
Abstract
Background
Substance use stigma has been framed as contributing to the drug toxicity crisis. We theorize the political function of drug criminalization as contributing to a system of stigma that exerts social control over people who use illicit drugs (PWUID). Consequently, drug decriminalization may be a potential destigmatizing solution. Since decriminalization is often positioned as an antistigma intervention targeting the public, it is important to understand how laypeople conceptualize decriminalization.
Methods
We acquired, via a Freedom of Information request, 221 deputations sent to the City of Vancouver regarding Motion B.4, which would advance decriminalization. We used reflexive thematic analysis to explore: (1) how laypeople conceptualized drug (de)criminalization and its relation to the (de)stigmatization of PWUID; and (2) the potential implications of the various conceptualizations of (de)criminalization for the autonomy of PWUID.
Results
Supporters of Motion B.4 commonly assumed decriminalization would destigmatize PWUID. Supporters also often argue that the drug toxicity crisis is a public health problem, not a criminal one. However, the public health model of decriminalization advocated by some supporters still limited the autonomy of PWUID. Meanwhile, those opposed commonly positioned social control of PWUID as necessary, including opponents who argued that decriminalization was a form of systemic neglect that abandons PWUID. This view was echoed by some proponents, notably those who argued for a public health model of decriminalization. Finally, some proponents asserted that PWUID should be included in the policymaking process, though few deputations came from self-identified PWUID. All PWUID argued that decriminalization must exclude the police.
Conclusion
Our analysis of lay perspectives on decriminalization highlights the importance of models that adequately address all levels of stigma for PWUID. Models that fail to preserve the autonomy of PWUID are likely to reproduce their stigmatization.
Introduction
Since 2016, over 42,000 lives have been lost to the drug toxicity crisis in Canada (Public Health Agency of Canada, PHAC, 2023). In 2023 alone, there were an average of 78 opioid-related poisoning emergency department visits per day and 17 hospitalizations per day. The majority of these visits and hospitalizations were due to accidental poisoning. Policymakers and researchers alike have positioned substance use stigma as a contributing factor to the drug toxicity crisis (PHAC, 2023; Tyndall & Dodd, 2020). One theory of stigma defines it as a form of social control. Within this context, criminalization is theorized to be a stigmatizing process (Tyler, 2020; Tyler & Slater, 2018). Policymakers often suggest drug decriminalization as a potential structural intervention to target both substance use stigma and the drug toxicity crisis. However, little is known about how laypeople, who are the targets of this intervention, think about decriminalization. In this paper, we argue for the importance of understanding the perspectives of laypeople on decriminalization and its potential to reduce stigma toward people who use illicit drugs (PWUID). 1 Understanding these perspectives may shed light on the potential pitfalls of decriminalization policies and their potential to restigmatize PWUID. They may also inform the creation of decriminalization policies that are more likely to meaningfully address the complex nature of substance use stigma.
The British Columbia Context
In Fall 2020, the City of Vancouver received emails, letters, and speeches (i.e., deputations) from members of the community (i.e., laypeople), expressing opinions on Motion B.4, Work with Senior Governments to Address the Overdose Crisis. The motion, made on November 25, 2020, by then Mayor Kennedy Stewart, directs the Mayor to request an exemption from the federal government to the Controlled Drugs and Substances Act (CDSA) that would functionally “decriminalize” the possession of illicit drugs. This motion attempted to address the ongoing drug toxicity crisis, which has disproportionately affected British Columbia (B.C.). B.C. had the highest rate of accidental opioid toxicity deaths in 2022, comprising 32% of those in Canada (Public Health Agency of Canada, 2023). Motion B.4 was passed unanimously after amendments, an important early milestone in B.C.'s journey toward a three-year pilot project decriminalizing small amounts of opioids, crack and powder cocaine, methamphetamines, and MDMA in January 2023 (Government of B.C., 2023).
Decriminalization and Stigma Reduction Interventions
Motion B.4 cited then B.C. Premier John Horgan in naming drug decriminalization as “a necessary next step” in the destigmatization of PWUID. Substance use stigma has often been framed as a contributor to the drug toxicity crisis and drug decriminalization has been posited as a potential structural solution. Specifically, stigma is conceptualized as preventing help-seeking behavior, leading to increased isolation and risk for accidental overdose (Public Health Agency of Canada, 2023). Drug prohibition and substance use stigma have both been theorized as structural mechanisms fueling the drug toxicity crisis through policies that harm PWUID (e.g., strict limitations on opioids prescribed for harm reduction purposes; Tsai et al., 2019; Tyndall & Dodd, 2020). However, most antistigma research and interventions tend to target individual behaviors and attitudes (Livingston et al., 2012; Paluck et al., 2021; Rao et al., 2019). In the context of substance use stigma, a systematic review by Livingston and colleagues (2012) found that although individual interventions demonstrate positive short-term effects for stigma reduction, their long-term effects are unknown. From a more general prejudice reduction perspective, a meta-analysis by Paluck and colleagues (2021), which primarily consisted of individual-level interventions, found that effect sizes tended to be modest. As Paluck and colleagues (2021) put it, individual-level interventions are like “remedies for low-grade illnesses… [and] stronger medicine is demanded by global conditions in which prejudice is expressed through violence, discrimination, and exclusion” (p. 555). They go on to argue that a shift in focus to interventions that target prejudice at its structural roots is necessary. Research suggests that public policy reform addressing structural stigma has the potential to further influence individual behaviors, and thus social stigma, by reflecting and signaling a shift in cultural values (Cook et al., 2014). Indeed, activists, policymakers, and researchers are increasingly turning to decriminalization as a potential structural intervention to address substance use stigma and the drug toxicity crisis.
Stigma as a System of Social Control
Motion B.4 explicitly mentions destigmatization as a goal, but what is stigma? Goffman (1963) defined stigma as “arising when an individual, because of some attribute, is disqualified from full social acceptance” (p. 9). Since Goffman's seminal work, researchers have conceptualized stigma as operating on multiple levels, namely structural, social, and self (Livingston et al., 2012). Structural stigma is defined as the systemic degradation of a group via policies and institutions that limit their rights (Livingston et al., 2012; Scher et al., 2023). Social stigma refers to the negative public perception of a group. Finally, self-stigma is defined as the internalization of negative public perceptions among people who belong to a stigmatized group (Livingston et al., 2012). However, as Scher and colleagues (2023) point out, Goffman's definition of stigma is largely apolitical and missing an analysis of social power. It lacks an account of how and for what purpose the marks of stigma are placed upon groups (Tyler, 2020). In contrast, Tyler and Slater (2018) define stigma as a system of social control with a political function. They argue that stigma is not a preexisting condition of certain groups of people but rather is created relationally between not only people but also between people and systems. In this case, substance use stigma is partially created when people interact with the criminal punishment system. These interactions stigmatize the individual by marking them for exclusion (e.g., criminal records; Tyler, 2020). From this perspective, stigmatization acts as a means to remove social power from stigmatized groups and to give social power to nonstigmatized groups and to institutions and systems.
Drug Criminalization as a Stigmatizing System
When considered from Tyler and Slater (2018)'s (re)definition of stigma, drug criminalization can be conceptualized as a structurally stigmatizing process. Prohibition reifies emergent norms around substance use, namely that PWUID are inherently criminals, thereby creating or reinforcing negative associations with PWUID and stigmatizing them as a group. Negative associations with substance use are deeply intertwined with the racist and colonial roots of drug prohibition in Canada, which can be traced back to attempts to convert Indigenous peoples to Christianity and to anti-Chinese sentiment contributing to Canada's early antiopium laws (Boyd, 2017; Malleck, 2015). Colonial drug policies required Indigenous peoples to revoke their legal Indian status to be allowed to drink alcohol legally (Campbell, 2008). Meanwhile, opium was a legal vehicle through which the exclusion of Chinese people was justified (Boyd, 2017; Malleck, 2015). In both cases, lawmakers positioned drugs as a foreign, corrupting threat to the “purity” of the white, middle-class Christian, thereby justifying prohibition (Boyd, 2017). This positioned substance use as a stereotypically racialized activity, and racialized people in Canada continue to be disproportionately criminalized for their substance use today (Fataar et al., 2024; Owusu-Bempah et al., 2023; Wiese et al., 2023).
The effects of criminalization (e.g., criminal records) then act as a discrediting attribute that marks an individual for surveillance, capture, and control (Pescosolido & Martin, 2015; Tyler and Slater, 2018). Indeed, criminal law can be seen as an instrument used to define the social status of, and thus to exert social control over, various groups, denigrating some as criminals while protecting others (Burris, 2006). In this context, individual-level antistigma interventions seem inadequate for removing the complex structural layers of stigma imposed by criminalization (Scher et al., 2023). Consequently, drug decriminalization may be an important component of a robust movement toward the broader goal to destigmatize PWUID.
Public Policy's Role in Stigma Reduction
This raises the question: How do changes in public policies impact the stigmatization of specific groups at different levels of stigma? Hughes notes that though policy changes moving previously illegal activities into decriminalized or legal territory may signal a shift in social norms, they do not necessarily result in stigma reduction at an individual level. For example, although abortion is legal in Canada, getting an abortion remains a stigmatized activity (Hughes, 2017). Similarly, Tankard and Paluck (2017) found that the United States Supreme Court's 2015 ruling to legalize same-sex marriage changed people's current and future perceptions of Americans’ support for gay marriage (i.e., perception of wider social norms), but did not necessarily change their personal attitudes or beliefs regarding gay individuals. Together, these studies suggest that public policy reforms such as decriminalization may impact structural stigma, by removing systemic barriers to accessing rights, but may not necessarily influence social stigma at an individual level.
We know even less about the role that drug decriminalization may play in reducing social stigma toward PWUID. Gilroy (2023) provides the only statistical analysis of how Portugal's implementation of drug decriminalization may have impacted substance use stigma. The author investigated stigmatizing attitudes toward PWUID longitudinally in Europe, including in Portugal, with timepoints both before and following Portugal's implementation of decriminalization in 2001 (i.e., 1990, 1999, 2008, 2017). In the study, participants in Portugal rated “drug addicts” as the least desirable neighbors compared to other stigmatized groups at all time points (Gilroy, 2023). However, Portuguese participants’ desire for social distancing from “drug addicts” decreased over time. Notably, there was an increase in desire for social distancing between 1999 and 2008, encompassing the implementation of decriminalization in Portugal. However, the downward trend continued between 2008 and 2017. This suggests that decriminalization may have been associated with a negative short-term impact on participants’ views of “drug addicts,” but a positive long-term one. Though the data are correlational, the major relevant policy change during the study period was the decriminalization of drugs in Portugal, suggesting that decriminalization may have contributed to this improved overall view toward “drug addicts.”
In contrast, the negative view toward using marijuana or hashish in Portugal remained stable over time (i.e., it was unaffected by the decriminalization of drugs), as participants rated using these drugs as the “least justifiable” activity for people to engage in compared to homosexuality, abortion, divorce, and prostitution. Thus, the Portugal model of decriminalization may have affected public views on different groups of PWUID differently. Specifically, it seems that drug decriminalization was associated with an overall reduction in social stigma toward “drug addicts,” but was not associated with a corresponding reduction in social stigma toward people who use marijuana or hashish. Overall, the literature suggests that we cannot take for granted that drug decriminalization will contribute to the destigmatization of PWUID, nor that it will affect different levels of stigma or groups of PWUID in the same manner.
The Value of Lay Perspectives
The policymaking process for decriminalization has historically failed to consider and include the perspectives of those that such policy changes would directly affect: laypeople, especially PWUID (Greer & Ritter, 2019). However, given the context of current literature and public discourse, it is clear that decriminalization models have been conceptualized by a variety of groups, including laypeople. Importantly, there is no single model of decriminalization. The details of different decriminalization policies vary in how much autonomy they grant PWUID, and we argue that this has important implications for their potential effects on substance use stigma. Those advocating for decriminalization have conceptualized autonomy in this context as referring to PWUID's right to make their own decisions regarding their substance use (Canadian Public Health Association, 2024; Vancouver Area Network of Drug Users, 2010). This includes decisions such as whether to use substances, which substances to use, how much to use, and whether to seek substance use services, to name a few. In this study, we align our understanding and use of the word “autonomy” with this conceptualization.
Research examining lay perspectives is also lacking. To our knowledge, only two studies to date have examined PWUID's perspectives on decriminalization (Ali et al., 2023; Scher et al., 2023), and another has investigated police perspectives (Greer et al., 2024). However, none of these studies include the voices of the broader public. Research on technological and environmental policy has demonstrated the utility of including lay perspectives in policymaking (Lopez Cerezo and Gonzalez Garcia, 1996). Specifically, the inclusion of lay perspectives can make the policymaking process more efficient and effective by filling knowledge gaps that experts, who may be outsiders to the issue or community in question, might have. In the context of substance use policy, decriminalization is often positioned as an antistigma intervention targeted toward the public at large, and thus it is important to understand how laypeople, the people that these policies are targeting, think and talk about decriminalization and its relation to stigma. What do laypeople mean when they talk about decriminalization? What policies are they envisioning, and what do they think those policies will achieve, specifically regarding the various forms of stigma that PWUID face? These questions are important to answer, as they may help policymakers more effectively address substance use stigma through progressive drug policy. By better understanding how laypeople, especially PWUID, conceptualize decriminalization and its potential consequences, policymakers may also be better equipped to produce legislation that does not unintentionally restigmatize PWUID.
The present study aims to fill this gap by answering the following research questions: How do laypeople conceptualize drug (de)criminalization and its relation to the (de)stigmatization of PWUID in the context of Motion B.4 in the City of Vancouver? What are the potential implications of the various conceptualizations of (de)criminalization for the autonomy of PWUID?
Materials & Methods
Procedure
On March 3, 2021, the second author made a Freedom of Information request to the City of Vancouver for the written submissions regarding Motion B.4 from September 1, 2020, to March 3, 2021. We acquired 221 deputations with identifying information redacted. These deputations comprise the data for this study. Some of the deputations included form letters facilitated by various groups, namely Moms Stop the Harm, 2 the Coalition of Peers Dismantling the Drug War (CPDDW), 3 the Public Health Association of British Columbia and the Canadian Public Health Association (CPHA), 4 and a group of medical students at the University of British Columbia. 5 Since the purpose of this study is to analyze the implications of the arguments people made regarding decriminalization and not to focus necessarily on the most common arguments made, only unique deputations were considered, with each form letter counting as a single case. Personalized form letters were counted as unique cases. Of the 104 unique deputations, 95 (91.3%) were in support of the motion, while 9 (8.7%) were opposed. 6 Only 2 (1.9%) letters indicated they were written by PWUID, and 102 (98.1%) were from people who did not indicate that they were PWUID. Detailed case characteristics can be found in Table 1.
Case Characteristics.
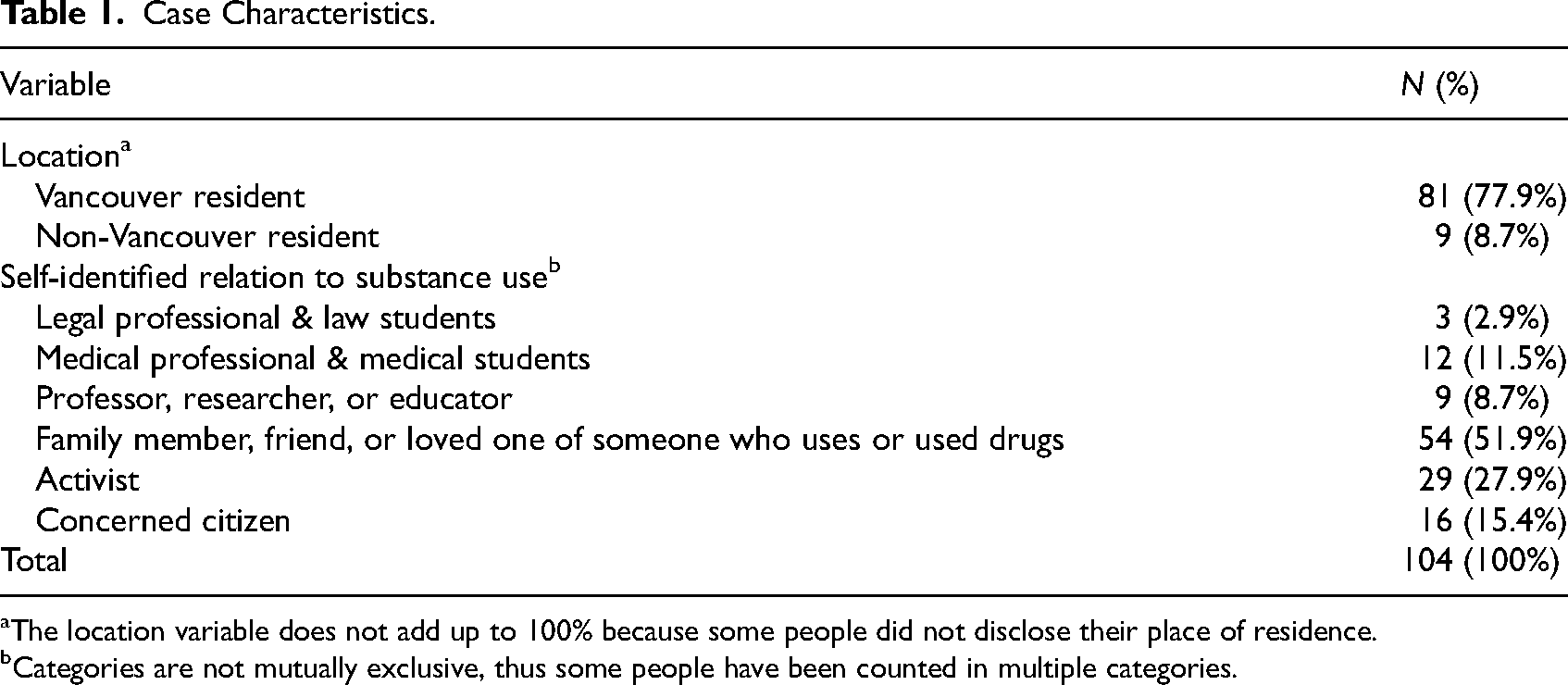
The location variable does not add up to 100% because some people did not disclose their place of residence.
Categories are not mutually exclusive, thus some people have been counted in multiple categories.
We analyzed the data using reflexive thematic analysis, an iterative process of coding patterns in both manifest (directly observable) and latent (implicit) meanings of data (Braun & Clarke, 2022). Patterns are then identified to create themes in relation to the research questions. First, we reviewed the deputations to familiarize ourselves with the data and to gain an overall understanding of its content. Then, the first author created a coding framework based on the research questions and the deputations. Using the coding framework, the first author sorted quotes from the deputations into relevant codes. Throughout this process of reviewing and coding the data, the first author removed and added codes from the framework as data was interpreted and reinterpreted. Additionally, the first author met with the second author weekly to discuss the coding process and multiple perspectives on initial interpretations of the data. These meetings often resulted in changes to the coding framework to reflect new insights. The first author repeated this process until reviewing the data did not result in new interpretations of the framework, either in isolation or when discussed with the second author. Next, using the research questions as a guide, the first author synthesized the codes to create themes that highlight patterns in the data. Creating themes included a process of meeting with the second author weekly to discuss evolving interpretations of the data. Themes were changed as new insights were created through discussion.
Our ontological approach to data analysis was critical realism. Critical realism posits that the world consists of two “layers”: one that encompasses events and experiences, or in other words, the things that happen; and another that includes the structures and power dynamics underlying the things that happen (Patomäki & Wight, 2000). Research from a critical realism perspective aims to identify and illuminate “the structures, powers, and tendencies that structure the course of events” (Patomäki & Wight, 2000). Meanwhile, our epistemological approach to data analysis was social constructionism. Social constructionism argues that people create a joint or social understanding of the world (Galbin, 2014). This socially constructed meaning then intersects with, influences, and is influenced by other aspects of reality. Research from a social constructionism view, in part, aims to elucidate the meanings constructed in discursive language.
Given the politicized nature of drug policy reform, both authors reflected on how their positionality could impact the analysis. The first author is a multiply marginalized (queer, agender, neurodivergent, Muslim, Pakistani-born immigrant) social justice organizer with experience advocating around substance use stigma, harm reduction, and police abolition. Consequently, they interpreted deputations from the perspective that decriminalization is a positive step for the destigmatization of PWUID. It was important for them to engage in a regular practice of critical introspection, as well as discussion with the second author, to ensure that all deputations were analyzed to allow for a variety of potential meanings.
Despite the first author's familiarity with harm reduction activism, she does not have lived experience with using criminalized substances. Thus, her understanding of how such stigma is created and maintained, and how it affects PWUID is limited to academic study. Furthermore, as an able-bodied individual from a middle-class background living in Canada as a citizen, her perspective may prevent her from thinking about manifestations and impacts of stigma rooted in ableism, classism, and precarious migrant statuses that others may have centered in their deputations. To combat this, she familiarized herself with and consulted resources produced by PWUID on the issue of drug decriminalization throughout the analytic process, including those from these social perspectives.
The second author is a cisgender, heterosexual, White, male, able-bodied settler who also benefits from class privilege due to his family background and his current occupation as a university faculty member. He does not have lived experience of criminalized substance use or substance-use-related stigma. As a community-based researcher, he has worked closely with PWUID since 2018 on projects related to the meaningful inclusion of PWUID in research and advancing critical perspectives on interventions to address substance use–related stigma. Politically, he has worked alongside advocates for drug policy reforms (e.g., decriminalization, safer supply) and helped organize efforts to support the expansion of harm reduction services (e.g., supervised consumption, withdrawal management). His privileged identities and lack of lived experience with criminalized substance use necessitated self-reflexivity when interpreting how people discussed drug decriminalization in the deputations. This was enacted through regular meetings and analytical discussions with the first author and immersion in contemporary scholarship, journalism, and perspectives from PWUID on drug decriminalization.
Analysis
The 104 unique deputations submitted to the City of Vancouver provide insight into the conceptualizations of drug decriminalization among laypeople. Below, we present four main themes that highlight laypeople's perspectives on decriminalization: (1) drug decriminalization is assumed to reduce substance use stigma, but how is left unexplained; (2) from criminalization to medicalization: new forms of social control envisioned under drug decriminalization; (3) framing criminalization as necessary for the social control of PWUID; and (4) insufficiently included, but important: the anticarceral perspectives of PWUID.
Drug Decriminalization is Assumed to Reduce Substance Use Stigma, but How Is Left Unexplained
Supporters of the motion commonly argued that drug criminalization leads to the stigmatization of PWUID. How people discussed stigma implies their understanding of the relationship between stigma and public policy, if any. Furthermore, how people invoke stigma also implies the solutions they believe can address both the stigmatization of PWUID and the drug toxicity crisis. For example, a Registered Nurse Practitioner working in the Downtown Eastside of Vancouver argued in their letter, “We cannot make claims that we are anti-stigma when we are pro-criminalization of people who use drugs.” This argument equates the stigmatization of PWUID with the criminalization of drugs, a sentiment shared by most supporters of the motion. The argument suggests a direct link between criminalization and substance use stigma, positioning criminalization as at least a contributor to, if not a cause of, stigma. Assuming such a relationship, the implied solution to the stigmatization of PWUID necessitates decriminalization.
However, the mechanisms of change that would allow for decriminalization to destigmatize PWUID were commonly left vague and unexplained. Although people often cited criminalization as a stigmatizing force, they largely did not explain how criminalization creates this stigma, nor how drug policy reform may destigmatize PWUID.
It is perhaps unsurprising that stigma was commonly invoked in arguments and that its mechanisms were not explained when considered in the context of the deputations: people attempting to convince politicians to make a specific policy decision. The motion itself mentions destigmatization as a goal. Thus, the motion created a context in which those submitting deputations may have assumed a priori that decriminalization would address stigma. Furthermore, the mechanisms of destigmatization may not have been considered important to explain in this context. It is perhaps sufficient and more pertinent to simply state the desired goal of destigmatizing PWUID to make a compelling argument to City Council. However, this omission makes it unclear whether those submitting deputations have an idea of what those mechanisms might be. This potential lack of understanding of mechanisms of change presents a challenge, as public policy, including decriminalization, has the potential to both destigmatize and restigmatize PWUID (Hughes, 2017). Without an understanding of how criminalization contributes to stigma, models of decriminalization risk failing to destigmatize PWUID, serving only to reinforce current systems of oppression.
From Criminalization to Medicalization: New Forms of Social Control Envisioned Under Drug Decriminalization
A common refrain among supporters was that the drug toxicity crisis is a public health problem, not a criminal one. In their coauthored deputation, the Public Health Association of British Columbia and the CPHA wrote, “The alternative to criminalization is a public health approach.” However, just as there is no singular model of decriminalization, there is no singular public health approach. Some public health approaches, such as the one advocated for by many submitting deputations, prioritize the autonomy of PWUID (CPHA, 2024; Csete et al., 2016). These approaches focus on harm reduction, addressing the social determinants of health, and on providing PWUID with options other than criminalization to tackle issues arising from substance use.
Meanwhile, other public health approaches to decriminalization do not necessarily also advocate for the removal of police involvement entirely, nor for relinquishing state control over PWUID. Instead, such approaches focus on diverting PWUID to treatment, sometimes mandating treatment in order to avoid criminalization (Mosher & Yanagisako, 1991). We call this a carceral public health approach. A subset of deputations from supporters of decriminalization advocated for a carceral public health approach. For example, a clinical counselor in support of the motion argued that: It troubles me that there are still those who believe that if we punish those with addictions enough, they will somehow stop using. They misunderstand the very nature of addiction, which perpetuates repetitive behaviours despite devastating consequences… Just as our brains can't handle the exponential growth of unencumbered coronavirus, a brain in the grips of addiction is not always able to process and assign meaning to the consequences it has experienced, until it is too late… To see an elected official take meaningful action against one of the core systemic maladies helps to give meaning and direction to addiction treatment. It gives a glimpse of a better world wherein drug use and addiction are actually treated as public health issues…
Those advocating for a public health approach also often cited Portugal as a successful model to emulate. In one instance, a supporter of the motion argued, “Portugal's shift towards a more health-centred approach to drugs, as well as wider health and social policy changes, are equally, if not more, responsible for the positive changes observed.” However, as Woods (2011) noted, police “maintain a critical role in the decriminalized regime” in Portugal. Specifically, police confiscate substances and give citations to begin the process of administrative sanctions for those caught with substances. While these sanctions do not mandate treatment, people may be coerced into entering treatment, as doing so can suspend all sanctions (Woods, 2011). Thus, the Portugal model, in its use of police as an enforcement arm of public health policy, continues to be one that exerts control over PWUID. By using coercive measures to control people through treatment, the Portugal model supplements its prison system with a carceral version of the public health system. People who use illicit drugs in Portugal themselves have noted that the country's use of dissuasion committees “show[s] Portugal to be a far cry from a country that no longer polices or controls the lives of people who use drugs” (International Network of People Who Use Drugs, 2018). Those submitting deputations to the City of Vancouver citing the Portugal model as one to emulate, as six deputations did, were thus not arguing for an anticarceral response to the drug toxicity crisis, but rather for a carceral response recreated in a new image.
This carceral public health approach was echoed by three opponents of drug decriminalization who expressed some concern for the health of PWUID. For example, a Vancouver resident opposed to the motion argued, “Making drugs legal is NOT the right solution. Instead, you should be looking at rehabilitation centres that actually put a strict plan in place for the addicts, or build mental facilities for those truly with mental problems.” Similar to some proponents of decriminalization, this argument suggests a public health approach to the drug toxicity crisis. It does so in a manner that does not relinquish state control over PWUID, specifically by advocating for the medical system to put in place a “strict plan” to exert control over PWUID.
Framing Criminalization as Necessary for the Social Control of PWUID
While most deputations were in support of Motion B.4, nine (8.7%) deputations were in opposition. Similar to those advocating for a carceral public health approach, the arguments made by opponents of decriminalization demonstrated a perceived connection between drug criminalization and the social control of PWUID. Indeed, their arguments suggested that the ability to socially control PWUID was a welcome and comforting feature of criminalization that they feared losing. Part of these opponents’ concerns around decriminalization involved the potential for the loosening of state control over PWUID. For example, six of those opposed argued that decriminalization should not be pursued because it could lead to an increase in community harm, including health and physical safety. One individual asserted: Legalizing possession of non-prescription illegal drugs in Vancouver is not only irresponsible on the part of the mayor and council but will increase crime. If your [sic] going to decriminalize drugs then you need to decriminalize crime in general. You could save even more money by disbanding the [Vancouver Police Department] who would no longer be needed.
Notably, however, the safety of PWUID is not considered in these arguments. Instead, the perceived risks to the safety of the community, constructed as consisting of people who do not use drugs, are prioritized and weaponized against PWUID to justify their social control. This is especially the case when PWUID are positioned as the perpetrators of violence. For instance, one Vancouver resident shared, “I left my apartment yesterday to go to the store and witnessed 5 SEPERATE [sic] occurrences of active meth and what I'm guessing is heroin use… I'm certainly not going to be raising a family here as it stands.” The individual invokes a perceived harm to children by stating that they will not raise a family in Vancouver due to the public presence of PWUID. However, no specific harm was detailed. This implicitly positions witnessing substance use as harm toward children. Such an argument not only perpetuates the stigmatizing belief that PWUID are dangerous but also goes further to suggest that the visible existence of PWUID in public is in itself dangerous. The police and prison systems are thus once again justified as necessary to protect the broader community, namely children.
The rhetorical use of children in this argument is crucial, as children are a vulnerable class of people that do not have the relative power to protect themselves. Threats to children's safety, whether real or not, are thus effective rhetorical devices to shut down discussion about an issue (Marshall, 2005). If witnessing PWUID is assumed to be dangerous to children, the justification of removing PWUID from the public, such as through the prison system, becomes easier, regardless of the harm done to those individuals in the process.
A Paternalistic View of Social Control as Governmental Care for PWUID. Our analysis identified a subtheme whereby some deputations arguing for the social control of PWUID via criminalization did so by expressing a paternalistic form of care for PWUID. In the three cases where opponents of decriminalization expressed concern for the welfare of PWUID, they did not also advocate for the autonomy of PWUID. For example, an individual opposed to the motion asserted: [The decriminalization] movement is encouraging more people to do drugs, increase criminal activity, and mostly making a mess of the City. The City needs to get there priority [sic] straight. Instead, they need to look into making more mental health services, food set ups, and housing for these individuals available instead of drugs. As the City ever consider [sic] supplying drug addicts with clean medicated drugs instead of discriminalizing [sic] street junk. Decriminizating [sic] drugs might be an easy route for the City and politics but it's the worse things [sic] the City can do for the individuals. They need to actually care of [sic] the individuals.
Despite this concern for the welfare of PWUID, however, the individual quoted above also echoes stigmatizing beliefs that PWUID are perpetrators of community harm. They suggest that decriminalization would lead to an increase in substance use and crime. By juxtaposing their stigmatizing statements with an expressed desire to help PWUID, the writer implies that PWUID cannot help themselves and it is the moral imperative of the broader community to intervene. Such a view patronizes PWUID and removes their agency. Instead, criminalization is apparently viewed as a useful social norm that deters people from engaging in substance use in the absence of self-control. In line with a critical perspective on stigma and criminalization as a system of social control, opponents of decriminalization viewed criminalization as a dam holding back a flood of PWUID who would otherwise perpetrate unfettered community harm. This implies that the police and prison systems, as enforcers of criminalization, are benevolent protectors of not only the broader community but of PWUID themselves. State control of PWUID is thus argued to not be harmful but rather in the best interests of PWUID.
Insufficiently Included, but Important: The Anticarceral Perspectives of PWUID
Importantly, a small number of supporters advocated for the agency of PWUID in the policymaking process by asserting that developing an effective decriminalization policy requires including PWUID. For example, a letter from a public health researcher in Vancouver noted, “This change must be informed by and with people with lived experience of substance use or it is destined to continue to perpetuate harm.” This argument suggests that excluding PWUID from policymaking risks creating harmful decriminalization models, reaffirming and making explicit the concern that some decriminalization policies may be restigmatizing for PWUID (Hughes, 2017). The solution suggested to avoid reproducing harms for PWUID is simple: include PWUID in developing decriminalization policies.
Ironically, the voices of PWUID appeared to be largely missing within the deputations overall. There were only two unique deputations sent by people who self-identified as PWUID. The first was a form letter created by the CPDDW, submitted by 112 individuals, and the other was from someone who identified themself as a Vancouver resident. This failure to actively center the voices of PWUID is indicative of a larger issue in drug policymaking, namely that PWUID have historically been insufficiently included or excluded entirely from the policymaking process (Greer & Ritter, 2019). In Vancouver, for example, the decriminalization model put forth by then Mayor Kennedy Stewart after Motion B.4 passed was criticized by the Vancouver Area Network of Drug Users (VANDU) for failing to meaningfully include PWUID in consultations, despite a promise to do so (Larsen, 2021). Indeed, both unique deputations from PWUID explicitly argued that PWUID must be included in policymaking for decriminalization to effectively address the drug toxicity crisis and destigmatize them.
Notably, both unique deputations from PWUID also made anticarceral arguments, stating that the police must not be included in decriminalization models. Such anticarceral views were repeated by a minority of proponents. For example, four supporters of the motion recognized the shortcomings of the Portugal model specifically and advocated against it. For example, a public health researcher living in Vancouver said, “We know that punishing people financially and administratively does not work and actively causes harm. Forced entry into treatment also does not work… We must adopt key learnings from Portugal's experience around decriminalization.” This researcher explicitly argued against the punishment-oriented version of decriminalization implemented by Portugal. Others, while not citing Portugal directly, also recognized the harmful nature of carceral decriminalization models. One public health researcher and former harm reduction worker living in Vancouver explained: My colleagues and I have lost friends and loved ones to the overdose crisis. When I was younger, had someone told me that police don't arrest, but they might come harass you or take you off to treatment, [sic] it would not have removed the fear. For many of the people I've known, loved and lost, not having that fear would have made a difference. Repeal the CDSA and release and void charges for those imprisoned by it. Defund the police and reroute funding to [social welfare] programs.
Given the carceral nature of currently implemented decriminalization models, the CPDDW's demands position these models as being ineffective at their stated goals of destigmatizing PWUID and addressing the drug toxicity crisis. Once again, the assertion is that police are the major source of harm for PWUID and that they must be removed entirely for those harms to be addressed.
Discussion
This study examined how laypeople conceptualize substance use (de)criminalization and its implications for the (de)stigmatization of PWUID in the context of a motion to request a federal exemption to the CDSA for the City of Vancouver. Among supporters of the motion, decriminalization was commonly assumed to destigmatize PWUID. Likewise, criminalization was commonly linked to the stigmatization of PWUID. This echoes the perspectives of PWUID (Scher et al., 2023), whose voices were largely missing from the deputations. Another common refrain among supporters was that the drug toxicity crisis is a public health problem, not a criminal one, and thus our responses should utilize the healthcare system rather than the criminal punishment system. In some cases, calls to pivot responses to the healthcare system excluded the complete removal of police involvement. Proponents of the motion also argued that PWUID should be included in policymaking. Meanwhile, opponents of the motion commonly positioned criminalization as a necessary stopgap to avoid further community harm. This was true even among opponents who argued that decriminalization was a form of systemic neglect that abandons PWUID. These results raise wider questions about the importance of how laypeople understand the potential for drug liberalization policies to act as an intervention for the stigmatization of PWUID.
Potential Mechanisms of Change
Despite the common assertion within the deputations that decriminalization is a necessary step toward the destigmatization of PWUID, the mechanisms by which such policy-induced stigma change may occur were typically left unexplained. However, we can speculate what such mechanisms may be based on relevant research. Current literature examining the role that public policy reform may play in stigma reduction suggests that policy addresses stigma on a structural level, which then has the potential to influence individual behaviors, and thus social stigma, by reflecting and signaling a shift in cultural values (Cook et al., 2014). Thus, decriminalization has the potential to shift social norms around the perception of PWUID. For example, removing the association between substance use and crime may disrupt the public assumption that PWUID are dangerous to the broader community. This suggests that the specific model of decriminalization is crucial, as the model sets the new social norms. These new norms may reduce social stigma of PWUID, but it is equally possible that they may restigmatize PWUID, such as by inadvertently reinforcing negative associations with substance use (Hughes, 2017). Future research could improve our understanding of which decriminalization models are likely to be effectively destigmatizing and, importantly, how those policies may be most effectively crafted to comprehensively destigmatize PWUID.
Criminalization as State Control of PWUID
Even among proponents of the motion, some deputations echoed stigmatizing beliefs about PWUID. This was best exemplified by some of those who argued for a carceral public health approach to the drug toxicity crisis. Although many argued that the solution to the drug toxicity crisis lies in treatment, not punishment, not all then further argued for giving PWUID autonomy over their substance use. Instead, some supported the inclusion of police as an enforcement arm of public health, thus advocating for a treatment approach that maintained state control over PWUID. When considered in the context of Tyler and Slater's (2018) conceptualization of stigma as a system of social control, a decriminalization model that maintains state control over PWUID is not destigmatizing, but rather restigmatizing. Under this framework, destigmatizing PWUID, as a project of removing state control over PWUID, requires an anticarceral approach. Thus, it is possible that such carceral public health approaches to decriminalization, as some proponents advocated for, will fail to destigmatize PWUID structurally. In fact, the International Network of People Who Use Drugs (INPUD, 2021) has observed that most of the drug decriminalization models currently in place globally (e.g., Portugal, Czech Republic, and Germany), including those using public health approaches, continue to “rely on methods that, at their heart, are about social control” (p. 6) and thus, have “given rise to new or additional forms of stigma” (p. 36). Like in our data, INPUD observed that stigmatization based on criminalization is often simply shifted to stigmatization based on the pathologization of substance use.
Other proponents of the motion agreed with such anticarceral sentiments, citing the police as a nexus of harm for PWUID. These deputations support past literature problematizing the role of policing in the lives of PWUID in Vancouver. For example, Collins and colleagues (2019) found that the police presence in Vancouver's Downtown Eastside was a barrier to PWUID's access to overdose prevention sites. Similarly, barriers to engaging in harm reduction due to police presence were associated with greater odds of nonfatal overdose among women sex workers in Metro Vancouver (Goldenberg et al., 2020). Furthermore, current research suggests that the police act as a deterrent for accessing harm reduction services, thus perpetuating the drug toxicity crisis, while simultaneously eliciting behaviors deemed criminal. Earp and colleagues (2021) argue that drug criminalization pushes people to engage in ancillary criminal behaviors to access illegal substances, thereby creating a positive feedback loop of criminalization. In one study, Del Toro and colleagues (2019) found that contact with police was longitudinally associated with higher delinquency among Black and Latino boys. In line with labeling theory, which suggests that being labeled as a criminal increase one's likelihood of future criminal behavior (Bernburg, 2019), these findings suggest that contact with police itself, and not just drug criminalization, is criminogenic. Thus, eliminating contact with police and removing the label of “criminal” may be one crucial part of how decriminalization policies can destigmatize PWUID.
A Paternalistic View of PWUID
Among those opposed to the motion, criminalization was largely viewed as a dam preventing community harm from escalating. Social control and stigmatization were implied to be positive aspects of criminalization, as opponents often equated substance use with both crime and mental health issues. This argument relies heavily on an ableist viewpoint, whereby those with mental health issues are automatically deemed dangerous. Opponents of decriminalization implicitly argued that state control of PWUID is thus necessary for the safety of not only the broader community but also of PWUID themselves. This paternalistic view of PWUID strips them of their agency. Ironically, it also echoes the state control advocated for by some proponents of the motion. In some cases, proponents also expressed stigmatizing beliefs about PWUID, including the assertion that they are dangerous to the broader community. The disagreement between these proponents and those opposed to the motion thus lies not in whether PWUID should be controlled by the state, for they both agreed that they should, but rather how (i.e., in which system) the government should enact the social control of PWUID. Opponents argued that the police and prison systems should continue to hold this role, while some supporters asserted that the role should shift to the healthcare system. In either case, PWUID were viewed as unable to make sound decisions for themselves and thus, state intervention was deemed necessary.
Centering the Voices of PWUID
Importantly, the two unique deputations submitted by PWUID argued for anticarceral models of decriminalization. If we prioritize the voices of PWUID themselves in policymaking, as some proponents of the motion argued, it is important to consider that policing is often cited as a central issue. From the INPUD's (2021) perspective, born out of the lived and living experiences of PWUID, “models of decriminalisation that continue to use sanctions and other forms of punishment do not reduce stigma and discrimination against people who use drugs.” However, the voices of PWUID continue to be insufficiently included in policymaking (Greer & Ritter, 2019). Only two unique deputations were submitted by self-identified PWUID, though it is important to acknowledge that 112 PWUID submitted their own copy of the form letter drafted by the CPDDW.
Since Motion B.4 was passed in the City of Vancouver, the Government of B.C. has taken over the decriminalization initiative and successfully gained an exemption to the CDSA until January 2026 (Government of B.C., 2023). People who use illicit drugs, however, have criticized the province for failing to adequately consult them and for passing a decriminalization model that, among other complaints, relies on the police (Pivot Legal Society, 2021). People who use illicit drugs have consistently argued for decriminalization models that preserve their autonomy, and thus tackle stigma structurally. For example, in their “Manifesto for a Drug User Liberation Movement,” VANDU advocated for a decriminalization model that maintains their “right to obtain, prepare, and ingest drugs, and to be intoxicated on drugs… without criminalization or unsought interference from other individuals or organizations, as long as [their] drug use does not directly harm other people” (2010). This manifesto was a radical document for its time, centering the autonomy of PWUID in a conversation that largely excluded them. However, the language of this manifesto and the voices of PWUID have been co-opted and watered down in broader discussions surrounding decriminalization (Mullins, 2023). In recent years, the focus of policymakers concerned with substance use stigma has largely been in the realm of social stigma and changing individual people's attitudes. Consequently, the structural stigma considerations being emphasized by PWUID have been neglected. Overall, the public discourse surrounding the B.C. model of decriminalization boils down to one central sticking point: that of state control over PWUID. Ironically, despite a supposed commitment to the destigmatization of PWUID, the B.C. Model continues to assert social control over PWUID through both the police and healthcare systems, thus perpetuating structural stigma.
Limitations
Although the deputations that comprise the study sample provide a unique strength in that individuals were not influenced by demand effects of interviews, it is important to acknowledge the limitations of such a sample. The deputations were produced for a specific context and purpose, namely to convince the City of Vancouver to pass or reject a motion. Shaped by this context, the deputations may provide a limited window into laypeople's conceptualizations of decriminalization or its relation to stigma. Furthermore, not all people who may have an interest or stake in shaping decriminalization policy were able or willing to participate in the deputation process. Notably, only two unique deputations were sent by PWUID. As such, a diversity of perspectives from PWUID is missing from this analysis. Future research should build on research such as Scher and colleagues (2023) to intentionally examine the perspectives of PWUID on the relation between (de)criminalization and (de)stigmatization.
Conclusion
In deputations sent to Vancouver City Council regarding a motion on decriminalization, PWUID themselves and some proponents argued that meaningful destigmatization will require a decriminalization approach that addresses the structural stigma of the system of marking, control, and exclusion created by criminalization. This anticarceral approach contrasts with the arguments of opponents of the motion, who viewed state control of PWUID as a social benefit. This view was also echoed by some proponents, notably those who argued for a carceral public health model of decriminalization. Since the data for this study were produced in Fall 2020, B.C. has functionally reversed its decriminalization pilot program by disallowing drug possession in public spaces due to public backlash (BC Centre for Disease Control, 2024; CBC News, 2024). This reversal of a progressive attempt to decriminalize illicit substances follows the reversal of a similar pilot decriminalization in Oregon (Rush, 2024). Despite these changes, this study reminds us that laypeople have a variety of perspectives on decriminalization and its potential to destigmatize PWUID. In order to create decriminalization policies or any drug policies at all that have the greatest likelihood of meaningfully reducing both social and structural stigma toward PWUID, we need to better comprehend how laypeople understand these concepts. If policymakers want to address substance use stigma through decriminalization, our analysis highlights the importance of models that adequately address all levels of stigma for PWUID. Based on our findings, we argue this requires meaningfully involving PWUID in the policymaking process. From an anticarceral perspective, the autonomy of PWUID must be preserved in the implementation of decriminalization, and any model that fails to do so is likely to reproduce their stigmatization.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
Author Biographies
Dr.