who use them. This notion of moralization was clear from one participant who contrasted illegal drugs to those that are legally regulated and the impact that drug criminalization has on people who use illegal substances: “[Drug laws] are ridiculous…The criminalization of it causes the criminal act, it causes the stigma, it causes a lot of the harm…They don’t mind that I’m addicted to my anti-depressants…that's not morally wrong, but it's morally wrong if it's cocaine, if it's heroin, or whatever.” (Caucasian, Female, 63 years old)
Self Stigma: The Internalization of Social Messaging
Although not all participants had experienced incarceration or arrest, criminalization and the stigma associated with this criminalized social identity was acutely known to all participants. Participants often applied messages and stereotypes about people who use drugs to themselves, internalizing these negative messages and believing them to be true. Some were aware of this internalization of stigma whereas others were not. For example, when asked if the criminalization of drugs had impacted their lives in any way, one participant responded by explaining the ways in which they experienced these negative moral associations with drug use: “Yes, overwhelmingly so…it took me years and years to realize that because internalized stigma impacts your perception of self…your whole sense of self being negative comes from criminalization because the messaging that you can be a decent human being and be a drug user is completely counter-indicated by the idea that it is illegal, illicit and therefore morally wrong to a lot of people. So that kind of gets into your head and affects how you think about yourself.” (Caucasian, Gender-Queer, 44 years old)
Social Stigma as Experienced by People Who Use Drugs
Another form of stigma that participants felt was shaped by criminal drug laws was the widespread negative, moralized beliefs held regarding people who use drugs. In light of the existing evidence pertaining to causes and social determinants relating to drug ependency, this “social stigma” toward people who use drugs was perceived as outdated and inaccurate: “There's plenty of evidence now…what causes it [addiction] or what some of the causes are. So you don’t go on and tell me I’m a bad person.” (Caucasian, Female, 63 years old) “When something is illegal it creates or it normalizes this idea of something being bad and therefore, people who do it and break the law are bad. “(Indigenous, Male, 55 years old) “Public opinion is so harsh on substance use and not in a good way, not calling the government out in the context in which we should be…it's borne from our own ideals and the majority of the population are opposed to it or uneducated…”charge the people [who use drugs]”, and “force them to get help”, and “they’re all pieces of shit” (Caucasian, Female, 52 years old) “People do define success as total abstinence, but it doesn’t need to be. Some people can do it, some people can’t, but because of the stigma again…Nobody is a nasty dirty addict until somebody else finds out that you’re doing it.” (Caucasian, Female, 63 years old)
Structural Stigma Propogated by Criminalization
In participants’ narratives, structural stigma related to drugs was clearly attributed to Canada's criminal drug laws: participants believed that “the harms from drug laws…are greater than the harms from the drug themselves” (Indigenous, Male, 55 years old). Stigma was the crucial link between drug laws and the harms people experienced, especially the impact deriving from a criminal record on education and employment. For example, having a criminal record related to drug possession produced major structural barriers in participants’ lives: “[A criminal record] made it really hard for me to start over. I can’t get a job with anything that I really wanted to do before I started using drugs, and now that I have cleaned up… it's making it really hard for me to move on with my life. I wanted to go to school to be in the mental health field, but I’m not allowed to because of my criminal record.” (Caucasian, Female, 22 years old) “So, people are quite often, you know, forced to do sex trade work, people get beat up, murdered, all kinds of horrible things that come from our current [drug] policies. They [drug laws] just really add to preventable negative outcomes for people.” (Caucasian, Female, 52 years old)
Being forced into the illegal market, both for means of employment and for accessing illegal drugs presented clear dangers, including exposure to varying degrees of violence. Most participants felt that a direct consequence of criminalization was the push toward more marginal spaces of income generation and social life: “My opinion is that for people who use drugs, it is a result of the social conditions surrounding…the implementation of drug laws in terms of…people having to resort to desperate means to afford their drug of choice…”(Mixed Caucasian, Male, 37 years old) “…the main problem, which is the criminalization of drugs…this criminalized system that makes people sicker…less able to engage in activities that would help them achieve some kind of stabilization or like achieve their version of what happiness looks like…”(Caucasian, Male, 64 years old) “First of all, the current drug laws, they inflict needless suffering on people who are already disempowered… They make their likelihood of recovery and rehabilitation very unlikely.” (Indigenous, Male, 46 years old)
Drug War Inertia: Perpetuating Structural Stigma Through a Lack of Political Movement on Drug Law Reform
Participants were aware of ongoing efforts to liberalize drug laws and implement progressive drug policy interventions in Canada (largely driven by people who use drugs themselves), such as increased access to harm reduction services and the implementation of safe supply programs. However, most participants called for more government action, in particular drug decriminalization. Overall, there was a sense of disappointment and frustration toward the government's unwillingness to make these legal changes, with one participant passionately stating: “the present war on drugs and the present inertia of the overdose crisis is really government supported genocide” (Caucasian, Female, 52 years old). Withholding from this desired legal reform sent a clear message to the wider society about the ascribed value and worth of people who use drugs within society: “We are talking about ending stigma but if the federal government is not, if Justin Trudeau is not behind decriminalization? What message does that send…?” (Caucasian, Gender non-conforming, 33 years old). By continuing to approach this crisis through the lens of criminality, the Canadian government was believed to be perpetuating a view of people who use drugs as criminals: “I believe that criminalization and the drug laws in Canada still set the tone around stigma and that prevents proper policy use, and laws from being passed…I think they’re pretty archaic and backwards, and not helpful.” (Caucasian, Gender-Queer, 44 years old) “For some reason alcoholism is now accepted as a disease, or health condition. But there's always been that moral line, it's a disease if its alcohol, but for any other substance it's a moral defect….there's kind of a similar thing with…cannabis now that its legalized there's a store on every corner and we’re all allowed to do it all of a sudden it [cannabis] is okay and its not bad anymore just because the government says it's okay.” (Caucasian, Female, 63 years old)
For many participants, a common understanding was that it was stigma, a product of drug criminalization, that prevented the innovation of “proper drug policy” (Caucasian, Gender-Queer, 44 years old) in other areas such as the wider uptake of safe supply programs. For many, the primary barrier to decriminalization and wider drug policy reform was the lack of political will within Canadian politics. This lack of political will was highlighted when comparing the government's actions in response to COVID-19 versus those in addressing Canada's ongoing drug toxicity crisis: “I think the two [simultaneous pandemics] are the prime examples of the stigma towards PWUD. We have two public health emergencies killing people in every province. In a lot of provinces overdose deaths have raised, but we don’t have the same support, we don’t have the same financial resources, we don’t have the same social or public support. It's very much the othering of the other crisis.” (Caucasian, Female, 31 years old)
The comparison between the robust and adequately financed national response to the COVID-19 pandemic and that of the ongoing drug toxicity crisis was believed to symbolize the priorities of the government. Despite being two very different public health issues, the stark contrast between responses to these two health emergencies was seen to epitomize the unchallenged and well-entrenched inertia of stigma toward people who use drugs. This difference in responses was not only demoralizing for people who use drugs but also sent a strong message to Canadians about the worth and value of people who use drugs in the eyes of the government. What is clear from these accounts is that people who use drugs believe that drug laws and government (in)action play a major role in creating and perpetuating the various levels of stigma facing people who use drugs within Canadian society.
Perceived Benefits of Drug Law Reform
In the context of participants sharing how Canada's drug laws were currently “not working,” they described their support for the decriminalization and legalization of illegal drugs. The perceived benefits of these reforms included destigmatization, increased social support, and a reduced presence of police in the lives of people who use drugs.
Destigmatization of People Who Use Drugs Through Drug Law Reform
Several participants cited the role of decriminalization in alleviating social stigma and reshaping public views held toward people who use drugs: “Anti-stigma campaigns are slightly effective but they feel a little bit ugly to me. With anti-stigma campaigns as long as we’re [PWUD] criminalized, you’re not gonna change the mindsets of people in the most effective way that is necessary… That is why, political leaders are using those reasons [stigma] and excuses to not be effective.” (Caucasian, Female, 52 years old)
This participant explains her belief that anti-stigma campaigns used to target stigma are ineffective and are used by political leaders as a means of appearing to be tackling the drug toxicity crisis without committing to the required structural change. While decriminalization was seen as the best way to address stigma in the short term, some participants believed that more robust reform through drug legalization should be the intended long-term goal: “Decrim is super important but I think it's a short-term goal as opposed to [the] longer-term goal of actual legalization of substances.” (Caucasian, Female, 52 years old) “If it was legalized they [kids] are not going to be afraid to say ‘no, my mom uses every day’, because now if they could say that without any repercussions.” (Demographics N/A) “It [decriminalization] will take away from the [focus on] enforcement. There will be more open, creative dialogue, you know, it's not underground any more people will talk about it openly” (Indigenous, Male, 46 years old).
Shifting Drugs Away From Policing
Participants believed that decriminalization could shift the paradigm around drugs, most notably by altering the relationship between police and people who use drugs: “It's not [that] police are bad people they are just conforming to a system and it turns people's - it socially constructs the way they think, right” (Caucasian, Male, 30 years old). Participants felt that by removing people who use drugs as targets of criminalization, policing practices and objectives could become more supportive of people who use drugs, as opposed to their primary focus on deterrence and punishment, enshrined through criminal law. Further, in removing the criminality associated with drug use, concerns about the threat of arrest would also be removed: “The constant threat of police and being arrested, at any time and having your life ripped apart. That's just a terrifying threat that hangs over you all the time.” (Caucasian, Male, 64 years old) “Just needing help and knowing that…what you’re doing is being criminalized. A lot of the time there's a first responder to a situation right and if they [police] are the first responder and what you’re doing is illegal then you’re going to be prosecuted for that activity. If [illicit drugs are] decriminalized then they defer you and they give you access to help and support, they [medical services] become the first point of contact. That first point of contact currently, or usually ends up being prosecution or incarceration and…I don’t think it needs to go there. If…they were able to defer you for support, it…would really help.” (Indigenous, Male, 46 years old)
Discussion
By taking a critical realist approach, this study examined how people who use drugs experience, perceive, and interpret Canadian drug laws, the structural manifestations of stigma and potential alternatives such as the decriminalization of illegal drugs. Our participants suggested that Canada's current legal framework is responsible for producing and perpetuating the stigma people who use drugs experience across multiple areas of life and levels of manifestation: structural, social, and within the self. Stigma was understood as being a direct result of the criminalization of drugs and therefore as having been politically produced (as drug laws were made or justified) and perpetuated through government reluctance for drug law and policy liberalization. To reduce stigma and its consequences, drug law reforms such as decriminalization and legalization were perceived as viable and urgent solutions. These findings highlight the embedded nature of stigma in the lives of people who use drugs as well as the symbolic effect that policy direction, allocation of resources, and political attitudes and action can have in producing or perpetuating stigma among people who use drugs and society at large.
The accounts of participants in our study support the work of scholars demonstrating how structural stigma negatively impacts mental health, social and environmental conditions for people who use drugs (Friedman et al., 2021; Hansen et al., 2014; Hatzenbuehler & Link, 2014; Livingston, 2020; Major et al., 2018; Perales & Todd, 2018; Pugh et al., 2015). Sibley et al. (2020) discuss how identity and the social process of identity formation have important health implications for people who use drugs. Within a social constructionist framework (McCullough & Anderson, 2013), identity is a culturally negotiated phenomenon that is not static but constantly evolving in relation to our socio-cultural context. In turn, conceptions of self are transformed by the world around us. Sibley and colleagues suggest that the progression of certain people who use drugs into drug dependency brings about a degree of identity transformation—one's identity is diminished by the socially ascribed negative traits of someone who uses drugs. This process has significant negative impacts on mental health (Sibley et al., 2020). The direct impact of stigma on mental health is again reaffirmed through the accounts given by our participants.
The social marginalization created through stigma also hinders people who use drugs from accessing health care services (Sibley et al., 2020). Our findings support the assertion that drug dependancy can be conceptualized as a “person in a particular social world disorder” (Jacobs & Flanagan, 2013, p.3) due to the increased understanding of the importance of the social, political and legal context within the process of achieving stability and wellbeing amidst drug dependancy. As such, the reduction of stigma toward people who use drugs could in fact have important implications within efforts to facilitate and increase the well-being of people who use drugs and the pursuit of positive change.
In addition to the more instrumental concerns of how stigma experiences may worsen mental health, block access to services or prevent wellbeing, our data also highlights how participants interpret the criminalization of illegal drugs as a process of marking and categorization. Amidst the rise of anti-stigma “discourse” surrounding the drug toxicity crises in Canada and beyond (Fischer, 2020), it is important to draw attention to how people who use drugs themselves understand their exclusion, stereotyping, and dehumanization as a moral concern, not simply a matter of reduced access to resources (Bayer, 2008).
In line with this observation, our findings have important implications for conceptualizations and theories of how stigma is produced. In research examining stigma within the HIV/AIDS epidemic, Herek (1998) wrote extensively about how the process of law-making can be applied to the stigma experienced by people who use drugs. Laws and policy interventions are thoughtfully considered between politicians, lobbyists, the public, and the media. This democratic process reveals to people who use drugs “first, that their fellow citizens and elected representatives endorse stigmatizing views; second, that their fundamental rights are open for debate; and third, that they have relatively limited power to resist the dominant ideology” (Livingston, 2013, p.10; Friedman et al., 2021). Building on this argument, the experiences and perspectives of our participants suggest that it is the law that enshrines our social norms and values and identifies behaviors that warrant being punished and socially ostracized. Through this process of criminalization and everyday enforcement by police, people who use drugs believed that laws served to reinforce and legitimize the exclusion and stigmatization they experience because of their use of illicit substances.
Participants openly and profoundly believed that drug laws produced the negative beliefs, moral associations, and structural inequities experienced by people who use drugs in Canada. This matters, not only because our findings highlight the fact that people who use drugs experience stigma in tangible and clearly impactful ways, but also because it suggests a top-down, unidirectional link between structural, social, and self stigma. The identification of this link within the field of drug policy highlights the potential for structural interventions, such as the liberalization of drug laws, to be more effective than those at the individual or social levels to address stigma. With regards to what is currently being done to fight the very real and damaging effects of stigma, people who use drugs questioned the effectiveness of anti-stigma campaigns such as those that focus on addressing stigmatizing language only (e.g., “Say ‘people with a substance use disorder’ instead of ‘addict’,” see Ashford et al., 2019; Kelly et al., 2021; Livingston, 2021b). While these linguistic interventions may (for some people) help humanize people who use drugs (studies show small to moderate stigma reduction effects within controlled, experimental manipulations of person-centered language) they can at best only be a starting point. In a rare critique of dominant anti-stigma discourse and Canadian government policy reports on stigma, Fischer (2020) argues that addressing stigma through the individualistic types of interventions that government and public health bodies tend to prioritize is merely a convenient way to position stigma as an isolated entity. By focusing on framing and in turn tackling stigma alone, as if it has single-handedly caused the drug toxicity crisis, politicians can deflect from the needed legal reform that may not only address the structural foundations of the drug toxicity crisis but simultaneously address the production and perpetuation of stigma. Although there exists a large body of literature which documents and examines the stigmatization of non-criminal behaviors (eg., smoking, obesity, and mental health; Barry et al., 2014; Phillips & Shaw, 2013) within the context of substance use, there are also findings from recent legalization projects (Aranda et al., 2021; Hughes & Stevens, 2007; Osburne & Fogel, 2017) which suggest that stigma and in turn its negative impacts can be addressed through legal reform. Decriminalization, at its core, removes the stigmatizing label of “drug user” as “criminal,” which categorizes people who use drugs as deserving of structural and social stigma (Fischer, 2020). The legalization and regulation of illegal substances would further symbolize the destigmatization of people who use drugs, especially if it were accompanied by shifting the allocation of resources from policing drug use toward supporting public health and social development. Our participants believed that the most direct and impactful intervention to reduce both social and structural level stigma would be the enactment of drug policy reform.
Most existing evaluations of stigma capture the subjective perceptions of people impacted at the self and social levels (Adlaf et al., 2009; Latkin et al., 2010; Meyers et al., 2021; Palamar et al., 2013; Stengel, 2014). In these studies, the focus of participants is to disclose overt, everyday, interpersonal experiences of discrimination. This research directive often produces findings that speak to risk factors that suggest individual level interventions as a means of alleviating stigma. In contrast, the impact of more pervasive structural factors is much harder to measure and identify. In turn, little ground has been made in conceptualizing how laws and policies produce or perpetuate stigma (though see Seear et al., 2017). As a result, in relation to the alleviation of stigma pertaining to people who use drugs, few studies are yet to acknowledge “the law” as a critical object of analysis.
Policy Implications
Our research supports the findings of scholars from other fields (Blake et al., 2018; Meadows et al., 2021; Pescosolido et al., 2008) who highlight the unidirectional (structural to social) process in which laws and policies shape forms of social stigma directed toward marginalized groups. Our participants felt strongly that stigma is perpetuated through political inaction on drug law reform in the face of injustice and preventable suffering. As evidenced by Twenge and Blake's (2021) research examining stigma following changes to same-sex marriage laws in the U.S., changes in public perception and the alleviation of social stigma may in some situations follow changes in the law. Participants discussed this exact phenomenon in relation to cannabis and alcohol regulation, suggesting that the true destigmatization of people who use drugs would become more possible following the decriminalization of drugs.
However, in other social contexts, destigmatization has not necessarily followed decriminalization. For example, Hughes (2017) outlines how the decriminalization of abortion in Maritime Canadian provinces did not coincide with the destigmatization of abortion. Likewise, Abel and Fitzgerald (2010) demonstrate how the decriminalization of sex work in New Zealand may have contributed to reductions in various forms of stigma for sex workers but by no means eliminated stigma. In the realm of drug decriminalization specifically, people who use drugs from international contexts that have enacted various versions of “decriminalization” suggest that reductions in stigma have not always followed, or if they have, they have not necessarily resulted from the decriminalization law itself (INPUD, 2021). As drug-related stigma becomes more widely identified as an internatonal phenomenon and criticized on the international stage (UNODC, 2016; Yang et al., 2018) our analysis offers a lens through which the structural implications of drug laws can be considered within international contexts. While our findings suggest people who use drugs have good reason to believe that drug decriminalization would create downstream impacts on the stigma they experience, more research is needed to assess how different models of decriminalization may impact different levels of stigma (Greer et al., 2022).
We are currently at an important crossroads within the history of Canadian drug policy. While we remain at the height of the national drug toxicity crisis (Snowdon, 2022), since collecting our data in 2020, several reforms have occurred across the province of BC demonstrating that further, more meaningful reform is possible. On the 22nd of November 2021, the city of Vancouver became the first city in Canada to be successful in their application for a federal exemption from the Canadian Controlled Drugs and Substances Act (CCDSA) to permit a city-wide model of decriminalization. Despite this reform, these changes are implemented as a pilot (January 31st 2023 to January 31st 2026) and include a threshold of possession of 2.5 grams, significantly lower than what experts and advocates had recommended (Canadian Drug Policy Coalition, 2022). The Canadian Association of People Who Use Drugs believes by continuing to criminalize this population of people who use drugs, the Canadian Government continues to violate the Canadian Charter of Rights and Freedoms. This push-back once again demonstrates the importance of meaningfully including the voices of people who use drugs within policy discussions as a means of mitigating the risk of unintended consequences within drug policy interventions. Our study speaks to the importance of taking seriously the voices of people who use drugs both within research and broader policy discussions. Finally, it is important to note that decriminalization is at best a partial cure for drug toxicity deaths and further measures such as the legal regulation of safe supply would be necessary to reduce current levels of overdose death (Bonn et al., 2020, 2021; Ivsins et al., 2020; Scheim et al., 2020; Tyndall, 2020).
Limitations
The study sample was partly recruited through a drug user network in BC that is fairly involved in drug policy reform and programming in the province. As such, the views toward drug law reform and narratives may be more homogenous than people who use drugs who are less connected to drug policy discourse. However, knowing the potential influence of dominant narratives in this network, we purposively sampled participants outside of this network and outside of BC altogether. Future research will benefit by seeking more diverse perspectives from different communities of people who use drugs. A further limitation was having to collect data over telephone due to COVID-19 social distancing requirements. We recognize that certain individuals without access to a telephone likely could not take part in our study. We attempted to address this issue by facilitating interviews through telephone access through community organizations and friends of potential participants. Additionally, in-person interviews may have elicited a greater rapport between the participant and interviewer.
Conclusion
From the perspective of many people who use drugs, criminal drug laws produce and perpetuate stigma. The clear recommendation of our participants was that in order to bring about a concrete reduction in the harms associated with self, social and structural stigma, the liberalization of drug laws and policies, and in particular the decriminilization of drugs is imperative. There is already a wealth of evidence demonstrating how the criminalization of drugs exacerbates drug-related risks and harms. This study explicitly highlights how drug criminalization is a root cause of drug-related stigma. Borne from the experiences of people who use drugs, this is the central finding of this paper and a finding we believe needs to be explored with further research, particularly within evolving drug policy contexts.
Footnotes
Acknowledgments
We would like to thank both the people who use drugs who informed the study design, question guides, and reviewed drafts of our findings as well as those who participated in our study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by the William and Ada Isabella Steel Fund and Small Social Sciences and Humanities Research Council (SSHRC) Grant through Simon Fraser University.