
Abstract
Mobile health (mHealth) interventions for mental health and well-being have increased exponentially in recent years. In this digital era, mHealth interventions are proving to be a useful tool in the promotion of mental health for university students. This mixed-methods study explored the feasibility, practicality, and acceptability of a mental health application (app) designed to address mental health challenges among university students. Overall, a total of 1100 participants completed an online survey, and data were analysed using statistical analytics software. Most of the participants were female (72.73%) within the 18–20 age group (64.64%) and in their first year of study (46.18%). The results show that at least 98.7% of the participants owned a smartphone, 80.8% had access to mobile data, 66.9% used Android software, 20.09% had historically been diagnosed with a mental health challenge, and 26.6% had used an online health app. Sixty-two participants were enrolled across 16 focus group discussions. Qualitative data were analysed using thematic analysis, which revealed four facilitators of app acceptability (exposure to mental health apps, convenience, accessibility, and confidentiality) and three barriers to app acceptability (preference for face-to-face therapy, overreliance on app, and fear of misdiagnosis). The findings suggest that an app that is convenient, accessible, confidential, and nonpathologising can be a feasible and acceptable intervention to address mental health challenges.
Keywords
Globally, over 40% of university students have experienced symptoms of depression, 30% anxiety, and 48% stress (Brown, 2018). In South Africa, mental health challenges among university students are also on the rise (Bantjes et al., 2016). A national mental health survey conducted by Bantjes et al. (2023) among students at 17 South African universities estimated a 37% prevalence of anxiety disorders, with at least 24% of students reporting symptoms related to posttraumatic stress disorder and social anxiety disorder. Studies conducted in South Africa and the United Kingdom have shown that most university students in these countries with mental health challenges avoid seeking help despite the availability of free counselling services on campus (Bantjes et al., 2020; Kaminer & Shabalala, 2019; Mitchell et al., 2017). Global and South African research has shown that major barriers to help-seeking behaviour include low mental health literacy, stigma associated with receiving treatment, fear of diagnosis, reliance on friends, lack of trust in therapists, attending classes during the day, and cultural beliefs (Broglia et al., 2021; Hellem et al., 2022; Mitchell et al., 2017). Poor help-seeking behaviours contribute significantly to the mental health burden within the student population (Broglia et al., 2021). These elevated levels of mental health challenges and poor help-seeking behaviours among university students highlight the need for an intervention that is accessible and student-friendly. Developing a mental health application (app) specifically for university students can be a valuable and feasible intervention to address mental health challenges and help-seeking barriers among students.
Mobile health (mHealth) refers to the use of wireless technology, such as mobile phones, to achieve health objectives (World Health Organization, 2018). mHealth apps can deliver health information, track progress, and assist with behaviour change (Ben-Zeev et al., 2015). Global literature has suggested that mobile apps for mental health that are guided by therapeutic approaches such as cognitive behavioural therapy, interpersonal therapy, and mindfulness, may improve mental health challenges such as depression, anxiety, stress, and mood disorders (Haeger et al., 2022; McCloud et al., 2020). Systematic reviews based on global studies have shown that mental health apps guided by psychological theories are effective, suggesting that they can be used as an adjunct to face-to-face therapy (Khademian et al., 2021; Lui et al., 2017; McCloud et al., 2020; Wang et al., 2018; Wozney et al., 2017).
Over 20 million people in South Africa own a smartphone, and almost 70% of these individuals are young people between the ages of 15 and 25 years (Taylor, 2023). In addition, 75% of online traffic in South Africa is generated from mobile phone devices and 15% of the traffic comes from social media users between the ages of 18 and 35 years (Qwerty Digital, 2017). Research conducted in South Africa on smartphone use among university students shows that at least 51% of students spend over R120 (±$6.60) on data bundles monthly (Masiu & Chukwuere, 2018). With the heightened access to smartphones and mobile data, there is a high probability that the average South African university student owns a smartphone, uses their phone to access the internet, and is likely able to afford data, making a mobile health intervention both accessible and affordable for this population.
While a mobile phone intervention may be an appropriate endeavour based on accessibility and affordability, global research has also shown that excessive mobile phone use increases young people’ susceptibility to negative mental health (Lattie et al., 2019; Thomée, 2018; Wacks & Weinstein, 2021). Studies conducted in South Africa have also reported challenges related to mobile phone use among young people, such as smartphone addiction, lower social interactions, and symptoms of depression (Dietrich et al., 2021; Masiu & Chukwuere, 2018). Given these challenges, one could argue that a mental health app may not be the best alternative, given the reported negative association between mobile phone use and mental health in this population group. However, extensive global research confirms the potential for mHealth to address mental health challenges among young people, including students (Grist et al., 2017; Haeger et al., 2022; McCloud et al., 2020; Yilmaz & Bohara, 2021).
Despite the rise in mental health challenges and high mobile phone use among South African students, studies on the use of mHealth interventions for mental health challenges among this population group are limited (Borghouts et al., 2021). Therefore, there appears to be a need to explore the feasibility of a mental health app within the South African context.
Bowen et al. (2009) suggested that eight areas should be explored when determining the feasibility of an intervention: demand, acceptability, implementation, adaptation, integration, expansion, practicality, and efficacy testing. This study focused on three of the eight areas that determine feasibility—demand (the use or need of intervention by the target group), practicality (how the intervention can be delivered to the target population), and acceptability (reception of the intervention by users)—to understand the needs of students. The aim of this study was to explore the feasibility and acceptability of a mental health app intervention among university students. This study forms part of a larger one, with a broader focus on developing a mental health app for university students.
Methods
The researchers employed a convergent parallel mixed-methods research design. Quantitative and qualitative data were collected online through a survey and focus group discussions (FGDs) from March 2 to October 12, 2021. The online survey was developed and conducted on REDCap, a secure web-based application for developing and managing surveys. Online FGDs were conducted using either the Zoom or Google Meet platforms, depending on the participants’ preferences.
Setting
The study was conducted online during alert Levels 1 and 3 lockdowns of the COVID-19 pandemic, a period during which movement was restricted and social distancing mandatory to prevent transmission. Since there was minimal access to the university facilities and most students were studying online, our study was conducted online to avoid the spread of COVID-19.
Participants
Eligible participants were undergraduate and postgraduate university students between the ages of 18 and 24 and enrolled full-time at any South African university. The age criterion was based on literature showing that young people between the ages of 18 and 24 years have higher levels of psychological distress and are more inclined to use technology (Hakami, 2018; Moran, 2016). We used convenience sampling as a strategy to reach more students across South African universities (Bryman, 2016).
Recruitment procedures
A bulk e-mail with a link to the online survey was sent to 35,609 students. After completing the survey, participants were informed about the FGDs. Those interested in participating were sent a link that included the FGD dates and times, and they were asked to select a suitable date and time for their participation. Posters containing information about the study and links to the survey and FGD schedule were shared on the WhatsApp, Facebook, and Instagram social media platforms.
Data collection
Measures
The online survey collected the following sociodemographic data: age group, gender, level of study, faculty, citizenship, and geographical location. Data were collected on practicality and demand, both as measures of feasibility. For practicality, we assessed (a) smartphone ownership; (b) access to data or Wi-Fi; (c) previous use of health apps, which required a yes/no response; and (d) mobile phone software use, which required the selection of IOS, Android, or other category. For demand, we assessed (a) previous use of health apps and (b) history of mental health challenge diagnosis, both of which required a yes/no response.
Interview guide
A semi-structured FGD interview guide was used to collect data with the aim to explore students’ perceptions on the acceptability of a mental health app as an intervention. The questions in the interview guide included the following: What are your thoughts about using a mental health app to alleviate psychological distress? What could be the benefits or challenges of using a mobile app for mental health?
Ethics
The study was approved by the human research ethics committee (H21/01/23) of a university in the Gauteng province, South Africa. All study participants signed an online consent form by clicking on the ‘I agree to participate’ button before participation. Participants were informed that participation was voluntary, and they were allowed to end the survey at any time. FGD participants switched off their cameras and used pseudonyms to strengthen anonymity and confidentiality. A distress protocol was in place in case students experienced emotional distress.
Data analysis
Quantitative data were analysed using Statistical Analytics Software (SAS) version 9 by running descriptives and frequencies for both sociodemographic and feasibility data. Qualitative data were analysed using the six steps of thematic analysis as suggested by Braun and Clarke (2006): (a) data familiarisation, (b) generation of codes, (c) theme searching, (d) reviewing of themes, (e) defining of themes, and (f) data write-up.
Survey results
The survey reports on the sociodemographics of participants and the feasibility (practicality and demand) of a mental health app.
Sociodemographics
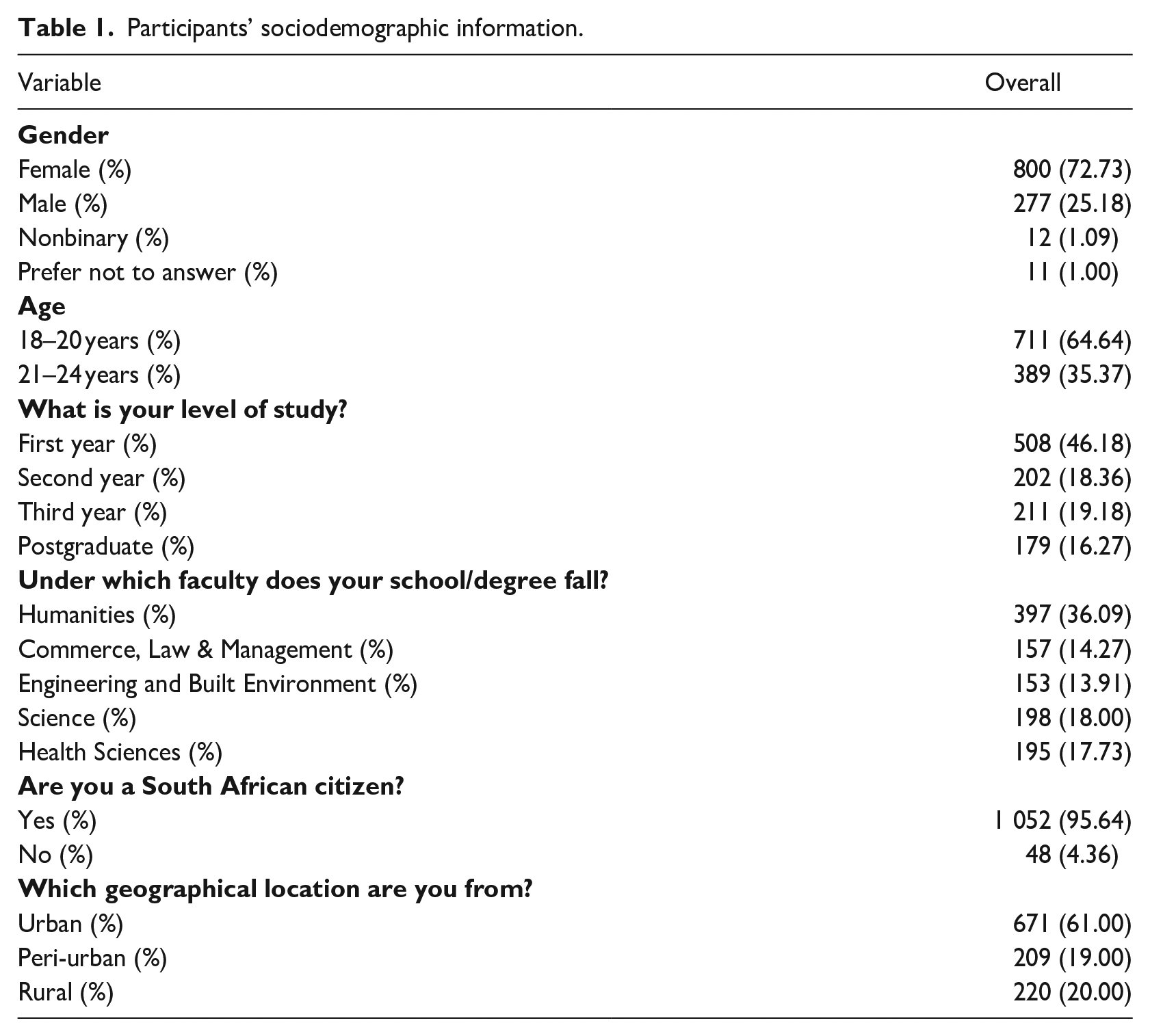
A total of 1100 students participated in the online survey. As illustrated in Table 1, 72.73% of the participants were female (n = 800), 64.64% were aged 18 to 20 years (n = 711), 46.18% were in their first year of study (n = 508), and 36.09% were enrolled in the humanities faculty (n = 397). A sizable proportion of participants (95.64%, n = 1052) were South African citizens from an urban location (61%, n = 671).
Participants’ sociodemographic information.
Feasibility (practicality and demand) of a mental health app
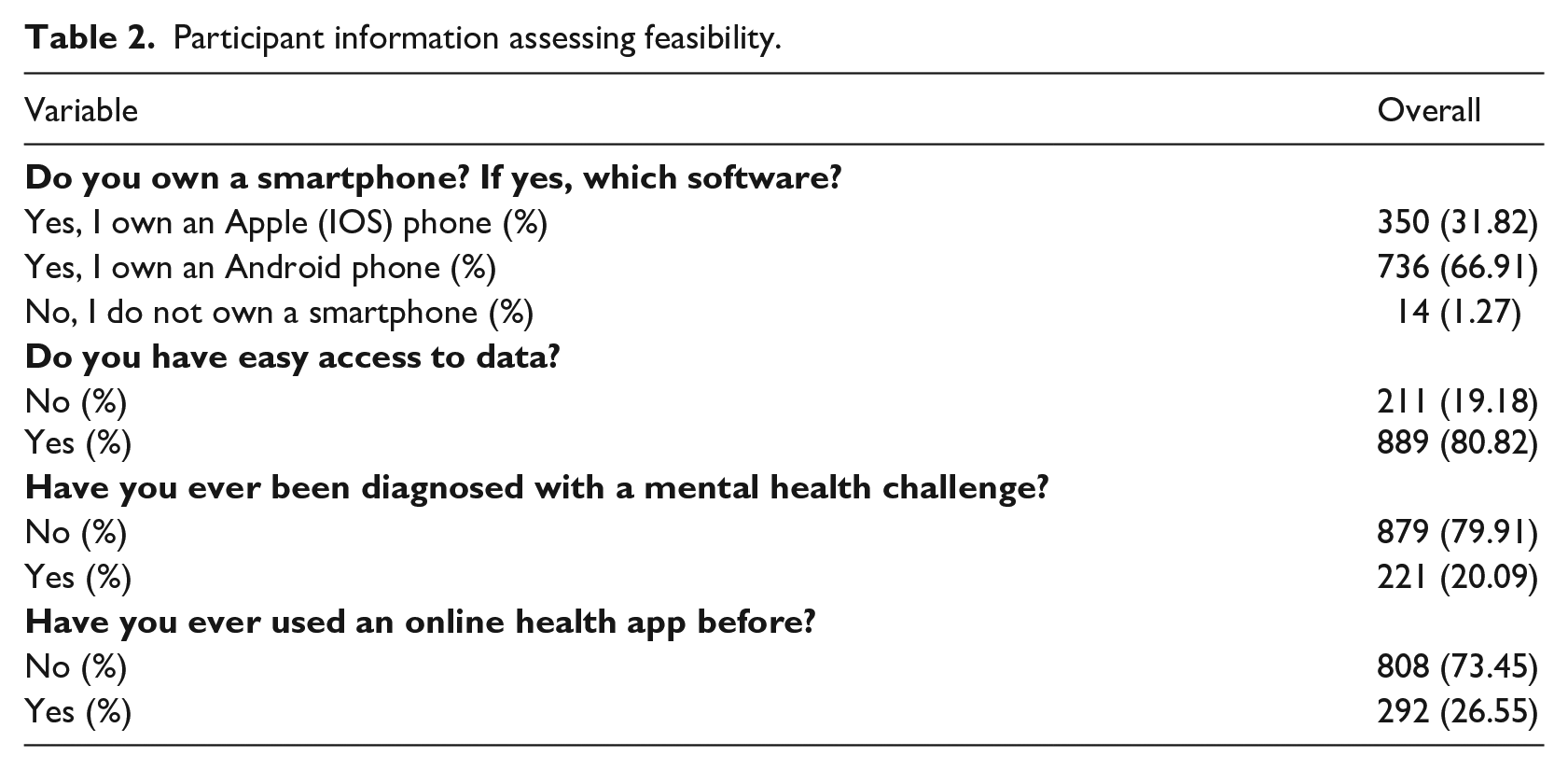
Table 2 shows that 98.73% of the participants (n = 1086) owned a smartphone, with 66.91% (n = 736) owning an Android smartphone. At 80.82% (n = 889), the vast majority had easy access to data. Around 20% of the participants (n = 221) had previously been diagnosed with a mental health challenge and 26.6% (n = 292) had used a health app for their health needs.
Participant information assessing feasibility.
Acceptability of a mental health app intervention
Sixty-two participants were enrolled in FGDs to explore the acceptability of a mental health app as an intervention for university students. Most FGD participants were female (n = 34), within the 21–24 age group (n = 37), and in their third year of study (n = 22).
Qualitative results
Theme 1: potential facilitators of the acceptability of a mental health app intervention
Thematic analysis revealed potential facilitators to the acceptability of a mental health app intervention as a main theme with four subthemes—exposure to mental health apps, convenience, accessibility, and confidentiality.
Exposure to mental health apps
Exposure to mental health apps facilitated the acceptance of a mental health app intervention. Some participants were already using meditation apps to alleviate feelings of anxiety or distress. Their existing exposure to meditation apps facilitated their potential acceptance of a mental health app intervention designed to address students’ mental health challenges. One participant shared, I have used a meditation app before to address some of my mental distress and I think that was way better. So, I guess a mental health app can work for me. (FGD, male, 22, third year)
Some participants were exposed to evidence-based mental health apps, which was a facilitator to their potential acceptance of a mental health app designed for university students in the future. However, one participant hinted that the app she used was American and did not fit the financial and social circumstances of South African university students. The participant further hinted that because of her experience with the mental health app, she would be willing to use an app that meets the needs of South African university students: The app I used before was honestly great, it was an American app, but it had limited free content and I needed to pay for premium content. I stopped using the app even though I needed the help. But my overall experience with this app was good and I think because of this experience I can use an app made for South African university students. (FGD1, female, 19, first year)
Convenience
Convenience was a major facilitator in the acceptance of a mental health app. Participants stated that an app would provide the help needed in the comfort of one’s own space. Convenience was discussed particularly in relation to students who were uncomfortable with seeking face-to-face counselling or those with social challenges. In these cases, a mental health app was seen as a potential alternative: I think it will be a good option for those who are not comfortable going in-person; it [an app] becomes an alternative for them. I think it is a good idea, it provides them help in the comfort of their own space. (FGD12, female, 20, third year)
Convenience was also discussed in terms of affordability. While acknowledging that an app could not replace in-person therapy in its entirety, some participants suggested that access to free support via the app would reduce the expense of seeing a therapist: If it’s going to work as a therapist, then we don’t have to wake up and use transport. The session will be in our own personal space. So, it’s going to work. (FGD11, male, 21, third year)
Accessibility
Most participants recognised that university students own smartphones, have access to the internet, and spend significant time on their phones, making a mental health app an easily accessible tool for university students: That is smart [mental health app idea] because most of us [students] are always on our phones. We can easily use the app since it would be on our phones. (FGD12, male, 21, third year) I think it would be a good idea because in today’s age, there are few people who do not have phones or internet access. (FGD5, male, 21, third year)
A simplified approach to help-seeking was also discussed as part of accessibility. Considering that few students seek mental health support on campus, some participants believed that an app would make help more accessible to students and would provide them with an opportunity to discuss their mental health challenges openly: I think an app would be extremely helpful, especially for those who are afraid but are not willing to see a therapist. (FGD5, male, 21, third year) So, I think it can work [mental health app]. It can increase the number of people opening [up] about their mental health. (FGD10, male, 21, third year)
Participants also discussed accessibility in terms of location and distance. One participant shared that an app may be useful for students who cannot easily access counsellors outside of the university because of location or distance. This could be particularly true in times when the university is in recess or for students who live in rural settings far from the university: It might work for people who do not have the access to a counsellor. So those people might download the app and might get help in some sense on what they are facing. So, people who are far away from the city or far away from getting help with the university counsellor. (FGD2, male, 20, second year)
Confidentiality
The confidentiality afforded by an app was a facilitator to using a mental health app. The participants in this study argued that students are generally apprehensive about sharing personal information with therapists based at university counselling centres. Because of this, students have put up barriers that prevent them from seeking help. Some participants, therefore, considered an app to be a tool that could be used to address mental health challenges without oversharing their personal information or experiences with a therapist: I would prefer having an app rather than having therapy in person or online. An app is not really a breach of my personal space and information privacy barriers that I put up. (FGD3, female, 19, second year)
The fear of judgement from therapists and the stigma associated with mental health challenges were identified as common barriers to help-seeking among university students. Participants shared that most students avoid face-to-face therapy because of the fear of judgement or having their personal challenges discussed with other therapists. Some participants shared that an app could address this challenge because it would offer them solutions to their problems without the risk of identification or having their personal information shared with other therapists: I would really go with the app because it solves the challenge of seeing a therapist, who might talk about you after. For as long as you can see a therapist, there is a discomfort of sharing issues with them. An app is easier; it is confidential, and it doesn’t know who you are. You just talk about your problems, and just get the solutions that you can get, and you are out. So, I totally agree with an app. (FGD10, male, 22, third year)
Confidentiality was also discussed in terms of anonymity. Student participants seemed to want to address their challenges anonymously. Most participants shared that using the app anonymously would address the stigma associated with seeking face-to-face mental health assistance: Even if there is a support group on campus, we are not going to go, even if it is helpful. We do not go because everyone is going to know our story; they are going to look at us differently or treat us different. So, if there is an app and it is anonymous, it would work perfectly. (FGD2, female, 22 third year)
Theme 2: potential barriers to the acceptability of a mental health app intervention
Thematic analysis revealed potential barriers to the acceptability of a mental health app intervention as the main theme with three subthemes, these being preference for face-to-face therapy, overreliance on the app, and fear of misdiagnosis.
Preference for face-to-face therapy
Some participants, particularly those who were already making use of counselling services, stated that they preferred face-to-face therapy over an app for their mental health needs. They shared that in face-to-face therapy, they can hold a conversation, get physical touch and mirroring of emotions, things that an app cannot do: Using an app will not be more effective like seeing a therapist face-to-face. I think, emotions get hidden when you are talking to someone over the phone[.] It is not the same as talking to someone face-to-face. Sometimes you just need a hug from the other person. (FGD6, female, 22, second year)
Overreliance on the app
The possibility of overrelying on an app for mental well-being was identified as a potential barrier to its acceptability. Some participants argued that apps, including a mental health app, could be problematic if an individual has poor time management, a mobile phone addiction, or spends more time than they should on their mobile phone: The only reservation I have is not being able to manage the mental health app properly in terms of time management. Everything is in your hands. If you are addicted to your phone or certain apps on your phone, how will you make sure that this new app that you are getting does not become a problem[?] (FGD1, male, 20, second year)
When discussing overreliance on an app, participants raised issues of ‘toxicity’ from apps. One participant remarked that she had experienced toxicity from certain apps, even the ones which have good elements, which could be a barrier to using a mental health app. She suggested that she would be interested in using an app that is designed to address her individual needs: I can get ‘toxic vibes’ from apps. You know all apps have their good and their bad and this could be a barrier for me to use this [mental health] app. So, an app that will help me as an individual is an app I’d like on my phone. (FGD3, female, 18, first year)
Fear of misdiagnosis
Most participants identified the fear of misdiagnosis as a potential barrier to using a mental health app. Participants argued that if the app is used as a diagnostics tool, it could make an incorrect diagnosis based on the selected symptoms, particularly for mental health challenges with similar symptoms, such as anxiety and depression: I think if we do have the app, it must work in a way that it does not give the wrong results. So instead of saying they have anxiety, it says they have depression. It must not give the wrong diagnoses. (FGD2, female, 22 third year)
Discussion
The overall results from this study suggest that a mobile-based intervention for university students can be a feasible and acceptable intervention to address mental health challenges. Quantitative results on the demand of a mental health app intervention showed that only one-third of participants had used a health app for their mental health and physical needs. This finding varies from findings of a study conducted in the United Kingdom, where 80% of the students had used a health app for their well-being (Payne et al., 2012). Another study conducted in Saudi Arabia showed that at least 56% of the students in that study had used a health app for their physical health (Jabour et al., 2021). The low usage of health apps among participants in our study compared with participants in high-income countries, such as the United Kingdom and Saudi Arabia, may suggest that many South African students might not have access to or knowledge of available health apps. In addition, the contradictory findings may suggest a shortage of health apps developed with South African students in mind.
The findings on mental health history show that at least one in five of the participants had been previously diagnosed with a mental health challenge. This finding is consistent with findings from other studies conducted among students at South African universities (Bantjes et al., 2019). Findings on high levels of mental health challenges from previous studies and this current study confirm that university students in South Africa are experiencing mental health challenges, which validates the need for an intervention designed to address their mental health needs.
Quantitative results on practicality show that an app could be a feasible intervention since almost all the students participating in the study owned a smartphone—almost two-thirds had Android smartphones, and the remaining one-third had IOS smartphones. This usage finding is contrary to findings from high-income countries such as Saudi Arabia and the United Kingdom, where most students were using IOS smartphones (Jabour et al., 2021). Given the differences in context, this finding suggests that Android mobile phone devices might be more accessible and affordable within the South African student population compared with IOS mobile phone devices. The finding of high Android smartphone ownership can be a guide to developers in the South African context to focus on Android-based app interventions for the student target market. In our broader study, of which this mixed-method study was a subset, we used these findings to develop a prototype app on Android. However, we acknowledge that developers who prioritise both Android- and IOS-based interventions stand to reach more students and increase usefulness.
Most students in this study had easy access to data or Wi-Fi. As expected, this finding reveals that students would be able to access a mobile-based intervention, as global studies also show that students spend a considerable proportion of their time on their mobile phones (Ataş & Çelik, 2019; Masiu & Chukwuere, 2018). However, given the economic disparity in South Africa, this finding may only be applicable to students enrolled at urban universities who constituted the majority participants in this study. A study conducted by Reddy Moonasamy and Naidoo (2022) found that 57% of students enrolled at rural universities were concerned about the cost of internet access for their online learning sessions during the COVID-19 pandemic. This finding may be an indicator of data or internet access challenges among university students enrolled at rural universities.
Previous exposure to mental health apps was also identified as a facilitator to the acceptability of the proposed mental health app. Some students have previously used apps as a self-help tool for their mental health care needs. Compared with university students in the United States and the United Kingdom, students in this study seem to be more exposed to meditation apps than evidence-based mental health apps, highlighting a potential gap in mental health apps that offer a variety of evidence-based interventions for South African university students (Haeger et al., 2022; McCloud et al., 2020).
The students in this study discussed comfort and affordability as two factors of convenience and identified these as important aspects of an app’s acceptability. Similarly, other feasibility studies have discussed ease of access and affordability as being crucial to mobile intervention acceptance (Ardi et al., 2018; Cliffe et al., 2022). Interestingly, in this study, easy access to an app was found to be a potential bridge between students and therapists, especially for those who have reservations about seeing a therapist. An app was perceived as a tool that could gradually help users recognise the benefits of seeking mental health assistance from a therapist.
Confidentiality, particularly aspects of privacy and anonymity, was also an important theme. Similarly, global research shows anonymity and confidentiality are two key motivators for young people to use mental health apps (Oliveira et al., 2021; Zhou et al., 2019). In contrast, confidentiality breaches such as third-party access to information and complicated privacy policies are shown to be major concerns among mental health app users globally (Koh et al., 2022; Wies et al., 2021). The participants in this study hardly discussed privacy policies in relation to using an app, highlighting a need for more in-depth discussion on this topic. This is particularly important for the South African context in which measures such as the Protection of Personal Information Act (POPIA) are in place to protect individual privacy. Future app developers and users should prioritise having discussions on personal information safety before developing or adopting mental health apps.
A preference for face-to-face therapy because of its ability to offer human connection is a barrier to the acceptance of an app. This finding reveals the inadvisability of replacing a mental health specialist with an app, particularly for those who have critical mental health challenges. This shortcoming of a mental health app does not diminish its potential effectiveness but suggests that mental health app interventions introduced to university students could function as a resource to be used alongside face-to-face therapy and not a replacement for therapy (Borghouts et al., 2021; Koh et al., 2022).
Overreliance on a mental health app was identified as a potential barrier to mental health app acceptance. This finding is pertinent given the increase in smartphone addiction, which is associated with mental health challenges such as depression and anxiety (Lei et al., 2020; Liu et al., 2022). This finding calls for developers to exercise caution and not overuse enabling features that may require users to be constantly online or overreliant on the intervention. Instead, an app should function as a tool that provides the necessary support when needed (Borghouts et al., 2021; Koh et al., 2022).
Fear of misdiagnosis was also identified as a potential barrier to the acceptance of a mental health app. Research has suggested that digital tools are more likely to misdiagnose mental health challenges in users because the diagnostic criteria often overlook subjective experiences (Yan et al., 2022). Conversely, other research has shown a high digital accuracy rate in diagnosing mental health challenges such as mood disorders, eating disorders, and behaviour challenges (Grist et al., 2017; Yilmaz & Bohara, 2021). As the debate around the accuracy of diagnosis using digital tools continues, the finding of this study suggests that an app intervention should be designed in a manner that avoids diagnosing or psychopathologising users. Instead, it should give users an opportunity to reflect on their own experiences or feelings by using nonclinical self-report scales while encouraging them to consult with a mental health professional for a diagnosis.
Strengths and limitations
This study contributes to the current conversation on the role of technology in the field of psychology. The findings of this study add to the knowledge gap on student mental health and the use of mHealth interventions in South Africa. The findings of this study suggest that a mental health app can be a feasible intervention for university students. However, this study is limited as it only reports on the feasibility and practicality of and demand for mHealth interventions and not the processes of developing a mental health app or evaluating the effectiveness of mHealth interventions. Future studies can work towards developing and evaluating mental health app interventions for university students.
In addition, this study focused on a single mHealth intervention and did not explore other digital interventions, such as artificial intelligence. Future studies can explore whether other digital interventions can effectively contribute to mental health and well-being of university students within the South African context. This study also does not explore the social and economic vulnerabilities of disadvantaged student populations, which should be a major consideration for future mHealth interventions. Another major limitation of the study is the sampling strategy; while convenience sampling provided easy access to participants, most of the participants were from a single university; therefore, the findings of this study cannot be generalised to all South African university students.
Conclusion
The study indicates previous exposure to mental health apps, convenience, accessibility, and confidentiality as potential facilitators of acceptability. Preference for face-to-face therapy, overreliance on the app, and fear of misdiagnosis are potential barriers to acceptability. The study highlights the need and feasibility of mHealth mental health interventions for university students. This preliminary study addresses a knowledge gap by offering mHealth software developers and members of the psychology community information on how to engage the mental health of university students in a practical and feasible manner. Accessible mHealth mental health interventions have the potential to reduce the mental health burden and the inequality gap in accessing mental health care to an extent.
Footnotes
Acknowledgements
The authors acknowledge Dr. Mamakiri Mulaudzi for contributing to qualitative data analysis, and the Africa Unit for Transdisciplinary Health Research and Prof. Lusilda Schutte for general support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The PhD study was funded by the National Reserach Foundation (MND200415513713) and the Ithemba Foundation. The study was partially supported through Janan Dietrich’s South African Medical Research Council (SAMRC) funding through its Division of Research Capacity Development (under the Early Career Investigators Programme) from funding received from the South African National Treasury.