
Abstract
Due to the widespread occurrence of mental disorders among adolescents, there is globally a recognised need to assess the mental well-being of higher education students. Those in extended programmes, dealing with self-esteem and capability challenges intensified by peer and institutional attitudes, might face heightened susceptibility to mental health issues. Moreover, research suggests that the 2020 COVID-19 pandemic likely worsened students’ mental health difficulties. This study aimed to assess the prevalence of mental health issues among students in a South African university’s extended curriculum programme in 2022 while exploring potential gender differences. Furthermore, by comparing these findings to a 2017 study, it sought to assess the COVID-19 pandemic’s potential impact on the mental health of extended programme students. Paper-based questionnaires evaluated depression, anxiety, and stress symptoms among first-year extended programme students in 2017 (pre-COVID, n = 208) and in 2022 (within the pandemic, post-lockdown, n = 202). The results showed consistently high levels of mental health issues for both cohorts, with no statistically significant difference between the cohorts. However, female students in the 2022 cohort faced notably more mental health challenges than their male peers. Universities should enhance mental health education and awareness campaigns and explore new counselling methods to assist the growing number of students in need of support. Further research ought to investigate the factors behind the heightened mental health issues, especially among female students.
The World Health Organisation (WHO) defines mental health as more than the absence of mental disorders. It is about being mentally well, enabling individuals to handle life’s challenges, utilise their abilities effectively, and contribute to society. Mental health is essential for decision-making, relationships, and shaping our world. According to WHO, it is a fundamental human right crucial for personal, community, and socio-economic development (WHO 2022c, Concepts in mental health section).
Mental disorders, like depression, bipolar disorder, and anxiety disorder, impact mental health. In 2019, approximately 280 million people had depression, 40 million had bipolar disorder, and 301 million had anxiety disorders globally. Sadly, many lack access to effective prevention and treatment (WHO, 2022b). Adolescents also face mental health challenges, with one in seven individuals aged 10–19 years experiencing mental disorders. Depression, anxiety, and behavioural disorders are the primary causes of illness in this age group, and among older adolescents, suicide ranks as the fourth leading cause of death (WHO, 2022a).
Higher education institutions globally recognise the necessity to ensure the mental health of their students, who typically fall within the late adolescence or early adulthood stage (Cvetkovski et al., 2019; Larcombe et al., 2016; Naylor, 2022; Ward et al., 2022). The WHO’s World Mental Health International College Student (WMH-ICS) initiative, launched in 2012, aimed to identify prevalent mental disorders and students in need of treatment; implement interventions for at-risk students, and determine the provision of treatment or preventive services to a large body of students (Auerbach et al., 2018; Cuijpers et al., 2019). Surveys conducted at 19 tertiary institutions across eight countries, including South Africa, revealed that approximately one-third of first-year students displayed at least one common Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) anxiety, mood, or substance disorder, with the average age of onset occurring in early to middle adolescence, and with major depression disorder being the most prevalent (Auerbach et al., 2018). These findings are also reflected in other studies (Larcombe et al., 2016; Li et al., 2022; Naylor, 2022; Ward et al., 2022). South African researchers in the WMH-ICS initiative (see Bantjes et al., 2021; Bantjes et al., 2023; Auerbach et al., 2018) have contributed significantly to the knowledge on the state of mental health among South African university students. Independent studies on this topic include work by Eloff and Graham (2020), Meintjes (2020), and Wagner et al. (2022).
The COVID-19 pandemic may have contributed to poor mental health among students, as global studies show increased anxiety and major depression disorders (WHO, 2022b). With the outbreak of the COVID-19 pandemic, tertiary education institutions worldwide had to switch to online teaching and assessments (Evans et al., 2021; Lee et al., 2021; Le Vigouroux et al., 2021; Werner et al., 2021; Wieczorek et al., 2021). In South Africa, conventional academic activities were suspended, and online platforms were adopted, with limited campus access granted (Republic of South Africa, 2020; Van Schalkwyk, 2021). Various studies (Chen & Lucock, 2022; Di Consiglio et al., 2021; Evans et al., 2021; Halperin et al., 2021; Le Vigouroux et al., 2021; Wieczorek et al., 2021; Zimmermann et al., 2021) have explored the pandemic’s impact on students’ mental health, revealing increased psychopathological symptoms, especially among female students (Chen & Lucock, 2022; Di Consiglio et al., 2021; Werner et al., 2021). However, limited research has focussed on the later stages of the pandemic.
First, this study aimed to assess mental health issues among first-year students enrolled in a South African university’s extended curriculum programme in 2022. These programmes cater to students who, despite obtaining a National Senior Certificate that allows for university entrance, did not fulfil all mainstream programme admission criteria. Such students often grapple with self-worth and ability questions, exacerbated by peer and institutional attitudes in higher education (Council on Higher Education, 2013).
Second, the study sought to compare the 2022 findings with a 2017 study (Meintjes, 2020), aiming to shed light on how the COVID-19 pandemic may have enhanced mental health challenges among extended programme students. The 2017 study primarily focussed on depression and self-regulated learning and the possible effect of these constructs on students’ academic performance, and also touched on anxiety and stress.
Finally, acknowledging prior research indicating higher mental health issues among females (Auerbach et al., 2018; Bantjes et al., 2023; Li et al., 2022; Liu et al., 2022; Seehuus et al., 2021), the third aim was to determine whether depression, anxiety, and stress prevalence were higher in female students compared to male students.
Methods
Participants
In 2017 and 2022, all first-time registered students in the science faculty’s extended curriculum programme at a South African university were invited to participate. In 2017, 208 students (78% of 266 eligible) voluntarily participated, while in 2022, 202 students (87% of 232 eligible) willingly took part in the study.
Instruments
In both the 2017 pre-COVID and 2022 post-lockdown COVID-19 studies, the short version of the Depression, Anxiety and Stress Scales (DASS-21) (Lovibond & Lovibond, 1995; Psychology Foundation of Australia, 2022) was used. The DASS-21 is not a substitute for individual diagnostic psychological assessments, but effectively measures depression, anxiety, and stress levels in normal populations quantitatively (Henry & Crawford, 2005). It comprises 21 Likert-type self-report items, with seven items for each scale (depression, anxiety, and stress), taking about 10 min to complete. The sum of item scores on each scale is categorised as normal, mild, moderate, severe, or extremely severe. The DASS-21 demonstrates solid psychometric qualities, including good internal consistency (Cronbach’s alpha > .70), construct validity, and reliability (Cohen et al., 2007; Henry & Crawford, 2005; Sinclair et al., 2012; Weiss et al., 2015). In both the 2017 and 2022 studies, Cronbach’s alpha values for the DASS-21 questionnaire scales exceeded .7, affirming reliability in a South African context. Depression, anxiety, and stress showed high consistency with Cronbach’s alpha values in 2017 at .856, .770, and .765, respectively, and in 2022 at .860, .784 and .802.
Procedure
The pre-COVID cohort completed the DASS-21 questionnaire from 27 to 30 March 2017, while the post-lockdown cohort completed it from 11 to 13 April 2022. For both cohorts, this period aligned with the seventh week of academic activities, during which no major assessments were scheduled.
Ethical considerations
Permission from the University of the Free State’s general/human research ethics committee (UFS-HSD2016/1064; UFS-HSD2021/2082/22) was secured for both the 2017 pre-COVID and 2022 post-lockdown studies. All participants, aged 18 or above, were fully informed about the research and volunteered to take part. Measures were taken to ensure their confidentiality and privacy. Recognising that some participants may have been facing mental health challenges, a contact list of support structures was provided.
Data analysis
Data analyses utilised IBM Statistical Package for Social Sciences (SPSS) software. Scores for each DASS Questionnaire (DASS-21) scale were calculated and doubled, facilitating comparison with Lovibond and Lovibond’s (1995) categorisation in the full DASS-42 Questionnaire. Henry and Crawford (2005) found comparable outcomes between doubled DASS-21 scale scores (averaging 5.66 for depression, 3.76 for anxiety, and 9.46 for stress) and DASS-42 scores (averaging 5.55 for depression, 3.56 for anxiety, and 9.27 for stress). This suggests the suitability of DASS-21 scores for comparative use. The DASS developer’s website (http://www2.psy.unsw.edu.au/groups/dass/) also recommends doubling DASS-21 scores for comparison with the DASS-42 categorisation. Subsequently, levels of depression, anxiety, and stress were categorised as normal, mild, moderate, severe, or extremely severe based on the groupings in Table 1.
Standard and adjusted DASS-42 questionnaire categorisations.
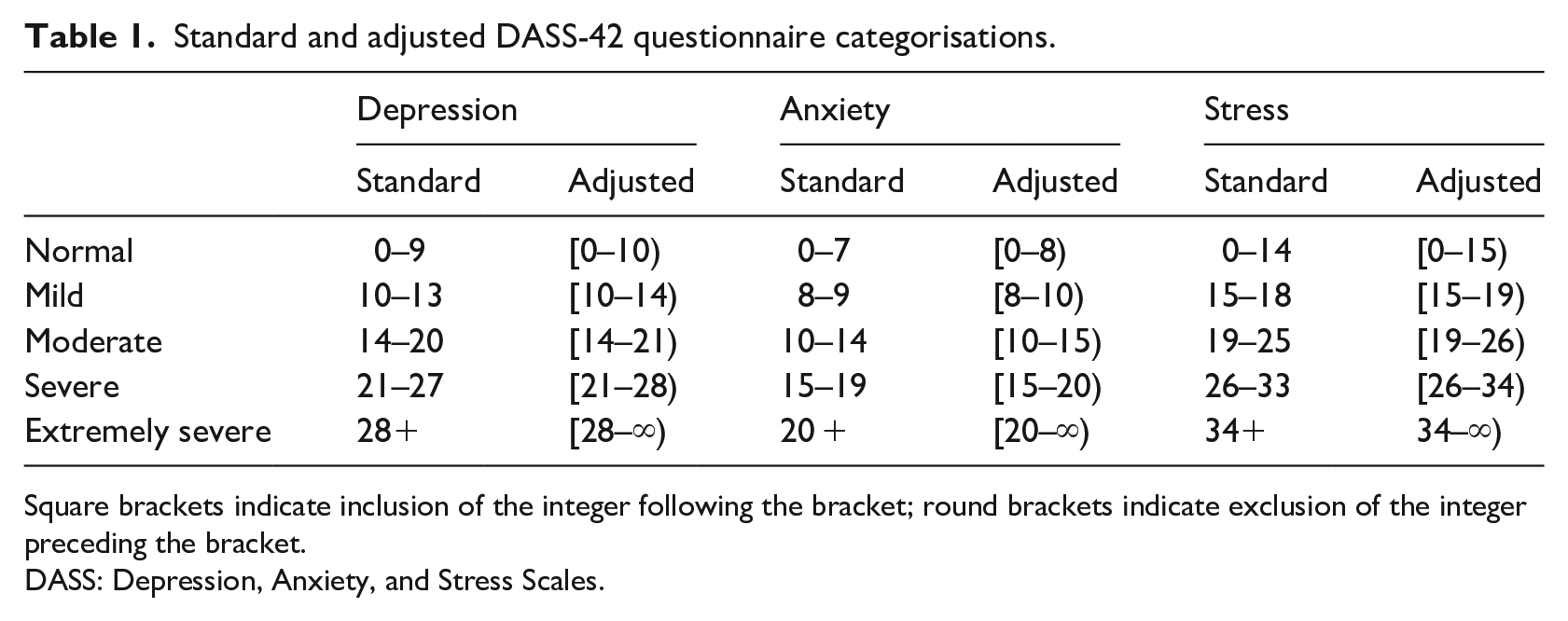
Square brackets indicate inclusion of the integer following the bracket; round brackets indicate exclusion of the integer preceding the bracket.
DASS: Depression, Anxiety, and Stress Scales.
Newman’s Mean Across Available Item(s) Approach (Newman, 2014) was used to calculate scores if participants did not answer all items on a scale. In 2017, the response rate was 78%, with a full response rate of 72% and a partial response rate of 6%. In 2022, the response rate was 87%, with a full response rate of 80% and a partial response rate of 7%. However, employing this approach led to issues, as some participants’ scores fell between categories (e.g., 13.2 for depression). To address this, adjustments were made to the subscales, as detailed in Table 1.
Pearson correlations were computed on DASS questionnaire scores for each cohort. Independent samples t-tests assessed differences in depression, anxiety, and stress levels across cohorts, genders within each cohort, men across cohorts, and women across cohorts. One participant in the 2022 cohort identified as ‘other’ and was subsequently not included in the statistical analysis to simplify the process.
Results
The average age of participants in both cohorts was 18.7 years. There was a higher participation of women (57.7 % in 2017 and 65.7% in 2022) than men. Table 2 displays descriptive analyses of DASS questionnaire scale categories for both cohorts.
Descriptive analyses of the DASS questionnaire scale categories per cohort.
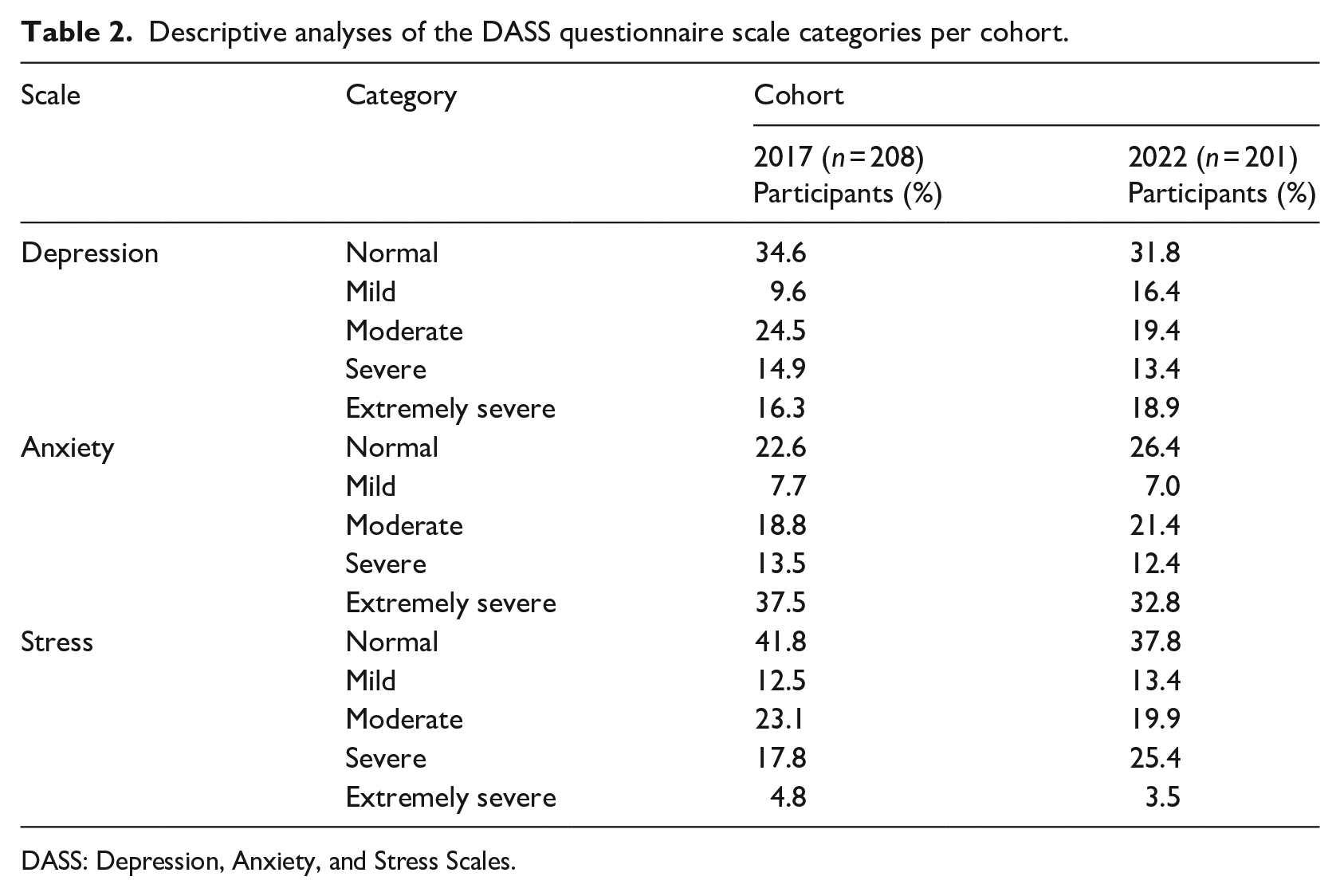
DASS: Depression, Anxiety, and Stress Scales.
Roughly two-thirds of participants in both cohorts displayed symptoms of depression, ranging from mild to extremely severe, with nearly a third falling into the severe and extremely severe categories. Severe and extremely severe anxiety affected 51.0% (2017) and 45.2% (2022) of the participants, while stress in the severe and extremely severe categories affected 28.9% (2022) and 22.6% (2017) of participants.
Table 3 shows Pearson’s correlation coefficients for the DASS questionnaire, revealing strong, significant positive correlations between depression and anxiety, depression and stress, and stress and anxiety within both cohorts. The levels of depression, anxiety, and stress for both cohorts were also analysed by gender. These results are represented in Table 4.
Pearson correlation coefficients for the DASS questionnaire scales.
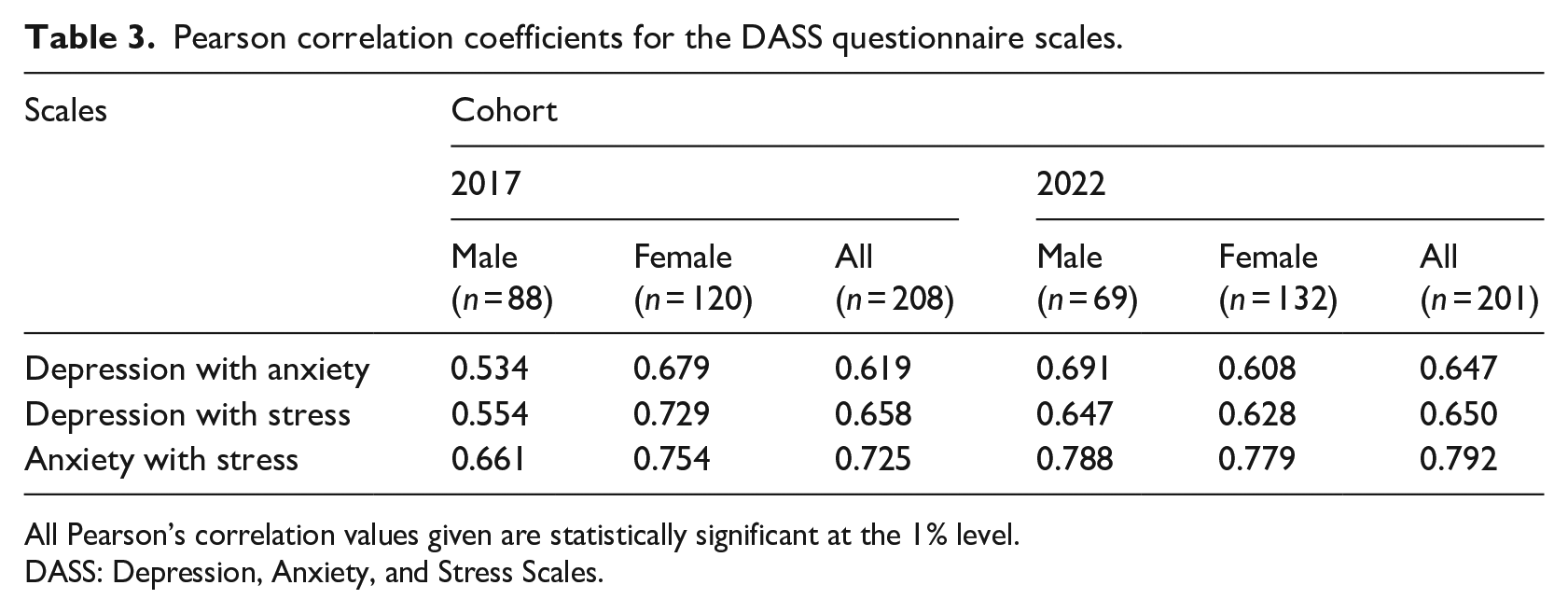
All Pearson’s correlation values given are statistically significant at the 1% level.
DASS: Depression, Anxiety, and Stress Scales.
Comparison of the DASS categories according to gender.
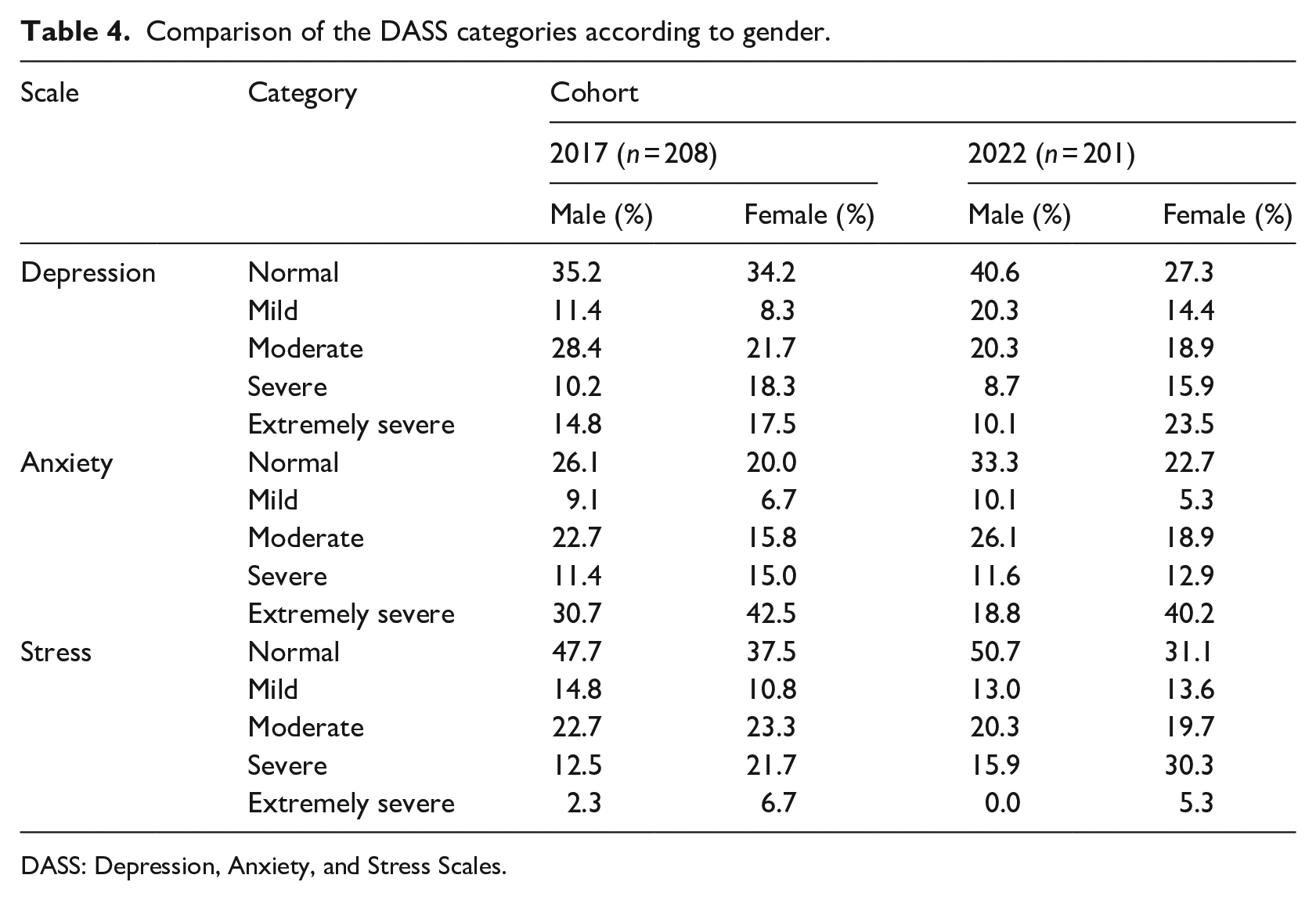
DASS: Depression, Anxiety, and Stress Scales.
In the 2017 cohort, severe to extremely severe depression affected a higher percentage of females (35.8%) than males (25.0%). This gender difference was more pronounced in 2022, with 39.4% of females falling in these categories for depression, compared to only 18.8% of males. For anxiety in 2017, 57.5% of females and 42.1% of males were in the severe to extremely severe categories, while in 2022, 53.1% of females and 30.4% fell into these categories. Stress levels were consistently higher among females in both cohorts. In 2017, 28.4% of females and 14.8% of males were in the severe to extremely severe stress categories. In 2022, 35.6% of females and 5.9% of males were in the severe to extremely severe stress categories.
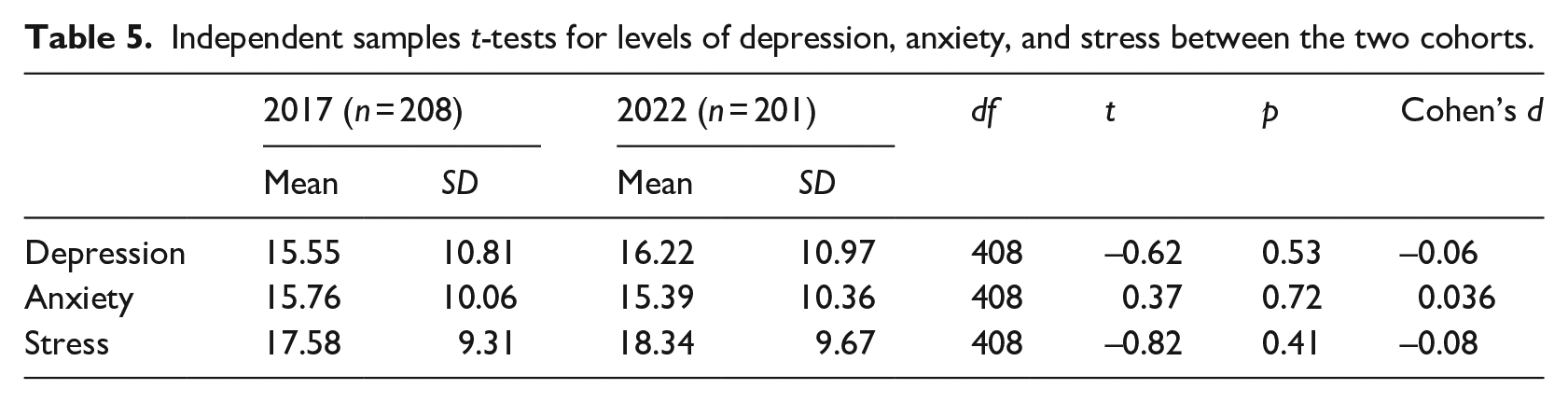
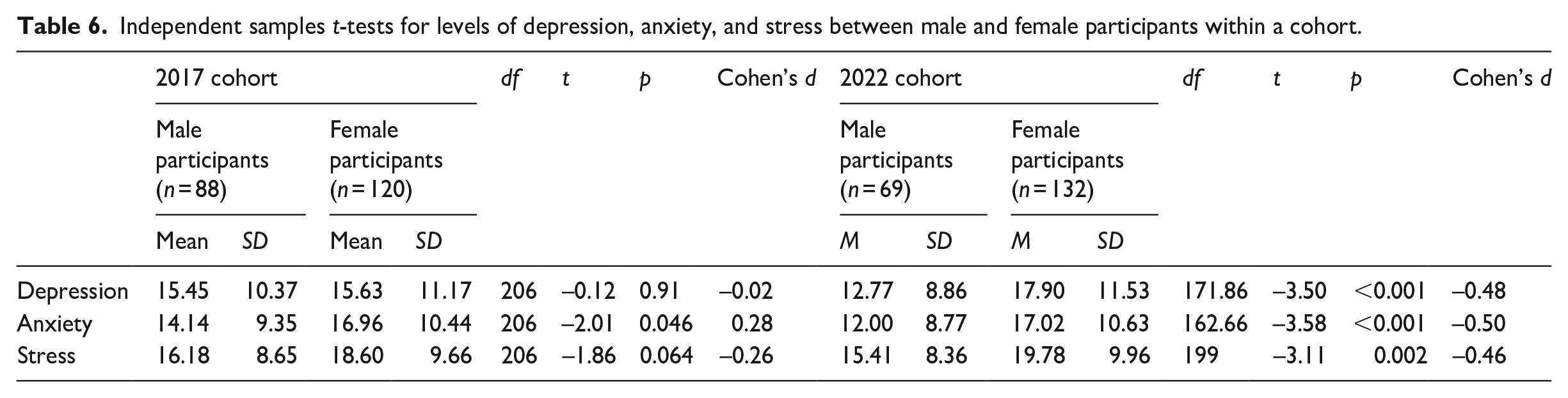
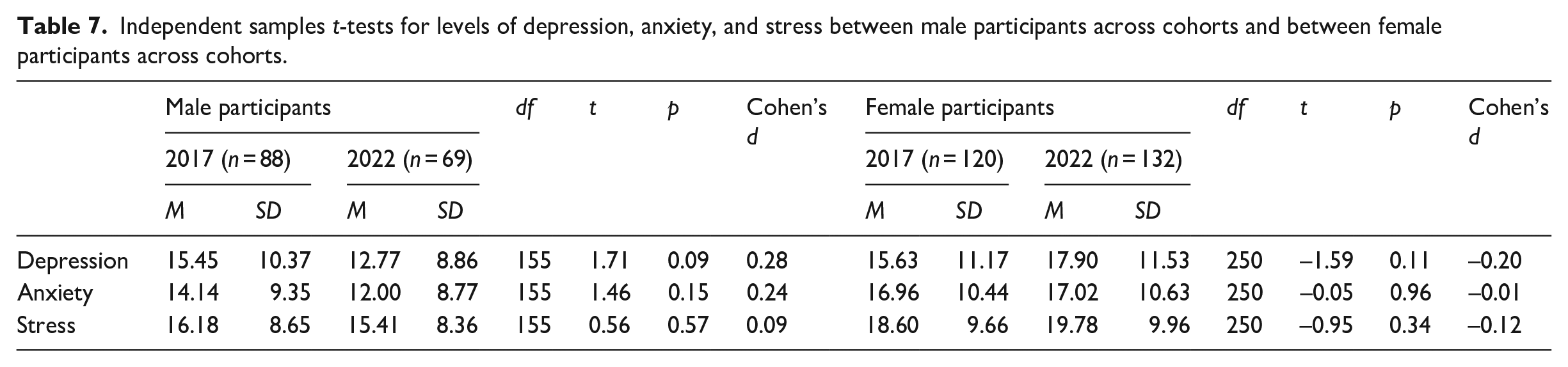
Independent samples t-tests compared depression, anxiety, and stress levels across cohorts (Table 5), genders within each cohort (Table 6), and male participants across cohorts (Table 7), as well as female participants across cohorts (Table 7). The only statistically significant difference emerged between genders within each cohort. In the 2017 cohort, females showed significantly higher anxiety levels than males, while in 2022, females displayed significantly higher levels of depression, anxiety, and stress than males.
Independent samples t-tests for levels of depression, anxiety, and stress between the two cohorts.
Independent samples t-tests for levels of depression, anxiety, and stress between male and female participants within a cohort.
Independent samples t-tests for levels of depression, anxiety, and stress between male participants across cohorts and between female participants across cohorts.
To control for Type 1 error across multiple tests in Tables 5 to 7, the Benjamini–Hochberg (BH) correction method (Benjamini & Hochberg, 1995) was applied. This involved ordering p-values, assigning ranks, and comparing each p-value to its critical value, calculated as (i/m)Q, with i as the rank, m as the total number of tests, and Q set at a 0.05 false discovery rate in this study. Any p-value smaller than (i/m)Q was considered significant. The results are outlined in Table 8.
Benjamini–Hochberg correction for multiple hypothesis testing.
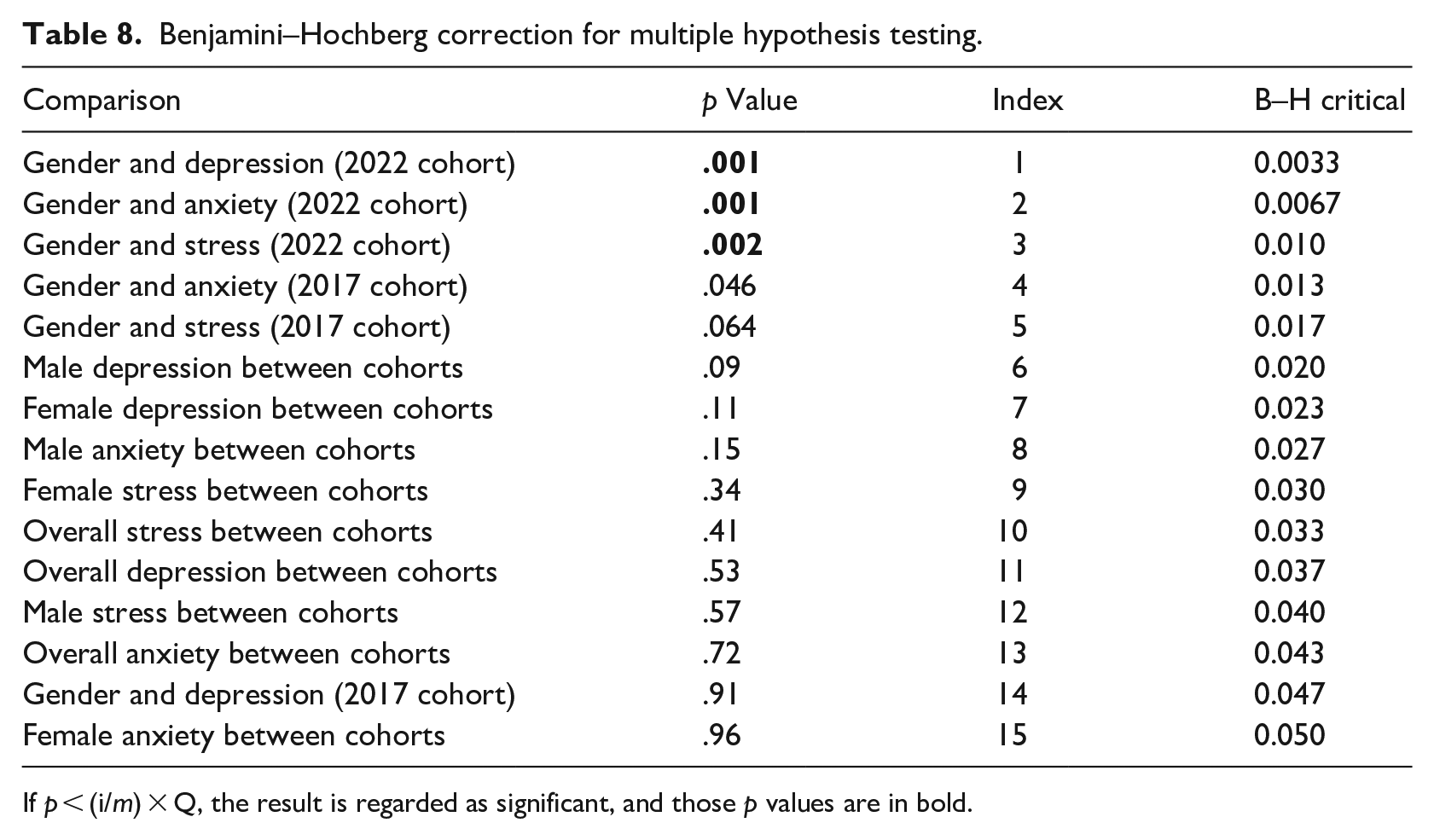
If p < (i/m) × Q, the result is regarded as significant, and those p values are in bold.
After applying the Benjamini–Hochberg correction, the higher levels of depression, anxiety, and stress exhibited by the female participants of the 2022 cohort remained significant when compared to male participants. However, the higher levels of anxiety exhibited by the female participants in the 2017 cohort compared to the male participants, became nonsignificant.
Discussion
This study aimed to assess mental health issues among first-year students enrolled in a South African university’s extended curriculum programme in 2022 while exploring potential gender differences. Furthermore, by comparing these findings to a 2017 study, it sought to assess the COVID-19 pandemic’s potential impact on the mental health of extended programme students.
The average depression levels were slightly higher in the 2022 cohort (M = 16.22, SD = 10.97) compared to the 2017 cohort (M = 15.55, SD = 10.81). This difference was not statistically significant, t(408) = –0.62, p = .53. Severe and extremely severe depression symptoms were present in about one-third of both cohorts (31.2% for 2017 and 32.3% for 2022). These depression symptom levels are high compared to most other studies; however, comparisons are challenging due to differences in measurement instruments and the specific focus on extended programme students. Seehuus et al. (2021) found 12.29% prevalence of severe and extremely severe depression symptoms in American college students using the DASS-21 questionnaire. Wagner et al. (2022) reported a 10% prevalence of severe depression symptoms in first-year undergraduates at a South African university using the Patient Health Questionnaire-9. Bantjes et al. (2023) found a 15.4% prevalence of recent major depressive episodes among undergraduate students at 17 South African public universities using the Composite International Diagnostic Interview Screening Scales. Naylor (2022), using the DASS-21, noted higher psychological distress in students with low tertiary entrance scores. Within this group, 34.0% experienced severe or extremely severe depression symptoms, akin to the findings in this study.
The depression rates of the 2017 female participants were slightly higher (M = 15.63, SD = 11.17) than the 2017 male participants (M = 15.45, SD = 10.37), but this was not statistically significant, t(206) = –0.12, p = .91. In the 2022 cohort, the gender difference was significant, t(171.86) = –3.50, p < .001, with females (M = 17.90, SD = 11.53) exhibiting higher depression rates than males (M = 12.77, SD = 8.86). Other studies (Bantjes et al., 2023; Seehuus et al., 2021; Ward et al., 2022) also found higher depression rates in females compared to males. There were no statistically significant differences between male participants’ overall depression scores in 2017 (M = 15.45, SD = 10.37) and 2022 (M = 12.77, SD = 8.86) cohorts, t(155) = 1.71, p = .09, nor between females in the 2017 (M = 15.63, SD = 11.17) and 2022 (M = 17.90, SD = 11.53) cohorts, t(250) = –1.59, p = .11.
In 2017, anxiety levels were slightly higher (M = 15.76, SD = 10.06) than in 2022 (M = 15.39, SD = 10.36) but this difference was not significant, t(408) = –0.37, p = .72. Severe and extremely severe anxiety affected 51.0% of the 2017 cohort, and 45.2% of the 2022 cohort. This study found higher severe and extremely severe anxiety levels compared to many others. For instance, Seehuus et al. (2021) found 13.67% prevalence of severe and extremely severe anxiety symptoms among American college students. Wagner et al. (2022) reported 18% prevalence of severe anxiety symptoms, and Bantjes et al. (2023) found 10.9% prevalence of recent (past 30 days) generalised anxiety disorder. Naylor (2022) observed 47.9% severe anxiety symptoms among students with low tertiary entrance scores, aligning closely with this study’s findings.
In the 2017 cohort, there was a statistically significant difference, t(206) = –2.01, p = .046, in anxiety scores between female (M = 16.96, SD = 10.44) and male participants (M = 14.14, SD = 9.35). However, after applying the Benjamini–Hochberg correction, this difference became nonsignificant. In the 2022 cohort, a significant gender difference was observed, t(162.66) = –3.58, p < .001, with females (M = 17.02, SD = 10.63) reporting higher anxiety scores than males (M = 12.00, SD = 8.77). Similar findings were reported in other studies (Bantjes et al., 2023; Seehuus et al., 2021) indicating a higher incidence of anxiety symptoms among females compared to males. There were no statistically significant differences in overall anxiety scores between male participants in the 2017 and 2022 cohorts, t(155) = 1.46, p = .15, nor between female participants in the 2017 and 2022 cohorts, t(250) = –0.05, p = .96.
The 2022 participants, on average, had higher levels of stress (M = 18.34, SD = 9.67) compared to the 2017 participants (M = 17.58, SD = 9.31), however, this difference was not significant, t(408) = –0.82, p = .41. Severe and extremely severe stress levels affected 22.6% of the 2017 cohort and 28.9% of the 2022 cohort, resembling Naylor’s (2022) findings that 24.5% of students with low tertiary entrance scores experienced severe or extremely severe stress symptoms. The 2022 cohort exhibited a significant gender difference, t(199) = –3.11, p = .002, in the overall incidence of stress, with females (M = 19.78, SD = 9.96) reporting a higher incidence of stress than males (M = 15.41, SD = 8.36), though no significant differences were found in the overall incidence of stress between female (M = 18.60, SD = 9.66) and male (M = 16.18, SD = 8.65) participants in the 2017 cohort, t(206) = –1.86, p = .064. There were no significant differences between the overall stress scores of male participants in 2017 and 2022, t(155) = 0.56, p = .57, nor between female participants in 2017 and 2022, t(250) = –0.95, p = .34.
The correlation coefficients of both the cohorts were significantly positive between depression, anxiety, and stress. Thus, participants who presented with one of the three mental health symptoms most likely also presented with at least another one.
This study did not find evidence suggesting that the 2022 cohort faced more mental health challenges compared to the 2017 cohort. This suggests that the pandemic might not have worsened mental health issues for extended programme students, contrary to earlier pandemic-related studies (Chen & Lucock, 2022; Di Consiglio et al., 2021; Evans et al., 2021; Halperin et al., 2021; Le Vigouroux et al., 2021; Wieczorek et al., 2021; Zimmermann et al., 2021). Notably, many previous studies were conducted shortly after the pandemic’s start during strict lockdown measures, unlike this study, conducted more than 2 years after the initial outbreak when restrictions had eased. This return to pre-COVID levels of mental health problems after the relaxation of strict lockdown measures was also observed by Di Consiglio et al. (2021), highlighting the resilience of students who completed their secondary education amid challenging lockdown circumstances.
While the current study did not explore factors beyond gender for the prevalent mental health issues among university students, other research indicates various other contributors. Various studies (Larcombe et al., 2016; Li et al., 2022; Liu et al., 2022) propose that lifestyle, academic year, social media usage, belonging to ethnic or sexual minorities, and lower family socio-economic status contribute to increased mental distress among students. The elevated levels of depression and anxiety observed among extended programme students, often entering university with lower admission scores, align with Naylor’s (2022) findings for individuals with low tertiary entrance scores. Naylor suggests that these students may feel unprepared and overwhelmed at the start of their studies, potentially contributing to their increased psychological distress.
Conclusion
In both the pre-COVID (2017) and post-lockdown (2022) cohorts, high levels of depression, anxiety, and stress was prevalent. In both cohorts, more females than males presented with severe and extremely severe symptoms of depression, anxiety, and stress. The institution should prioritise enhancing mental health education and awareness campaigns, employing well-researched strategies for optimal impact. Considering the scale of the problem, innovative therapy approaches may be necessary due to potential funding challenges for traditional individual therapy sessions. Further research is needed to investigate factors contributing to heightened mental health problems, especially among female students.
This study was conducted at a single tertiary institution in South Africa and focussed on a specific group of students within one faculty. Therefore, the findings cannot be generalised. In addition, the possibility exists that participants may not have been entirely truthful in the self-report questionnaires, especially when sensitive questions were involved. Furthermore, data collection for both cohorts was confined to 1 week in the academic calendar, which might have yielded different results if conducted at another time of year.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.