
Abstract
Mental disorders are among the most poorly treated illnesses in sub-Saharan Africa. It is estimated that 70%–80% of South Africans consult traditional health practitioners for the treatment of psychological ailments. As traditional health practitioners maintain a strong role in assessing and treating patients with mental illness in this context, this study contributes to the burgeoning research literature on the topic. Semi-structured in-depth interviews were conducted with 18 traditional health practitioners in Johannesburg, South Africa, between January and May 2022. Interviews were transcribed and translated into English. The data were managed using NVivo 12 software and thematically analysed. Traditional health practitioners interviewed generally perceived mental illness to be of supernatural causation, either as a result of bewitchment, a calling for patients to become THPs themselves, due to displeased ancestors, or due to natural causes. Traditional health practitioners identified eight primary treatments that they use for treating mental illness. Among these were throwing of bones (tinhlolo) to start communicating with ancestors, steaming (ukufutha) to start a cleansing process, sneezing (umbhemiso) to forcefully dispel the spirit causing the illness, induced vomiting (phalaza), and the administration of laxatives (mahlabekufeni) to remove the spirits poisoning the body as well as animal sacrifice to purge spirits and communicate with ancestors. This is all followed by cutting (ukucaba), which is the final part of the treatment and ensures that the evil spirit cannot return. Due to the ubiquity of traditional health practitioner usage for mental illness in sub-Saharan Africa, it is essential to understand what conceptions traditional health practitioners have of the aetiology of these disorders as well as their modalities for administering treatment.
Introduction
Mental disorders are considered among the most poorly treated illnesses in sub-Saharan Africa (Kabamba, 2014). In South Africa, while over 16% of adults are estimated to suffer from a common mental disorder, just over 5% of those with a disorder receive treatment from a clinic or hospital (Audet et al., 2017). Previous studies estimate that between 70% and 80% of South Africans consult traditional health practitioners (THPs) for the treatment of illness, with higher rates for psychological ailments, although these figures are largely estimates, as most THPs do not keep records of the patients who make use of their services (Ashforth, 2005; Crawford & Lipsedge, 2004; Kahn & Kelly, 2001; Mzimkulu & Simbayi, 2006; Thornton, 2009). While some researchers have characterized mental healthcare in South Africa as composed of two ‘duelling’ and ‘largely incommensurate paradigms’ when describing Western psychiatry and traditional healing traditions, noting the ‘discordance between cultural beliefs and conventional psychiatric concepts of disease’ (Kahn & Kelly, 2001, p. 35; Ojagbemi & Gureje, 2021, p. 455), others have posited that these paradigms are not necessarily incommensurate as some THPs incorporate ideas regarding causation and treatment of mental illness that are borrowed from biomedicine (Galvin et al., 2023; Hampshire & Owusu, 2013; Mendu & Ross, 2019).
Historically, relatively little attention has been paid to the unique sociocultural elements of mental disorders and their treatment in Africa. Recent research has shown that even when receiving effective hospital treatments, roughly 60% of mental health service users in contemporary sub-Saharan Africa will simultaneously consult THPs for mental health treatment (Ojagbemi & Gureje, 2021). While some writers predicted in 1960s and 1970s that traditional belief systems in Africa would disappear with ‘modernization’ (Ashforth, 2005), many indigenous Africans continue to embrace and promote traditional African worldviews which inform health seeking and healing practices, including beliefs and practices related to sorcery and bewitchment (Kabamba, 2014). In addition, other studies in South Africa have noted the increasing numbers of people becoming traditional healers in recent years (Campbell & Amin, 2014; Thornton, 2017). In many traditional African belief systems, mental health issues are among the most commonly perceived problems related to bewitchment or ancestors, and THPs and religious advisors are viewed as experts in these realms (Kpobi et al., 2019; Ngobe, 2015). Many researchers have realized the importance of religio-cultural elements related to mental illness causation and treatment in sub-Saharan Africa in recent years; thus, this study contributes to the growing scientific literature on the subject (Moshabela et al., 2016; Sorsdahl et al., 2010a; Thornton, 2017; Van der Zeijst et al., 2021). As THPs maintain a strong role in the assessment and treatment of patients with mental illness in this region, this research seeks to understand perceived causes as well as forms of treatment dispensed by traditional healers through the perspective of the local healers themselves.
Methods
Participants
The purpose of this study is to examine the perceived causes and treatment modalities for mental illness among THPs in Johannesburg, South Africa. This study enrolled 18 THPs practicing in townships surrounding Johannesburg, South Africa, between January and May 2022. The determination of the sample size was guided by the concept of saturation in which interviews no longer reveal new content and participants often repeat information previous interviewees reported. Eligibility criteria included: (a) being 18 years of age or older; (b) being able to provide informed consent and consenting to the recording of the interview, and (c) being recognized as an official THP after completing thwasa (traditional healer training). The THPs interviewed lived and worked in Soweto, Katlehong, or Vosloorus townships. While THPs in South Africa are generally divided into diviners (sangomas) or herbalists (inyangas), the healers in this study generally practised both divination and used herbs for treatment (Ngobe, 2015; Shange & Ross, 2022).
Instruments
An interview guide was developed with guidance from two THPs associated with the Health Economics and Epidemiology Research Office (HE2RO) at the University of the Witwatersrand. This guide was pilot tested on two THPs in January 2022. However, the responses generated during the pilot phase are not included in this analysis. Questions included examples such as, ‘What is the role of the THP with regard to persons with mental illness?’, ‘What do you believe are the different causes of mental illness?’, ‘What forms of treatment do you provide for people suffering from mental illness?’ Additional probing questions based on responses given were used as follow-ups to elicit more in-depth discussion.
Mental illness was described as distortions in thought patterns and behaviour, though each healer used their own set of terms to describe it. Mental illness was most often best understood using the isiZulu term, ukuhlanya, which roughly translates to ‘madness’ in English, though other terms were also used. Interviews lasted between 35 and 60 min and were conducted by the study’s principal investigator and research assistants (who were all practicing THPs themselves or in training) at the home or workplace (indumba) of the healer. Research assistants were fluent in English, isiZulu, and isiXhosa and could ensure real-time translations in cases where the interviewee did not speak fluent English.
Study design and procedure
A qualitative study design was utilized, with semi-structured interviews to elucidate THP perceptions of illness aetiology and treatment practices with regard to mental illness. Researchers used an inductive approach in which data informed the development of theory and hypotheses rather than the inverse. All THPs reported treating patients with mental illness. Participants were recruited using a snowball sampling technique in which THPs were referred by means of word of mouth. Participating healers were asked if they could provide contact information for other healers working in Johannesburg. This sampling strategy allowed the researchers to maximize the representation of healers from throughout the townships surrounding Johannesburg.
Ethical considerations
This study received approval from the Human Research Ethics Committee at the University of the Witwatersrand (#M210815) and the Research Committee of Johannesburg Health District (#GP_202111_059). Participants provided written informed consent and were compensated ZAR 100 (roughly $7) for their time. This amount was determined together with the University of the Witwatersrand and HE2RO. All COVID-19 protocols were followed during the collection of study data.
Data analysis
The interview recordings were transcribed and then translated into English. With regard to translated terminology, while some African traditional concepts may not have direct English equivalence, the authors have attempted to ensure the closest approximate meaning possible. African concepts from the Nguni languages are used. Two authors reviewed all English transcripts for content related to the perceived aetiology and treatment of mental illness in THP practices. The transcripts of interviews were analysed on an ongoing basis throughout the study process to ensure that emerging themes could be understood and explored further. Themes were developed iteratively and refined, resulting in the generation of a final set of codes. Both researchers subsequently utilized NVivo 12.0 to code the transcripts.
Results
Eighteen THPs were interviewed for this study, including nine males and nine females. Healers ranged between 21 and 74 years of age, with an average age of 39 years old. The THPs also had between 2 and 48 years of experience as healers, with an average of 16 years.
Causes
The THPs interviewed identified the following four primary causes of mental illness: (1) bewitchment, (2) having a ‘calling’ to become a THP, (3) displeased ancestors, and (4) natural causes. Of the four causes, the first three are considered ‘traditional’ or ‘spiritual’ causes as opposed to ‘natural’ causes which include drugs, stress, or illnesses, such as HIV/AIDS. While ‘traditional’ illnesses are meant to be treated by THPs, ‘natural’ illnesses are considered to require intervention by doctors or hospitals.
Bewitchment
The most common cause of mental illness identified by the THPs was bewitchment (ukuthakatha). Bewitchment generally entails the use of magic to visit illness or misfortune upon another person. As one THP describes, There are those people, our people and traditional doctors . . . they can make a muthi [herbs] mixture to make you mad. So, you will be bewitched. (Female, 68)
The most common form of bewitchment resulting in mental illness cited by THPs was amafufunyana which is a form of spirit possession. The vast majority of THPs noted that people suffering from mental illness through amafufunyana are generally possessed by animal spirits. Among the animal spirits cited were the spirits of snakes (cited by three THPs), monkeys (cited by three THPs), horses (cited by two THPs), dogs (cited by three THPs), and buffalos, vultures, baboons, tigers, and cats (cited by one THP each). THPs described how, when bewitched with the spirit of an animal, the possessed individual will mimic the actions of that animal. For example, If someone is bewitched using a horse, the person would roam around the streets, they wouldn’t stay in one place. (Male, 30)
Three THPs mentioned possession by a mythical creature called a ‘tokoloshe’, in addition to animal spirits mentioned above. As one describes, Tokoloshe, I don’t want to call them dwarfs, but most of the time they are classified as dwarfs . . . It’s a dwarf, a mythological creature. But you can see it. It’s like a demon. (Female, 37)
Another noted that tokoloshe are different than the animal spirits mentioned above, as they are ‘created by the witches from the human being’ (Female, 50). In this sense, they are human rather than animal spirits. In addition to mental illness, tokoloshe possession can also have other effects on an individual: It controls your body . . . It’s a devil spirit that comes in the night. It makes people itchy. But it depends on the person. (Male, 26)
In addition to amafufunyana, bewitchment can also happen through muthi (herbs) that are used to cause ailments such as mental disturbance: Being bewitched comes in 2 ways. Either they send an animal spirit on you, or they use muthi on you. (Male, 30)
However, the results of bewitchment extend far beyond simply mental illness, as the THPs describe individuals getting into car accidents, losing their marriages, or even dying as a result of bewitchment (Male, 28).
Calling to become a healer
An ‘ancestral calling’ to become a traditional healer was the second most common cause of mental illness described by the THPs. Once an individual has a calling, they are then supposed to enter thwasa, or training to become a traditional healer. THPs generally have a calling when their ancestors were also healers in the past. As one THP described, I am a sangoma because my aunt was a sangoma . . . So, I had that in my family . . . A calling is something that happens naturally. I was seeing snakes and sometimes I was talking alone, sometimes I wouldn’t answer you. I was in my own world, that’s a calling. (Male, 40)
Similar to the above description, other THPs also described hallucinations and other symptoms commonly associated with mental illness when they or their patients have a calling. The symptoms become particularly serious when the individual resists the calling: When you refuse to take the calling you end up being crazy. The ancestors come to you and become aggressive towards you. They don’t understand why you aren’t taking the calling. You get sick, you get crazy. (Male, 30)
In this sense, many individuals who experience mental illness and are told they have a calling enter thwasa to become a THP themselves.
Displeased ancestors
Other THPs described how mental illness can be a result of ancestors (amadlozi) who are angry with an individual. As one describes, Your ancestors can be mad at you. They feel that you don’t acknowledge them. There are some people, the ancestors come angry and make actions on you. (Female, 29)
Therefore, this is not because the individual has a calling but rather because the ancestors feel ignored or are trying to correct actions that they do not agree with: They [the ancestors] are trying to align you. To align you to the right route. It’s a cultural thing. You need to do certain rituals to introduce them to your ancestors. And if those rituals are not done it can make you crazy (ukuhlanya). (Female, 38)
In addition, if the ancestors feel they have some sort of unfinished business, they can coerce someone into acting on their behalf (Female, 68). Similar to resisting a calling, ignoring one’s ancestors can have dire consequences, including death: Ancestors can make a person crazy (ukuhlanya) without it being a calling. Sometimes they can do it so . . . they can tell your family what to do. You can’t ignore that. They will come to you up to five times. Ancestors don’t reason. They aren’t like people. They can eliminate you, you die, or make you go crazy. (Male, 21)
Natural causes
Finally, the THPs described mental disorders that are of ‘natural’ causes. Natural causes can include poverty, stress, trauma, illnesses such as HIV/AIDS, and drug addiction (Female, 38). Due to the high rates of HIV in South Africa, healers described receiving patients who develop mental illness or neurocognitive disorders due to the long-term effects of the disease: There are those, like HIV people, too many of them are getting confused because of HIV. (Female, 68)
Hence THPs generally refer patients who are determined to have a mental illness due to natural causes to hospitals for treatment, as they do not consider these forms of care as within their realm of expertise: If you cannot treat traditionally you have to take them to a doctor. (Female, 37)
Treatments
The THPs interviewed identified eight primary treatments for mental illness. Among these were: (1) throwing bones (tinhlolo), (2) steaming (ukufutha), (3) sneezing (umbhemiso), (4) vomiting (phalaza), (5) laxatives (mahlabekufeni), (6) animal sacrifice and (7) cutting (ukucaba). The most common trajectory for treatment among the THPs interviewed for this study is depicted in Figure 1.
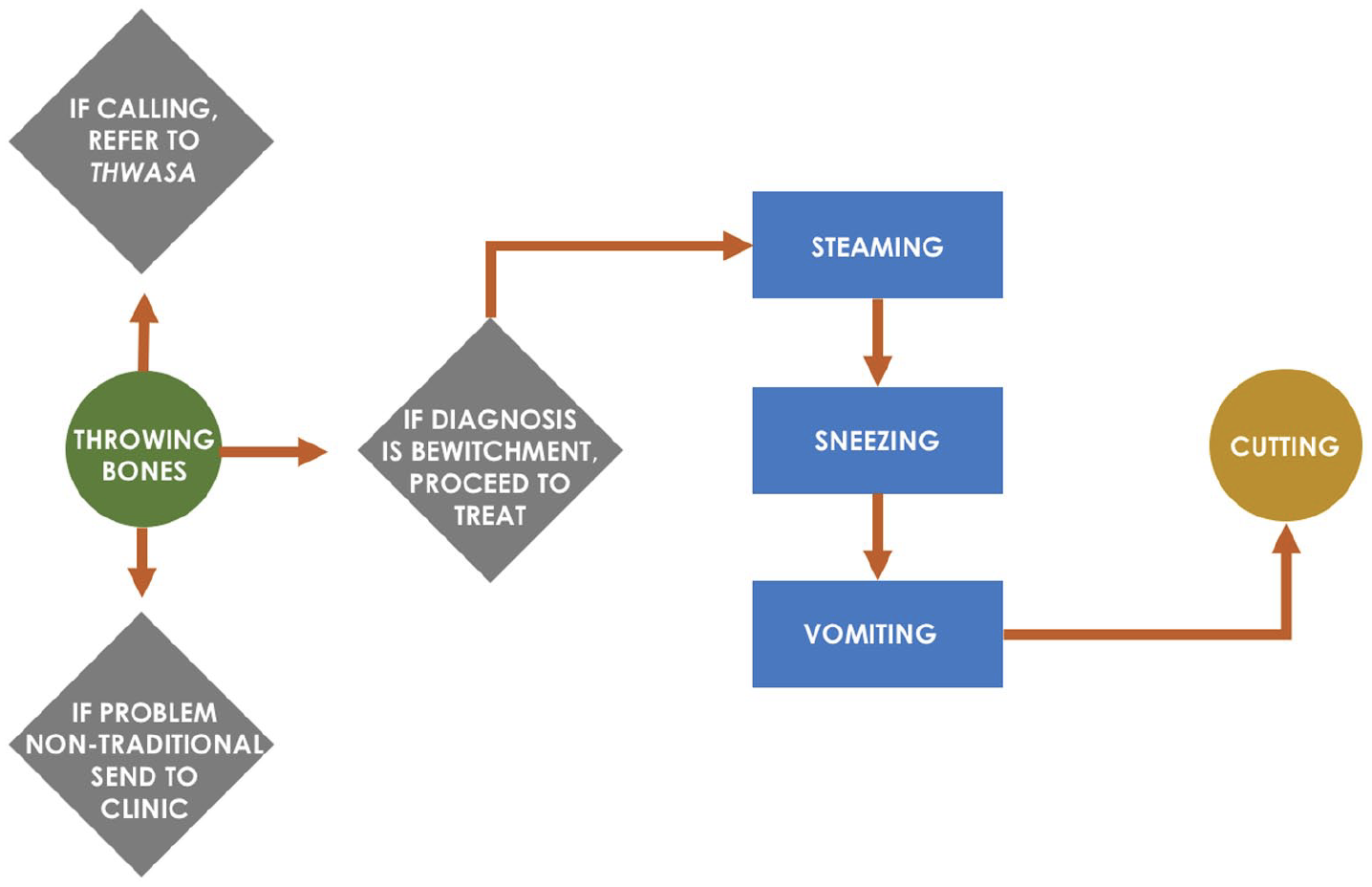
Flowchart depicting most commonly cited treatment pathways by THPs interviewed in this study for patients experiencing mental illness.
Throwing the bones
When treating an illness, THPs first ‘throw bones’ (tinhlolo). Throwing bones is a form of divination in which 20 to 40 items, including bones, dice, shells, dominoes and other objects, are thrown onto a mat and ‘read’ by the THP in communication with the patient’s ancestors. As described by one healer, In the hospital they do x-rays first. My x-ray is throwing the bones. The bones direct me to what kind of healing you get. (Male, 29)
The ritual of throwing the bones, therefore, represents the primary way to interpret the cause of the presenting illness, as well as how to treat it: The bones will tell me what kind of sickness this is. I will throw those bones down. I will say, oh this man, I think he has HIV sickness. The bones will say no. I say, then what is it? Then I will check the witchcraft. The bones will tell me, or the ancestors will show me that we are fighting with this man. That’s where I start to cure them. From the bones, I know now what kind of things I should use for this man [to treat him]. (Female, 68)
Each bone or item has a specific meaning for the THPs. One THP described how different bones, dominoes, dice, or shells indicated different causes of illness, depending on the way they fell when thrown onto the mat. For example, a cheetah bone indicated whether or not the patient has a calling based on whether it fell right side up or down. A goat bone determined if the person was a victim of bewitchment or not, depending on how it landed (Male, 30). Many healers also used a translucent red object to establish if the illness was ‘in the blood’ (Female, 68).
Steaming and sneezing
Following the divination through ‘throwing the bones’, THPs generally start by cleansing the patient by means of steaming (ukufutha). As one described, this ‘opens the pores of your body’ (Male, 21). Steaming usually takes place by placing the patient under a blanket and proceeding to burn herbs. However, some healers also steam with animal body parts: We don’t treat them with muthi only. We use animal skins, animal brains, animal teeth, animal nails. You mix muthi to put inside the nostrils [of the patient] and it works with the brain. Whatever bewitchment they have. And then you put muthi with steam to chase away all the evil spirits that bewitched them. (Female, 38)
Steaming was primarily described as a treatment for afflictions related to bewitchment and functioned as a way to dispel the harmful spirit: The steam, you breathe in here [pointing to nose]. You inhale this smell. If that sort of animal you’re bewitched with, it will get out and run away . . . After the steam makes it go out, I can see it’s witchcraft. After the patient has inhaled the steam and the animal the person was bewitched with has run out, the person will start regaining their consciousness. (Female, 68)
However, steaming is not done as a treatment on its own. Rather, it is done in conjunction with other processes, primarily sneezing (umbhemiso): The first treatment I will do is to steam them. I will use animals and types of different animal bones and herbs to steam them with. Immediately after you’re done steaming, I make them sniff something so that they sneeze. (Male, 40)
Similar to steaming, sneezing is utilized as the next approach of dispelling the spirit causing the illness: Your head was filled with this spirit from the bewitching animal. But now if you sneeze, you take out the breath from that animal. (Female, 68)
Some healers described that sneezing functions as a way to ‘release the tension’, to ‘open the mind-set’ or even as a sort of ‘thermometer’: Sneezing is the traditional healer’s thermometer. The traditional healer will use sneezing as a temperature gauge. She puts ground herbs on the back of the hand for the patient to snort . . . When she gives the person the herbs to sniff, the amount of time it takes to sneeze determines if the person is going to be well or not. (Female, 74)
Vomiting and laxatives
Other forms of purgation generally follow steaming and sneezing, usually in the form of self-induced vomiting (phalaza). The patient is made to vomit by means of a mixture of muthi (herbs) and warm water which causes the ‘poison’ to be expelled (Male, 40). Similar to steaming and sneezing, vomiting is also considered a way for the patient to rid themselves of the spirit causing them harm: The vomit it takes out the . . . Ok, it’s like this. When a person is bewitched, they have a small animal [spirit] put inside of them. Some of them it’s in the stomach some of them it’s in the head. So, you have to do the full course because you never know if it’s in the head or the stomach. So, the sneezing is the head and the vomiting is the stomach. (Female, 38)
Induced vomiting is not the only way to rid the body of the spirit causing harm. However, some healers describe the use of laxatives (mahlabekufeni) to force the ailment out through the patient’s stomach: It [laxatives] makes you poop. That makes your stomach run, so you can bring that dirtiness out of your body through your stomach. (Male, 26)
Healers tended to be generally aware of the risks of practices such as induced vomiting or laxatives on patient health. Particularly for people with HIV/AIDS, these treatments can potentially do more harm than good by flushing antiretrovirals from the system, among other side effects: I don’t like to make people vomit because I don’t always know their HIV status. For some of them . . . Unless I know their viral load and CD4 count. Only then will I make them vomit. (Female, 68)
Some THPs noted that they only induce serious forms of purgation such as induced vomiting or laxatives when they know the patient is ‘strong’, adding that ‘they can’t be weak for that [vomiting or laxatives]’ (Female, 62).
Animal sacrifice
While not as commonly employed as the forms of purgation mentioned above, the THPs also use animal sacrifice as a treatment for many illnesses, including mental illness. The primary animal sacrificed by THPs is a chicken. As one THP describes, The mother of the patient feeds the chicken muthi and speaks to the chicken. You’re speaking to the evil spirit within the child [who is sick]. You tell the chicken you want the evil spirit out of her child. Then you slaughter the chicken with your hand, you crack the neck, and then throw it in the river, and it [the evil spirit] goes away. (Male, 28)
Others described removing certain parts of the chicken for the patient to wash with prior to throwing the chicken carcass into the river: After [slaughtering the chicken] I would take the blood and certain insides of the chicken and mix with muthi and pour it on your skin. That’s when you talk to you ancestors, you talk to them, you assist them, you show them the way. I wash you with medicine, and blood and insides of the chicken, that means I allow you to talk to the ancestors yourself. (Male, 21)
Of primary importance in this tradition is the use of the gall bladder (inyongo) and the bile inside which allows contact with one’s ancestors: You cleanse yourself with the bile, you’re purifying yourself with it so you’ll be able to connect with your ancestors. You bathe with the bile. (Male, 30)
The colour of the chicken also has significance in this ritual, with some THPs defending the use of white-feathered chickens and others arguing that black-feathered chickens are more effective.
Cutting
The last step in treatment is almost always cutting (ukucaba). Cutting involves the healer making small incisions on the skin of the patient with a razor and then rubbing muthi in the cuts. The purpose of cutting is to offer long term protection to the patient as one healer describes: When people are mentally disturbed, I don’t use cutting until I realize that it is traditionally related. First, I will use sneezing and vomiting, and then to protect you so the thing doesn’t come back again, that is when I will cut you. But you can’t cut before. This is how the treatment goes . . . The cutting is based on the belief that if we cut you before the treatment, we are protecting you from the treatment. So, I must first take out whatever is bad and then protect you. (Male, 40)
Many healers also described cutting as a form of ‘strengthening’ or ‘making the patient strong’. In this way, the spirits that previously harmed the individual will be unable to return and harm them again: After the whole treatment, if you see the person is ok now, starting to reason, behavior is changing, then you do ukucaba so the evil spirits can never come back again. To protect that person. (Female, 38)
Incisions are usually made on the head, stomach, arms, legs, and feet and generally do not result in infection according to the healers interviewed as they are not deep cuts.
Discussion
This study examined the perspectives of 18 THPs in Johannesburg, South Africa regarding the aetiology and treatment of mental illness. Healers generally attributed mental illness to supernatural causes and prescribed healing rituals that primarily included forms of purgation as a cure for patients to rid themselves of the spirit causing them harm.
Causes
With regard to the cause of mental illness, the THPs interviewed generally perceived mental illness to be of supernatural causation, as a result of bewitchment, a calling for the patients to become THPs themselves, or due to the ancestors of the patient being displeased. A minority of causes were perceived as ‘natural’ or biopsychosocial, meaning they stem from traumatic experiences, stress, poverty, illnesses such as HIV/AIDs, or addiction. While few studies exist on these subjects, research in South Africa has confirmed this distinction between ‘supernatural’ and ‘natural’ aetiologies for mental illness among healers (Crawford & Lipsedge, 2004; Sorsdahl et al., 2010b). Another study decided to subdivide ‘supernatural’ causes into ‘spiritual’ and ‘socio-cultural’ factors and subdivided ‘natural’ causes into ‘psycho-social’ and ‘physical’ factors (Shange & Ross, 2022). As it is the role of a spiritual healer to determine the cause of a patient experiencing mental distress, other researchers also found that it is common for mental health problems in this setting to be attributed to ‘traditional causes’ – in particular bewitchment or the influence of ancestors (Mzimkulu & Simbayi, 2006; Ngobe, 2015; Sorsdahl et al., 2010a).
THPs claim to utilize supernatural powers as diagnosticians to ascertain who – rather than what – causes misfortune and illness (Louw & Duvenhage, 2016; Mzimkulu & Simbayi, 2006; Shange & Ross, 2022). In this sense, illness and misfortune are often perceived to be a result of ‘witches . . . believed to have the ability to mobilize their evil powers and the forces of nature to harm other people’ (Sorsdahl et al., 2010a, p. 286). Some scholarship on this subject has explored the relationship between misfortune and imprecations – or curses – in traditional belief systems in South Africa (Ashforth, 2005; Mzimkulu & Simbayi, 2006). Researchers describe how the root cause of misfortunes can be attributed to jealousy among friends or family members, often referred to as the ‘elemental motive of witchcraft’ (Ashforth, 2005, 34). This jealousy can lead to an array of different sorcery-related illnesses and disorders as depicted in Peltzer’s (1999, 2001) extensive nosology. In particular, the distinction between ukuthakatha and amafufunyana – two different but overlapping conceptions of bewitchment – was examined in other research, with amafufunyana referred to as a ‘wastepaper basket term’ among healers to designate hallucinations, delusions, outbursts of aggression, and violence (Mzimkulu & Simbayi, 2006, p. 418).
In addition to bewitchment, similar studies to this one have described the important role of ancestors (amadlozi) as the cause of mental distress (Mzimkulu & Simbayi, 2006; Sorsdahl et al., 2010a). This can either take the form of a calling to become a healer as a result of ancestors passing down their gift as a THP from the past, or because the ancestors feel neglected or their advice was unheeded (Crawford & Lipsedge, 2004). In this sense, ancestors may withdraw their protection or make someone fall ill if family members do not perform certain rituals or commit acts they disagree with (Mzimkulu & Simbayi, 2006). Finally, as South Africa has among the highest rates of HIV infection in the world, AIDS, substance abuse, and life stressors are also increasingly acknowledged as root causes of mental distress by THPs (Sorsdahl et al., 2010a).
Treatment
When treating patients, the THPs interviewed for this study first determined the nature of the illness and how to administer treatment to the patient by ‘throwing the bones’ (tinhlolo). Other studies have examined this divination practice in which a collection of natural objects (such as bones, shells, dice, pieces of plastic, beads, and dominoes) are thrown onto the ground and interpreted by the healer in conjunction with the ancestral spirits (Crawford & Lipsedge, 2004; Shange & Ross, 2022; Thornton, 2009, 2017). Each of these objects has a range of meanings and serves as a ritualistic way not only to determine the cause of the ailment but also to show how to treat and cure it. As described in his seminal work, Healing the exposed being: The Ngoma healing tradition in South Africa, Robert Thornton (2017) argues that the goal of THP treatment is to cleanse and restore wholeness in patients as a way to protect their ‘exposed being’ (p. 121). In this conception of the self, individuals are always exposed to outside forces such as bewitchment or possession and the healer’s job is to seal them off from these malefic forces. Other authors confirmed this view arguing that THP treatments are aimed at ‘harmonizing the patient with their environment through neutralizing sorcery, appeasing ancestors’ (Crawford & Lipsedge, 2004, p. 131).
Communication with the ancestors (ukuphahla) throughout treatment is paramount, as the THP must simultaneously determine the wishes of the patient’s ancestors in treatment while also using their own ancestors for guidance and direction while treating (Mzimkulu & Simbayi, 2006; Thornton, 2017). This includes determining the appropriate forms of purgation that are necessary to restore wholeness to the patient’s being by ‘flushing out evil spirits’ (Shange & Ross, 2022, p. 516). Many other studies in South Africa have examined these forms of healing, ranging from steaming with herbs, washing, induced vomiting through the nose or mouth, sneezing, laxative herb mixtures, enemas, incising, and bloodletting (Ashforth, 2005; Mzimkulu & Simbayi, 2006; Ngobe, 2015; Shange & Ross, 2022; Thornton, 2017). While not all of these were reported among the THPs interviewed for this study, there was significant overlap with other research in respect of treatment modalities.
Of central importance in these treatments is the use of muthi (herbs), which can be composed of leaves, bark, seeds, roots, or animal products, including bones, teeth, fats, organs, and skin (Thornton, 2009, 2017). As observed during the course of this study, researchers noted that these muthi are generally maintained in large collections of unlabelled glass bottles and jars, which are kept in the healer’s workspace (indumba). The administration of the muthi can be done orally, through the nose, anally using enemas, or by means of small incisions in the skin, usually in order to induce the desired purgative effect of extracting the spirit causing harm (Sorsdahl et al., 2010a; Thornton, 2017). After completing their rituals and administering treatment, healers conclude the healing process with cutting (ukucaba), which other research has referred to as ‘vaccinations’ against future harm (Shange & Ross, 2022).
In addition to better understanding the practices of THPs in these locations, another primary purpose of this study was to identify harmful practices that may be detrimental to patients. By identifying these practices, researchers and practitioners can work with healers to decrease or eliminate rituals and/or treatments that may further harm patients. One study noted the harmful uses of commercial liquid antiseptics or benzene in the treatment of mental illness by THPs. However, this was not observed during the course of this study, despite asking participants during interviews if they used these items (Sorsdahl et al., 2010a). Another study noted other risky practices among THPs, such as herbal toxicity when healers administered certain muthi to patients, resulting in kidney or liver damage (Kajawu et al., 2016; Shange & Ross, 2022). These same authors warn about the risks of inducing a patient to vomit, particularly as this can reduce the effectiveness of some biomedical treatments. In our study, many healers seemed aware of the health risks of induced vomiting, particularly for HIV-positive patients. Similarly, some research warned about healers utilizing the same razor blade when cutting (ukucaba) different patients, thereby risking HIV infection (Kajawu et al., 2016). Occasionally, healers also will claim that they have the ability to cure HIV/AIDS as well as other sexually transmitted diseases, which can also represent a significant risk to patient health (Peltzer, 1999; Sorsdahl et al., 2010a). Several healers in this study made similar claims.
As this study is qualitative and only involved 18 THPs, it is not meant to be generalizable to the general population of healers in Johannesburg or Southern Africa. Rather, this study provides specific and detailed information about a unique population of interest. While there are many similarities with other studies that have examined the perceived aetiology and treatment of mental illness by THPs in Southern Africa, more research is needed to fully assess the ways in which these healers diagnose and treat patients with mental health problems.
Conclusion
The purpose of this study was to examine the perceived aetiology and treatment practices for mental illness among THPs in Johannesburg, South Africa. Other researchers have cited similarities in approaches to traditional beliefs and healing throughout sub-Saharan Africa (Kajawu et al., 2016; Ngobe, 2015; Ngoma et al., 2003). Despite this, our understandings of the characteristics and practices of healers as well as those using their services remain limited. As an overwhelming percentage of the population in sub-Saharan Africa continues to depend on traditional medicine to help meet healthcare needs (particularly for ailments such as mental illness), it is important for research to understand what conceptions THPs have of the aetiology of these disorders, as well as their modalities for administering treatment. Future research should continue to document the ways in which healers approach healthcare in these regions using methods that contribute to nuanced understandings of traditional worldviews and the emerging field of African psychology, as well as interventions that can foster collaboration between THPs and biomedical professionals to better inform local policy and practice (Gone & Kirmayer, 2020).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the Fogarty International Center and the Office of Behavioral and Social Sciences Research (OBSSR) of the National Institutes of Health under Award Number D43 TW010543. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.