
Abstract
The World Health Organization (WHO, 2021) estimated that globally, by 2030, one in six people will be aged 60 years or over, and by 2050, the number of persons aged 80 years or older is expected to triple and reach over 400 million. The same WHO report highlighted that by 2050, 80% of these persons will live in low- and middle-income countries. In response to this phenomenon of an ageing population, the United Nations General Assembly declared 2021–2030 the UN Decade of Healthy Ageing and supported global collaboration bringing together governments, international agencies, academia, the private sector and the media to foster longer and healthier lives (WHO, 2021).
At the same time, there has been a shift in the perspective of older age. Although for a long time it was considered an age of frailty and dependency, of decline and regression, in recent years this pessimistic outlook has been abandoned. Nowadays, older age is seen as a privilege that brings together gains on many levels and brings new opportunities. The perspective of going through the third stage of life in a reasonable state of health, which allows for commitments to family and sociocommunity activities, rather than conventional retirement, has already become a desirable norm. In this context, studying the factors that contribute to an increased quality of life becomes a necessity.
Health-related quality of life (HRQoL) has long been a concern of policy makers, researchers, and health practitioners (Bakas et al., 2012). According to previous findings, among older people social support increases HRQoL (Årestedt et al., 2013; Hofman et al., 2021). Although less studied, previous results have reported a positive relationship between PsyCap and HRQoL (Jurek & Niewiadomska, 2021; Santisi et al., 2020). Addressing this literature gap, the current study aimed to investigate the explanatory mechanisms by which perceived social support and PsyCap affect HRQoL among older adults.
According to the general definition proposed by the World Health Organization, quality of life refers to “an individual's perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns. It is a broad ranging concept affected in a complex way by the person's physical health, psychological state, personal beliefs, social relationships and their relationship to salient features of their environment” (WHO, 1996). HRQoL is a subordinate construct that assesses quality of life strictly from the perspective of the optimal functioning of an individual's health.
The theoretical model proposed by Wilson and Cleary (1995), later revised by Ferrans et al. (2005) conceptualized HRQoL by combining the biomedical and social science paradigms. Therefore, HRQoL has been conceptualized as a construct composed of eight health-related concepts: physical functioning; role limitations due to physical health problems; role limitations caused by emotional problems; energy/fatigue; emotional well-being; social functioning; pain; and general health perceptions (Hays et al., 1993; Ware & Sherbourne, 1992). Two sets of scores can be calculated, a synthetic profile including all health concepts, and two summary scores: a Physical Component Summary (PCS) and a Mental Component Summary (MCS).
Perceived Social Support and HRQoL
Social support refers to the care and help (both perceived and actually received) from others, relying on a sense of belonging to a social network (House, 1981). Structural measures of social support are quantitative evaluations concerning both the sources that provide support and the number of social interactions an individual initiates with others (Helgeson, 2003). Social support has been established as an indicator of membership in social groups, generating beneficial health effects (Årestedt et al., 2013). Considered as a form of social integration, social support represents a more stable construct over time, being easier to integrate into psychological intervention programs and public health policies (Brissette et al., 2000).
Previous studies provided consistent data indicating that social support increases HRQoL among older adults (Ethgen et al., 2004; Kyriazidou et al., 2022; Șahin et al., 2019; Shen et al., 2022). Results from a meta-analysis confirmed that the individuals who reported higher levels of social support showed better health status, better functioning in role-related activities, higher psychosocial adjustment, adaptive coping strategies, higher engagement in performing health-relevant behaviors, and higher levels of well-being, quality of life, and self-actualization (Wang et al., 2003).
Social support decreased susceptibility to certain physical and mental illnesses and was even associated with a lower mortality risk (Seeman, 2000). Results from a longitudinal study demonstrated that social support positively predicted HRQoL three years after receiving a breast cancer diagnosis (Leung et al., 2014). According to the same study, informational support provided by the life partner had the strongest positive effect on HRQoL over time. Similarly, other longitudinal studies have reported results confirming the positive relationship between social support and HRQoL among stroke patients (Teoh et al., 2009).
Social support is an essential factor for older people who depend on family, friends, or institutions to carry out daily activities or to access medical and social services. Addressing this aspect, the Centre for Disease Control and Prevention conducted the 2000 Missouri Older Adults Needs Assessment Survey on adults aged 60 years and above (CDC, 2005). According to the results, visits from friends and relatives, friendships as a source of emotional support, accessibility of medical services and specialized help for chronic illnesses or disabilities were associated with better HRQoL. Older adults with lower educational attainment and lower annual income reported greater vulnerability to HRQoL impairment.
Positive Psychological Capital (PsyCap) as Mediator
Positive psychological capital refers to a positive psychological condition that facilitates personal growth and development (Luthans et al., 2004). PsyCap relies on four pillars: self-efficacy, hope, optimism, and resilience. According to the conceptualization proposed by Luthans and collaborators (2007), psychological capital is a higher-order construct that implies a positive developmental state characterized by: having confidence to take on challenging tasks and put in the necessary effort to succeed (self-efficacy); making a positive attribution about succeeding now and in the future (optimism); persevering toward goals and, when necessary, redirecting paths in order to succeed (hope); when beset by problems and adversity, manifesting sustained effort and the ability to bounce back and start over (resilience). Relying on this conceptualization of PsyCap, practitioners have developed psychological interventions aiming to improve coping strategies and optimize individual functioning (Salanova & Ortega-Maldonado, 2019).
Results from previous studies provided consistent evidence indicating a positive relationship between social support and PsyCap (Gu et al., 2021; Liu et al., 2013; Lv et al., 2022). In addition, social support was a significant predictor for the four PsyCap resources (Jemini-Gashi et al., 2021; Sagi et al., 2021). PsyCap mediated both the relationship between social support and depression and between social support and anxiety (Liu et al., 2013). PsyCap also mediated the relationship between social support and treatment burden in a group of older patients diagnosed with chronic obstructive pulmonary disease (Gu et al., 2021). Other studies reported the mediating role of PsyCap in the relationship between social support and self-neglect among community-dwelling older adults (Zhao et al., 2022), between social support and loneliness (Luthans et al., 2007), and between social support and psychological well-being (Newman et al., 2018).
Originally developed within the research concerning the field of organizational psychology, PsyCap has been predominantly investigated along with domain-specific variables such as job performance (Alessandri et al., 2018; Avey et al., 2011) and quality of work life (Wardani & Anwar, 2019). Certainly, the protective role of PsyCap resources is not limited to the work domain. Previous studies have provided consistent evidence of positive associations between PsyCap and subjective well-being (Culbertson et al., 2010; Luthans et al., 2008). Furthermore, PsyCap was a significant predictor of well-being in the most important areas of life—health, work, and social relationships (Luthans et al., 2013). Data from a recent longitudinal study indicated that PsyCap had both a positive effect on life satisfaction and a negative effect on anxiety and depression, with stress acting as a mediator for these relationships (Turliuc & Candel, 2022).
Among retirees, the protective role of the PsyCap resources was directed toward maintaining health and optimizing individual functioning. To our knowledge, only a few studies addressed the relationship between PsyCap and HRQoL in this population segment, reporting a positive relationship. Consequently, higher levels of PsyCap contributed to an increase in HRQoL (Ahmadboukani et al., 2023; Jurek & Niewiadomska, 2021).
The Current Study
Based on the theoretical model of HRQoL (Ferrans et al., 2005; Wilson & Cleary, 1995), and drawing on the empirical evidence summarized in the previous sections, we aimed to investigate the role of some explanatory variables in the relationship between social support and HRQoL among older adults. Firstly, we hypothesized that perceived social support positively predicts both physical health (H1.1) and mental health (H2.1). Further, we anticipated that compound PsyCap mediates both the relationship between perceived social support and physical health (H1.2) and between perceived social support and mental health (H2.2). Finally, we hypothesized that the four PsyCap resources—hope, optimism, resilience, and self-efficacy—act as parallel mediators of the relationships between perceived social support and the two components of HRQoL (H3.1 and H3.2).
Method
Participants
The sample consisted of 319 participants (114 men and 205 women) aged 65–90 years (Mage = 71.1, SD = 4.8). The selection criterion regarding the minimum age of the participants was based on the official retirement age limit. In most Western countries, the third age begins with the age of 65 and corresponds approximately to the period of retirement from work. According to the legislation in force in Romania, the standard retirement age for men is 65, while women can retire after 61 years and 6 months. Some professions do not impose different retirement age limits for men and women. Therefore, we collected data only for participants aged 65 and above. In our sample, 58.4% of the participants were married, 4.5% were divorced, 3.2% were cohabiting with their significant other, and 33.9% were widowed. In terms of the last level of education completed, 10.1% of the participants had only completed primary education, 24.1% secondary education, 46.1% high school or vocational education, 16.9% graduated from university, and 2.8% completed postgraduate education.
Monthly income was used as an indicator of socioeconomic status. Participants were asked to indicate the value of their monthly income, choosing between: (a) < 1500 RON, (b) between 1500–3000 RON, and (c) > 3000 RON. The previous income categories were created based on the average pension amount in Romania, which at the time of the survey was 1778 RON (∼350 Euro; National Institute of Statistics (NIS, 2023)). The minimum pension at the time was 1000 RON (∼200 Euro). The results indicated that 54.5% of the participants reported receiving an average income, 33.5% had a monthly income of less than 1500 RON (∼300 Euro), that is, below the minimum national income, and 11.9% reported a monthly income above 3000 Lei (∼600 Euro).
Measures
Perceived Social Support. The Multidimensional Perceived Social Support Scale (MSPSS; Zimet et al., 1988) contains 12 items that assess support received from (1) a significant other, (2) family, and (3) friends. Participants rated each item on a 7-point Likert scale ranging from 1 (totally disagree) to 7 (totally agree). A sample item was: “I feel like I can share the problems I face with my family.” The instrument had no indirect items. The total scores were first computed as an average per subscale, and then as an overall total score, calculated as the average of all the items. Higher scores indicated an increased level of perceived social support. Previous research reported excellent psychometric properties for the MSPSS scale (Bruwer et al., 2008). In the current study, Cronbach's alpha coefficient was .93 for the significant other's support subscale, .93 for family support, .96 for friend support, and .93 for overall social support.
PsyCap. The Compound PsyCap Scale (CPC-12, Lorenz et al., 2016) includes 12 items assessing the four positive psychological capital resources. The items were evaluated on a 6-point Likert scale, from 1 (totally disagree) to 6 (totally agree). A sample item was: “I am confident that I could successfully cope with unexpected events.” The instrument had no indirect items. We used both the total composite score and the four total subscale scores. The psychometric properties of the Compound PsyCap Scale were well-established (Lorenz et al., 2022). In the current sample the Cronbach alpha coefficient for compound PsyCap was .93, while for the subscales, it was .81 for hope, .89 for optimism, .80 for resilience, and .88 for self-efficacy, indicating adequate levels for the items’ internal consistency.
HRQoL. We used 36-Item Short Form Survey (SF-36; Medical Outcome Survey). The SF-36 is a generic instrument that assesses HRQoL, but also represents a general indicator of health status. The instrument was widely used in research and clinical practice, individually or in conjunction with other surveys specifically adapted to the study of certain health conditions (Ojelabi et al., 2017). An example of an item is “During the past 4 weeks, how much did pain interfere with your normal work (including both work outside the home and housework)?.” The Short-Form Health Survey (SF-36) contains a 36-item scale measuring eight health-related concepts: (1) physical functioning; (2) role limitations due to physical health problems; (3) role limitations caused by emotional problems; (4) energy/fatigue; (5) emotional well-being; (6) social functioning; (7) pain; and (8) general health. Cronbach's alpha coefficient indicated adequate levels of internal consistency for the eight subscales as follows: .91 (1), .86 (2), .80 (3), .79 (4), .80 (5), .69 (6), .83 (7), and .79 for (8). The Cronbach's alpha coefficient for the overall score was .94. To compute the values for PCS and MCS, we first standardized each of the eight scales by calculating z-scores. Next, the z-scores were multiplied by the factor weights for PCS and MCS, and the scores on all eight subscales were summed. Finally, these values were converted to t-scores by multiplying the results for PCS and MCS by 10 and adding 50. Scores for each dimension range from 0 to 100, with higher scores indicating better health.
Procedure
The study procedure and instruments were in full compliance with the Declaration of Helsinki and the University's Code of Ethics. The studýs protocol has been approved by the Universitýs Ethics Committee (registration form n°188). The participants received information regarding the purpose of the study, being stated that their responses were anonymous and strictly confidential and would only be used for the purpose stated in the current research. The participants gave their informed consent to participate. The instruments were applied online, on a platform that facilitated data collection. The time required for the application was approximately 25 min.
Analytic Strategy
As preliminary statistical analyses, we computed means, standard deviations and Pearson correlations between the study variables, using the SPSS 26 software. Following the study hypotheses, we proposed two simple and two parallel mediation models using Model 4 from PROCESS macro version 4.2 of the IBM SPSS tool. Five thousand bootstrap samples were adopted by building bootstrap-based confidence intervals in order to estimate 95% confidence intervals (Hayes, 2018). The effects are considered statistically significant only when confidence intervals exclude zero (Hayes & Scharkow, 2013).
Simple mediation analysis was used to test the mediating effect of compound PsyCap both in the relationship between perceived social support and physical health (Model 1) and between perceived social support and mental health (Model 2). Subsequently, we analyzed whether the four PsyCap resources act as parallel mediators in the relationship between perceived social support and both the physical (Model 3) and mental components of HRQoL (Model 4), controlling for age as a covariate.
Results
Descriptive Statistics and Correlational Analyses
All measured variables were normally distributed. Table 1 presents the means, standard deviations, and Pearson correlation coefficients. The results indicated significant positive associations both between perceived social support and PsyCap (r = .47; p < .001), and between social support and the two components of HRQoL—physical health (r = .22; p < .001) and mental health (r = .29; p < .001). Compound PsyCap positively correlated with physical health (r = .41; p < .001) and mental health (r = .60; p < .001). Moreover, PsyCap resources were also positively correlated both with the eight HRQoL components and the two summary scores (PCS and MCS). Thus, high levels of hope, optimism, resilience, and self-efficacy were associated with better physical and mental health.
Means, Standard Deviations, and Correlations Among the Study's Variables.
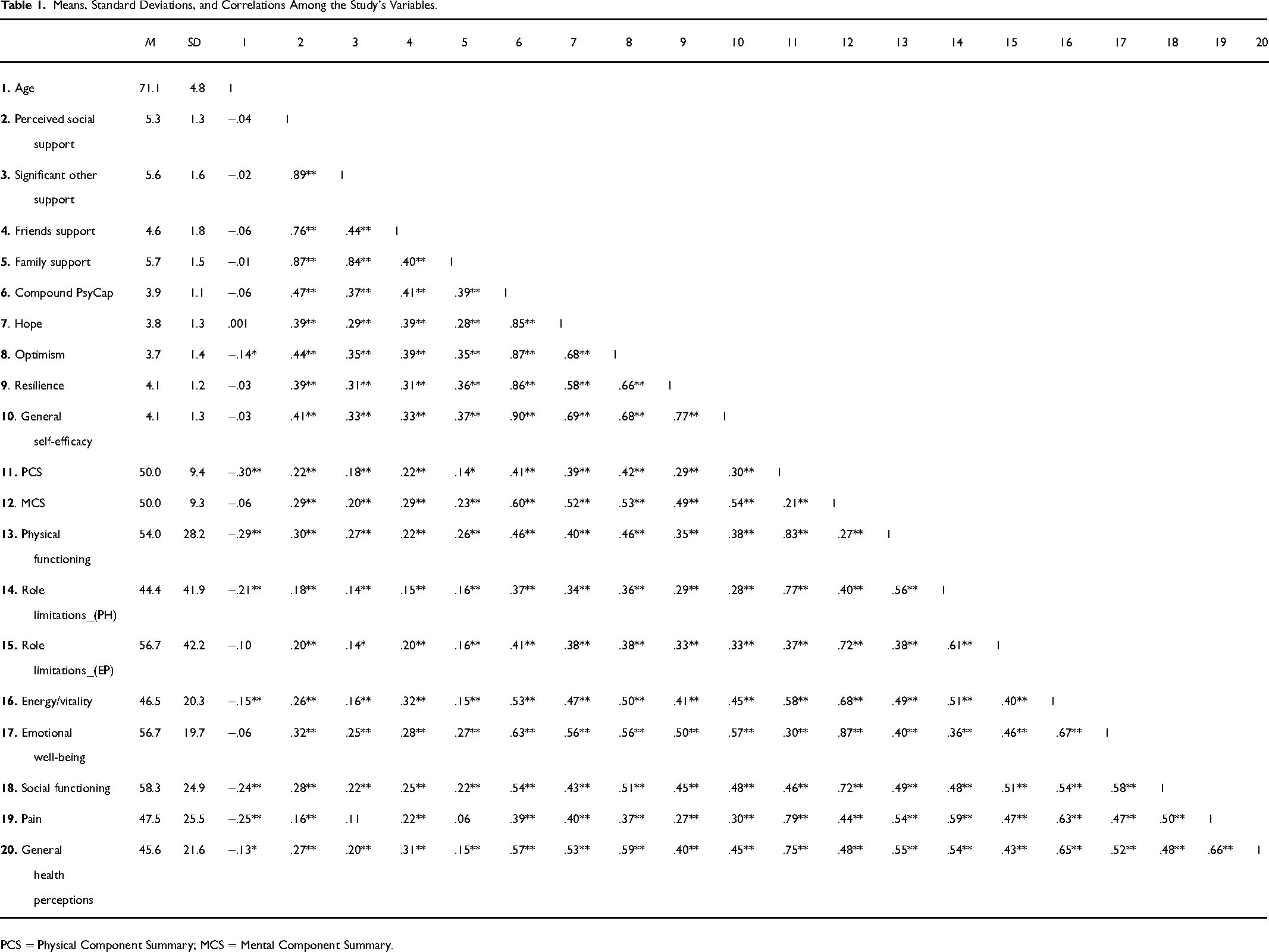
PCS = Physical Component Summary; MCS = Mental Component Summary.
It was observed that pain was not significantly correlated with significant other support (r = .11; p = .061 > .050), nor with family support (r = .06; p = .258 > .050). Older participants reported lower levels of optimism (r = −.14; p = .011 < .050), lower physical functioning (r = −.29; p < .001), more limitations due to physical health (r = −.21; p < .001), lower levels of energy (r = −.15; p < .001) and social functioning (r = −.24; p < .001), increased pain (r = −.25; p < .001) and poorer general health (r = .13; p = .020 < .050). Moreover, older participants showed lower scores on the physical health component (r = −.30; p < .001). The complete results of the correlational analyses are summarized in Table 1.
Additionally, we analyzed gender differences for each of the investigated variables. The results of independent sample t-tests indicated that the only significant difference was obtained for hope as a PsyCap resource. Men scored significantly higher on hope compared to women (t(317) = 2.227; p = .027; d = 0.26).
We conducted several one-way ANOVAs to compare differences between participants with low, medium and high socioeconomic status. One-way ANOVA results indicated that participants with low socioeconomic status reported less friends support, lower levels of PsyCap, hope, optimism, and poorer general health compared to those with medium and high socioeconomic status. Eta squared (η²) indicated small size effects. The complete results are summarized in Table 2.
One-Way ANOVA Results Regarding the Socioeconomic status (SES).
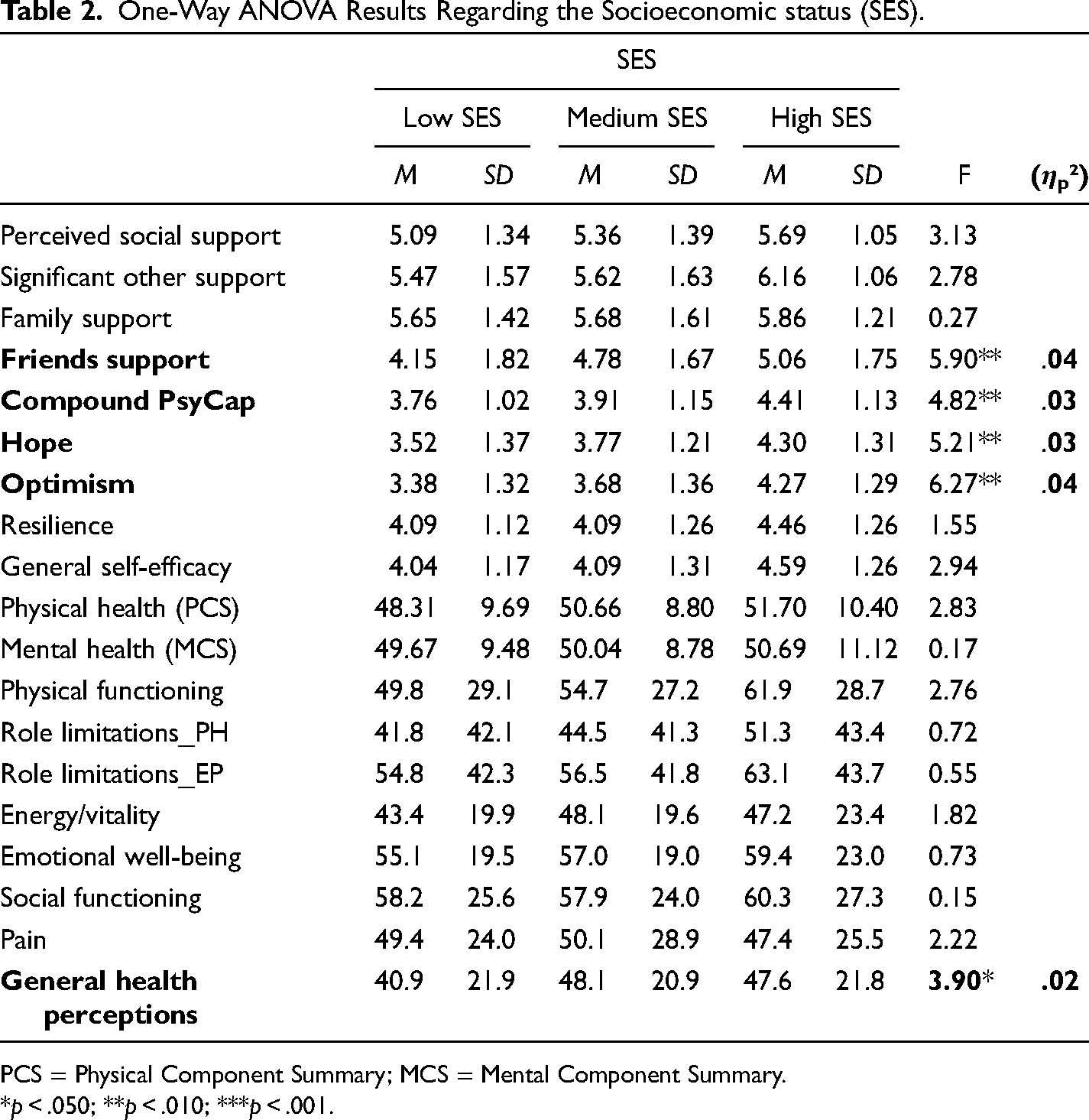
PCS = Physical Component Summary; MCS = Mental Component Summary.
*p < .050; **p < .010; ***p < .001.
Furthermore, the study compared the differences between the participants’ mean scores on several psychological variables, according to the last completed level of education. We aimed to identify if there were significant differences between the participants with primary education, lower-secondary education, high school studies/secondary school system, higher education/university education and postuniversity education. In order to analyze the differences between participants’ completed levels of education, we conducted several one-way ANOVAs (Table 3).
One-Way ANOVA Results Highlighting the Differences in Terms of the Level of Education.
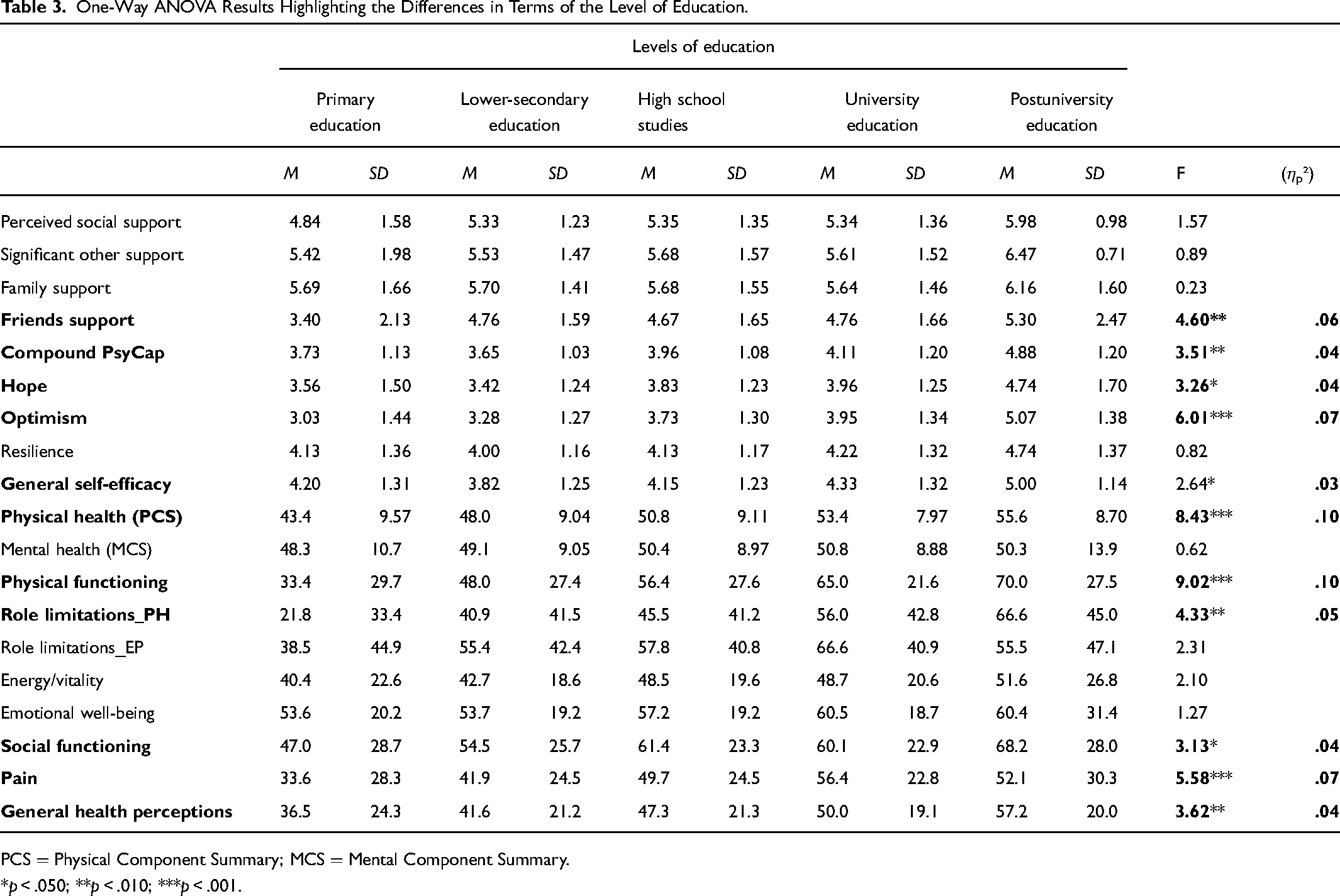
PCS = Physical Component Summary; MCS = Mental Component Summary.
*p < .050; **p < .010; ***p < .001.
The significant effects of one-way ANOVAs were highlighted in the table below. The results indicated that compared to those with higher education, participants who only completed primary education obtained lower scores for friends’ support, PsyCap, hope, optimism, self-efficacy, lower levels of physical and social functioning, more limitations due to physical health issues, more pain, poorer general health and lower scores on the physical health component. Eta squared (η²) indicated medium size effects.
Simple Mediation Models
For the first model, the statistical results indicated that social support positively predicted PsyCap (β = .47; p < .001) which in turn positively predicted physical health (β = .37; p < .001; Figure 1). Age was a significant covariate for physical health (β = −.27; p < .001). The total effect was statistically significant (C = .208; p < .001; 95% CI [0.7296, 2.1623]). Including PsyCap as a mediator results in the direct effect of social support on physical health becoming nonsignificant (c'=.035; p = .527 > .050). The indirect effect was statistically significant (a*b = .173; [0.1135, 0.2460]), thus PsyCap fully mediated the relationship between perceived social support and the physical health component. Hypotheses H1.1 and H1.2 were confirmed (Figure 2).
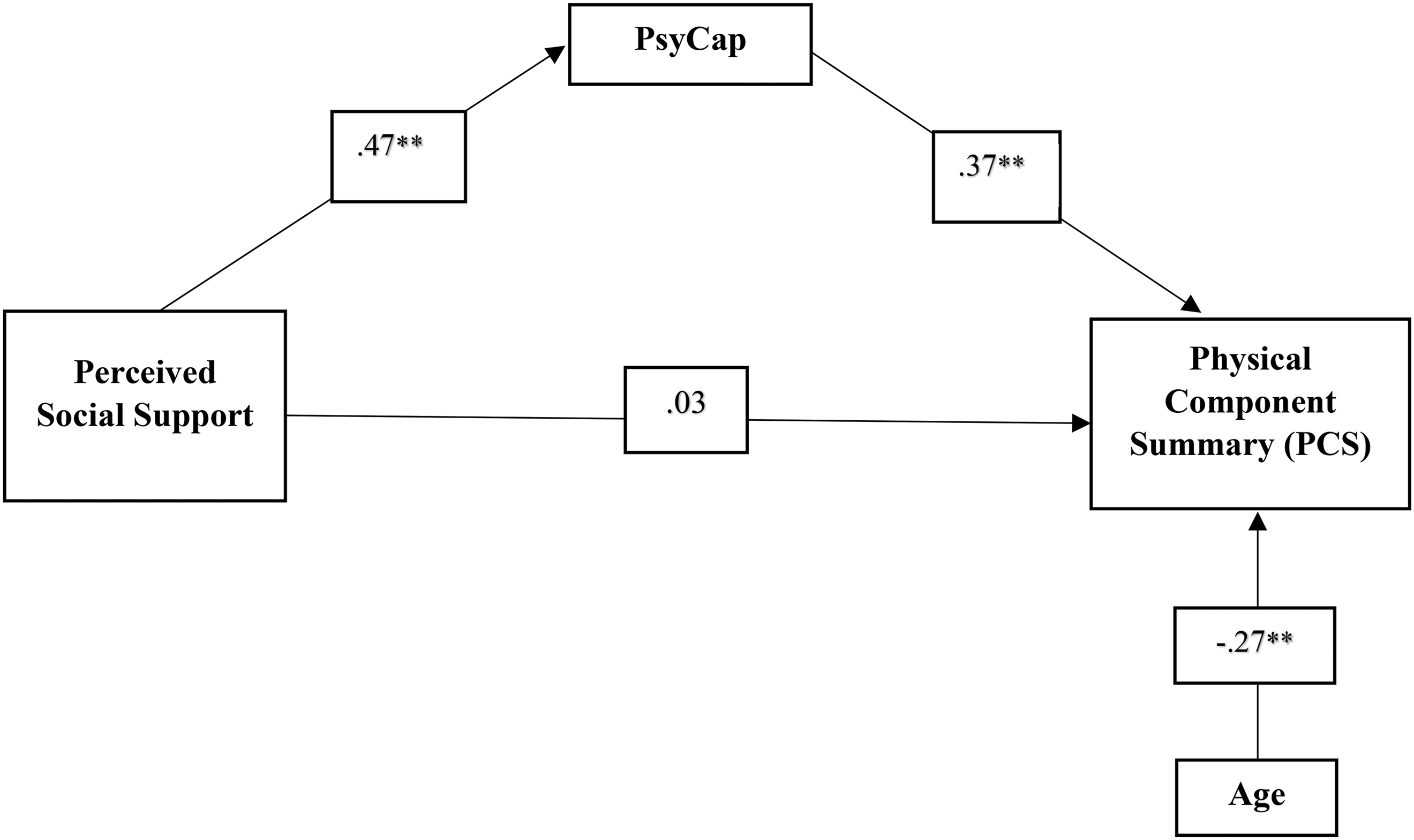
First simple mediation model. Path coefficients are standardized estimates. *p < .050; **p < .010.
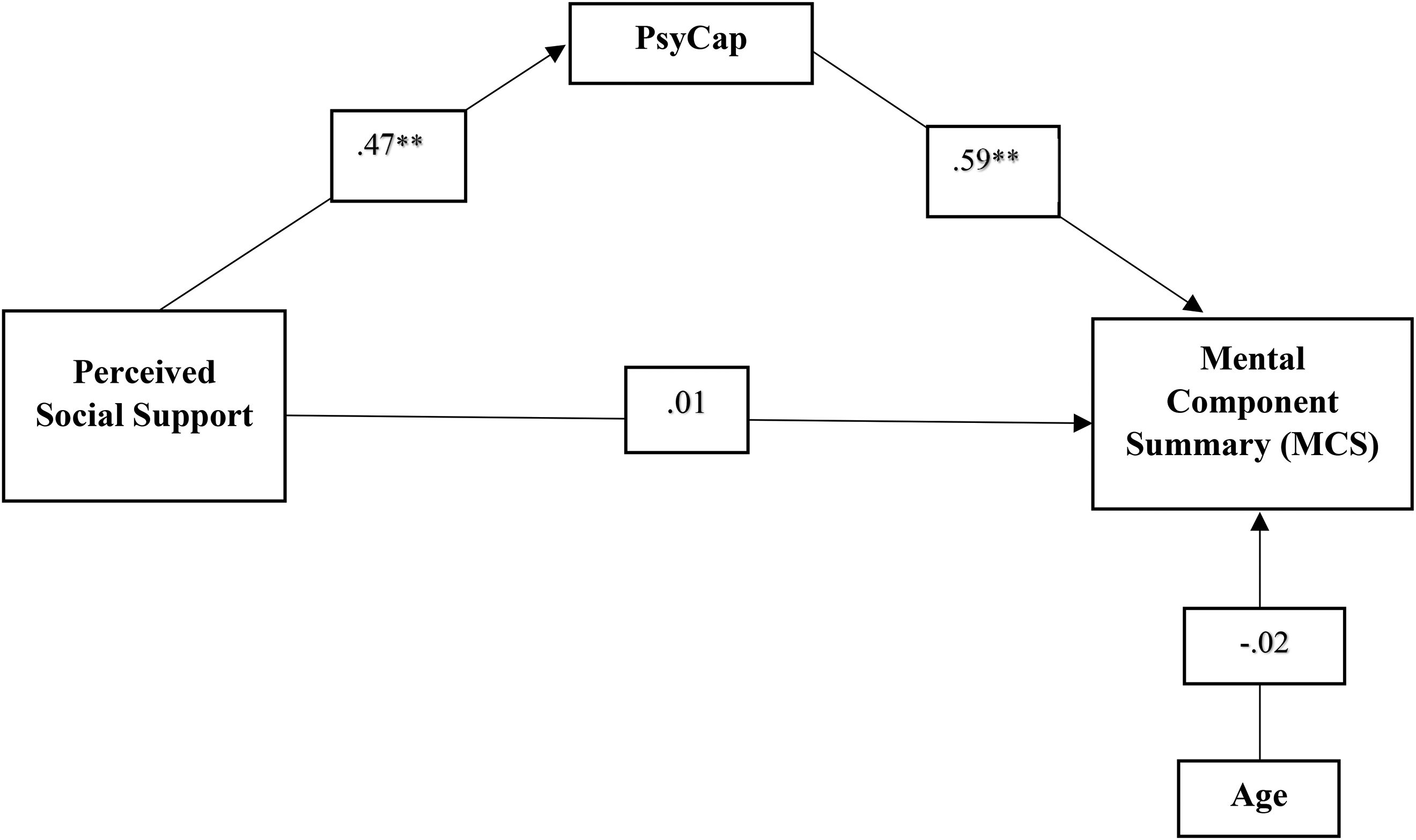
Second simple mediation model. Path coefficients are standardized estimates. *p < .050; **p < .010.
For the second model, the results of the mediation analysis showed that social support positively predicted PsyCap (β=.47; p < .001) which in turn positively predicted mental health (β = .59; p < .001). Participants’ age was not a significant covariate for mental health (β = −.02; p = .627 > .050). The total effect was statistically significant (C = .285; p < .001; 95% CI [1.2334, 2.6939]). Similar to the first model, after including PsyCap as a mediator, the direct effect of social support on mental health became nonsignificant (c'=.009; p = .858 > .050), while the indirect effect was statistically significant (a*b = .275; [0.2091, 0.3446]). Therefore, PsyCap fully mediated the relationship between perceived social support and the mental health component. Hypotheses H2.1 and H2.2 were sustained.
A Monte Carlo Power Analysis for Indirect Effects (Schoemann et al., 2020) was used to estimate statistical power. According to the results, for both models, a statistical power of 1.00 (p < .050) was reached in a sample of 319 participants. Subsequently, the statistical power of both models surpassed the .80 probability, which complied with the criteria required to adequately reject a false null hypothesis.
Parallel Mediation Models
We tested two mediation models with the four PsyCap resources as parallel mediators in the relationship between perceived social support and the two components of HRQoL, controlling for participants’ age (Figure 3).
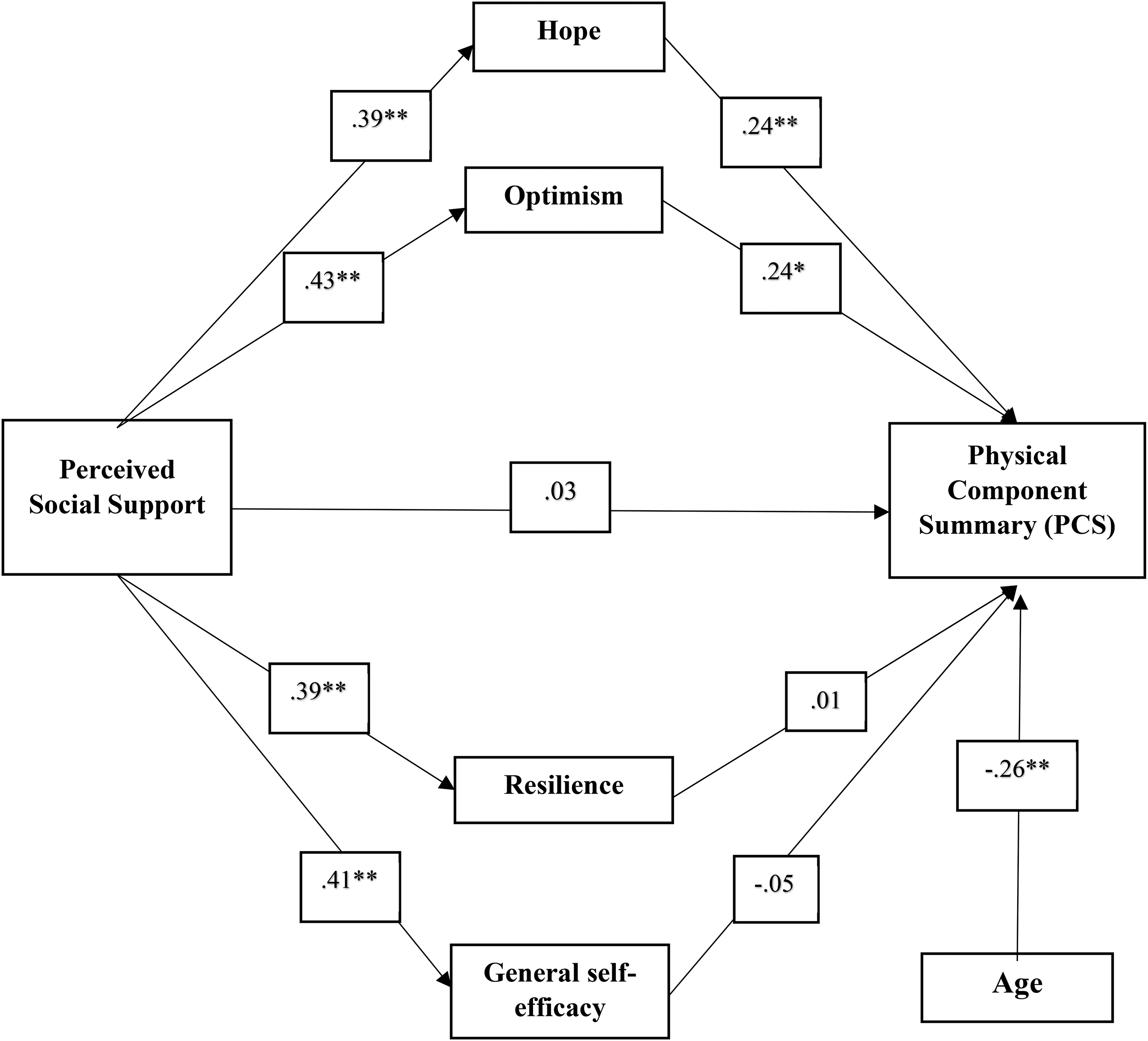
First parallel mediation model. Path coefficients are standardized estimates. *p < .050; **p < .010.
According to the statistical results, social support positively predicted hope (β = .39; p < .001), optimism (β=.43; p < .001), resilience (β=.39; p < .001), and self-efficacy (β=.41; p < .001). However, out of the four mediators, only hope (β=.24; p = .001 < .050) and optimism (β=.24; p = .002 < .050) positively predicted physical health. Participants’ age was a significant covariate only for physical health (β = −.26; p < .001). The total effect was statistically significant (C = .208; p < .001; 95% CI [0.7296, 2.1623]).
We noted that the direct effect was not statistically significant (c'=.030; p = .584 > .050). The first (a1*b1 = .093; 95% CI [0.0358, 0.1618]) and the second (a2*b2 = .102; [0.0309, 0.1791]) indirect effects were significant, while the third (a3*b3 = .005; [−0.0598, 0.0740]) and the fourth (a4*b4= −.023; [−0.0917, 0.0553]) indirect effect were nonsignificant.
By testing the total indirect effect (β = .178; 95% CI [0.1185, 0.2494], we observe that it was statistically significant. Only hope and optimism were parallel mediators of the relationship between perceived social support and physical health. Therefore, hypothesis H3.1 was partially supported (Figure 4).
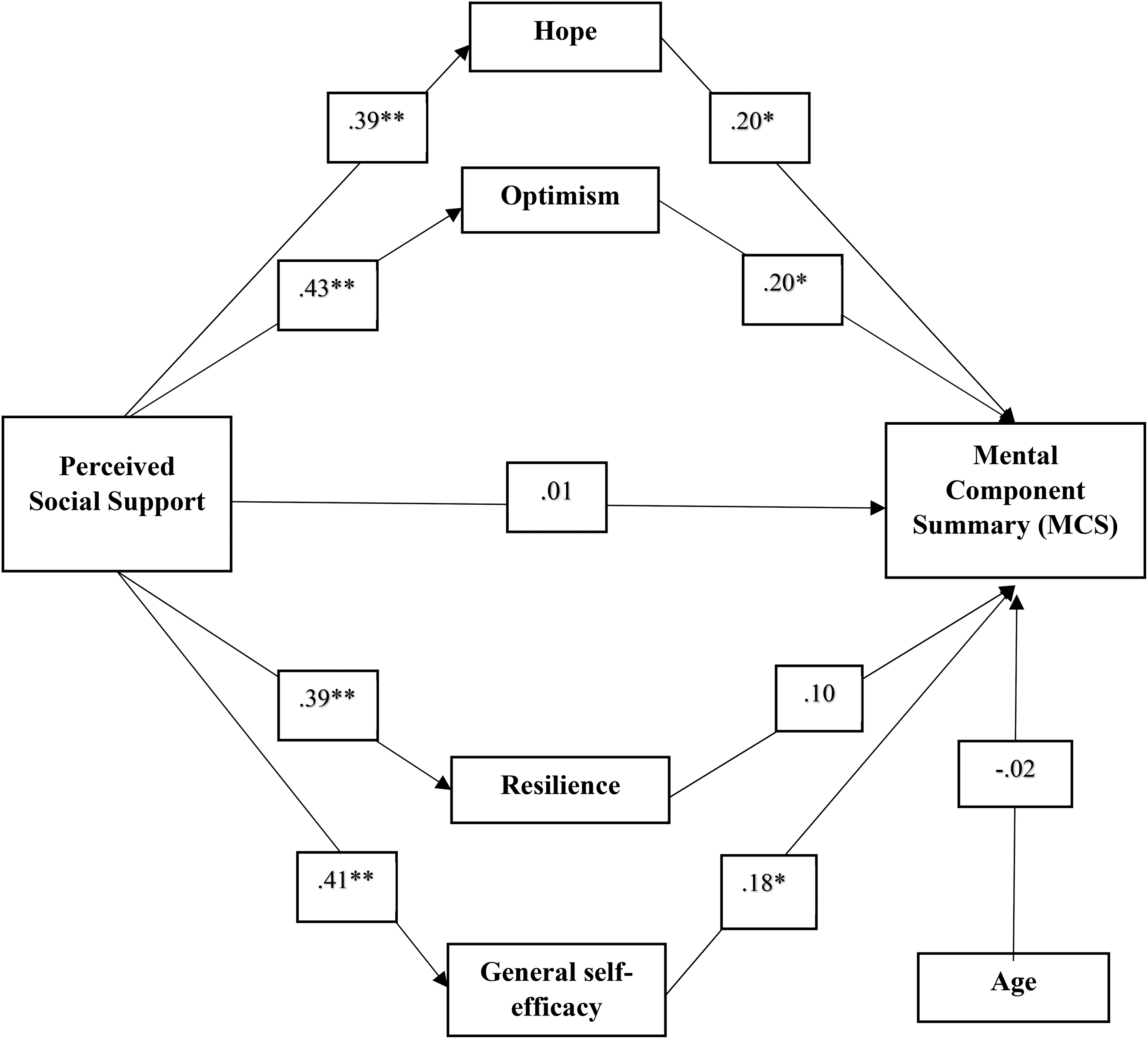
Second parallel mediation model. Path coefficients are standardized estimates. *p < .050; **p < .010.
For the second parallel mediation model, the results showed that social support positively predicted hope (β=.39; p < .001), optimism (β=.43; p < .001), resilience (β=.39; p < .001), and self-efficacy (β=.41; p < .001). Still, only hope (β=.20; p = .004 < .050), optimism (β=.20; p = .006 < .050), and self-efficacy (β=.18; p = .023 < .050) positively predicted mental health. The total effect was statistically significant (C = .285; p < .001; 95% CI [1.2334, 2.6939]).
The direct effect was statistically nonsignificant (c'=.008; p = .874 > .050). Nevertheless, the first (a1*b1 = .076; 95% CI [0.0156, 0.1416]), the second (a2*b2 = .085; [0.0134, 0.1622]) and the fourth (a4*b4= .076; [0.0075, 0.1475]) indirect effect were statistically significant, while the third indirect effect (a3*b3 = .040; [−0.0276, 0.1126]) was nonsignificant. By testing the significance of the total indirect effect (β=.277; [0.2076, 0.3455]), we observed that hope, optimism, and self-efficacy were parallel mediators of the relationship between perceived social support and mental health. Thus, the H3.2 hypothesis was partially confirmed.
A Monte Carlo Power Analysis for Indirect Effects was used to estimate statistical power (Schoemann et al., 2020). According to the results, for the first parallel mediation model a statistical power of .95 (p < .050) was reached both for a1*b1 and a2*b2 indirect effect. For the last model, a statistical power of 1.00 (p < .050) was obtained for the indirect effects of a1*b1, a2*b2, and a3*b3 on a sample of 319 participants. Therefore, to reject a false null hypothesis, required sample sizes were computed and statistical power exceeded the .80 probability.
Discussion
The current study aimed to investigate the relationship between social support and HRQoL among older adults, as well as testing some of the psychological mechanisms that explain this relationship. Therefore, we analyzed the mediating role of positive psychological capital—both as compound PsyCap and as individual resources—in the relationship between perceived social support and the two components of HRQoL (PCS and MCS).
Although the statistical analysis indicated positive significant relationships between social support and the two components, it also showed that mental health was better explained by social support compared to physical health. The same observation applies when analyzing the preliminary correlations between the components of social support and PCS and MCS. The support of an individual's significant other, as well as friends and family's support were better correlated to mental health rather than physical health. The literature provided consistent evidence to highlight the benefits of a supportive climate in order to increase HRQoL (Årestedt et al., 2013; Ethgen et al., 2004; Hofman et al., 2021; Kyriazidou et al., 2022; Şahin et al., 2019; Shen et al., 2022). From this perspective, our results align with previous findings.
The current study showed that compound PsyCap fully mediated the relationship between social support and physical/mental health. Moreover, hope and optimism were parallel mediators in the relationship between social support and physical health, while the same PsyCap resources, along with general self-efficacy, also mediated the relationship between social support and mental health. Social support was, consequently, a significant positive predictor both for compound PsyCap and its four resources. More social support—either from family, friends, or a significant other—generated a higher level of PsyCap. These results are in agreement with previous research (Gu et al., 2021; Jemini-Gashi et al., 2021; Liu et al., 2013; Lv et al., 2022).
Retirees that could rely on their social network presented higher levels of individual PsyCap resources. According to Gu et al. (2021), social support contributed to an increase in PsyCap by converting external interpersonal resources into an aggregate construct defined as a global intrapersonal resource. Another argument sustaining this perspective refers to PsyCap as a state-like variable that is prone to change (Luthans et al., 2008). It can definitely be stated that a supportive climate contributes to the creation of a favorable life context, which in turn promotes an increase in PsyCap.
Furthermore, perceived social support led to an increase in compound PsyCap, which in turn was associated with higher levels of physical and mental health. In other words, those who received greater support, help and care were more hopeful, more optimistic, more resilient and self-efficient, while also presenting better HRQoL. Higher levels for the physical and mental health components indicated a better physical functioning, less role limitation due to physical health/emotional problems, decreased bodily pain, higher levels of energy and emotional well-being, higher social functioning and better general health.
The current study's statistical results also identified positive significant relationships between compound PsyCap and both physical and mental health. Hope and optimism positively predicted physical health, while the same PsyCap resources, along with general self-efficacy positively predicted mental health. PsyCap resources had a higher impact on mental health (Turliuc & Candel, 2022) compared to physical health. Thus, the relationship between social support and physical health was explained by hope and optimism, while the same mediators, together with general self-efficacy, explained the relationship between social support and mental health.
Contrary to our expectations, resilience did not significantly predict either physical health or mental health. This result was not entirely surprising, even though it did not align with previous literature. Mixed results have been reported in previous research regarding the relationship between resilience and health. For example, resilience positively predicted life satisfaction (Rossi et al., 2007) while negatively predicted mental health negative outcomes such as depression, anxiety, and apathy (Laird et al., 2019). On the other hand, another study's results indicated that resilience acted as a buffer in the relationship between perceived stress and the physical component of HRQoL (and not for the mental health component; Serrano et al., 2023). It must be considered that physical health, as proposed by the theoretical model of HRQoL, measures an individual's physical functioning. Some of the previous studies reported no associations between resilience and physical functioning (Battalio et al., 2017; Silverman et al., 2015). Therefore, resilience was more important for certain social constructs which allow for a greater self-report subjectivity than physical health. Accordingly, the results of a study showed that in the case of retirees suffering from neurological disease, other variables such as depression had a higher impact on health compared to resilience (Schönenberg et al., 2022; Terrill et al., 2016).
The Conservation of Resources theory (Hobfoll & Shirom, 1993) provides a theoretical background for a better understanding of the practical implications of the current findings. According to this theory, resources do not occur separately; on the contrary, resources develop as constructs formed by interdependent components that foster one another, contributing to the development of resource passageways. To this end, caravan passageways consist of certain environmental peculiarities that favor, support, develop, and protect an individual's resources or, on the contrary, act as detractors which undermine one's resource reservoirs (Chen et al., 2015).
The participants’ age was a significant covariate only for physical health (not for mental health). The older the participants were, the lower levels of physical health they reported. This result was in accordance with the expectations, since ageing gradually decreases an individual's physical capacities, generating specific health issues, commonly referred to as geriatric syndromes. Data from a longitudinal study analyzing the responses of 7,195 older adults indicated that cumulative adverse life events accelerated physical health deterioration (Levinsky & Schiff, 2021).
The current study was based on one of the most commonly used HRQoL theoretical models, Wilson and Cleary's model, revised by Ferrans et al. (2005). Previous evidence-based studies confirmed the explanatory mechanisms between the model's base constructs (Sousa & Kwok, 2006). The investigated variables concerned both physical and mental health as components of HRQoL in older adults, which constitute a less studied population sample due to difficult access. The novelty resides in the use of positive psychological capital (a concept traditionally pertaining to the field of organizational psychology) in a different research direction, one that promotes the principles of active, healthy ageing. Summarizing, the results of this study demonstrated that social support leads to an increase in positive psychological capital, which, in turn, contributes to the optimization of the physical and mental components of HRQoL. This alternative explanatory path suggested that the effect of social support could be explained by its role in facilitating social interactions, as well as increasing the availability of external and internal personal resources. Regarding the practical implications of the results, HRQoL intervention programs designed for older adults should consider two main aspects. The first one should consist of implementing efficient strategies that facilitate the social integration, in order to ensure adequate access to qualitative social support, while the second should entail the participation of retirees in psychotherapeutic programs focused on enhancing positive psychological capital. Being defined as a state-like variable, PsyCap is open to change, each component having the potential to be developed through practical intervention (Luthans et al., 2008; Turliuc & Candel, 2022).
Limitations and Future Research Direction
Beyond the strengths of this present study, it also presents some inherent limitations. Firstly, this study used cross-sectional data, which limits the understanding of the psychological processes on an individual level. Secondly, the results were obtained from a convenience sample of older adults, unequal in terms of participants’ gender and without any specific constraints regarding relevant health-related parameters. Thus, our results cannot be extrapolated to the general population of retirees. The results must be specifically interpreted within the context of the investigated sample. Larger studies that include participants pertaining to different population subsets could indicate the degree to which our results could be generalized. For future research, longitudinal designs are recommended, along with the use of experimental manipulation in order to allow a more accurate identification of causal mechanisms between the investigated variables.
Conclusion
To conclude, the current study proposed a series of new perspectives regarding the relevant factors that promote an increase of HRQoL in the third age. The results were not limited to simply identifying the relationships between variables, but relied on investigating the underlying explanatory mechanisms. Our findings indicated significant positive associations between perceived social support, PsyCap, physical health and mental health. Compound PsyCap fully mediated the relationship between perceived social support and physical/mental health. When looking separately to PsyCap resources, hope and optimism positively predicted physical health, while hope, optimism, and self-efficacy positively predicted mental health. Thus, the mediating effect of PsyCap confirms that it constitutes an alternative path for the explanation of the relationship between perceived social support and HRQoL.
Footnotes
Author's Contributions
All authors have contributed equally to the data acquisition, analysis, manuscript drafting, interpretation of the results, and critical revision. All authors read and approved the final manuscript.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.