
Abstract
Introduction
As of 2018, out of the 21.2 million who needed substance treatment in the past year, only 3.7 million (17.5%) received any treatment (SAMSHA, 2020). Traditional treatment approaches are “acute” and short-term – they rely on isolated treatment episodes and brief biopsychosocial stabilization and medication (White, 2008). They are also professionalized – in that they primarily utilize health and mental health professionals to reduce substance use disorder and other psychiatric disorder symptoms. Since the 1970s, service delivery systems which have used this acute model have more of a business orientation, that is, they are short-term and designed to be time limited to respond to insurance payment systems.
This contrasts a newer perspective on recovery care models which emphasize long-term supports and recognizes many different pathways to recovery. Recovery care models – or “recovery management” are becoming more prominent as more secular, spiritual and religious mutual aid societies focus on addiction and recovery in the United States (Humphreys, 2003; Kyrouz et al., 1997; White, 2007). In fact, of the 22.4 million US adults who have resolved an issue with substance use disorder, half had taken advantage of these mutual aid societies (Kelly, Abry et al., 2019; Kelly, Bergman et al., 2017; Reddon & Kerr, 2020). Even within medical systems, there is also a growing understanding of chronic care and disease management which occurs over long periods of time (Donroe et al., 2020; Pincus & England, 2015).
There has also been a rise of recovery support services (i.e., case management/care coordination, employment, housing, family related services, along with 12-step groups), voucher based programming, and recovery care organizations (RCOs) which have gained inspiration from mutual aid societies and have become more mainstream because of funding mechanisms provided through SAMSHA, Rural Community Opioid Response Program, and other entitites (SAMSHA, 2010). This growth and diversity of recovery organizations essentially has led to a separate culture of recovery which has forced a re-evaluation of crisis-oriented, professionally-directed, acute care approaches, which emphasize isolated treatment episodes.
Individuals with substance use disorders also experience a variety of psychosocial problems which make sobriety more challenging, including financial problems and unemployment, criminal justice involvement, unstable housing and homelessness, and isolation from social support systems (Luchansky et al., 2000). These problems are also associated with lower treatment retention (Pickard et al., 2020; van den Berk Clark et al., 2021), and demand more wrap-around services and collaborative care models. Furthermore, individuals generally engage in a process of “recovery” when they are back in their home communities, which suggests that supports need to be located locally (Ashford et al., 2020). The challenges presented by acute care models thus have led to “recovery-oriented systems transformation” pilots in States like Connecticut and cities like Philadelphia. However, some states have utilized funds differently, and instead have focused on increasing consumer choice, reducing the prominence of “credentialed” professionals and establishing long-term support programs providing housing, emotional support, etc (Laudet & White, 2010).
In 2004, the Access to Recovery (ATR) initiative was established to expand access to recovery support services through SAMSHA's competitive grants to States, especially to underserved populations (e.g., pregnant women, rural dwellers, individuals involved in criminal justice systems) through voucher-based programs to increase choice (Krupski et al., 2009). Between 2004 and 2007, twenty-nine states received funding through the ATR mechanism. Grants required programming that was person-centered, provided individualized and comprehensive services across the lifespan, where systems were anchored within communities, offered integrated continuity of care programming, and were responsive to personal belief systems. By 2010, SAMSHA awarded 33 ATR grants to states and nonprofits to promote the implementation of recovery-oriented systems of care (ROSC), which essentially attempted to reduce program fragmentation (SAMSHA, 2010). These programs essentially attempt to frame recovery as a process of change whereby individuals overcome and manage their substance use disorder, get and maintain a stable and safe place to live, engage in meaningful daily activities which lead to independence and full participation in society, and have relationships and social networks which provide support and stability (SAMSHA, 2010, 2021).
According to SAMSHA, recovery programs are expected to be person-centered, respect diversity, and reduce health disparities both in access and in outcomes (SAMSHA, 2021). However, this does not bring much clarity to how funding towards recovery programs is spent and which programs tend to be implemented more widely in different states as a result of this funding. To better understand the recovery models and how they have been applied in real-world settings, this paper examines how recovery funding is dispersed at the State level and what recovery programs are being funding using SAMSHA's funding archive.
Methods
Data was collected from SAMSHA's funding archive (https://www.samhsa.gov/grants/archive). SAMSHA's funding archive includes all competitive grant annoucements and awards from 2001 through 2020. Authors identified grants for recovery-oriented programs, as follows: vouchers, peer support, 12-step programs, recovery training, recovery support services, recovery community organizations, drop-in centers, recovery-oriented systems of care, and integrated wrap around services. Data was collected on funding by year, state, and program.
Data Source
Data sources included the SAMSHA grant awards archive, which includes funding announcements and grant awards from SAMSHA from 2004–2021 (https://www.samhsa.gov/ grants/archive). These announcements provide information about amount of funding, the entity funded and requirements for funding. These grant awards are separated into three categories: (1) Center for Mental Health Services (CMHS), (2) Center for Substance Abuse Prevention (CSAP), and (3) Center for Substance Abuse Treatment (CSAT). Additional data was accessed from SAMSHA's state funding archive which only includes data from 2014 to 2021 (https://www.samhsa.gov/grants-awards-by-state).
Data Analysis
Funding was collected for each state, for each year and sparklines were created to show change in funding over time. Additional descriptive statistics were also collected, including total SAMSHA funding, population data and per-capita recovery funding (See measures section). A coding workbook was also developed which included the recovery programs listed in the previous section as well as additional program and project goals. Data were collected from 50 states and coders regularly debriefed to ensure agreement. A radial chart was developed using methodology described by Policy Viz at (https://policyviz.com/2019/12/04/the-radial-map/) (Schwabish, 2021) to show major recovery programs by state.
After recovery programs were identified, those implemented more than 50 times across the US were included into a latent class model. Latent class analysis was used because of the assumption that states used a combination of different programs to establish a recovery delivery system and that the grants for each program can be grouped into a smaller number of distinct clusters known as latent classes based on their profile of recovery program implementation and funding over the past 20 years. Latent class modeling aims to obtain the smallest number of clusters that accounts for all the association between the variables, in this case, between recovery programs implemented. These latent class models had two parts: the first fits probabilities of who belongs to which class and othe other describes the relationship between classes and the observed variables. The “gsem” command was used to examine grant awards (using logit) and grant amounts (log-link), along with year and state as predictors. To estimate statistics which show probabilities of class membership, we used the “estat lcprob” command, and to estimate mean for each item in each class, we used the “estat lcmean” command.
Measures
Funding. Funding includes all money received through federal competitive grants which requires that monies be spent on recovery programming. These funding mechanisms included the Access to Recovery funding mechanism and the Recovery Community Services Program (via CSAT). (SAMSHA) Funding was tracked from 2004–2020. Total state substance funding was also tracked from 2014–2021 and averaged.
States. State includes all US states and territories which received SAMSHA funding for recovery programs.
Type of Recovery Program. Recovery programs are defined as individualized – person-centered programs which are comprehensive, based within communities, responsive to diverse belief systems and perspectives and include all developmental stages (White, 2008). These include vouchers, peer support, 12-step programs, recovery training, recovery support services, recovery community organizations, drop-in centers, recovery-oriented systems of care and integrated wrap around services. If additional programs, interventions, or services were identified in the grant (see data analysis section), they were also included as text in the results section.
Results
A total of 482 grants focused on recovery programs were recorded since 2004 with an average of 9.3 ± 6.4 grants per state. Total funding was 425 million dollars with a mean amount of 8.2 ± 8.0 million dollars per state. Funding peaked between 2004 (at 106.2 million) and 2007 (98.7 million) and averaged 9.3 ± 11.5 million in subsequent years. From 2004–2020, about 32 of the states experienced lower levels of funding; 2010 and onward, 7 states recovery funding stayed about the same, while 15 states had increased recovery funding after 2010 (See Table 1).
Total Funding by State for Recovery Programs 2004–2020 in Millions.
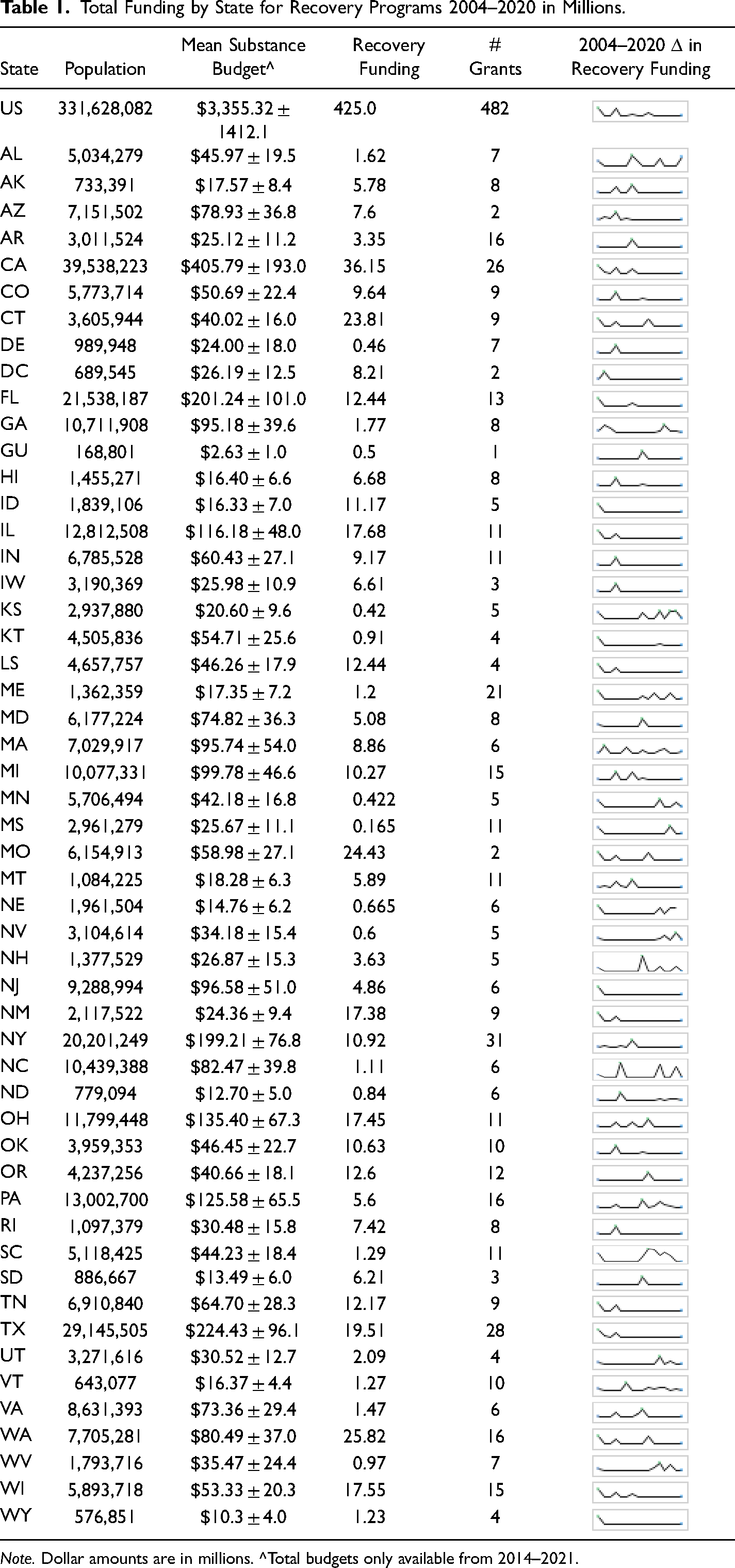
Note. Dollar amounts are in millions. ^Total budgets only available from 2014–2021.
The 10 states which received the highest amount of per-capita funding were DC ($11.9 million), New Mexico ($8.2 million), Alaska ($7.8 million), South Dakota ($7.0 million), Rhode Island ($6.8 million), Connecticut ($6.6 million), Idaho ($6.1 million), Montana ($5.4 million), Hawaii ($4.6 million) and Missouri ($4.0 million). The 5 states which received the lowest amount of per-capita funding were Mississippi ($0.05 million), Minnesota ($0.07 million), North Carolina ($0.1 million), Kansas ($0.14 million) and Georgia ($0.17 million). Funding was more generous to established voucher-based programs.
Funding overall for SAMSHA programs averages 3.4 billion per year with states averaging about 63.3 ± 29.1 million per year (See Table 1). Funding specifically allocated toward recovery programs is a very small percentage of this funding. For the US, per capita funding for SAMSHA programs is $666.0 ± 4.0 per year. Recovery funding from 2004–2020 (16 years) is $1.28 per capita. States with the highest per capita funding were Georgia ($563.8 ± 3.7), Pennsylvania ($114.4 ± 5.0), North Carolina ($105.9 ± 3.8), Wisconsin ($92.4 ± 3.4), California ($70.3 ± 4.9), Texas ($68.6 ± 3.3), Alabama ($62.7 ± 3.9), Missouri ($54.4 ± 4.4) and South Carolina ($49.9 ± 3.6). States with the lowest per capita funding were Arkansas ($0.64 ± 3.7), North Dakota ($1.08 ± 6.4), New Mexico ($1.21 ± 4.4), DC ($1.22 ± 18.2), Idaho ($1.27 ± 3.8), Vermont ($1.90 ± 6.9), South Dakota ($1.95 ± 6.7), Tennessee ($2.22 ± 4.1), Alaska ($2.46 ± 11.5) and Maine ($2.81 ± 5.3).
Voucher based programs and recovery support services received the most funding overall with voucher-based grants being about $290.2 million and recovery support services being about $355.3 million (See Supplementary Table 1). Voucher-based grants, although relatively large (Mean = 4.0 ± 1.7 million), were only offered for three years (2004, 2007, and 2010), while recovery support services were offered every year from 2004–2020. After 2013, funding shifted toward focusing on a combination of recovery support services ($39.6 million) and peer support services ($32.4 million). Additional programs that were identified in funding announcements included data collection/quality improvement, involvement of the broader community, advocacy efforts, family network services/family support, consumer driven programs, culture change, workforce development, evidence-based practices, program expansion, infrastructure support/expansion, vocational rehabilitation, faith-based programs, support for veterans, expanded access to behavioral health services, building leadership, improvement of treatment capacity and “systems of care.” Figure 1 shows implementation of programs across all 50 states.
Latent class models were fitted successively, starting with a one-cluster model (whereby it is assumed that all states implement the same combination of progrmas) and then adding another cluster for each successive model. Indictors of LCA were implementation of and funding for Vouchers, Peer Support, Interagency Networks, Recovery Support Services, Recovery Care Organizations, Recovery Oriented Systems of Care, Family Network Servcies/Family Support, Consumer Driven Programs, Program Expansion, Infrastructure Support, Vocational Rehab, Faith Based Programs, Behavioral Healht Services, Building Leadership and Improved Treatment Capacity. LCAs specified 2–5 classes. The best fitting model, as indicated by BIC for recovery program implementation was the four class model and for funding received was the three class model. As shown in Table 2, this model included the following: (a) Peer focused (Pr (Class) = 0.09, 95%CI = 0.08, 0.10) – funding focused on organizations and programs which emphasized peer support which included peer support and recovery support services, (b) Treatment focused (Pr (Class) = 0.14, 95%CI = 0.12, 0.18) – funding appeared to be used for acute treatment – with a focus on program expansion, behavioral health services and treatment capacity. This funding tended to be associated with also receiving funding for faith based groups, (c) System focused (Pr (Class) = 0.57, 95%CI = 0.54, 0.59) – funding included many more different types of recovery programs in order to build a more comprehensive system of care, and (d) Consumer focused (Pr (Class) = 0.19, 95%CI = 0.17, 0.21) – this funding was similar to the treatment focused class but also included consumer focused funding and programs.
Latent Class Margins of Grants Fundings Programs.
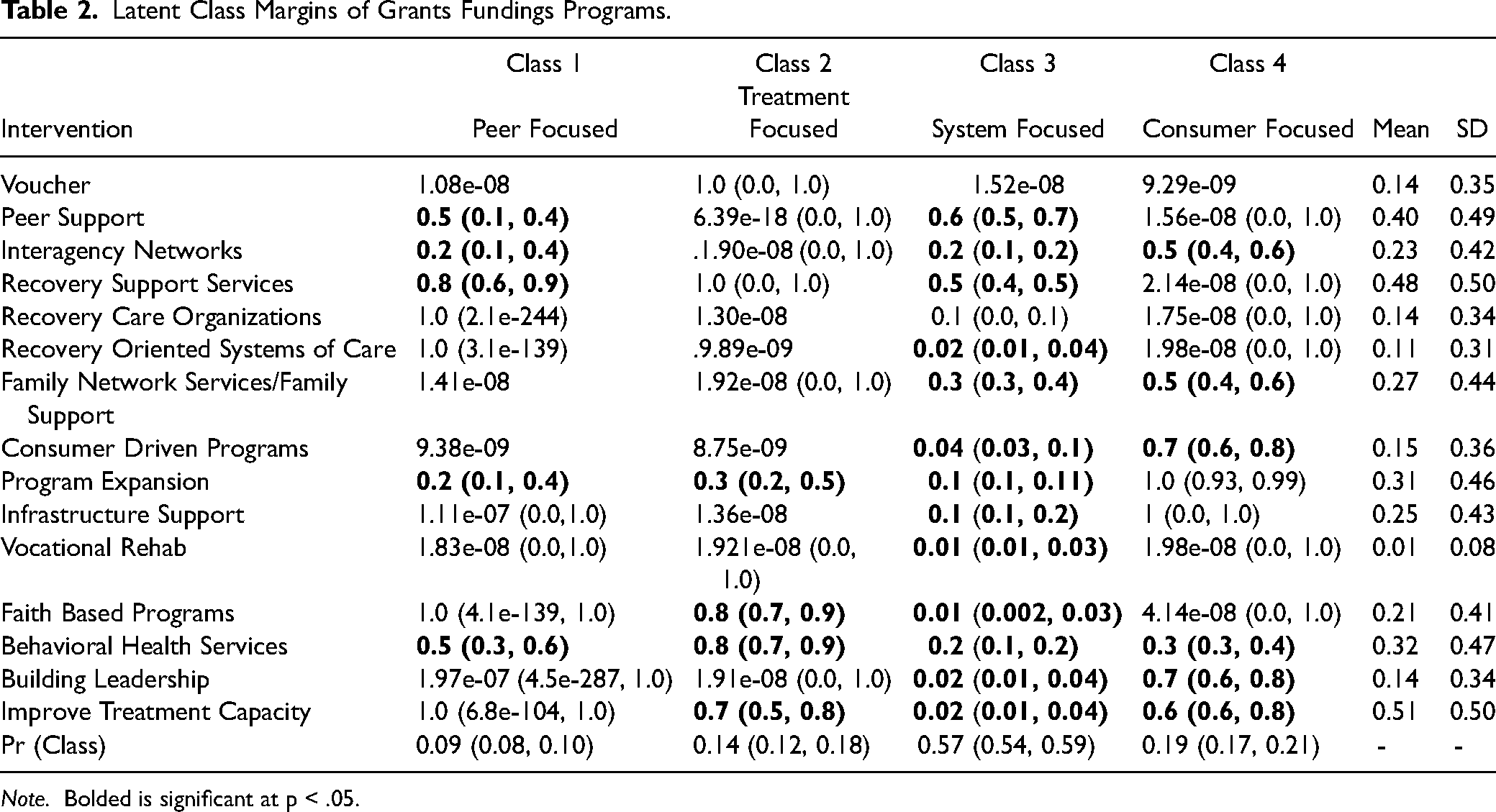
Note. Bolded is significant at p < .05.
When grant amount was used instead of grant receipt, the best model indicated three classes. These classes (as shown in the Supplementary Table) are different than award type, as follows: (a) Interagency focused (Pr(Class) = 0.21, 95%CI = 0.18, 0.24) – funding focused specifically on a combination of interagency and infrastructure support, (b) Recovery support focused (Pr(Class) = 0.66, 95%CI = 0.63, 0.69) – funding still included interagency networks but also included recovery support services, recovery care organizations and family network services, and (c) Voucher and Faith Based Focused (Pr (Class) = 0.13, 95%CI = 0.11, 0.17)– whereby much funding was allocated toward voucher programs, recovery support services and program expansion which also included faith-based and behavioral health services.
Discussion
Just about every state took advantage of recovery funding from 2004–2008, with a total of about $400 million being distributed. Mean grant amount and number of grants varied substantially, and some states decided to take advantage of some recovery program opportunities (like vouchers or ROSC programs) where others did not. Overall, this paper revealed three items of note: (1) that voucher programs stopped being used after 2010, (2) that recovery service systems programs remained the most popular, lasted the longest, and attained the most funding and (3) the ROSC programs – although promising because the model sought to change how treatment delivery was structured to ensure long-term services for individuals with substance use issues – was only accepted by about half of the states.
In 1996, as part of welfare reform legislation, Congress inserted a provision known as “Charitable Choice” into welfare-to-work legislation, the community service block grant program, the Children's Health Act and SAMSHA substance treatment programs (Kennedy, 2003). These programs were developed to ensure that faith-based organizations would also be eligible for state contracts and be able to deliver services because they are often closer to communities, have untapped resources, and are often prevented from traditional government contracts because of “unnecessary barriers” (Kennedy, 2003). These provisions also allowed these organizations to retain their religious identity which sometimes allowed them to connect with individuals on a spiritual level.
These efforts were expanded in the Bush era through a series of executive orders which included White House offices of Faith-Based and Community Initiatives and reduced regulatory barriers to accessing nonprofit status. Funding to faith-based organizations, as a result, increased by 40% between 2003–2007 (White, 2009). In 2004, the administration developed the Access to Recovery (ATR) program to enable individuals with substance use issues to have a choice between faith-based and secular substance treatment providers via the use of vouchers to individuals (Krupski et al., 2009). ATR also provided recovery support services ensuring that many charitable organizations could also contribute to substance treatment, even when they did not employ professional staff.
Nonetheless, the voucher-based programs failed to expand the use of faith-based organizations in substance use treatment because many faith-based organizations lacked organizational capacity to complete successful grant applications or meet documentation requirements, get licenses or even meet regulatory requirements to be eligible for grants (Kramer et al., 2005). A bigger problem though, is the assumption that faith and religion go hand-in-hand with recovery. Legal restrictions on prohibitions of proselytizing made it difficult for faith-based organizations to separate religious services from evidence-based practices and reduced the potential to ensure that participation with religious service was, in fact, voluntary (Kramer et al., 2005).
Regardless, the ATR program was instrumental in ensuring that recovery-focused programs gained greater prominence, in comparison to existing clinical and medical services (Gaumond & Whitter, 2013). ATR also expanded the service menu and ensured that long-term social services were also provided to deliver continuum of care for individuals with substance use disorders (Krupski et al., 2009). This led to the establishment of networks between service providers to better respond to substance abuse in the long term (Gaumond & Whitter, 2013; Kramer et al., 2017). It was also necessary given cuts in social service funding when Aid to Families with Dependent Children was replaced by Temporary Assistance to Needy Families (Bentele & Nicoli, 2012).
Also of interest was the take-up of ROSC programs by states. As mentioned previously, ROSC programs use “recovery” as a type of organizing construct for the substance treatment and prevention delivery system (White, 2008). ROSCs essentially are coordinated networks of community-based stakeholders who ensure that individuals with substance use issues have the services and supports that they need and that those services are person-centered and strengths-based (SAMSHA, 2010). The mission of ROSCs is to ensure long-term recovery where individuals not only achieve abstinence but also improved health, well-being, and quality of life (White, 2007). The model emphasizes chronic treatment over acute treatment, local recovery communities over professional organizations and experts, leadership by clients of services rather than administrators, and access to a broad range of social services over long periods of time to ensure stable recovery (White, 2008).
Meanwhile, the current political economy of substance treatment delivery systems, just like health and mental health delivery systems, has shifted significantly since even the 1990s when most of these strategies were developed. Privatization of social services in the 1980s meant that States issued RFPs and treatment organizations had the opportunity to compete for contracts to provide treatment (Smith, 2010). Over time, larger organizations with more capacity were able to be more competitive, and the state often just renewed contracts. These organizations also had longstanding ties to government and their previous informal arrangements led to more formal contracts. As a result, a smaller group of organizations often dominated the service-delivery systems and many other smaller organizations either brutally competed for smaller amounts of money or attempted to work with or merge with the larger organization on their terms (Smith & Mogro-Wilson, 2008).
When funding levels for substance abuse, as well as a host of other social service programs, were cut substantially in the mid 1980s and continued to be cut through the 1990s, organizations shifted their fundraising to Medicaid and other state level health subsidies (Smith, 2010). Many substance treatment organizations could also rely on fees or private insurance, so many adopted more of a medical and business approach (Kimberly & McLellan, 2006). It is important to note here that federal, state, and local level insurance have their own regulatory requirements and performance measures in order to reduce fraud, improve outcomes, and reduce costs more generally (Smith, 2010). These requirements and measurements created organizational constraints, most notably, in substance use disorder treatment, because they required medical and mental health professionals to provide time-limited services. They also seemed to align with funding mechanisms via SAMSHA which highlighted interagency organizational changes, increased behavioral health services and program expansion.
Given a political economy where treatment is medicalized, treatment is highly specialized and segregated from other health and social services systems, addiction counseling is professionalized, programs and institutions have a business orientation (i.e., profit, and reimbursable care more important than recovery), communities of recovery are disconnected from treatment very large research institutional wield power over smaller organizations in a political economy, and service delivery systems are fragmented, it is no wonder that many states have not adapted ROSC systems or ensured they were used on a statewide basis (Gray et al., 2015; White, 2008). ROSC systems which are larger and include statewide partners have the capacity to reduce the institutional leverage of many of the treatment providers who through dominating treatment systems and consistently winning contracts for many years, also reduce competition and ensure a business and medical approach to treatment instead of a long-term, person-centered approach.
The use of recovery models in the delivery of effective substance prevention and treatment is both intriguing and necessary given the chronic nature of substance use disorders. However, more needs to be known about the scale, efficacy, and complications of these programs and program implementation. This study was limited because it only was able to evaluate federal competitive funding mechanisms to States, counties, or nonprofits. There is less information about how discretionary funding is distributed through single-state agencies or funding provided through other federal or state sources. Also, more needs to be known about organizational constraints of implementing interventions utilizing recovery models and ROSC expansion and sustainability. Future studies should explore the implementation, sustainability and reach of recovery programs, especially as they relate to the opioid epidemic.
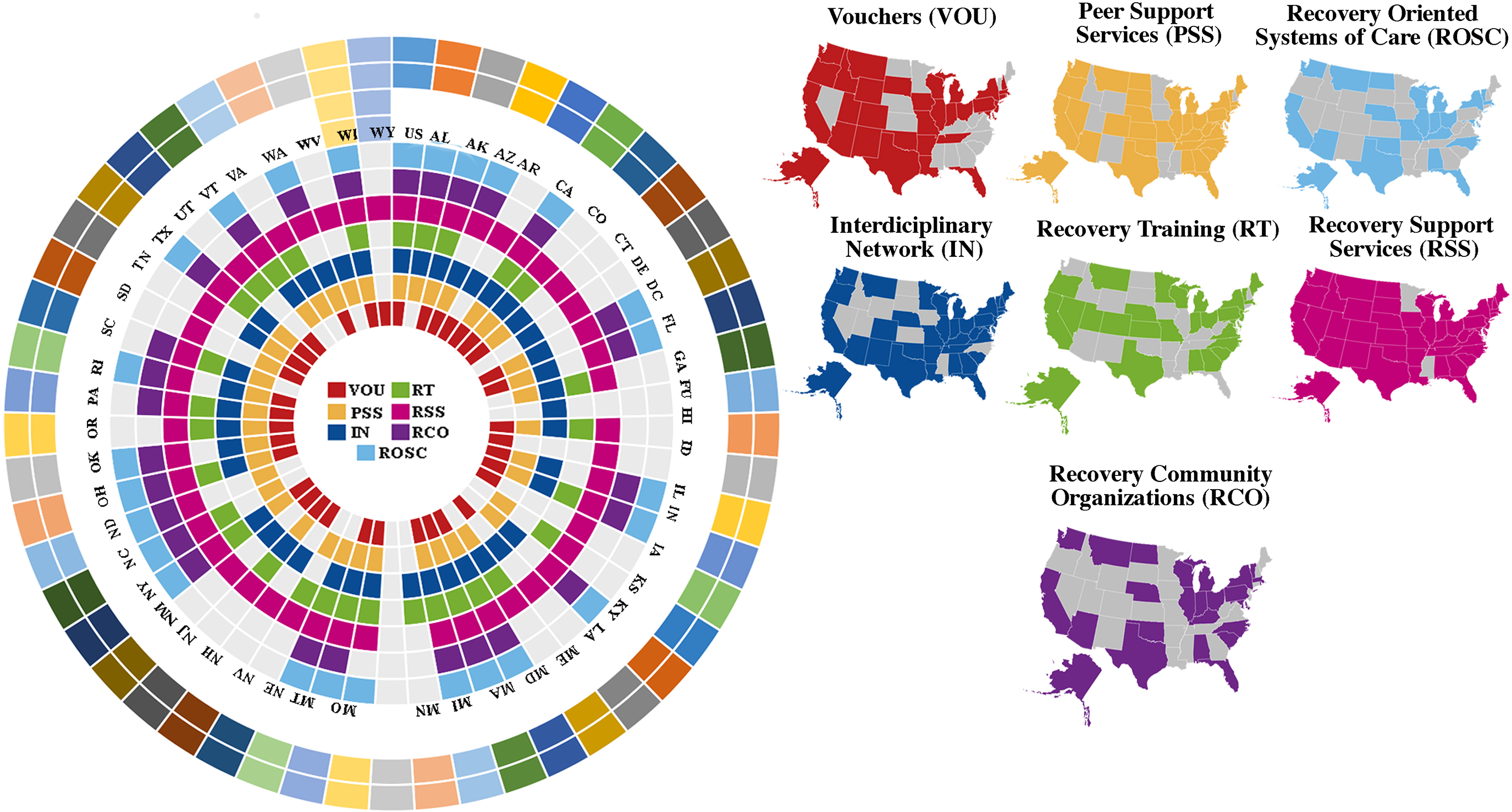
Recovery program take up by state 2004–2020.
Supplemental Material
sj-docx-1-dre-10.1177_00472379231217830 - Supplemental material for Funding and Implementation of Recovery Oriented Treatment Programs in the US from 2006–2020
Supplemental material, sj-docx-1-dre-10.1177_00472379231217830 for Funding and Implementation of Recovery Oriented Treatment Programs in the US from 2006–2020 by Carissa van den Berk-Clark, Margarita Fedorova, Emily Duncan, Tiffany Ju and Joseph Pickard in Journal of Drug Education
Supplemental Material
sj-docx-2-dre-10.1177_00472379231217830 - Supplemental material for Funding and Implementation of Recovery Oriented Treatment Programs in the US from 2006–2020
Supplemental material, sj-docx-2-dre-10.1177_00472379231217830 for Funding and Implementation of Recovery Oriented Treatment Programs in the US from 2006–2020 by Carissa van den Berk-Clark, Margarita Fedorova, Emily Duncan, Tiffany Ju and Joseph Pickard in Journal of Drug Education
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under U77HP03042 entitled “MAHEC 2017–2022: A Statewide Network for Interprofessional Health Care Workforce Development and Practice Transformation in Rural and Underserved Missouri” and the Saint Louis University Drs. Mary Susan and Robert Heaney Primary Care Research Fund. This information or content and conclusions are those of the author(s) and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the U.S. Government.
Supplemental material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.