
Abstract
Objective
COVID-19 may lead to a range of clinical outcomes among older people with psychiatric and medical conditions. Evidence guiding management of future outbreaks among this vulnerable population in psychiatric hospital settings are sparse. In this study, we examined the correlates of poor clinical outcomes related to COVID-19 and explored the perspectives of COVID-19 survivors hospitalized in psychiatry settings.
Method
The correlates of poor clinical outcomes related to COVID-19 were examined using a retrospective chart review of 81 older people hospitalized in psychiatry settings. Correlates of clinical outcomes related to COVID-19 were assessed by multiple logistic regression models. In addition, the perspectives of 10 COVID-19 survivors were explored by qualitative interviews. The qualitative data was subject to thematic analysis.
Results
Although 25.9% (n = 21) participants were asymptomatic, there was high COVID-19 related mortality (14.8%; n = 12). Vitamin-D deficiency, anticholinergic burden, and isolation policies within psychiatric wards were significantly (p < 0.05) related to COVID-19 related deaths. In qualitative interviews, participants emphasized the importance of strengthening local support networks and making vaccination centers more accessible.
Conclusions
Reducing anticholinergic prescriptions and improving isolation policies may help to mitigate poor clinical outcomes. Future research investigating the impact of vitamin-D supplementation on COVID-19 related outcomes is warranted.
Introduction
Coronavirus disease 2019 (COVID-19) is the most consequential global health and economic crisis of the 21st century. 1 The United Kingdom (UK) is one of the most affected countries, and more than 192,000 people have lost their lives due to COVID-19 in the UK. 2 Morbidity and mortality related to COVID-19 are higher among those aged over 65 years.3-8 A growing body of evidence including recent systematic reviews highlight the increased risk of poor clinical outcomes and deaths related to COVID-19 among people with psychiatric illness and/or chronic physical illnesses.3,9-17 Older people with multiple psychiatric and physical illnesses are one of the most vulnerable groups for experiencing COVID-19 related poor clinical outcomes. However, COVID-19 leads to highly variable clinical outcomes within this vulnerable population. Pertinent data on the factors associated with poor clinical outcomes related to COVID-19 among older people with psychiatric illness, especially in inpatient psychiatric settings, remain sparse. 18 There is little evidence to guide the management of future outbreaks among older people with psychiatric and physical illnesses in inpatient psychiatric settings. 19 There are ongoing efforts by the UK Government to learn lessons from the pandemic. 20 There is urgent need for gathering more evidence to guide the management of COVID-19 outbreaks in inpatient old age psychiatry settings. Hence, we aimed to address this need by investigating the clinical outcomes of COVID-19 and the correlates of poor clinical outcomes among older people in inpatient psychiatry settings. Moreover, we conducted in-depth interviews to explore the perspectives of older people with psychiatric illnesses, who have survived COVID-19.
Methods
Study design
We conducted a mixed-method study. A retrospective review of electronic medical records and medication charts was conducted to investigate the correlates of poor clinical outcomes related to COVID-19 among older people in inpatient psychiatry settings. We adopted a case control design framework to identify the sociodemographic, health, and treatment variables associated with poor clinical outcomes related to COVID-19. Later, we conducted in-depth telephone interviews to explore the perspectives of older people with psychiatric illness, who survived COVID-19 in inpatient psychiatry settings.
Setting
The mental health services for older people (MHSOP) in the Nottinghamshire Healthcare National Health Service (NHS) Foundation Trust (NOTTSHC) provides mental health care for people with dementia and older people with mental health needs in Nottinghamshire, UK. The NOTTSHC MHSOP includes five inpatient wards with a total of 91 mental health beds.
Participants
All service users, who have received treatment in a NOTTSHC MHSOP ward and have been diagnosed with COVID-19 during their treatment, including people with early onset dementia (age<65 years) were included in the retrospective chart review. Eligible psychiatric inpatients were not excluded because of their age, gender, ethnicity, language, or clinical diagnoses, unless they requested to opt out of the chart review. We obtained necessary ethics approval from the London South-East Research Ethics Committee (REC). The REC advised removing the consenting process for the retrospective chart review because all members of the research team provided direct clinical care in the NOTTSHC MHSOP in-patient units and they had access to the medical records. Among those who were included in the retrospective chart review, all eligible psychiatric inpatients, who had capacity to make an informed decision regarding participating in in-depth interviews, were considered for the qualitative component. Those, who provided written informed consent, were recruited for the in-depth interviews.
Recruitment
This study was conducted from April 2020 to May 2021. We did not include the potential SARS-CoV-2 B.1.1.529 (Omicron) variant cases of COVID-19 in this analysis. Consecutive sampling of all eligible psychiatric inpatients was employed for the retrospective chart review. All authors provided direct clinical care in the NOTTSHC MHSOP psychiatry in-patient units. They had access to the electronic medical records and medication charts of the psychiatric inpatients, who were eligible to be included in the retrospective chart review. Purposive sampling was used to recruit people for the in-depth interviews. Eligible people, who had capacity and were able to provide written informed consent, participated in the in-depth interviews.
Retrospective chart review
We collected data on sociodemographic profiles, psychiatric illnesses, medical illnesses, current mental and physical health medications, COVID-19 symptom profile, COVID-19 isolation practices, and clinical outcomes related to COVID-19 of all psychiatric inpatients from their electronic medical records and medication charts using a structured proforma. We estimated the total anticholinergic burden due to all current mental and physical health medications for each psychiatric inpatient using the Medichec online tool (https://medichec.com/). 21 The UK Government currently defines all deaths within 28 days of a positive COVID-19 test as COVID-19 related deaths, 2 and we followed this definition. We defined poor clinical outcome related to COVID-19 by the need for general hospital or intensive care unit (ICU) admission due to COVID-19 or death related to COVID-19. 2
In-depth interviews
We contacted all (n = 27) eligible psychiatric inpatients, who survived COVID-19 and were deemed to have capacity by their treating clinicians to make an informed decision regarding participating in in-depth interviews. 10 of them provided written inform consent. Three declined without specifying any reason. The reported reasons for declining were being too unwell to participate in the study (n = 8) and being unable to recall the experience of COVID-19 with adequate detail (n = 6). All ten in-depth interviews were conducted over telephone. Each interview lasted between 45 and 60 minutes, and all interviews were audio-recorded. The in-depth interviews were guided by the following five themes: (i) personal experience of COVID-19, (ii) experience of health service use, (iii) personal coping mechanisms, (iv) suggestions for improving existing health services, and (v) suggestions for further research. Supplementary material 1 presents the interview guide. The recorded interviews were transcribed verbatim. The transcription accuracy was checked and confirmed by an investigator, who conducted all in-depth interviews.
Data analysis
Data from the retrospective chart review were analysed using STATA-17.0 (Stata Corp LLC, TX, USA). Frequencies and proportions were calculated for all categorical study variables. Correlates of clinical outcomes related to COVID-19 were assessed by calculating adjusted odds ratios (AOR) with 95% confidence intervals (95% CI) using multiple logistic regression models that included age and gender as co-variates. All associations with P-values less than 0.05 were considered statistically significant. Moreover, we analysed the qualitative data using thematic analysis. Through an iterative process, transcribed qualitative data were mapped onto a framework that was revised to include new concepts. The emerging codes from the iteration process were refined and filtered into categories. The emerging sub-themes were harnessed and refined into broad themes. 22 Later, each theme was summarised and interpreted to address the study objectives. We enhanced reflexivity by collaborative discussion of our qualitative findings within our research team and with our clinical colleagues.
Results
Participants’ characteristics
Sociodemographic and Clinical Characteristics of Psychiatric Inpatients who were Included in the Retrospective Chart Review (n = 81).
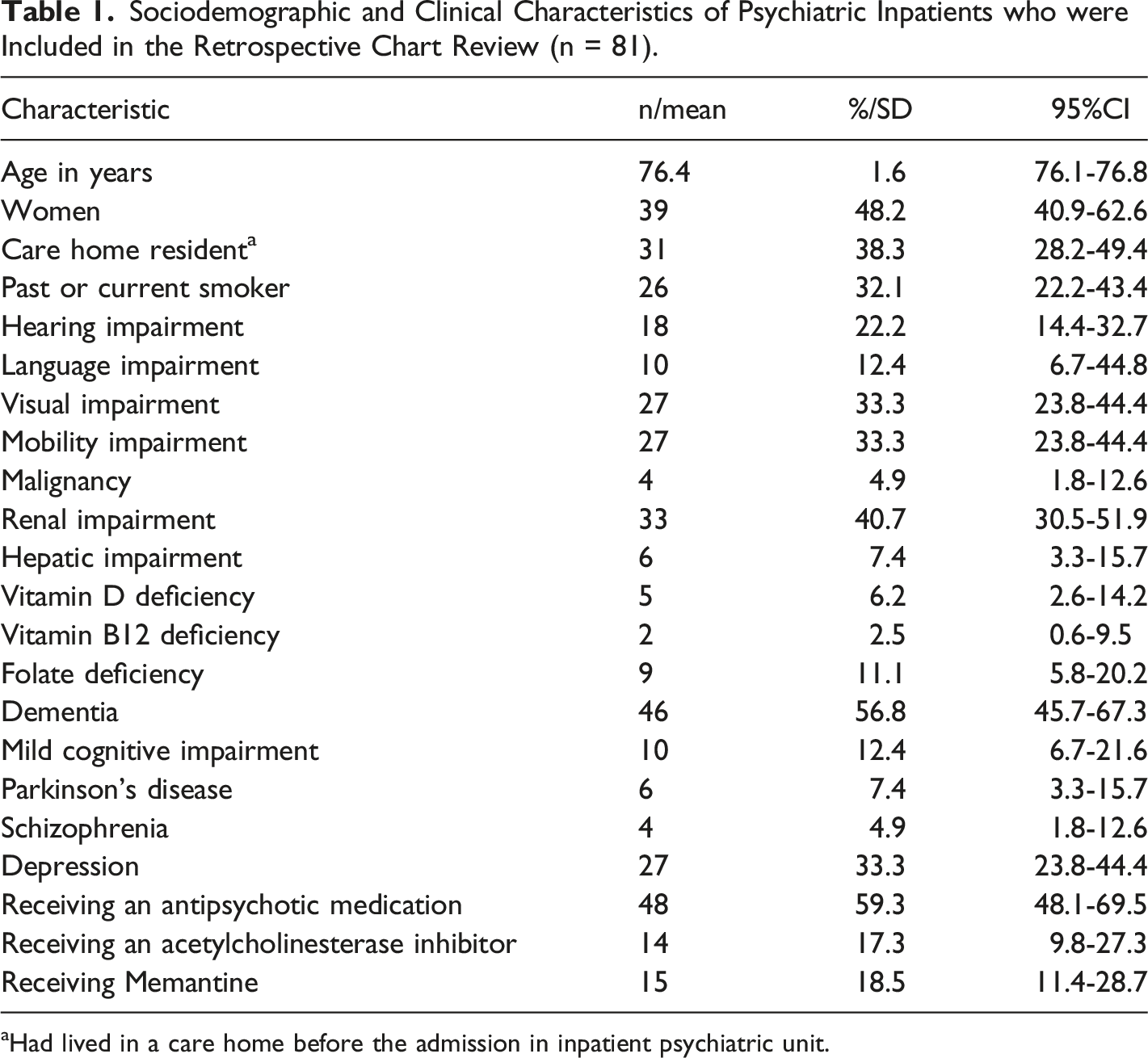
aHad lived in a care home before the admission in inpatient psychiatric unit.
Thirty six (44.44%; 95% CI 33.89-55.52%) psychiatric inpatients were receiving an antidepressant medication. Mirtazapine (n = 14; 17.28%; 95% CI 10.43-27.27%) was the most commonly prescribed antidepressant, followed by Venlafaxine (n = 7; 8.64%; 95% CI 4.13-17.20%), Trazodone (n = 6; 7.41%; 95% CI 3.32-15.69%), and Sertraline (n = 5; 6.17%; 95% CI 2.56-14.15%). A benzodiazepine was regularly prescribed to 14 (17.28%; 95% CI 10.43-27.27%) psychiatric inpatients, and five (6.17%; 95% CI 2.56-14.15%) were on Lithium. Moreover, eighteen (22.22%; 95% CI 14.37-32.72%) psychiatric inpatients were voluntarily admitted, when they had COVID-19. 39 (48.15%; 95% CI 37.36-59.11%) and 24 (29.63%; 95% CI 20.60-40.59%) psychiatric inpatients were admitted under the UK mental health act (MHA) and the mental capacity act (MCA), respectively. Mean duration of mental health hospital stay before testing positive for COVID-19 was 48.26 (95% CI 38.42-58.10) days.
Clinical manifestations
Twenty one (25.92%; 95% CI 17.45-36.70%) psychiatric inpatients did not experience any COVID-19 related symptom. The prevalence of COVID-19 related symptoms was as follows: fever (n = 31; 38.27%; 95% CI 28.23-49.42%), cough (n = 35; 43.21%; 95% CI 32.75-54.32%), reduced oxygen saturation (n = 41; 50.62%; 95% CI 39.71-61.47%), confusion (n = 32; 39.51%; 95% CI 29.35-50.66%), and other symptoms including changes in smell and taste (n = 28; 34.56%; 95% CI 24.91-45.68%). The COVID-19 isolation policies and practices varied during the study period. 34 (41.98%; 95% CI 31.61-53.10%) psychiatric inpatients were transferred to a dedicated COVID-19 isolation ward within NOTTSHC MHSOP, after they tested positive for COVID-19, and they were cared for in that isolation ward for the following 14 days. 24 (29.63%; 95% CI 20.60-40.59%) psychiatric inpatients stayed in their mental health wards, and they were isolated from COVID-19 negative psychiatric inpatients in their wards for periods varying between 7-14 days. 23 (28.40%; 95% CI 19.54-39.30%) psychiatric inpatients remained in their mental health wards without any segregation from COVID-19 negative psychiatric inpatients.
Correlates of mortality
Correlates of Poor Clinical Outcomes and Deaths Related to COVID-19 among the Psychiatric Inpatients (n = 81).
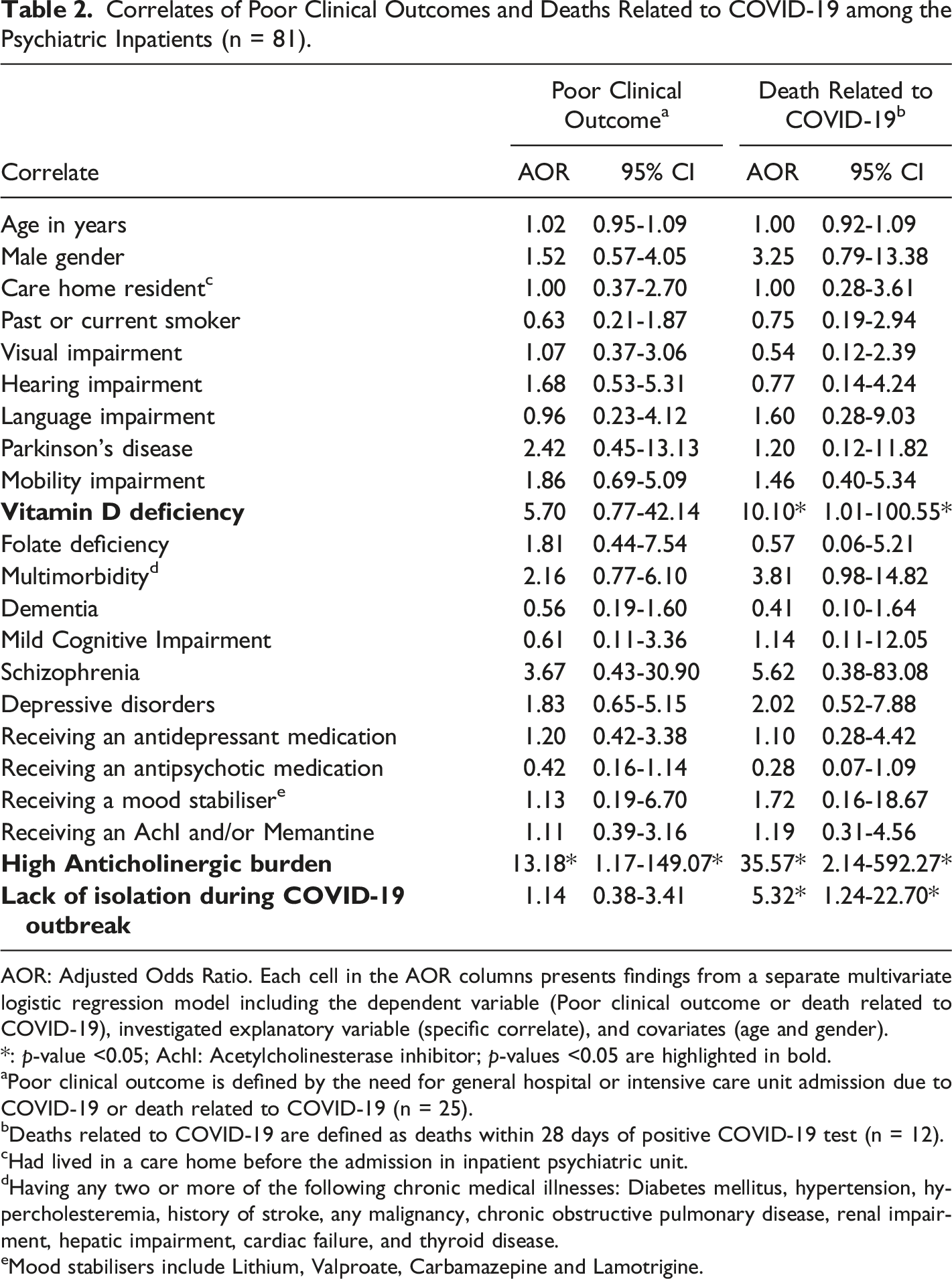
AOR: Adjusted Odds Ratio. Each cell in the AOR columns presents findings from a separate multivariate logistic regression model including the dependent variable (Poor clinical outcome or death related to COVID-19), investigated explanatory variable (specific correlate), and covariates (age and gender).
*: p-value <0.05; AchI: Acetylcholinesterase inhibitor; p-values <0.05 are highlighted in bold.
aPoor clinical outcome is defined by the need for general hospital or intensive care unit admission due to COVID-19 or death related to COVID-19 (n = 25).
bDeaths related to COVID-19 are defined as deaths within 28 days of positive COVID-19 test (n = 12).
cHad lived in a care home before the admission in inpatient psychiatric unit.
dHaving any two or more of the following chronic medical illnesses: Diabetes mellitus, hypertension, hypercholesteremia, history of stroke, any malignancy, chronic obstructive pulmonary disease, renal impairment, hepatic impairment, cardiac failure, and thyroid disease.
eMood stabilisers include Lithium, Valproate, Carbamazepine and Lamotrigine.
Poor clinical outcomes
COVID-19 led to general hospital or ICU admission of 22 (27.16%; 95% CI 18.49-38.00%) psychiatric inpatients. Total number of psychiatric inpatients, who either required general hospital or ICU admission due to COVID-19 or died within 28 days of a positive COVID-19 test, was 25 (30.86%; 95% CI 21.67-41.88%). Table 2 presents the correlates of COVID-19 related poor clinical outcomes (n = 25). High anticholinergic burden 21 was the only study variable that was significantly (P = 0.037) associated with COVID-19 related poor clinical outcomes, after accounting for the effects of age and gender of the psychiatric inpatients. None of the sociodemographic variables, medical illnesses, mental health diagnoses, or physical health and mental health medications was significantly associated with COVID-19 related poor clinical outcomes.
Personal experience
Eight women and two men completed the in-depth interviews. Their mean age was 69 (95% CI 64.48-73.52) years. 2 of them had mild cognitive impairment, and two had required general hospital admission because of COVID-19. Figure 1 summarises the perspectives of the psychiatric inpatients, who survived COVID-19 in inpatient psychiatry settings, and Figure 1A summarises the psychiatric inpatients’ perspectives on their personal experience of COVID-19. Most participants reported asymptomatic or mild flu-like illness and good recovery. However, a participant reported feeling depressed because of perceived confinement and isolation. She said, “I think COVID didn’t affect me emotionally. It was the confinement that affected me. We all had to stay in one track of the of the ward and were not allowed to leave. We just had a like a 20 meters corridor to walk up and down and then your room”. Two participants reported experiencing persisting cough, fatigue, and headache after COVID-19. Apart from them, most participants reported that they were “almost back to normal”. They conveyed that there had not been any significant difference in their lives after COVID-19, except for their difficulties with social isolation. A summary of the psychiatric inpatients’ perspectives. (A) The psychiatric inpatients’ personal experience of COVID-19; (B) The psychiatric inpatients’ experience of health service use; (C) The psychiatric inpatients’ suggestions for improving existing health services.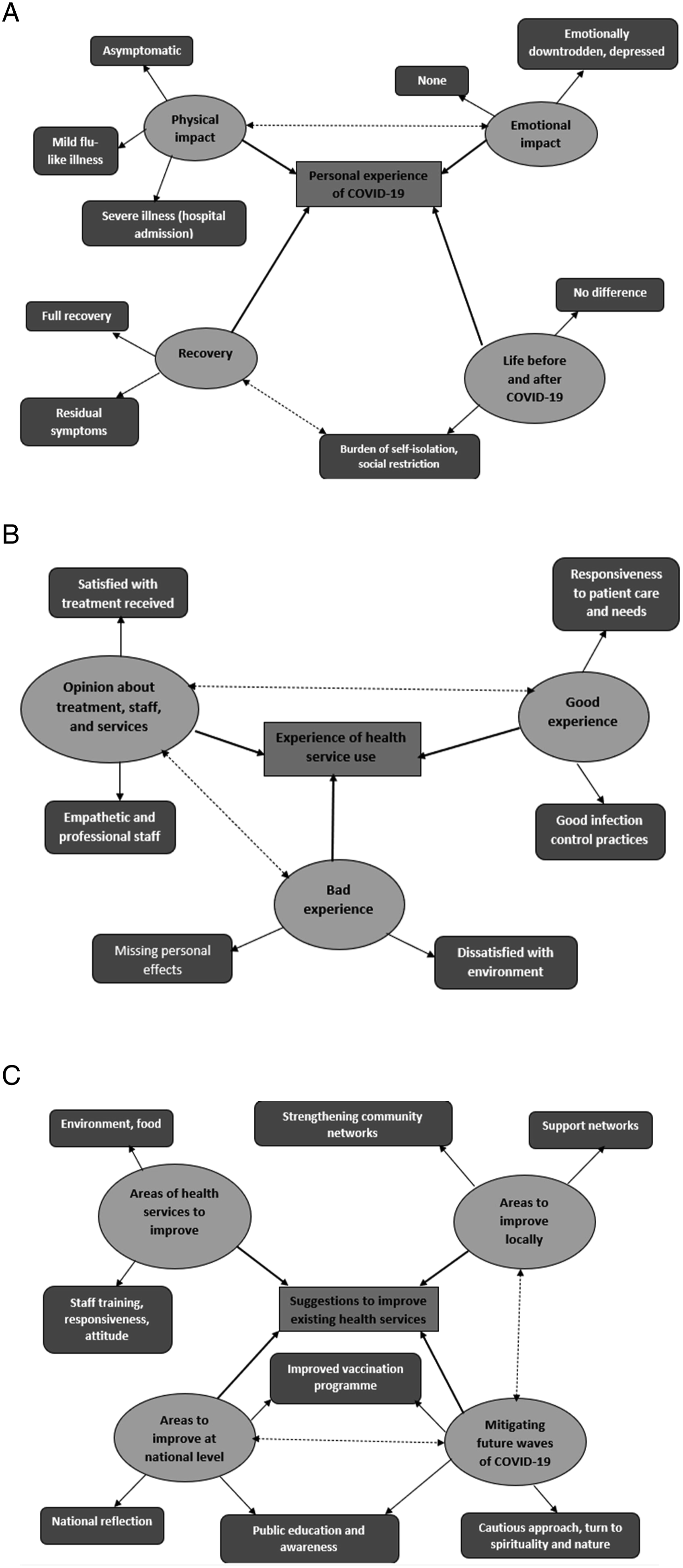
Experience of health services
Figure 1B provides an overview of the psychiatric inpatients’ perspectives on their experience of existing health services. We explored the psychiatric inpatients’ perspectives on staff, existing health services, and good and bad aspects of their experience. Nearly all psychiatric inpatients (90%; n = 9) reported satisfaction with staff and health services. They described the staff as “good and professional” and “responsive and helpful”. Several psychiatric inpatients appreciated good infection prevention and control practices and the need for isolation. However, COVID-19 related staff absence led to increased need for ad hoc staff. A few psychiatric inpatients reported concerns regarding the treatment, received from ad hoc staff. They conveyed that some ad hoc staff had not been so compassionate as usual ward staff, and that they were “missing personal effects”.
Coping with COVID-19
We discussed the strategies that helped to cope with COVID-19, and those that did not. Occupational therapy input, physical exercise within wards, reading books, listening to radio, and turning to hobbies reportedly helped coping with COVID-19. Several participants highlighted the benefits of peer support, especially from other COVID-19 positive psychiatric inpatients in their ward, and of spiritual coping mechanisms including prayers. A psychiatric inpatient stated, “I think God has sent this as a warning…We've got a beautiful world”. Another female psychiatric inpatient said, “I learnt to be a bit more careful with who I speak to and who I contact”. More than half of the psychiatric inpatients described their learning on the importance of wearing masks, following social distancing guidelines, and focusing on their physical health. Most psychiatric inpatients reported that their life after COVID-19 had been hampered by social isolation. A psychiatric inpatient explained how social isolation interfered with her rehabilitation in her local community after discharge, and how this negatively impacted her mental health.
Suggestions for improvement
Figure 1C summarises the psychiatric inpatients’ suggestions for improving health services. Participants suggested having more single rooms within mental health wards, improving food quality, and improving staff responsiveness and efficiency of managing COVID-19 outbreaks by further training. We explored the psychiatric inpatients’ suggestions for improving services at regional and national level. Several psychiatric inpatients emphasised the importance of strengthening local support networks, and suggested improving the sense of togetherness in their community. At the national level, the psychiatric inpatients suggested reflection on relevant national policies, learning from mistakes, enhancing public education and awareness about viral infections, increasing the number of vaccination centres, and making vaccination centres more accessible. When we explored their suggestions for mitigating further waves of COVID-19, the psychiatric inpatients suggested a cautious approach, turning to nature and spirituality, keeping people more informed about the rationale for social distancing policies, and improving public education and awareness about COVID-19.
Discussion
To the best of our knowledge, this is the first study that investigated the clinical outcomes of COVID-19 and their correlates among older people with psychiatric morbidity in specialist in-patient psychiatry setting. Prescription of medications with high anticholinergic burden was significantly associated with COVID-19 related poor clinical outcomes and deaths. Vitamin-D deficiency and isolation policies were significantly associated with COVID-19 related deaths. The strengths of this study include collecting detailed clinical data, consecutive sampling, broad eligibility criteria, including people with dementia, excluding potential Omicron variant cases of COVID-19, and gathering qualitative data.
The prevalence of asymptomatic COVID-19 (25.93%) in this study is less than that of nursing home residents (47.53%). 23 This may be attributed to higher prevalence of comorbid physical illnesses in this sample, and more frequent physical health monitoring in the in-patient psychiatry setting. New-onset confusion and worsening of confusion were the third most frequent COVID-19 related symptom, and this highlights the need for regular screening for delirium in this population. 24 Moreover, the all-cause mortality rate in this vulnerable population is higher than that of nursing home residents with COVID-19 in England. 25 There is urgent need for future research focusing on COVID-19 outbreaks in in-patient psychiatry settings, and for developing an evidence-based guidelines for managing future outbreaks in these settings. 19
Prescription of medications with high anticholinergic potential increases the risk of poor physical and cognitive outcomes in older adults.21,26 Polypharmacy and high anticholinergic burden have been associated with increased risk of poor clinical outcomes related to COVID-19.27,28 Our findings corroborate the association of high anti-cholinergic burden with COVID-19 related poor clinical outcomes, and add novel evidence for its association with COVID-19 related deaths. Biological mechanisms underlying these associations should be investigated further. Anticholinergic medications may impair mucociliary transport 29 and they increase the risk of pneumonia in older people. 30 They may increase the risk of aspiration by worsening confusion. Because of our limited sample size, we could not ascertain the contributions of individual anticholinergic medications towards COVID-19 related poor clinical outcomes. Reviewing anticholinergic burden of all prescribed medications, 21 and reducing prescription of medications with moderate to high anticholinergic potential may mitigate COVID-19 related poor clinical outcomes.31,32
Vitamin-D deficiency is associated with higher risk of COVID-19 infection.33,34 A systematic review that included 43 studies on COVID-19 has reported statistically significant associations of vitamin-D deficiency with the severity of COVID-19 symptoms and the case fatality rate. 35 However, another systematic review could not replicate the statistically significant association between vitamin-D deficiency and COVID-19 related deaths. 36 Vitamin-D is an immunomodulator that influences the innate and adaptive immune response to COVID-19. 37 However, the evidence supporting the routine use of vitamin-D supplementation for reducing COVID-19 related deaths and/or ICU admissions remain inconclusive.38-40 Our findings support the need for larger clinical trials investigating the efficacy of vitamin-D supplementation for reducing COVID-19 related deaths.
There is legal guidance for services supporting people of all ages with COVID-19 in the UK, 19 and we do not have any evidence-based guidelines for managing COVID-19 outbreaks in specialist in-patient psychiatry settings. The legal guidance discourages blanket bans, and supports the least restrictive services. It acknowledges the justifiable need for restrictive practice for maintaining the safety of psychiatric inpatients, such as isolating people with COVID-19 without their consent. 19 The public health and Government policies regarding COVID-19 were frequently changing during the study period in the UK. 20 Systematic evidence regarding the safety and the risks of following COVID-19 “social bubbles” in hospital wards is lacking. Our study provides an important preliminary evidence that such lack of segregation between COVID-19 positive and COVID-19 negative inpatients during COVID-19 outbreak in mental health wards increases the risk of COVID-19 related deaths. Although this finding should be interpreted with caution because of the methodological limitations, we recommend avoiding such “social bubbles” in acute mental health wards, especially in old age psychiatry settings, until the emergence of any evidence supporting this approach.
The SARS-CoV-2 variants and their clinical presentations have changed over time. However, we increasingly recognise the importance of learning the lessons and of being prepared for future COVID-19 and similar outbreaks in mental health wards. Pertinent research in specialist mental health settings and emphasising patient and public involvement are essential for making mental health services safer and more effective. COVID-19 survivors highlighted the importance of psychosocial interventions, spiritual coping mechanisms, strengthening local support networks and making vaccination centres more accessible. Such a holistic approach may facilitate improving the clinical outcomes of older people with psychiatric illness.
Study limitations
We should consider the limitations of its retrospective design, small sample size, exploratory data analysis, near absence of minority ethnic psychiatric inpatients, and lack of qualitative data from psychiatric inpatients with dementia. Our retrospective study design cannot establish causal relationships between the observed associations. Moreover, it will be challenging to generalise the findings of this single site study to other clinical settings that are different from ours.
Conclusions
Our findings support the need for reviewing anticholinergic burden of all prescribed medications, and reducing prescription of medications with moderate to high anticholinergic potential for older people with psychiatric morbidity. They add evidence for the association between vitamin-D deficiency and COVID-19 related deaths. They highlight the lack of evidence for implementing “social bubbles” during COVID-19 outbreaks in old age psychiatry inpatient settings. Moreover, our qualitative findings emphasise the importance of psychosocial interventions, spiritual coping mechanisms, and strengthening local support networks for improving clinical outcomes.
Supplemental Material
Supplemental Material - Correlates of poor clinical outcomes related to COVID-19 among older people with psychiatric illness - a mixed methods study
Supplemental Material for Correlates of poor clinical outcomes related to COVID-19 among older people with psychiatric illness - a mixed methods study by Surajudeen Abdulrahman, Naser Al-Balushi, Jason Holdcroft-Long, Uzma Khan, Bipin Ravindran, Sujata Das, and Anto P Rajkumar in The International Journal of Psychiatry in Medicine
Footnotes
Author contributions
We confirm that all authors met the four ICMJE criteria for authorship. SD, BR and APR conceived this study, and APR wrote the study protocol. JHL, UK, SD, BR, and APR completed the retrospective chart review. SA completed the in-depth interviews. SA and APR transcribed the in-depth interviews. NA and APR analysed the retrospective chart review data. SA analysed the qualitative data. SA and NA wrote the initial manuscript. APR provided necessary supervision for SA and NA. All authors were involved in critical revisions of the manuscript and all authors have approved the final submitted version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the authors’ time dedicated for this research, and their salaries were supported by the Nottinghamshire Healthcare NHS Foundation Trust, Nottingham, UK.
Ethical approval
This research has obtained ethics approval from the London South-East Research Ethics Committee (20/LO/1282/133124/2020).
Informed consent
Written informed consent was obtained from all participants before the in-depth interviews.
Data availability
The data that supports the findings of this study are available on request from the corresponding author (APR).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.