
Abstract
Numerous studies have been conducted among survivors of the genocide against the Tutsi on the prevalence of depression and post-traumatic stress disorder. However, thus far, no studies provide information on the frequency of comorbidity of these disorders, the prevalence of the new trauma-related diagnostic disorder known as complex post-traumatic stress disorder, and the role of social determinants, such as age, sex, marital status, employment category, education, and location, in the occurrence of these disorders. The present study was conducted to address these gaps. Genocide survivors (N = 261 participants; M = 46.30, SD = 11.95, females = 52.9%) took part in the study. They completed the International Trauma Questionnaire, the Public Health Depression Questionnaire, and the Harvard Trauma Questionnaire. Descriptive statistical analyses, bivariate analyses with two-tailed chi-square tests, and logistic regression were used to determine the prevalence of the above-mentioned disorders, comorbidity, and the associations between the social determinants and the assessed psychopathologies. Of the total sample, 47.1% presented with at least one of the assessed probable mental health disorders: 15.3% (n = 40) met the criteria for probable post-traumatic stress disorder, 15.3% (n = 40) for probable complex post-traumatic stress disorder, and 38.7% (n = 101) for probable depression. Of the participants with probable post-traumatic stress disorder and complex post-traumatic stress disorder, nearly half met the criteria for probable depression. Being married but not living with the partner was associated with probable complex post-traumatic stress disorder, and unemployment was associated with probable depression. Our findings suggest to clinicians and policymakers that they should consider comorbidity and social determinants in their interventions.
Introduction
In April 1994, systematically organized massacres of the Tutsi took place in Rwanda over a period of 3 months (Des Forges, 1999). It is estimated that at least 1 million Tutsi were killed, and many individuals were injured, sexually abused, or rendered homeless (Kayiteshonga et al., 2022). In addition to the traumatic experiences during the genocide, survivors continued to be affected by psychosocial consequences during the post-genocide period, such as by widowhood, poverty, and unemployment (Kayiteshonga et al., 2022).
Considering the traumatic experiences during the genocide and the related post-genocide adversities, it is unsurprising that many affected individuals experienced a high level of suffering and historical trauma (Mutuyimana & Maercker, 2022). This is also reflected in the prevalence of about 30% for probable post-traumatic stress disorder (PTSD) and about 40% for probable depression (e.g., Bahati et al., 2022; Mutuyimana et al., 2019, 2021). While recent studies suggest that PTSD and depression are the most common mental health disorders in the aftermath of trauma, up to this day, the proportion of survivors who are not affected by these disorders is still unknown. Genocide survivors were subjected to persistent and repetitive events that posed an extreme threat to their lives (Pham et al., 2004). This kind of exposure might be the source of the development of complex post-traumatic stress disorder (CPTSD) (ICD-11; World Health Organization, 2019).
No studies could be found that have studied the caseness of CPTSD among survivors of the genocide in Rwanda.
Existing literature indicates that PTSD and CPTSD are usually comorbid with depression (e.g., Flory & Yehuda, 2015; Spikol et al., 2022). While there are studies that have shown high prevalence rates of PTSD and depression among genocide survivors (e.g., Kayiteshonga et al., 2022; Mutuyimana et al., 2021), these studies have not assessed the rate of comorbidity. However, this is important because it is known that recognizing the comorbidity of diseases contributes to better treatment of these disorders and effectively improves patients’ health status (Valderas et al., 2009).
Furthermore, the comorbidity and prevalence of mental health disorders can be amplified by social determinants (Barr et al., 2022; Shim & Compton, 2020). This evidence of associations between social determinants, such as gender, age, education, employment status, and income, and various mental health disorders (e.g., PTSD, depression) has been found in studies around the world (e.g., Kessler & Bromet, 2013; Koenen et al., 2017). So far, only one study of the Rwandan population 14 years after the genocide found that being between 25 and 34 years of age, living in extreme poverty, having experienced the death of a close relative in 1994, being widowed or remarried, having suffered the loss of both parents, and living in Southern Province were associated with PTSD (Munyandamutsa et al., 2012).
However, the latter study did not specifically focus on genocide survivors, and it did not consider other mental health disorders such as depression and CPTSD. Therefore, the present study aimed to explore the caseness of (complex) PTSD, the comorbidity rates of (complex) PTSD and depression, as well as the role of social determinants (i.e., age, sex, age during genocide, marital status, employment category, and place of residence) in the occurrence of these disorders.
CPTSD versus PTSD ICD-11
According to International Classification of Diseases, 11th Revision (ICD-11), PTSD may develop following exposure to an extremely threatening or horrific event or series of events. It is characterized by three main symptoms, namely, re-experiencing the traumatic event or events in the present in the form of vivid intrusive memories, flashbacks, or nightmares; avoidance of thoughts and memories of the event or events, or avoidance of activities, situations, or people reminiscent of the event(s); and persistent perceptions of heightened current threat. A diagnosis of PTSD is made when the symptoms persist for at least several weeks and cause significant impairment in personal, family, social, educational, occupational, or other important areas of functioning.
CPTSD differs from PTSD mainly in two ways: the nature of traumatic event(s) and diagnostic features. CPTSD is a disorder that may develop following exposure to an event or series of events of an extremely threatening or horrific nature, most often prolonged or repetitive events from which escape is difficult or impossible (e.g., torture, slavery, genocide campaigns, prolonged domestic violence, repeated childhood sexual or physical abuse) (ICD-11; World Health Organization, 2019). The diagnostic criteria include all PTSD symptoms in association with three disturbances in self-organization (DSO) clusters: (1) affective dysregulation, (2) negative self-concept, and (3) disturbances in relationships and functional impairment must be identified (Cloitre et al., 2018; Maercker et al., 2022). A person cannot be diagnosed simultaneously with PTSD and CPTSD.
CPTSD versus borderline personality disorder
CPTSD and borderline personality disorder (BPD) share some common symptoms. Despite this, scientists maintain that the two conditions are different from one another, with overlapping yet distinct symptom profiles (Maercker et al., 2022). In the case of CPTSD, the three DSO clusters also parallel BPD features (Ford & Courtois, 2021). However, the specific DSO symptoms are relatively distinct from BPD symptoms.
CPTSD is characterized by the avoidance of close relationship while for BPD people have difficulty sustaining relationships. Regarding self-identity, individuals with CPTSD tend to have a more stable sense of self but struggle with consistent feelings of low self-worth, guilt, and shame while individuals with BPD, on the other hand, have a more unstable sense of self—they may not know who they are at their core and frequently change their interests.
Regarding emotional regulation, individuals with CPTSD often over-regulate emotions, using emotional numbing or withdrawing, to cope with reminders of traumatic experiences. On the contrary, BPD is characterized by under-regulation of intense emotions, resulting in expressions of intense anger or self-harm (Ford & Courtois, 2021; Maercker et al., 2022).
Methods
Participants
The sample of the study consisted of survivors of genocide against Tutsi in Rwanda with the ability to read and complete a written questionnaire. Individuals who recently experienced traumatic events were excluded from the study. The sample size was determined using the G-power rule for regression analysis.
Instruments
Social determinants
The variables of a newly developed brief demographic questionnaire were age, gender, education, marital status, employment category, religion, and place of residency.
PTSD and CPTSD stress disorder
To assess CPTSD, the International Trauma Questionnaire (ITQ; Cloitre et al., 2018) was used. The ITQ is based on the ICD-11 criteria for PTSD and CPTSD. It is composed of two subscales that assess PTSD and CPTSD with a total of 18 items.
Responses are rated on a 5-point Likert-type scale, ranging from 0 (not at all) to 4 (extremely). The total score can range from 0 to 72, whereas subscale scores range from 0 to 36. The cut-off of more than 2 for one of two symptoms of each cluster needs to be fulfilled for probable PTSD. For estimating CPTSD prevalence (henceforth referred to as ‘probable’ because it is based on self-reported symptoms), one of two symptoms from each of the three PTSD symptom clusters and one of two symptoms from each of the three DSO clusters must be present (Cloitre et al., 2018). In the present sample, Cronbach’s alpha for the total score was .93.
Depression symptoms
The nine-item Patient Health Questionnaire (PHQ-9) was used to assess depression symptoms (Kroenke et al., 2001). The measure corresponds with the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) depression criteria (American Psychiatric Association, 1994), with items rated on a scale of 0 (not at all) to 3 (almost every day). Score categories are 0–4 for no depression, 5–9 for mild depression, 10–14 for moderate depression, 15–19 for moderately severe depression, and 20–27 for severe depression (Kroenke et al., 2001). In the present study, Cronbach’s alpha for the PHQ-9 was .87.
Traumatic exposure
The first part of the Harvard Trauma Questionnaire (HTQ; Mollica et al., 1992) was used to assess the traumatic events experienced. Here, individuals were asked to indicate (i.e., “yes” or “no”) whether they had experienced a particular traumatic event (e.g., rape, torture, or lack of shelter).
To assess the particular traumatic experiences within the context of the Rwandan genocide, Part 1 of the HTQ questionnaire had been extended with 20 additional traumatic experiences (e.g., being forced to physically harm a family member and being forced to bury bodies). The final checklist of traumatic events was composed of 37 dichotomous questions and 1 additional open question (“Can you think another situation that was very frightening to you?”). This instrument was chosen because its items were easy to adapt to the experience of genocide survivors and it was previously used with Rwandans (see Mutuyimana & Maercker, 2022). In this study, it shows a high reliability, as the Kuder–Richardson 20 score was .92.
Procedures
Recruitment took place between December 2020 and March 2021. Prior to the data collection, all instruments were translated and back-translated into and from Kinyarwanda by two different bilingual expert panels. Data were collected by a team of four local clinical psychologists with expertise in the field recruitment of study participants. Individuals were approached by data collectors in their households.
The latter explained the purpose of the study to them and asked them to participate. Those who agreed to participate filled out the questionnaires either at home or in a nearby office of local leaders, depending on the participants’ privacy preferences. Approximately 10% of the participants completed the questionnaires online.
Ethical considerations
Ethics approval was obtained from the University of Rwanda’s Institutional Review Board, College of Medicine and Health Sciences (No. 72/CHMS/IRB/2021). Written informed consent was obtained from the respondents before the interview.
Data analysis
The data were analyzed using the IBM SPSS Statistics version 28. Prior to the analysis, the relevant assumptions of the statistical analysis were checked. Based on the exploration of missing values and outliers, we deleted 20 cases of online data which had more than 10% of missing data. The field data were found to have no missing values as data collectors checked the completeness of the questionnaire before the departure of the participant. No other outliers were detected. A visual inspection of the scatter plots of the residuals showed that the normality assumption was met.
The data met the assumption of an independent error distribution (Durbin–Watson value = 1.73), and the statistical collinearity test revealed no multicollinearity of the independent variables, as the values for tolerance (Tolerance < 0.25) and the variance inflation factor (VIF) (VIF ⩽ 2.5) were within accepted limits (Johnston et al., 2018).
A descriptive statistical analysis was performed to determine the socio-demographic characteristics of the participants, caseness, and comorbidity of the disorders. Bivariate analyses of the association between social determinants and psychopathologies were performed with two-sided chi-square tests.
At this stage, participants were divided into two groups: those who met the criteria of at least one of the screened diagnostic categories were designated as the clinical sample and assigned a code of one (1), whereas those not fulfilling the diagnostic criteria of any of the psychopathologies under consideration were designated as symptom-free and assigned a code of zero (0). Logistic regression was used to examine the relationship between each of the assessed probable mental health disorders and the investigated social determinants. The order in the hierarchical regression analysis was as follows: trauma exposure was included in Block 1, and social determinants were included in Block 2 (in the same block but in a stepwise fashion). This order was chosen so that the net effect of the control variable in the explained variance could be evaluated prior to the additional effect of the predictor variables of interest (Johnston et al., 2018).
Results
Demographic characteristics of the participants
The total sample consisted of 261 participants, of which 52.9% (n = 138) were female. Approximately half of the sample (50.6%, n = 132) lived in the city of Kigali and 49.4% (n = 129) in rural Rwanda.
The mean age of the participants at the time of the study was 46.30 years (SD = 11.95). A total of 41.3% of the sample (n = 108) reported that they had been between 5 and 12 years old at the time of the genocide, 31.4% (n = 82) had been between 13 and 25 years old, 23.7% (n = 62) had been between 26 and 44 years old, and 3.4% (n = 9) had been between 45 and 60 years old.
Most participants (59.8%) were married at the time of the study assessment, 18.0% were widowed, 17.2% were single, and 5.0% were separated or divorced. Of the 261 participants, 41.0% (n = 107) were employed, 22.2% (n = 58) were self-employed, and 36.8% (n = 96) were unemployed. A total of 23.4% of the sample (n = 61) had no formal education, 22.6% (n = 59) reported having completed primary school, 19.5% (n = 51) had attended secondary school, and 34.5% (n = 90) had completed a university education.
Most participants (93.5%) self-identified as Christians (n = 244), whereas 3.8% (n = 10) self-identified as Muslims and 2.7% (n = 7) indicated that they had no religious affiliation.
Caseness and comorbidity of the assessed probable mental health disorders
Of the total sample, 15.3% (n = 40) met the screening criteria for probable PTSD, and 62.5% (n = 25) of those also met the screening criteria for probable depression. Of the total sample, 15.3% (n = 40) met the screening criteria for probable CPTSD, and 85% (n = 34) of those additionally met the screening criteria for probable depression. Of the total sample, 38.7% (n = 101) met the screening criteria for probable depression. More than half of the sample (52.9%) did not meet the criteria for any of the assessed probable mental health disorders (see Table 1).
Caseness of psychopathologies and comorbidity.
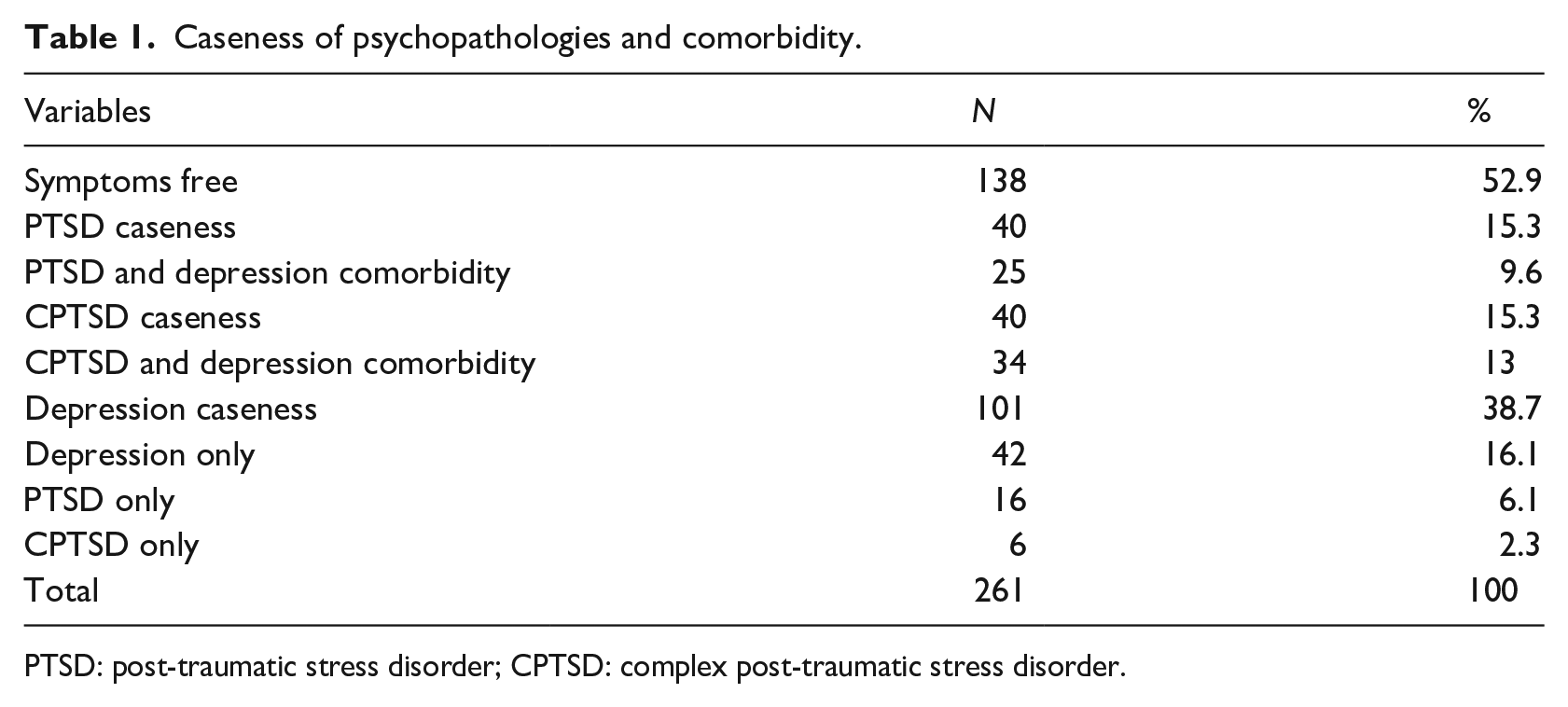
PTSD: post-traumatic stress disorder; CPTSD: complex post-traumatic stress disorder.
Bivariate associations between the social determinants and diagnostic categories (clinical sample vs symptoms-free sample)
Table 2 shows the results of the chi-square test. Employment, χ2 (1, N = 261) = 25.74, p < .001, age, χ2 (2, N = 261) = 14.85, p < .001, marital status, χ2 (2, N = 261) = 22.09, p < .001, and place of residence, χ2 (1, N = 261) = 5.21, p < .05 were significantly associated with the assessed probable mental health disorders.
Bivariate associations between social variables and psychopathologies (clinical sample vs symptoms-free sample).
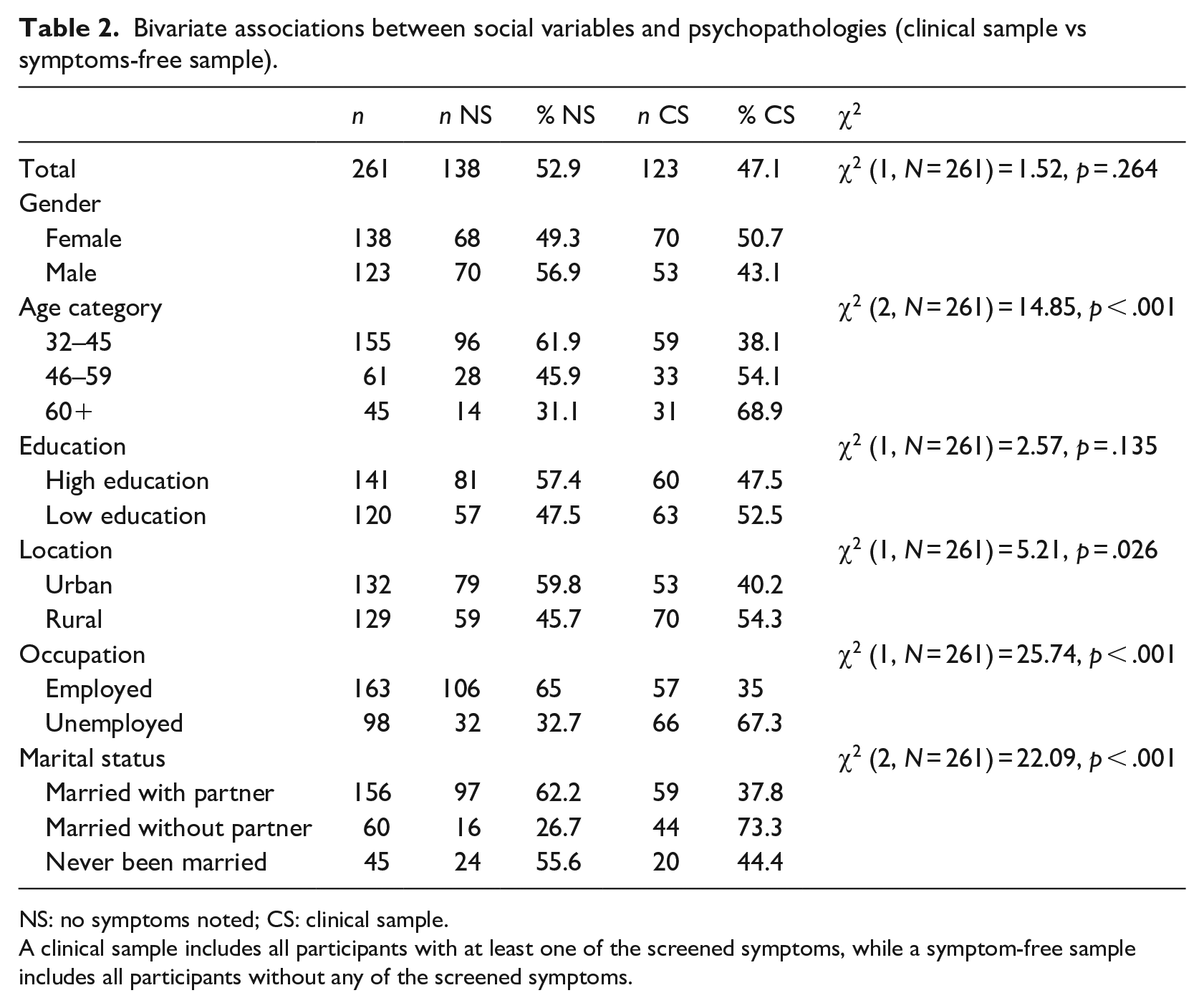
NS: no symptoms noted; CS: clinical sample.
A clinical sample includes all participants with at least one of the screened symptoms, while a symptom-free sample includes all participants without any of the screened symptoms.
Association between PTSD, CPTSD, depression, and social determinants
Logistic regression shows that of all the social determinants included in the model, only unemployment was associated with depression when controlling for the effect of traumatic exposure. Unemployed participants were three times more likely to report symptoms of depression than employed participants.
The model had a good fit and was statistically significant, χ2(1, N = 261) = 19.49, p < .001. It explained 25% (Nagelkerke R2) of the variance in depression and correctly classified 73.6% of cases (see Table 3).
Logistic regression of model fit for social determinants and depression.
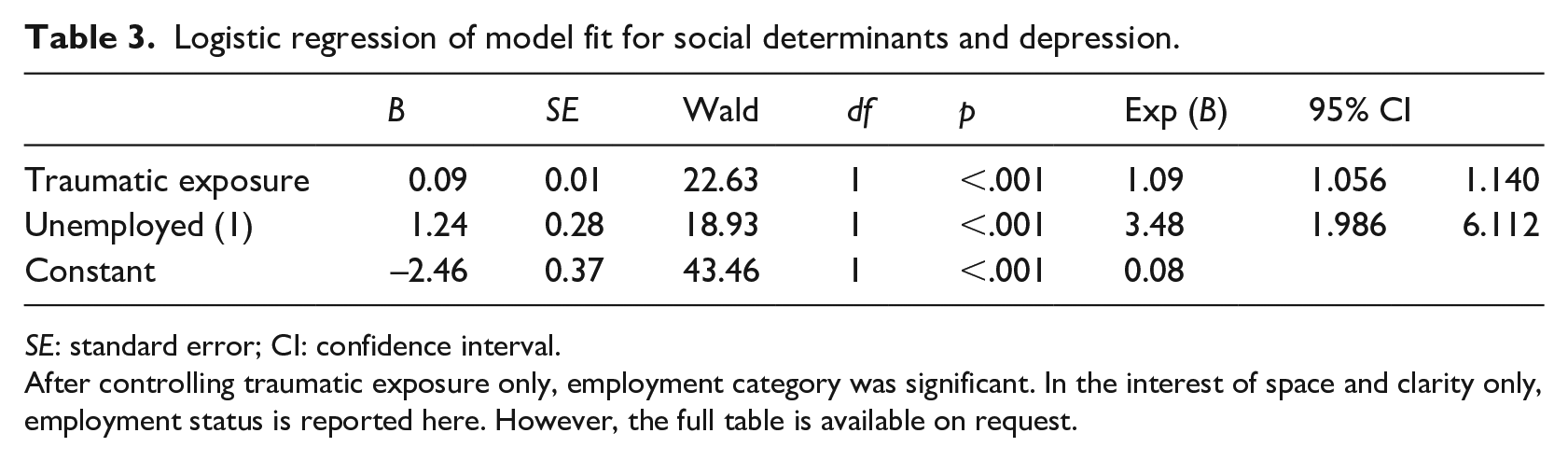
SE: standard error; CI: confidence interval.
After controlling traumatic exposure only, employment category was significant. In the interest of space and clarity only, employment status is reported here. However, the full table is available on request.
Table 4 shows that when controlling for the effect of trauma exposure, only marital status was significantly associated with PTSD symptoms. Married participants who did not live with their partners (i.e., those who were widowed, separated, or divorced) were four times more likely to report PTSD symptoms than married participants who lived with their partner. The model explained 20% (Nagelkerke R2) of the variance in depression and correctly classified 75.9% of cases. However, the model did not fit the data because the test of model fit was significant p < .05.
Logistic regression of model fit for social determinants and PTSD.
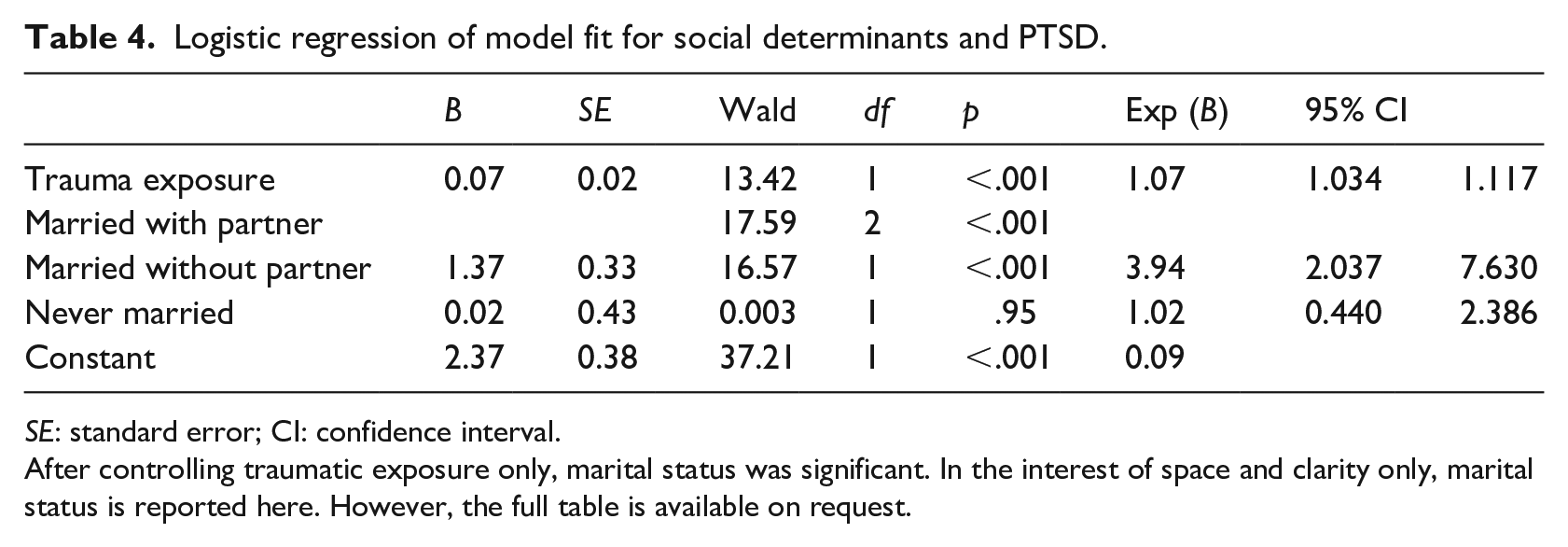
SE: standard error; CI: confidence interval.
After controlling traumatic exposure only, marital status was significant. In the interest of space and clarity only, marital status is reported here. However, the full table is available on request.
Table 5 shows that unemployed participants were almost three times more likely to have symptoms of CPTSD. Participants who were married but not living with their partners were almost four times more likely to have symptoms of CPTSD than participants who were married and living with their partner. The model had a good fit and was statistically significant, χ2 (1, N = 261) = 5.85, p < .001. It explained 30% (Nagelkerke R2) of the variance in CPTSD symptoms and correctly classified 85.1% of the cases.
Logistic regression of model fit for social determinants and CPTSD.
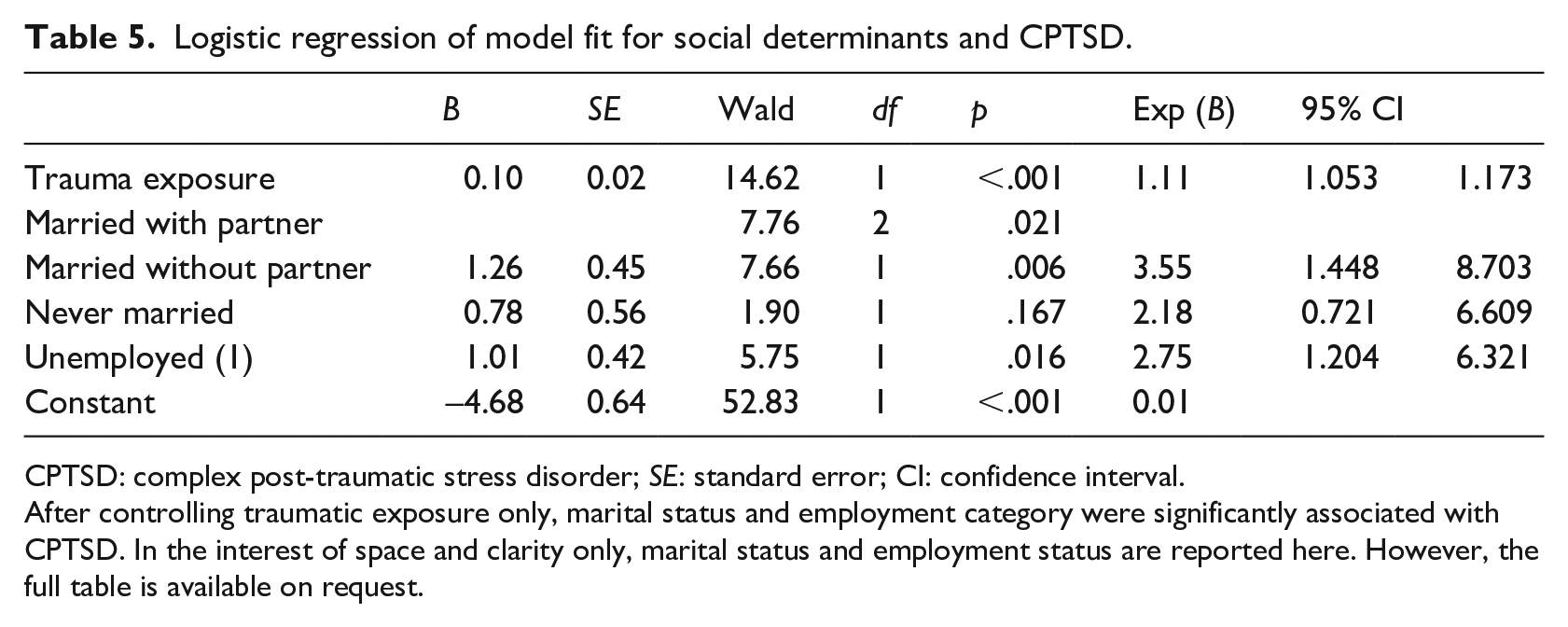
CPTSD: complex post-traumatic stress disorder; SE: standard error; CI: confidence interval.
After controlling traumatic exposure only, marital status and employment category were significantly associated with CPTSD. In the interest of space and clarity only, marital status and employment status are reported here. However, the full table is available on request.
Discussion
The aim of this study was to explore the caseness of probable CPTSD, the comorbidity rates of PTSD and CPTSD with depression, as well as the role of social determinants in the occurrence of these disorders.
The results indicated that the caseness of probable PTSD, CPTSD, and depression was comparatively high in this sample of genocide survivors. Depression was found to be a comorbid disorder in both PTSD and CPTSD. These findings are consistent with the literature on the prevalence of trauma-related disorders and their comorbid disorders in a sample that had experienced traumatic exposures (e.g., Maercker et al., 2022; Spikol et al., 2022).
Previous studies have already shown that PTSD and CPTSD occur as responses to traumatic life events and that their prevalence was high both in the general population and in clinical samples (e.g., Maercker et al., 2022; Spikol et al., 2022). In addition, it has been shown by different studies that approximately half of the individuals affected by PTSD and CPTSD are also diagnosed with a depressive disorder (Flory & Yehuda, 2015; Karatzias et al., 2019). Flory and Yehuda (2015) provided two explanations for such a comorbidity: first, the comorbidity may reflect overlapping symptoms. People with both disorders show greater social, occupational, and cognitive impairment. Second, the co-occurrence may represent a trauma-related phenotype, possibly a subtype of PTSD.
Therefore, diagnosing only one disorder may lead to a misdiagnosis and as such, the potential for inappropriate treatment (Maercker et al., 2022; Spikol et al., 2022).
Previous studies conducted with Rwandan samples have indicated a high prevalence of mental health disorders associated with trauma exposure, particularly genocide, including PTSD and depression (Bahati et al., 2022; Mutuyimana et al., 2021). The notable contribution of this study is the caseness of probable CPTSD in genocide survivors, the comorbidity rate, as well as the percentage of people who do not meet any criteria of probable screened disorders. This study has shown that depression is a comorbid disorder of PTSD and CPTSD.
More than half of the participants did not meet the criteria for the psychopathologies screened, which is in line with research showing that not all people affected by conflict develop a mental disorder (Charlson et al., 2019).
This study further examined the association of social determinants with depression, probable PTSD, and CPTSD. The results indicate that employment, age, marital status, and place of residence are significantly associated with at least one of the probable psychopathologies screened. More precisely, the results show that unemployment and being married but not living with the partner is associated with probable CPTSD while unemployment is associated with depression. None of the social determinants were significantly associated with PTSD.
Importantly, the correlational data do not allow for drawing conclusions on causality. Based on the current literature, the association between social determinants, CPTSD, and depression is most likely a two-way interaction. On one hand, social determinants contribute to psychopathology through structural mechanisms of power and stratification. Being unemployed and/or unmarried may exacerbate symptoms of stress, as important resources (e.g., having a fulfilling task, a steady income, or a caring partner) are lacking, but also due to the lower social status associated with being an unemployed or an unmarried person. In addition, having a mental disorder is a social category that by itself may lead to social exclusion.
Evidence from around the world shows that people with mental disorders suffer from discrimination in “what matters most” in their life, that is, marriage, employment, or social connection (Yang et al., 2014). On the other hand, symptoms of CPTSD and depression may hinder attempts to find employment or being in a relationship in the first place.
The study has the following limitations: this is a cross-sectional study, and therefore, no causal conclusions can be drawn. As the sample was a convenience sample, the results do not represent all genocide survivors in Rwanda.
It is also likely that individuals who suffer from severe mental health disorders were less likely to participate in the study. The instruments employed were self-report questionnaires that are subject to bias. Therefore, longitudinal studies using clinical interviews with large clinical and broader population samples are required for subsequent studies to confirm the results of their. Furthermore, as CPTSD and BPD are overlapping concepts, future studies are needed to explore the prevalence and comorbidity of these disorders in samples such as the one used in this study.
Conclusions and implications
The results of this study have several implications. Although the association between social determinants and mental disorders is highlighted, further studies are needed to examine other psychological determinants such as childhood trauma and their relationships to CPTSD. CPTSD, a new nosology in the literature, has not yet been considered in research and clinical settings in Rwanda. This study aimed to inform researchers and clinicians to consider not only PTSD but also CPTSD.
This study found that 52.3% of participants were free of the symptoms associated with the disorders under consideration. This points to the need for more research on protective factors in trauma contexts in Rwanda. Such research may identify culturally appropriate prevention mechanisms used by trauma survivors to overcome trauma. In addition, clinicians should consider comorbidity and the assessment of social determinants that can contribute to the maintenance of mental disorders.
Our results highlight the importance of making treatment available for survivors of the genocide in Rwanda. Effective treatment, which reduces symptoms of depression and CPTSD, will most likely not only alleviate the immediate burden of suffering due to these symptoms, but will in some cases also have more enduring effects, such as more fulfilling relationships. Evidence shows that the treatment of PTSD, CPTSD, and depression is effective also in low-resource settings such as Rwanda (Barbui et al., 2020; Cuijpers et al., 2018).
It is expected that the results of this study will help researchers, clinicians, and policymakers in the understanding of the long-term correlates of trauma other than PTSD and consider comorbidity and social determinants in their interventions.
Footnotes
Acknowledgements
The authors would like to thank the research assistants Jonas Bikorimana, Etienne Kayumba, Samuel Murwanashyaka, and Adelite Mukamana for their contribution in data collection, data entry, and data cleaning, as well as translation of the questionnaire into Kinyarwanda language.
Data availability statement
Request for the data or materials should be sent per email to the first author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.