
Abstract
Diminished vitamin D is common among older individuals. Sunlight contributes more to vitamin D synthesis than diet or supplementation. This study examined associations between objectively measured light exposure, vitamin D serum levels, and bone biomarkers in 100 men aged over 60 years. Light exposure was measured in lux via Actigraph monitors for 1 week. Significantly, greater levels of vitamin D were observed in participants with higher light exposure. Seasonal differences in lux were also noted. Significant differences in bone markers were not found. Objective measurement of light exposure is an inexpensive, simple, and effective way to address vitamin D deficiency.
Older adults, particularly those housebound, are susceptible to vitamin D deficiency and insufficiency because of reduced sunlight exposure, inadequate nutrition, dermatological changes, and diminished renal function (Witham and Francis, 2014). Reduced levels of circulating serum 25-hydroxyvitamin D (25(OH)D) have been associated with muscle weakness and reduced bone mineral density (BMD), along with subsequent falls and fractures leading to increased nursing home admissions (Weaver et al., 2010). Chronic deficiency results in osteomalacia (bone softening; known as rickets in children), osteoporosis (porous bone), faster turnover of calcium metabolic activity, and an increase in production of parathyroid hormone (PTH), which exacerbates the process of weakening bones (Parfitt et al., 2011; Visser et al., 2003). Vitamin D is also suspected to be important for maintaining proper immune system operation and cognitive function (Buell et al., 2010; Holick, 2004). Vitamin D may also offer a protective factor in a broad range of diseases such as diabetes, cancer, multiple sclerosis, Alzheimer’s disease, and dementia (Buell et al., 2010; Holick, 2004; Lips, 2001; Sakem et al., 2013).
The US Department of Health and Human Services estimated that one-third of the total US population is at risk due to insufficient (25(OH)D concentrations between 20 and 30 ng/mL) or deficient (25(OH)D concentrations below 20 ng/mL) levels of vitamin D and global estimates are as high as 40–50 percent for older adults having vitamin D deficiency (Buell et al., 2009; Laurentani et al., 2010; Looker et al., 2011; Sakem et al., 2013). Falls and associated injuries were estimated to cost the US$30 billion in 2010 (Center for Disease Control (CDC), 2014). Significant public health benefits such as increased quality of life and years of active life as well as reduced cost and burden of institutionalized and home direct care could potentially be realized by fewer falls and related consequences (American Geriatrics Society Workgroup, 2013).
The vitamin D precursor, 7-dehydrocholesterol, is activated in the skin by ultraviolet light (UVL), usually from the sun, but intense fluorescent lighting (emitting UV) can also induce the synthesis of vitamin D (Holick, 1996; Lips, 2001; Parfitt et al., 2011). The most widely accepted treatment for insufficient and deficient vitamin D level is oral supplementation; however, some have noted that this method for addressing the end goals of increasing physical function and reducing falls may not provide these benefits (Cummings et al., 2016; Hansen et al., 2015; Moyer; U.S. and Preventive Services Task Force, 2013). While dietary intake and supplementation augment production of vitamin D and provide a sparring effect, light exposure has been documented to provide as much as 90 percent of an individual’s vitamin D requirement (Hall et al., 2010; Holick, 2004; Lips, 2001; Lips et al., 2014). However, the amount of light exposure necessary to positively affect 25(OH)D levels varies based on personal circumstances (Holick, 2004; Lips, 2001; Lips et al., 2014). Latitudinal location and time of year are two major determinants of vitamin D production. Those living in more northern locations may experience virtually no vitamin D production for nearly half of the year (Lips, 2001). Production is also heavily determined by skin composition as well. Vitamin D production is higher in lightly pigmented skin compared to heavily pigmented skin (Lips, 2001). Furthermore, the skin in senior adults can continue to produce the precursors of vitamin D, but research shows that this organ no longer does so as efficiently as during youth because of reduced 7-dehydrocholesterol levels (American Geriatrics Society Workgroup, 2013; MacLaughlin and Holick, 1985; Sakem et al., 2013). Also, in an effort to reduce skin cancer, public health organizations have given blanket recommendations to limit sun exposure and increase use of sunscreen, which could be reducing population levels of 25(OH)D (Sinha et al., 2013). It has been suggested that a minimal “10-min exposure of head and arms (unprotected) three times per week is adequate to prevent vitamin D deficiency” or “doses small enough to produce only minimal tanning” can create beneficial increases in 25(OH)D (Armas et al., 2007; Lips, 2001).
Current research has not consistently demonstrated beneficial effects or reduced risk of disease and falls in the older population with the exclusive use of oral vitamin D supplementation (Bolland et al., 2014; Hansen et al., 2015). However, despite continued debate on the role of supplementation in producing various positive outcomes, there is little doubt that sunshine is the most important contributor to healthy vitamin D levels (Autier et al., 2014; Theodoratou et al., 2014). Research in objective monitoring of light exposure in respect to vitamin D and bone markers may yield valuable insight into diagnostic and treatment protocols in the older population.
One of the routinely used means of collecting outdoor activity and light exposure is via sunlight exposure questionnaires. Advantages of these instruments include low cost, fairly uncomplicated administration, and standardization (Falk and Anderson, 2012). However, questionnaires may provide imprecise measurement of vitamin D status due to the wide variety of personal factors that inhibit vitamin D production, such as sunscreen use, clothing material, and melanin pigment (Cargill et al., 2013; McCarty, 2008). Wearable light detection monitors have the potential to become valuable objective tools whose benefits include cost effectiveness, small size, and light weight, practicality in participants’ natural environments, and allowance for monitoring over long-term periods (Martin and Hakim, 2011). This method is also an effective means of reducing recall and reporting bias that could negatively impact the data.
Previous research to determine a correlation between objectively measured light in lux (one lumen per square meter) and serum 25(OH)D levels has been limited and yielded mixed results. Calogiuri et al. (2013) found no significant differences in vitamin D levels for those in an outdoor versus indoor activity group but did find a small positive correlation between vitamin D levels and objectively measured light exposure. Their participant group was limited in size (14), and the timetable between light exposure and blood draws being less than 24 hours post-exposure may have been too short to have demonstrated a significant difference in vitamin D levels. In another similar study, researchers in Korea were unable to confirm a relationship between serum 25(OH)D and sunlight measured by objective means; however, they noted a small sample size (20 women) and low compliance with outdoor activity due to cold weather during their November collection period as potential limiting factors (Lee et al., 2012).
Clearly, institutionalized and/or housebound elderly individuals are at greater risk of vitamin D deficiency. So, what is the likelihood of vitamin D deficiency or insufficiency in an older population if they are relatively active? The Robert E. Mitchell Center for Prisoner of War Studies had a unique opportunity to measure light exposure in a prior research project where activity and sleep were measured, and lux was included. We sought to identify in the same cohort of 120 older men whether light levels, measured by lux as a feature of ActiGraph accelerometer monitors, correlated with vitamin D and associated bone metabolic biomarkers.
Methods
Participants
The participants were a subset of Vietnam-era repatriated prisoners of war (RPWs) from all branches of services, as well as a matched comparison group (CG) of combat veterans (who had been in similar combat but were never captured/imprisoned). They have been voluntary contributors to the Robert E. Mitchell Center for Prisoner of War studies annual medical and psychological follow-up program within the Department of Defense since 1973. Their ages range from 61 to 86 years (mean = 73, standard deviation (SD) = 5). This study comprises 100 participants (76 RPWs and 24 CGs) who took part in medical follow-up at the Center between May 2012 and June 2013. Participants reported being in good physical health for their ages and were able to travel to the Mitchell Center in Pensacola, Florida, to engage in the study. Their average grip strength was above normal (45 kg) and their comfortable walking gait was on par with their age group (1.3 m/s) (Bohannon, 1997; Massey-Westropp et al., 2011). The majority of them were free from psychological diagnoses (76 participants). They supplied actigraphy and lux data and had a vitamin D assay collected as part of their routine medical follow-up. The other 20 from the original study (Fields et al., 2015) were omitted because they did not have a vitamin D assay collected at the time of actigraphy collection. Particulars of this cohort have been previously published (Segovia et al., 2013). This study was reviewed and approved by an institutional review board, and all participants included in this research have consented to being included in the study.
Lux meters
ActiGraph™ GT3X+ monitors (Actigraph™; LLC, Pensacola, FL, USA) with lux meters were used to gather exposure to light in our participants. These actigraphy monitors include triaxial accelerometers that identify movement, steps, kilocalories, as well as lux. The monitors have 512MB of memory and activity and light collection occurred at 30 Hz. Participants wore the monitor for seven consecutive days and nights on their non-dominant wrist. Typical lux level estimates for the GT3X+ were as follows (Table 1).
Lux level estimates.

Source: Hawks (2012).
Procedures
Blood samples were obtained as part of routine clinical practice, which included serum vitamin D, and other relevant bone biomarker data (calcium, phosphorous, and alkaline phosphatase). Actigraphy monitors with lux meters were scheduled to turn on when participants returned home. Lux levels were collected for 7 days and nights from 92 of the 100 participants. Of the remaining eight participants, seven wore the ActiGraph for 6 days, and therefore, lux was gathered for only those 6 days, and one participant wore the ActiGraph for only 4 days. These eight had forgotten to put on the device at the designated time.
Data analysis
A vitamin D assay of 30–100 ng/mL is widely considered within normal limits. Using this criterion as a cut point for normal (⩾30 ng/mL) and abnormal (<30 ng/ml) vitamin D levels, the data were divided into these two groupings to compare average daily light (in lux) exposure collected from the ActiGraph and the associated bone metabolic biomarkers. Since it took a year to collect this amount of data, seasonal differences had to be accounted for as well. The data were divided into the four seasons based on the official calendar start of the season in the northern hemisphere (i.e. fall, 21 September; winter, 21 December; spring, 21 March; summer, 21 June).
Results
Descriptive statistics of seasonal quartiles and mean lux illustrated differences in mean lux levels, particularly for fall and winter (see Table 2). A Bonferroni post-hoc alpha adjusted to p = .0125 (for four comparisons) indicated that winter lux levels were significantly lower than summer levels (p = .0001; large effect size = 1.75), and fall levels were significantly lower than summer levels (p = .011; large effect size = .803); but, spring versus winter was not significant because of the adjusted alpha for multiple comparisons. There were no significant differences between remaining seasonal levels (see Table 3).
Descriptive analysis of seasonal quartiles and mean lux differences.

Bonferroni analysis of seasonal quartiles and mean lux differences.

Descriptive statistics of vitamin D cut points between normal and abnormal serum levels showed mean lux differences (see Table 4). Independent t tests demonstrated statistically significant differences in mean lux levels between the two groups, t(98) = 2.53, p = .013. This difference was moderate in effect size (Cohen’s d = .51). The analysis of variance (ANOVA) for vitamin D by normal/abnormal levels was found to be significant (F(1, 98) = 6.38, p = .013, small effect size = .03) (Table 5).
Descriptive analysis of vitamin D cut points between normal and abnormal serum levels and mean lux.

ANOVA for normal/abnormal serum levels and mean lux.

ANOVA: analysis of variance.
Descriptive statistics of seasonal mean lux and vitamin D cut points between normal and abnormal serum levels illustrated some mean lux differences (see Graph 1). However, with the exception of the fall season, independent t-tests demonstrated no significant differences in mean lux levels between the two vitamin D groupings. Fall season’s significant mean lux difference between the two groups demonstrated a large effect size (Cohen’s d = 1.27). The ANOVA for vitamin D by the four seasonal levels was found to be significant (F(3, 96) = 7.36, p = .0001) (Table 6).
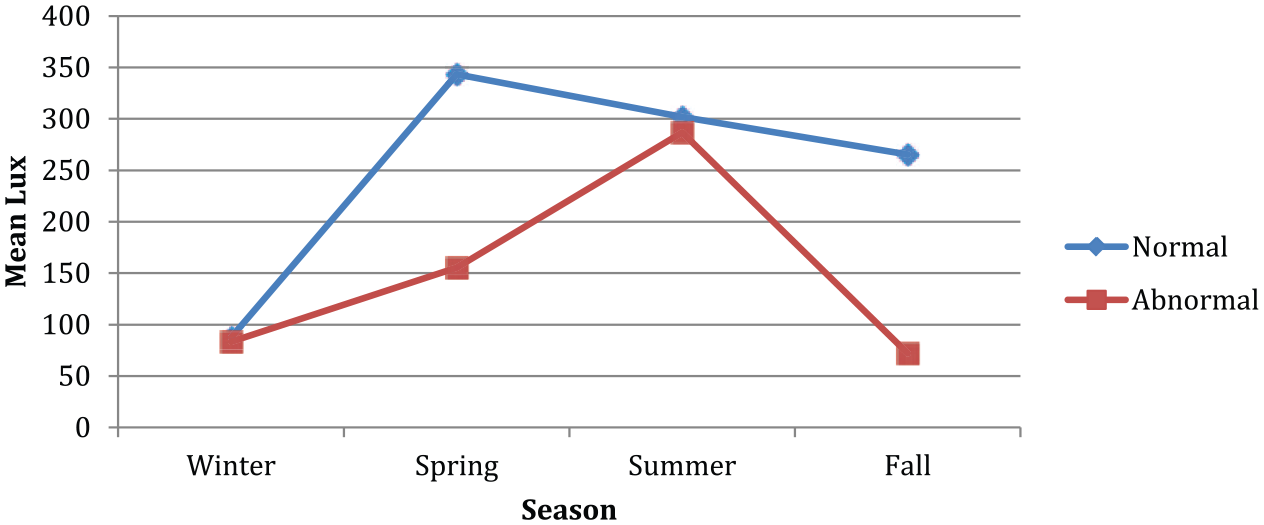
Seasonal mean lux and vitamin D cut points between normal and abnormal serum levels.
ANOVA for four seasonal levels and mean lux.

ANOVA: analysis of variance.
Descriptive statistics of the associated bone metabolic biomarkers showed no differences in the mean levels between the normal and abnormal vitamin D groupings, with the exception of possibly alkaline phosphatase. However, independent t-tests showed no statistically significant differences in any of these bone metabolic markers (calcium, t(98) = 1.50, p = .137; phosphorous, t(98) = .913, p = .364; alkaline phosphatase, t(79.6) = 1.50, p = .138).
Discussion
For this cohort, sunlight exposure translated into significantly higher levels of vitamin D, which is congruent with previous research. This finding was expected since there is a direct correlation between exposure to ultraviolet B (UVB) and serum concentrations of vitamin D. While the associations were not robust across all potential interactions between objectively collected light and vitamin D values, some of the associations were significant and indicate that further evaluation within a larger and more controlled design is prudent. A broad range of personal factors could have influenced the data including diet, clothing choice, and sunscreen use.
While there is no globally accepted stratum defining vitamin D values, a vitamin D assay of 30–100 ng/mL is commonly considered within normal limits. Using this criterion as a cut point for normal and abnormal vitamin D levels and comparing with average daily light (in lux) exposure collected from ActiGraph monitors, this study was able to partially establish anticipated seasonal differences in lux levels with winter and fall lux rates significantly lower than summer. These differences may be based upon seasonal sunlight variations as well as more amenable weather conditions that contribute to extended outdoor exposure. Also observed was an overall interaction between objectively measured sunlight with serum vitamin D levels showing that participants with abnormal vitamin D levels had significantly less average daily light exposure compared to those within normal limits of vitamin D. A significant increase in both lux values and vitamin D were observed during the fall season only. Contrary to expectation, the light exposure and vitamin D interaction was not significant across all seasons nor was it associated with bone metabolic markers.
Limitations
The use of a cohort of aged Caucasian men from a high socioeconomic status restricts the ability to generalize results to the average US population. Also, there were no data collected on diet, nutritional supplementation, or sunscreen use for the participants. Additionally, serum PTH levels may have provided additional insight but were not part of the routine laboratory tests. Finally, this study is a cross-sectional study, and causality cannot be determined. Despite these constraints, it is important to note that our findings are similar to results observed in previous research demonstrating the importance of continued research into objectively measured sunlight on the production of vitamin D and overall bone health.
Conclusion
With a large portion of the US population diagnosed with abnormal vitamin D levels and associated costs of fall-related injuries estimated in the billions of dollars, it is important to explore all available avenues of diagnosis and treatment of abnormal vitamin D. Today’s advances in technology have contributed to the production of smaller and less invasive personal health monitoring devices; the use of light meters to objectively obtain personal data on light exposure could offer healthcare providers, patients, and caregivers an opportunity to reliably evaluate reduced sunlight as a potential impediment to positive overall health. They could also provide a uniquely accurate and reliable tool for treatment and evaluation of any benefits received by sunlight therapy. Future research of vitamin D levels in older populations would benefit from the continued use of objectively measured sunlight exposure while controlling for such factors as dietary and supplementation intake of vitamin D as well as sunscreen use.
Footnotes
Acknowledgements
This article is a product of the Robert E. Mitchell Center for Prisoner of War Studies and was supported by a grant (ONR-FY13 N0001413AF00002) from the Office of Naval Research (ONR). The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the ONR or the Department of the Navy. The Robert E. Mitchell Center for Prisoner of War Studies would like to take this opportunity to give thanks to all our patrons for their participation in our studies, who make our research possible. To all our RPWs, we thank you for your courage, honor, and commitment. The staff of the Robert E. Mitchell Center is also to be commended for the high standard of healthcare provided to our patrons.
Declaration of conflict of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant (ONR-FY13 N0001413AF00002) from the Office of Naval Research (ONR). The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the ONR or the Department of the Navy.