
Abstract
This study investigated the extent to which intimate partner violence (IPV) is associated with antiretroviral therapy (ART) adherence among individuals receiving ART care in Johannesburg, South Africa. A two-stage purposive sampling method was used to recruit 200 men and women from two government ART sites through a cross-sectional survey. Adherence was obtained with the AIDS Clinical Trials Group (ACTG) questionnaire, exposure to IPV with the Violence Against Women Instrument (VAWI), and other demographic variables were assessed. Multiple regression analyses assessed the association between types of IPV, ART adherence, and demographic variables. Participants were predominantly female (67%), with ages ranging from 19 to 51 years (M = 34.9). The average ART adherence was 79%, and 51% reported exposure to IPV, mostly women (67%). Multiple regression analysis showed a significant negative association between IPV and ART adherence, with adherence decreasing by 18% (β = −17.92, p < .001) among those experiencing IPV. Sexual IPV had the strongest impact, reducing adherence by 30% (β = −29.71, p < .001), followed by emotional IPV (β = −12.53, p < .001) and physical IPV (β = −9.54, p < .001). Despite controlling for age, sex, years living with HIV, and ART duration, IPV remained negatively associated with ART adherence. The study highlights the pronounced negative influence of IPV, particularly sexual IPV, on ART adherence. In line with previous studies, we recommend the prioritisation of IPV screening in ART dispensing facilities and providing targeted psychosocial support to ART users exposed to IPV, especially women.
Keywords
Introduction
South Africa has made substantial progress in its fight against HIV/AIDS. From 2017 to 2022, the prevalence of HIV declined from 8 million to 7.8 million people, and viral suppression increased from 62% to 81% (Human Sciences Research Council [HSRC], 2023). The country is also steadily advancing towards the UNAIDS 95-95-95 targets of eradicating AIDS by 2030. As of 2022, 90% of people living with HIV (PLWH) were aware of their status, 91% were on treatment, and 94% of those on ART were virally suppressed (HSRC, 2023). This is a substantial improvement from the 85%-71%-87% figures achieved in 2017, during the period of the 90-90-90 targets. This progress is attributed to factors such as revised ART guidelines that provide immediate access to ART, regardless of clinical status; reductions in HIV infections; fewer infants born with HIV; and reduced AIDS-related deaths (Zuma et al., 2022).
Despite advances in expanding HIV treatment and reducing related health complications in South Africa, ART adherence remains suboptimal, particularly in major cities like Johannesburg (van Schalkwyk et al., 2021). Johannesburg is among the cities struggling to meet the UNAIDS 95-95-95 targets, reflecting challenges with treatment discontinuation, poor adherence, and retention in care (Campbell et al., 2020). High ART adherence (>95%) is crucial for PLWH to achieve viral suppression, prevent transmission, reduce infections, and improve health outcomes (Nachega et al., 2018).
Intimate partner violence (IPV), a form of interpersonal violence, is a pervasive barrier to ART adherence (Hatcher et al., 2019). IPV, a subset of domestic violence (DV), is distinctly defined as physical, psychological, or sexual violence between current or former partners, separate from broader household abuse such as child or elder maltreatment (Ali et al., 2016). South Africa has an exceptionally high IPV prevalence (55%), far exceeding rates in high-income countries (25%) (Statistics South Africa, 2020; World Health Organization [WHO], 2021). While IPV affects individuals of all identities, women are disproportionately vulnerable, with approximately one in five South African women and one-third of men reporting lifetime exposure (Gubi & Wandera, 2022; Selin et al., 2019). IPV manifests through (1) physical violence (acts causing bodily harm), (2) emotional violence (coercive control, humiliation), (3) sexual violence (non-consensual/coerced acts), and (4) economic violence (financial control/sabotage). Emotional and physical violence are most commonly reported, while sexual violence is often underreported due to stigma (Gibbs et al., 2022; Jud et al., 2023). In high-prevalence areas like Gauteng, home to Johannesburg, young women and girls face heightened risks (Mthembu et al., 2021). These overlapping forms of IPV, worsened by structural factors such as poverty and gender inequality, create complex barriers to health care access and adherence for PLWH.
Globally, IPV consistently predicts poor ART adherence, particularly in the Global South (Hatcher et al., 2019; Sardinha et al., 2022). In South Africa, a bidirectional relationship exists where violence increases HIV risk through coerced unprotected sex and prevention interference and worsens after HIV diagnosis (Jewkes et al., 2006, 2015). Economic violence through sabotaging financial resources limits health care access in settings with high inequality (Hatcher et al., 2022). Emotional violence shows particularly severe impacts on treatment adherence among adolescent girls and young women in high-prevalence regions like Gauteng (Mthembu et al., 2021). These challenges are worsened by the underreporting of sexual violence, which conceals its full impact on adherence (Gibbs et al., 2022).
IPV is a pervasive barrier to ART adherence that differs from structural factors (e.g., health care access) and individual factors (e.g., side effects) by operating through three interconnected mechanisms driving non-adherence. IPV undermines adherence by (1) direct coercive control tactics such as withholding medication, (2) exacerbating mental health conditions like posttraumatic stress disorder (PTSD) and depression that impair treatment management (Marinda et al., 2021), and (3) systematically eroding essential social support networks. These combined effects contribute to worsened HIV progression and reinforce gendered health disparities. The interplay of these mechanisms, amplified by structural inequalities, creates a syndemic dynamic that intensifies both IPV and HIV outcomes (Jewkes et al., 2015), positioning IPV as a uniquely complex adherence barrier intertwined with gender, economic, and health care disparities.
Given South Africa’s intersecting epidemics of IPV and HIV, research on the impact of IPV on ART adherence, particularly the differential effects of physical, emotional, and sexual violence, provides critical insights into the nuanced understandings of how IPV impedes treatment adherence. The findings can guide health care policymakers in strengthening efforts to identify, monitor, and address IPV within adherence care programmes. This study investigated the extent to which IPV was associated with ART adherence among individuals in ART care in Johannesburg, South Africa.
This study explored the following research question: What is the estimated association between IPV and ART adherence among individuals in ART care in Johannesburg, South Africa? Specifically, which type of IPV (physical, emotional, or sexual violence) exerts the strongest effect on ART adherence?
Through a cross-sectional study, we hypothesised that,
IPV would be negatively associated with ART adherence.
Physical, emotional, and sexual IPV would have varying effects on ART adherence.
The corresponding null hypotheses were:
There is no association between IPV and ART adherence.
Physical, emotional, and sexual IPV have no differing effects on ART adherence; that is, all types of IPV affect ART adherence equally or not at all.
Methods
Study design and setting
Data for this cross-sectional study were collected between 2018 and 2020 at two government clinics in southern Johannesburg: Nirvana Community Health Clinic (CHC) (Lenasia) and Diepkloof Provincial Hospital (Soweto). A 1-year gap in data collection occurred due to the primary researcher’s illness in 2019. Both clinics, part of the government ART network, are situated in a high-HIV prevalence region with increasing rates of IPV, particularly among PLWH (Mthembu et al., 2021). Serving large, diverse patient populations, these clinics ensured a representative sample and facilitated efficient data collection while capturing variations in patient experiences (Pillay et al., 2021). Their selection aligned with the study’s objective to examine the impact of IPV on ART adherence in a high-HIV-prevalence urban context.
Participants and sampling
A two-stage purposive sampling process was employed. First, Nirvana CHC and Diepkloof Provincial Hospital were selected from approximately 30 public health facilities in Johannesburg, representing clinics serving a population of 355,000 ART recipients at the time of the study (Gauteng Department of Health, 2017). Second, 200 participants were systematically recruited proportionally based on patient flow during medication refill days across both sites. Participants included men and women aged 18 years or older who had been on ART for at least 6 months, consistent with South African guidelines allowing sufficient time for adherence education and stabilisation (Gauteng Department of Health, 2016).
Sample size determination
We used G*Power software (version 3.1) to conduct an a priori power analysis and to estimate the required sample size of 200 men and women (Faul et al., 2007). Following the primary objective of estimating the association between IPV and ART adherence, a sample size of 200 was determined as the minimum necessary to compare the mean ART adherence between those experiencing IPV and those not, using a one-sided alpha of .05, effect sizes of 0.30–0.40, and a power level of 80%.
Instruments
Demographic factors
Participants’ age, sex, years of HIV diagnosis, and duration of ART were assessed, as these factors have been identified in the literature as potential determinants of ART adherence.
Intimate partner violence
IPV exposure was determined with the 13-item Violence Against Women Instrument (VAWI) that was developed by WHO (2005). Originally designed for women, the VAWI has been adapted for male populations, broadening its usage in IPV research (Nybergh et al., 2013). The VAWI examines three types of violence in intimate relationships that occurred within the last 12 months: physical violence (slapping and hitting), emotional violence (intimidation and humiliation), and sexual violence (forced or coerced sexual acts). Participants answer each question with ‘Yes’ or ‘No’, with a ‘Yes’ indicating exposure to IPV. The VAWI has shown high reliability, with a Cronbach’s alpha of .94 in this sample, aligning with previous findings in South Africa (Dunkle et al., 2006) and Kenya (Leis et al., 2021).
ART adherence
Participants’ ART adherence was assessed using the pill-dosage recall section of the AIDS Clinical Trials Group (ACTG) adherence follow-up questionnaire developed by Chesney (2000). They reported the number of doses missed over the four days before their clinic visit, with optimal adherence defined as no missed doses and suboptimal adherence indicated by any missed doses. The adherence ratio was calculated by dividing the number of doses consumed by the number prescribed and multiplying by 100 (Reynolds et al., 2007). In this study, the ACTG questionnaire showed good reliability (α = .87), which is consistent with the internal consistency of α = .85 reported by previous studies (Kekwaletswe et al., 2014). Participants who indicated missing doses were prompted to explore reasons for non-adherence through a section containing 14 items, which were assessed on a four-point Likert-type scale from ‘never’ to ‘often’.
Data collection procedure
Participants were recruited by the corresponding author and a trained assistant, both fluent in Sesotho and isiZulu (the most commonly spoken languages in the area), at two government HIV clinics during medication refill days. Patients were approached while awaiting medication, and the study’s purpose, benefits, and potential drawbacks were explained. Bilingual support ensured comprehension, with English proficiency required for participation, as both the consent form and questionnaire were provided in English. Interested participants provided informed consent before completing the questionnaire, which was piloted and refined for cultural appropriateness and administered with assistance. Participants in distress were referred to counselling services at Chris Hani Baragwanath Hospital, along with gender-based violence support information.
Data analysis
The questionnaires were analysed using IBM SPSS Statistics version 26 (IBM Corp, 2016), with descriptive statistics employed to summarise participants’ demographic information. Responses regarding exposure to IPV were categorised into four variables: overall IPV, physical IPV, emotional IPV, and sexual IPV, with ‘Yes’ coded as 1 (exposed) and ‘No’ as 0 (not exposed). ART adherence was calculated by dividing the number of doses consumed over four days by the number prescribed, resulting in a continuous adherence percentage from 0 to 100 (Reynolds et al., 2007). Data quality was confirmed with less than 5% missing values. Simple regression models were used to explore associations between IPV (independent) and ART adherence (outcome), with stepwise regression applied to assess the impact of different types of IPV on adherence. Assumptions for the regression analyses were checked to ensure data fitness.
Ethical considerations
Permission was granted by the University of South Africa (UNISA) and the Johannesburg Health District. Participation was voluntary and anonymous, and consent was obtained through a signed informed consent form. Ancillary care was addressed by referring participants experiencing distress or IPV to counselling services, along with information on gender-based violence support.
Results
Sample characteristics and ART adherence
As shown in Table 1, the majority of the 200 participants were female (67%, n = 134) and aged 31–40 years (49%, n = 99). Participants’ mean years living with HIV were 3 years (SD = 1.80), with most (41%, n = 81) reporting having lived with HIV for 3 to 4 years. Regarding ART duration, participants had been on ART for an average of 2 years (SD = 1.41). The mean adherence among participants was 79% (SD = 23.70), with more than half non-adherent (54%, n = 109).
Participant characteristics and HIV/ART history (n = 200).
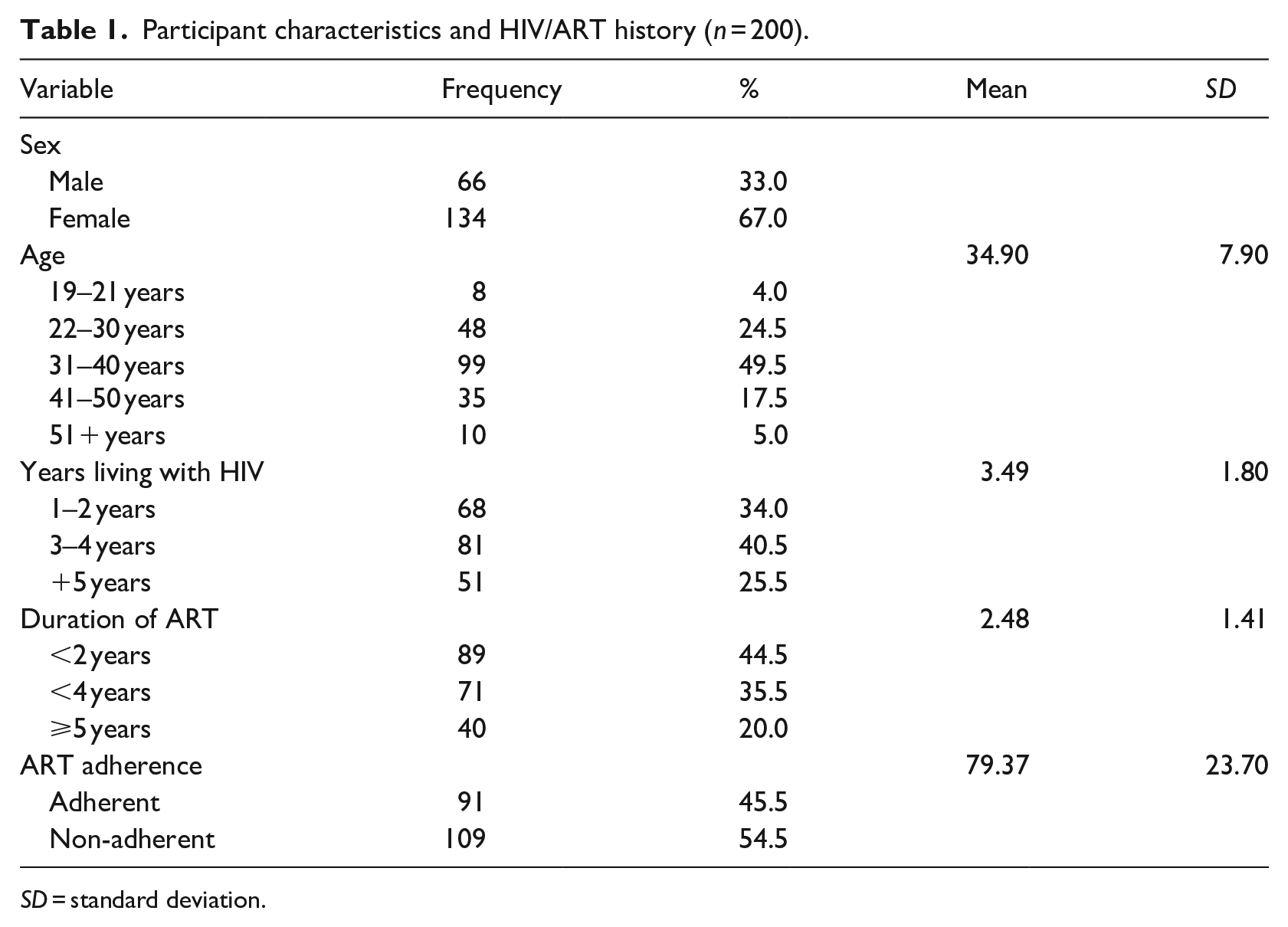
SD = standard deviation.
Reasons for suboptimal adherence
Non-adherent participants were asked to report how often they missed their medications for each of the 14 listed reasons over the past month, with the option to cite multiple reasons. As illustrated in Figure 1, data from 109 participants revealed that the most common reasons for skipping medication included being away from home (100%, n = 109), busyness (88%, n = 96), avoiding being seen taking antiretrovirals (82%, n = 89), feelings of depression (64%, n = 70), and changes in routine (62%, n = 63).
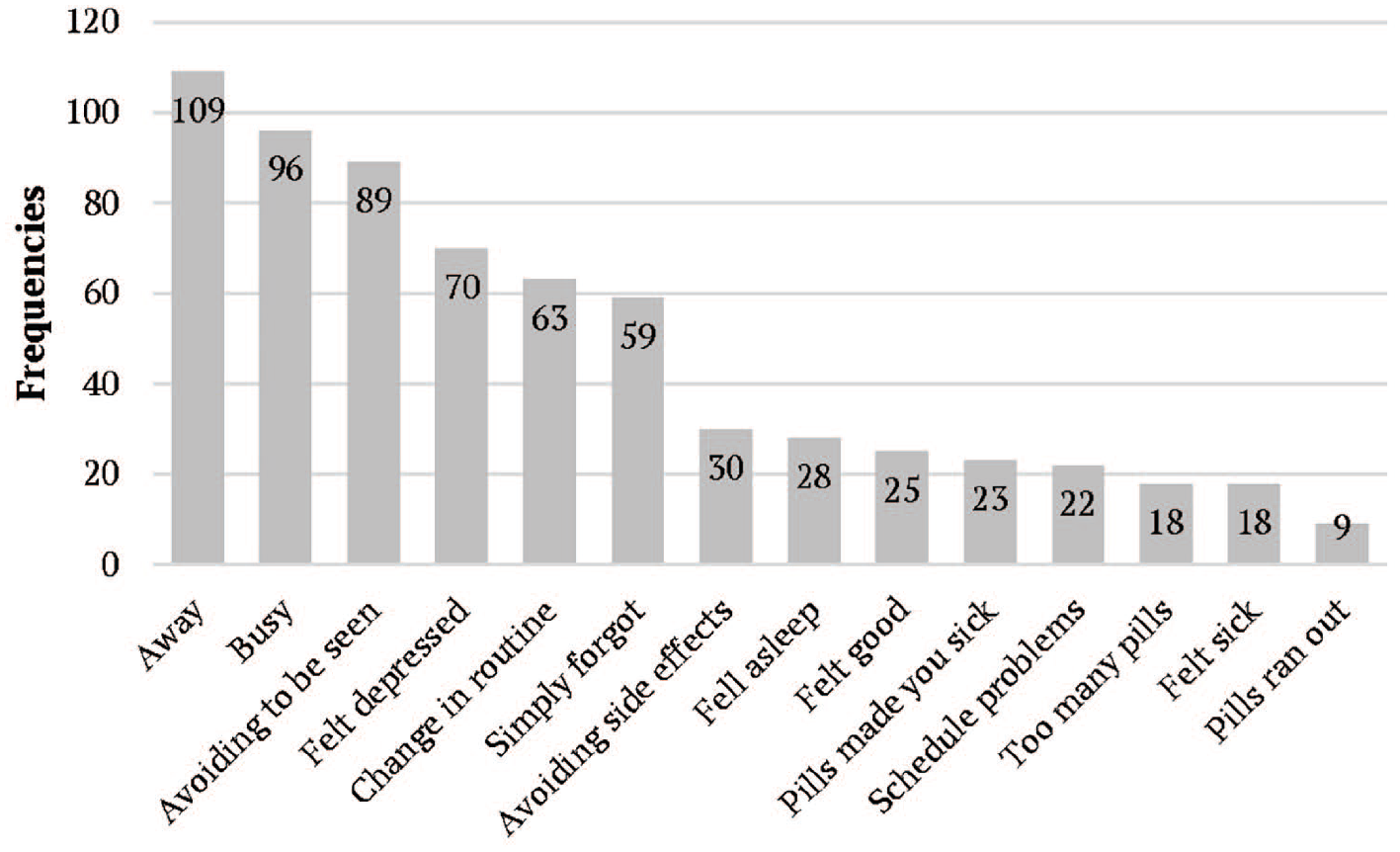
Participants’ reasons for suboptimal adherence (n = 109).
Exposure to IPV in the current relationship
In terms of exposure to IPV, more than half of the participants (51%, n = 102) reported being exposed to IPV in general (Table 2). Of those who reported exposure, more females (67%) reported exposure to IPV compared to males. Regarding exposure to specific types of IPV, most (89%) reported exposure to emotional violence, followed by physical violence (49%). Sexual violence was the least reported type of IPV (44%).
Number of participants reporting intimate partner violence (n = 102).
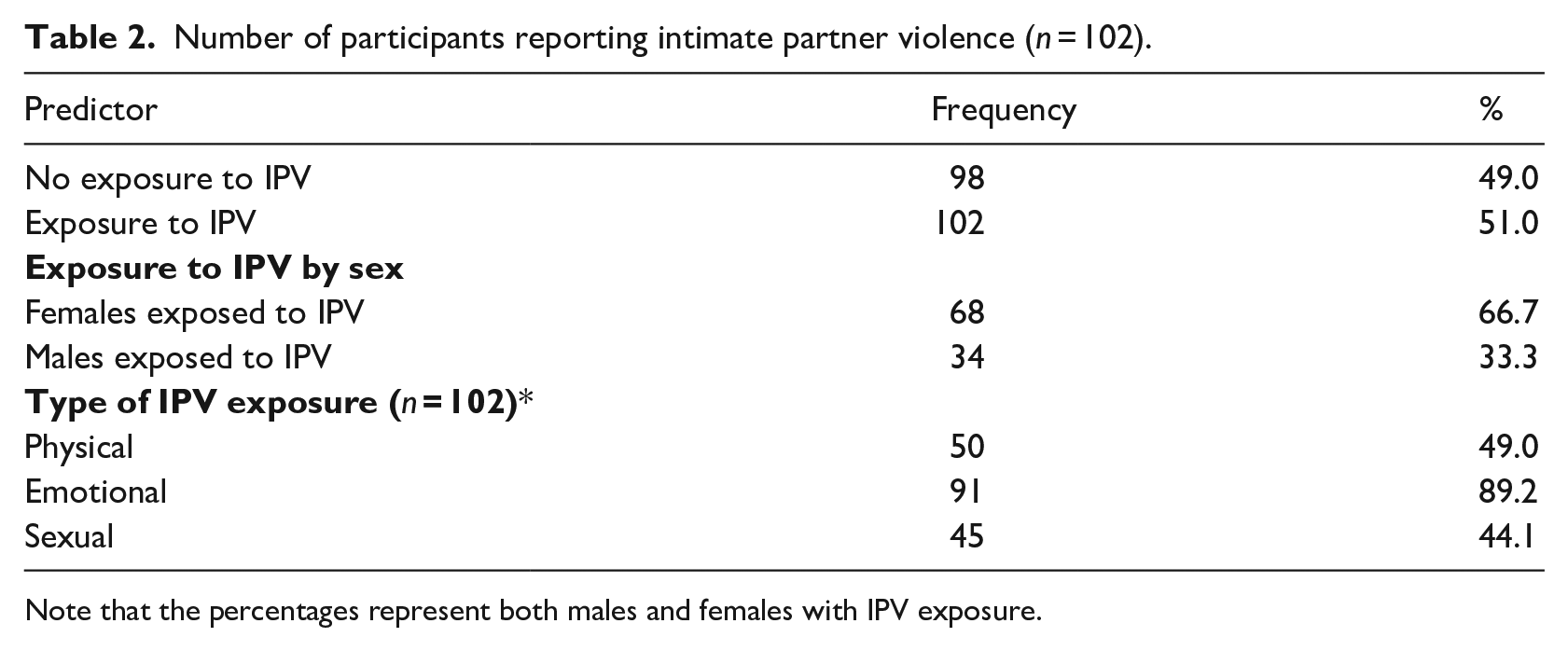
Note that the percentages represent both males and females with IPV exposure.
Simple regression of IPV and ART adherence
Results of the simple regression analysis, as shown in Table 3 (model 1), revealed that exposure to any form of IPV is associated with an 18% reduction in ART adherence (p < .001). Results (Table 3, Model 2) further revealed that all three types of violence, physical IPV (β = −9.54, 95% CI: [−15.75, −3.34], p < .001), emotional IPV (β = −12.53, 95% CI: [−18.81, −6.25], p < .001), and sexual IPV (β = −29.71, 95% CI: [−37.94, −21.47], p < .001), are negatively associated with ART adherence. Sexual IPV is associated with a 30% reduction in adherence, nearly three times higher than the 10% reduction linked to physical IPV and almost double the 13% reduction associated with emotional IPV.
Models of ART adherence – Beta coefficients.
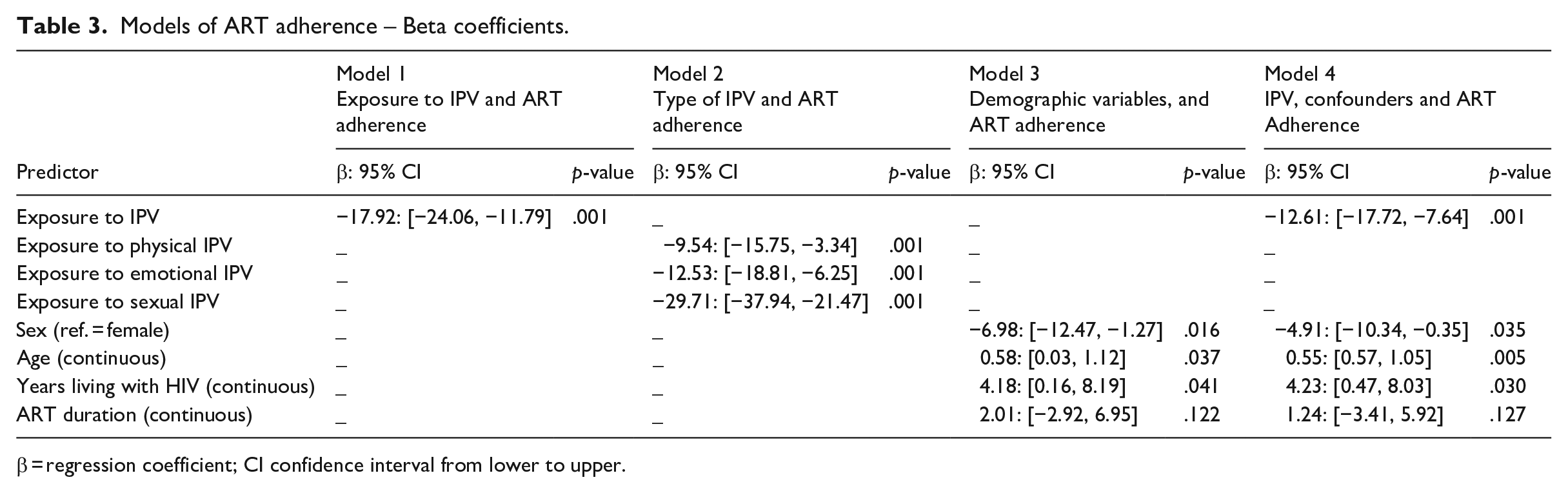
β
Further analysis of the demographic variables (Table 3, Model 3) revealed that, except for time on ART, sex, age, and years living with HIV were significantly associated with ART adherence. Being male was associated with a 7% decrease in ART adherence (β = −6.98, 95% CI: [−12.47 to 1.27], p < .016), while age was associated with a 6% increase in adherence (β = .58, 95% CI: [0.03, 1.12], p < .037). The number of years an individual had been living with HIV was significantly associated with an improvement of 4% in ART adherence (β = 4.18, 95% CI: [0.16, 8.19], p < .041). Exposure to any type of IPV (Table 3, Model 4) remained significantly and negatively correlated with ART adherence, even when regressed with other demographic covariates (β = −12.61, 95% CI: [−17.72, −7.64], p < .001).
Discussion
Characterising ART adherence and IPV
Based on the responses of 200 predominantly female participants (66%), the mean ART adherence rate was 79%, consistent with South African studies (63%–88%) (Laher et al., 2021; Moosa et al., 2019) but lower than Kenyan findings (95%) (Biomndo et al., 2021). Variability in adherence rates may reflect differences in study populations, sample sizes, and measurement methods. IPV was reported by more than half (51%) of the participants, with a significantly higher prevalence among females (67%) than males, aligning with South African and global trends highlighting the disproportionate burden on women (Hatcher et al., 2022). This gendered pattern is reflected globally, with 43% of women in Mexico (Bott et al., 2019) and 41% of women compared to 26% of men in the United States (Centers for Disease Control and Prevention [CDC], 2023) reporting lifetime IPV experiences.
Common reasons for non-adherence included being away from home, having busy schedules, and avoiding stigma, often linked with depression. These findings suggest that IPV may contribute to non-adherence through displacement, stigma, and mental health issues, creating chaotic living conditions that interfere with medication routines and clinic attendance (Lazenbatt & Devaney, 2014).
Commonly reported type of IPV in PLWH
The study found that emotional violence was the most common form of IPV among PLWH at 89%, followed by physical IPV (49%) and sexual violence (44%). These findings align with previous research in South Africa (Gibbs et al., 2022), Tanzania (Muluneh et al., 2020), and Germany (Jud et al., 2023), highlighting the prevalence of emotional abuse, which may serve as a precursor to physical or sexual violence (Renner et al., 2014). While sexual IPV was the least reported, consistent with underreporting in similar contexts (Okafor et al., 2021), its prevalence is generally higher in low- to middle-income countries than in high-income countries (WHO, 2021). Underreporting of sexual IPV may be influenced by fear of victimisation, stigma, societal norms, and psychological barriers such as denial and beliefs about male sexual entitlement (Jewkes et al., 2006; Mphaphuli & Smuts, 2021).
The estimated influence of IPV on ART adherence
The study found that exposure to any form of IPV is associated with an 18% decrease in ART adherence, rejecting the first null hypothesis. This finding is consistent with research from South Africa (Gibbs et al., 2022), India (Achchappa et al., 2017), and the United States (Hatcher et al., 2019). Poor mental health and dysfunctional home environments associated with IPV may explain this negative impact (Marinda et al., 2021). The second null hypothesis was also rejected, as the study demonstrated that all types of IPV negatively affected ART adherence. Sexual IPV is associated with a 30% reduction, significantly three times higher than physical IPV (10%) and nearly twice as high as emotional IPV (13%). These results align with previous research (Hatcher et al., 2022), emphasising the necessity for IPV screening and psychosocial interventions in ART care programmes. The pronounced negative effect of sexual IPV may be linked to mental health issues like depression and PTSD (Marinda et al., 2021), while physical IPV might be perceived as less severe due to societal norms and patriarchal values that legitimise violence (Sikweyiya et al., 2020). Socioeconomic vulnerabilities further exacerbate the cycle of violence and poor mental health (Tusa et al., 2022), highlighting the need for culturally relevant IPV interventions that address broader societal and economic factors that contribute to the normalisation and perpetuation of violence.
Demographic and other covariates of ART adherence
The study identified significant associations between ART adherence and demographic factors, including sex, age, and years living with HIV. Males demonstrated higher non-adherence rates than females, consistent with global trends showing men are 50% more likely to exhibit non-adherence, as highlighted in a 2020 systematic review across sub-Saharan Africa, North America, Europe, and Asia (Evans et al., 2020). Older age correlated with improved adherence (6% increase per year), aligning with findings from sub-Saharan Africa and high-income countries such as the United States and Australia (Mody et al., 2022). Longer HIV duration was associated with a 4% adherence increase, contrasting with prior evidence suggesting that longer pre-treatment durations may lead to suboptimal adherence (Davis et al., 2021). After controlling for demographics, IPV remained significantly linked to a 13% reduction in adherence (β = −12.61, p < .001), consistent with studies in Uganda and India reporting 30%–40% adherence declines due to IPV, even after adjusting for demographics (Hatcher et al., 2019; Srikrishnan et al., 2021).
Strengths and limitations
A key strength of this study is the diverse sample, which includes both males and females aged 18–51 years receiving ART from two clinics in Johannesburg, thereby enhancing the generalisability of the findings. Previous studies typically focused solely on specific populations, such as women (rightly so) or participants in clinical trials. However, we acknowledge limitations related to purposive samples and self-reported measures of IPV and adherence, which may introduce self-selection and recall bias and social desirability, potentially overestimating adherence and underreporting IPV experiences. Thus, findings should be interpreted with caution. The stigma surrounding IPV may further hinder participants’ openness in disclosing their experiences, particularly in a public setting. In addition, we did not assess socioeconomic status or other confounding factors that could influence the IPV-ART adherence relationship. Previous studies (e.g., Hatcher et al., 2019; Marinda et al., 2021) have demonstrated that these factors significantly influence ART adherence; therefore, their exclusion in the present study is a limitation. Future research should include these socioeconomic variables to better understand barriers to ART adherence among individuals experiencing IPV.
Conclusions and implications for practice
The study identified that all forms of IPV negatively impact ART adherence, with sexual IPV having the most pronounced effect. This highlights the urgent need for comprehensive strategies to address IPV, particularly through routine IPV screening and trauma-informed counselling, particularly for women. Despite South Africa’s policy advancements in addressing IPV and gender-based violence, implementation in primary health care remains insufficient. Strengthening the health system’s response through improved training, resources, and survivor-centred psychosocial services is essential to enhance ART adherence and health outcomes for PLWH.
Furthermore, men, younger individuals, and those with shorter HIV diagnosis durations were at higher risk of non-adherence, while older individuals and those with longer HIV histories demonstrated better adherence. Future research should explore demographic and socioeconomic factors influencing adherence, particularly among high-risk groups, to refine interventions. A multifaceted approach addressing both IPV and demographic disparities is critical for effectively addressing the social determinants of ART adherence in clinical practice.
Footnotes
Acknowledgements
We would like to extend our gratitude to the clinic staff at Nirvana Community Health Clinic and Diepkloof Provincial Hospital for assisting with the process of data collection, and to the participants for their information.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The corresponding author was a recipient of the University of South Africa Postgraduate bursary and the National Research Foundation free-standing scholarship for completion of the research.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to institutional ethics restrictions.