
Abstract
China required regions to expand outpatient benefit package since 2021, but whether it may induce moral hazard among non-chronic disease patients remains undetermined. We aimed to clarify effects of expanding outpatient benefit package on health-seeking behaviors, medical expenses and reimbursement of people without chronic disease. This study employed segmented regression of interrupted time series, utilized 5 765 419 non-chronic disease patients’ medical services records from January 2021 to December 2023 in Guangzhou, to analyze influence of expanding outpatient benefit package on non-chronic disease patients. (1) For health-seeking behaviors: monthly medical visits (β1 + β3=0.0069, P = .001) and the monthly number of outpatient visits (β1 + β3=0.0066, P = .001) exhibited a significant increasing long-term trend. This corresponds to significant annual increases of 0.08 per person in both medical and outpatient visits. (2) For medical expenses: the monthly outpatient medical expenses showed a significant upward trend (β1 + β3 = 6.9308, P = .002), which was equivalent to a significant increase of 83.17 yuan in outpatient medical expenses per person per year. (3) For expenditures of basic medical insurance funds: expenditure of basic medical insurance funds on outpatient medical services were significantly higher than pre-intervention levels by 35 yuan (β3 = 2.9169, P = .036), with a sustained significant growth rate of 52.51 yuan per person per year (β1 + β3 = 4.3762, P = .004). Monthly outpatient out-of-pocket expenses exhibited a significant instantaneous decrease of 135.27 yuan (P < .001), followed by a significant upward trend (β1 + β3 = 2.5562, P = .038), corresponding to an annual increase of 30.67 yuan per person. Within well-designed payment models, expanding outpatient benefit package among patients without chronic disease could enable them to get a more comprehensive and prompt treatment while total medical expenses and expenditure of the basic medical insurance funds are stable totally.
Keywords
Introduction
Outpatient services, as the cornerstone of modern healthcare systems, play a critical role in early disease screening, primary diagnosis and treatment, chronic disease management and patient education, which is essential for optimizing medical resource allocation and reducing societal disease burdens.1,2 In China, over 90% of all medical services are delivered through outpatient care (China Health Statistics Yearbook (2016-2023) shows annual outpatient visits accounted for 93.60% of the total medical visits on average). Against the backdrop of socioeconomic progress, demographic aging, transformation of spectrum of disease and medical technology innovations, the demand for outpatient services among China’s insured populations has become increasingly prominent compared to inpatient care in recent years. According to China Health Statistics Yearbook, from 2015 to 2020, outpatients’ per visit medical cost grew at an annual average rate of 6.79%, surpassing the 5.14% annual growth rate of inpatients’ per admission medical costs during the same period. However, owing to limited pooled funds and management capacity, the Chinese social health insurance system (SHI) only reimbursed the hospitalization expenses while outpatient expenses were predominantly settled through out-of-pocket payments or individual medical savings accounts in the early years. Along with advancement of China’s health care system reform, several regions attempted to make some compensation for outpatient costs of some chronic conditions like diabetes and hypertension. But it still couldn’t change the fact that the reimbursement for outpatient expenses was relatively low, 3 especially compared with inpatient care, which may discourage people from utilizing outpatient services, even inducing unjustified hospital admissions.4,5 To deal with these problems, the Chinese government issued the Guidelines on Establishing a Mutual-Aid Outpatient Guarantee Mechanism for Urban Employee Basic Medical Insurance in April 2021, requiring regions to set up a pooling mechanism for costs of general outpatient services formally so as to further relieve medical financial burdens. Subsequently, all regions set out to expand their own benefit package for outpatient services one after another in response to national requirements.
Theoretically, expanding outpatient benefit package could help to alleviate patients’ economic burden, take unmet medical needs of outpatient services and mitigate previously prevalent unjustified hospitalization demands stemming from inadequate compensation for outpatient services.6,7 Meanwhile, it enables patients to receive timely treatment that prevents minor illnesses from developing into serious conditions.8 -10 As a result, patients’ health outcomes improve while their medical expenses are reduced, with savings realized in the expenditure of the basic medical insurance funds,11,12 which aligns fundamentally with principles of cost-effectiveness. 13 These hypotheses have been substantiated by ample evidence in prior researches. For example, Du et al 14 and Liu et al 15 found expanding outpatient benefit package for diabetes outpatient care will make patients have a more rational health-seeking behaviors, a better health status while total medical expenses and expenditure of the basic medical insurance funds decrease at the same time. Similar conclusions also emerge in researches examining the impacts of polishing up outpatient coverage on hypertensive and neoplastic disease cohorts (He et al 4 ; Jiang et al 16 ).Nevertheless, some scholars have raised objections to this position. On the one hand, the current evidence for outpatient benefit package enhancements centers overwhelmingly on chronic disease populations, leaving influence on acute or episodic care patients largely unstudied. Considering the significant disparities in utilization patterns of outpatient services between these 2 cohorts,17,18 whether existing findings are generalizable to people without chronic conditions remains uncertain. On the other hand, at present the financing mechanism for outpatient pooled funds of Urban Employee Basic Medical Insurance—which reallocates premiums from individual medical savings accounts—may incentivize moral hazard in non-chronic disease populations through excessive service utilization, 19 ultimately bringing about inefficient resource use and unnecessary claims on the basic medical insurance funds. Official statistics from China Medical Security Statistical Yearbook,2024 show that there were 2.18 billion outpatient visits obtaining the claims in 2023, representing a 23.86% year-over-year increase that notedly exceeded the growth rate of 2.15% in 2022. Does the blowout growth in outpatient utilization involve unreasonable or inappropriate service use? No scholarly consensus has been established on this matter to date.
Given the unresolved contention, this paper employs China’s unified medical insurance claims database—with complete health service utilization records for all enrollees—to examine the following questions via an interrupted time-series regression analysis: (1) Will expanding outpatient benefit package affect non-chronic disease populations’ health-seeking behaviors and medical expenses? (2) Does expanding outpatient benefit package for non-chronic disease populations lead to accelerated growth of expenditure of the basic medical insurance funds and induce moral hazard?
Methods
Changes in Policy and Data Overview of the Sample Region
Changes in Policy of the Sample Region
Prior to December 2022, the outpatient benefit package for Urban Employee Basic Medical Insurance in Guangzhou, Guangdong Province, China was structured as follows: all eligible outpatient expenses incurred by the insured were reimbursable through the basic medical insurance funds according to a unified standard. No deductible applied for outpatient visits. For outpatient services delivered at community health service centers, pooled funds covered 80% of expenses, otherwise 55%. The reimbursement cap line for outpatient services was RMB300 per month.
After December 2022, Guangzhou optimized its outpatient benefits on the basis of the original system aforementioned. No modifications was made to the deductible. For outpatient services delivered at community health service centers, pooled funds cover 80% of expenses, otherwise 65%. But for retirees, the coverage percentage above mentioned increased by 5%. The reimbursement cap line for outpatient services now is RMB7200 per year and for retirees is RMB10 100 per year.
Details of Sample Data
Since 2021, there were no major policy change in Urban Employee Basic Medical Insurance for inpatient services in Guangzhou. And for outpatient services, the only reform was improving its outpatient benefits as mentioned before. To ensure the accuracy of results, this study chose to make use of detailed information concerning enrollees’ healthcare services from 2021 to 2023. As a retrospective study, the insured are divided into chronic disease cohorts and non-chronic disease cohorts by Guangzhou Healthcare Security Administration according to an official document which listed chronic disease with their identification criteria at the beginning of each year.
Therefore, we adopted a fixed cohort design. Specifically, we first identified all unique individuals who were registered in the chronic disease database in any year from 2021 to 2023, obtaining a union set of 1 070 173 chronic disease patients. This set of patients was then entirely excluded from all individuals who had outpatient visits during the 3-year period.
Finally, a total of 5 765 419 non-chronic disease patients were fully included in this study, which could avoid retrospective bias due to the use of survey data or sampling data and help improve the accuracy of the study results. The detailed data included all the medical visits records of both outpatient services and inpatient services utilized by non-chronic population within 3 years, whose amount were 59 767 971 records, including 58 605 421 outpatient records and 1 162 550 inpatient records. The claims database contained individual information (beneficiary ID, gender, age), medical institution information (name, level, type of institution), medical visit information (admission date and discharge date, outpatient service or inpatient service, disease diagnosis and disease code) and expenses information (total medical expenses, outpatient expenses, inpatient expenses, out-of-pocket expenses, expenditure of the basic medical insurance funds; Supplemental Additional File 1).
Study Model
Interrupted Time Series Analysis(ITSA)
Interrupted time series analysis (ITSA) has been proven to be the most effective quasi-natural experiment design for evaluating policy intervention effects.20,21 In this study, the breakpoint was set on December 1st, 2022 when improving outpatient benefit was officially executed in Guangzhou as an intervention point of the policy.
Variable Selection
The dependent variables (Yi) in this study included non-chronic disease patients’ health-seeking behaviors, medical expenses, expenditure of the basic medical insurance funds for them, which spanned 36 months from January 2021 to December 2023. See Table 1 for specific indicators of variables and their descriptions.
Specific Indicators of Variables and Their Interpretation.

Statistical Analysis
We employed segmented regression of interrupted time series to analyze policy impacts on 13 dependent variables metrics. The intervention occurred in December 2022, which coincided with the lifting of “Zero-COVID” policies and a subsequent surge in COVID-19 infections. To address these concurrent events, we included the natural logarithm of the monthly count of confirmed COVID-19 cases as a covariate. Furthermore, to account for seasonal patterns in healthcare utilization, particularly the increase in respiratory illnesses in winter, we controlled for seasonal effects using third-order Fourier terms in the models, which provided the best fit and were thus selected for the primary analysis. The model was set as follows:

Here, Yt represents 13 dependent variables at time t; Tt is a continuous variable counting the number of months at time t from the start of study, assigned values 0 to 35 for the period January 2021 to December 2023. X1t is an indicator for time t occurring before or after improving outpatient benefit, which was implemented at month 23 in the series (December 2022); X1tT1t is a continuous variable counting the number of months at time t after the reform (0 before the reform and 1―13 after the reform).
For parameters, β0 estimates the baseline level of the outcome at time zero; β1 estimates the baseline trend of the outcome before the reform; β2 estimates the level change in the outcome immediately after the reform; β3 assesses the post-intervention trend slope change. Thus, β1 + β3 can be used to evaluate the long-term trend of change following policy implementation.
All analyses and figures were produced using Stata 17. The Durbin–Watson (DW) test was applied to assess autocorrelation, as its absence is an assumption in interrupted time series analysis. A DW value close to 2 suggests no autocorrelation. Since autocorrelation was detected in some cost components, we employed the Newey–West estimator to fit the regression models, which provides consistent standard errors in the presence of autocorrelation and heteroskedasticity. We used the SQUIRE writing guide when drafting this article, and the SQUIRE checklist (Supplemental Additional File 2) to demonstrate adherence to the SQUIRE reporting guideline.
Results
Health-Seeking Behaviors
The regression results indicated that (Tables 2 and 3 and Figure 1) the monthly number of medical visits (β1 = −.0004, P = .641), the monthly number of outpatient visits (β1 = −.0005, P = .515), the monthly number of hospitalizations (β1 = −.0005, P = .003), and the monthly average length of a hospital stay (β1 = −.0197, P = .562) all exhibited a declining trend prior to the policy intervention. However, a transient increase occurred at the point of policy intervention. Specifically, the monthly number of medical visits increased significantly by 0.0982 (P < .001), the monthly number of outpatient visits increased significantly by 0.1014 (P < .001) and the monthly average length of stay per capita increased significantly by 0.7919 days (P = .039). The monthly number of hospitalizations per capita also increased (0.003, P = .430), but this change was not statistically significant.
Parameter Estimate (P value) in Segmented Regression Model.

Note. All monetary values are in Chinese yuan (¥). The model controls for seasonal effects and the number of COVID-19 cases. The complete set of control variables and seasonal coefficients are reported in Supplemental Additional File 5. Bold entries represent that the variables of concern are significant.
Significance levels: *P < .05, **P < .01, ***P < .001.
Annual Changes in Key Estimated Values of the Interrupted Time Series Analysis (ITSA) Model.

Note. Significance levels: *P < .05, **P < .01. All monetary values are in Chinese yuan (¥).

(a) Monthly number of medical visits, (b) monthly number of outpatient visits, (c) monthly number of hospitalizations, and (d) monthly average length of a hospital stay.
After the policy intervention, the changes in the utilization frequency of medical services (β3 = .00724, P = .001), the changes in the frequency of outpatient visits (β3 = .00724, P = .001), and the changes in the frequency of hospitalization (β3 = .0012, P = .002) all showed a significant upward trend compared with those before the policy intervention, while there was no significant change in the changes of hospitalization days (β3 = −.0454, P = .065).
Regarding the long-term trend (β1 + β3), both the monthly number of medical visits (β1 + β3=0.0069, P = .001) and the monthly number of outpatient visits (β1 + β3=0.0066, P = .001) exhibited a significant increasing long-term trend. This corresponds to a significant increase of 0.08 in the annual number of medical visits per person and a significant increase of 0.08 in the annual number of outpatient visits per person. In contrast, the long-term trends for the monthly number of hospitalizations (β1 + β3=0.0001, P = .08) and the monthly average length of a hospital stay (β1 + β3=-0.0652, P = .172) were not statistically significant.
Figure 1a to d ITS analysis of changes in health-seeking behaviors among non-chronic disease patients
Medical Expenses
As shown in Tables 2 and 3 and Figure 2, prior to the policy intervention, both the monthly medical expenses (β1 = 4.6265, P = .026) and the monthly outpatient medical expenses (β1 = 4.0928, P < .001) showed a significant upward trend, while the monthly inpatient medical expenses showed a significant downward trend (β1 = −68.1639, P < .001). At the time point of the policy intervention, the instantaneous changes in the monthly medical expenses (β2 = −17.9679, P = .784), the monthly outpatient medical expenses (β2 = 29.1526, P = .112), and the monthly inpatient medical expenses (β2 = −385.2676, P = .478) were not statistically significant.

(a) Monthly medical expenses, (b) monthly outpatient expenses, and (c) monthly inpatient expenses.
After the policy intervention, the monthly outpatient medical expenses showed a significant upward trend (β1 + β3 = 6.9308, P = .002), which was equivalent to a significant increase of 83.17 yuan in the outpatient medical expenses per person per year. In contrast, the monthly inpatient medical expenses showed a downward trend (β1 + β3 = −44.1095, P = .401), and the monthly medical expenses also showed an upward trend (β1 + β3 = 5.6618, P = .344), but neither of these 2 changes was statistically significant.
Figure 2a to c ITS analysis of changes in medical expenses among non-chronic disease patients
Expenditure of the Basic Medical Insurance Funds
As shown in Tables 2 and 3 and Figure 3, prior to the policy intervention, monthly expenditure of the basic medical insurance funds on medical services exhibited a non-significant upward trend (β2 = 1.8467, P = .138). The monthly expenditure of the basic medical insurance funds on outpatient medical services increased significantly (β2 = 1.4592, P < .001), while monthly expenditure of the basic medical insurance funds on inpatient medical services decreased significantly (β2 = −41.7685, P < .001).

(a) Monthly expenditure of the basic medical insurance funds on medical services, (b) monthly expenditure of the basic medical insurance funds on outpatient services, and (c) monthly expenditure of the basic medical insurance funds on inpatient services.
At the intervention point, there was a significant instantaneous increase in the monthly expenditure of the basic medical insurance funds on medical services, with an increase of 144.8301 yuan (P = .001). The monthly expenditure of the basic medical insurance funds on outpatient medical services also increased significantly and instantaneously by 164.3459 yuan (P < .001). Although the monthly expenditure of the basic medical insurance funds on inpatient medical services increased by 136.8689 yuan, this change was not statistically significant (P = .717).
Following the intervention, annual expenditure of the basic medical insurance funds on outpatient medical services were significantly higher than pre-intervention levels by 35 yuan (β3 = 2.9169, P = .036), with a sustained significant growth rate of 52.51 yuan per person per year (β1 + β13 = 4.3762, P = .004). In contrast, monthly expenditure of the basic medical insurance funds on inpatient services showed a decreasing trend (β1 + β13 = −42.6554, P = .243), while the monthly expenditure of the basic medical insurance funds on medical services exhibited an upward trend (β1 + β13 = 3.0967, P = .413), neither trend was statistically significant.
Figure 3a to c ITS analysis of changes in expenditure of the basic medical insurance fund among non-chronic disease patients
The results in Tables 2 and 3 and Figure 4 show that before the policy intervention, both the monthly out-of-pocket expenses (β1 = 2.8420, P = .001) and the monthly outpatient out-of-pocket expenses (β1 = 2.6277, P < .001) showed a significant upward trend, while the monthly inpatient out-of-pocket expenses showed a significant downward trend (β1 = −19.5738, P = .002).
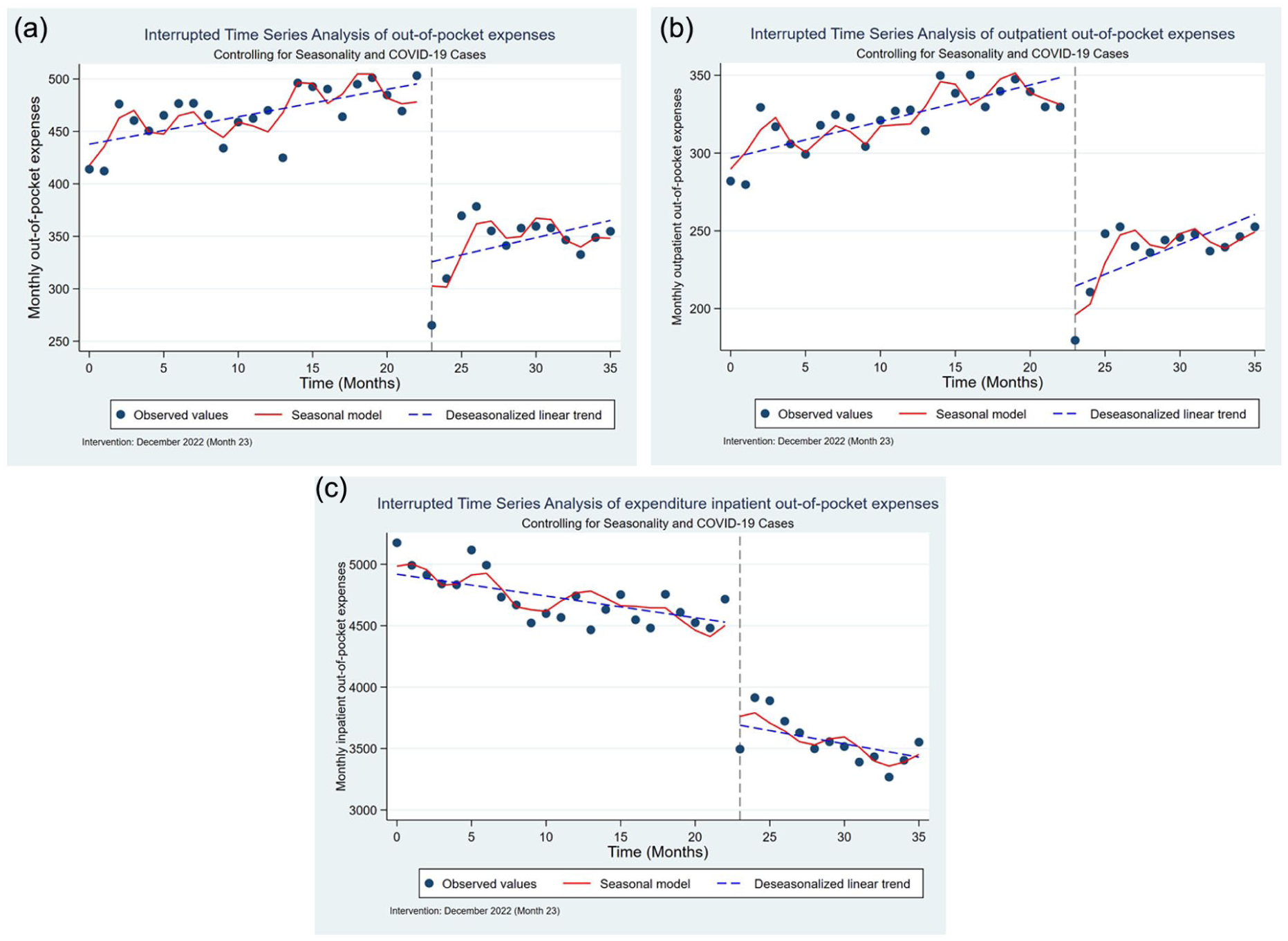
(a) Monthly out-of-pocket expenses, (b) monthly outpatient out-of-pocket expenses, and (c) monthly inpatient out-of-pocket expenses.
At the time of policy intervention, the monthly out-of-pocket expenses of patients decreased significantly instantaneously, with a decrease of 170.5311 yuan (P < .001); the monthly outpatient out-of-pocket expenses also decreased significantly instantaneously by 135.267 yuan (P < .001); the monthly inpatient out-of-pocket expenses also decreased significantly instantaneously by 837.0642 yuan (P < .001).
After the policy intervention, the monthly outpatient out-of-pocket expenses showed a significant upward trend (β1 + β13 = 2.5562, P = .038), that is, an increase of 30.67 yuan per person per year. In contrast, the monthly inpatient out-of-pocket expenses showed a downward trend (β1 + β13 = −12.901, P = .397). Although the monthly out-of-pocket expenses showed an upward trend in the long-term (β1 + β13 = 2.2111, P = .228), neither of them reached the level of statistical significance.
Figure 4a to c ITS analysis of changes in out-of-pocket expenses among non-chronic disease patient
Sensitivity Analysis
The study excluded the period from December 2022 to March 2023 (the peak of the pandemic) and re-evaluated the impact of policy interventions. The results show that the overall results remain robust. The results after the sensitivity analysis are presented in the Supplemental Documents (Additional File 3).
Discussions
The empirical results of this study indicated that expanding outpatient benefit package can facilitate non-chronic disease patients to make more use of medical services. Previous researches showed that insufficient security for outpatient expenses may result in pent-up demand for outpatient care among chronic disease patients, 22 whereas optimizing benefit package motivates proactive utilization of ambulatory services. 23 Our findings provide robust evidence that non-chronic disease cohorts exhibit same behavioral responses. But different from former conclusions on chronic disease population—where improved outpatient access reduces hospital utilization24,25 —our study yielded a somewhat counterintuitive finding that a reduction in outpatient out-of-pocket costs was associated with a higher hospitalization frequency for non-chronic disease patients, coupled with a decrease in their average length of stay. This phenomenon could be attributed to the increased outpatient volume, which potentially enables medical institutions to engage in “subthreshold admission” (a term used in China for unnecessary hospitalization), a financially motivated practice to secure higher income (Supplemental Additional File 4).
Generally speaking, increased healthcare utilization will bring about rising medical costs. However, results of this study revealed that through non-chronic disease patients added their monthly number of medical visits, there was no significant change in their monthly total medical expenses. As mentioned earlier, expanding the outpatient benefit package could encourage patients to actively utilize outpatient services, thereby facilitating early disease detection and intervention, which in turn helps prevent disease progression and save subsequent medical expenditure. Because of this, patient’s health status improves and the rapid growth of medical expenditure are restrained. What’s more, there are literatures demonstrating that when China’s annual practical outpatient reimbursement rate falls within the 42.27% to 64.11% range, expanding outpatient benefit package could make patients have a more rational health-seeking behaviors, a better health condition and a more reasonable medical expenses.14,26 Before December 2022, annual outpatient reimbursement rate of non-chronic disease cohorts in Guangzhou (32.56%) already neared this optimal interval. After policy implementation, it rose significantly to 61.14%, fully satisfying the evidence-based reimbursement rate threshold. It also further explains the absence of notable expenditure escalation following benefit improvements for outpatient.
From the results of this study, although expanding outpatient benefit package for non-chronic disease patients meant the medical insurance department would pay more in outpatient expenses, it did not cause a remarkable growth in total basic medical insurance fund expenditures. This stability results not only from the lower expenditure of the basic medical insurance funds for inpatient expenses due to patients’ better health outcomes,15,27,28 but also, significantly, from payment reforms in recent years in Guangzhou.29,30 Presently, Guangzhou employs caption payment for outpatient care while Diagnosis-Intervention Packet (DIP) payment for hospitalization. Under such circumstances, the transfer of medical expenses between outpatient services and inpatient services may be largely eliminated. To receive a stable even higher payment, medical institutions have to simultaneously cut down unnecessary expenditure for both outpatient services and inpatient services covered by the basic medical insurance scheme.31,32 As a result, patient’s financial burden of medical care is decline sharply. In addition, this study found expanding outpatient benefit package could induce moral hazard among non-chronic disease patients to some extent (See Supplemental Additional File 5). Specifically, it manifested as a concentrated surge in outpatient visits approaching the end of the insurance fiscal year (The settlement year of China’s basic medical insurance usually follows a natural year cycle). What it comes about mainly on account of the current financing mechanism for outpatient pooled funds, which relies on reductions in individual medical savings account contributions.33,34 This policy design makes non-chronic disease patients foster an improper perception that their personal benefits are injured. 35 Therefore, they deliberately pursue outpatient services that may be non-essential, especially near the end of the year, to maximize utilization of the insurance pool funds.
Conclusions
In conclusion, within well-designed payment models, expanding outpatient benefit package among patients without chronic conditions could enable them to get a more comprehensive and prompt treatment while total medical expenses and expenditure of the basic medical insurance funds are stable totally.
The positive findings on expanding outpatient benefit package for non-chronic disease patients in this paper are extremely important to China and other countries particularly those with comparatively deficient medical resources. The analysis for influence of improving outpatient benefit on non-chronic disease patients’ health-seeking behaviors, medical expenses and reimbursement not only supplement existing studies’ conclusions, but also inspire policy makers whose country implements a social health insurance system that it’s feasible to expand outpatient benefit package for non-chronic disease patients.
This study also has some limitations. First, it could not evaluate the effects of the policy expansion on patients’ health outcomes due to the absence of health status data in the insurance claims dataset. While we examine changes in healthcare utilization and financial protection, which are key intermediate steps toward improved health, the absence of direct health outcome measures (eg, clinical indicators, functional status, or quality of life) constitutes a significant omission. This limits our ability to assess whether the increased access and reduced financial barriers ultimately translated into better health, which is the paramount goal of the policy. Future research combining claims data with clinical records or survey-based health measures is essential to address this critical question.
Second, this study was conducted in Guangzhou, a high-income urban area in eastern China where advanced payment reforms (eg, DIP and capitation) have been implemented. Although these payment models are increasingly being adopted across China in the inpatient and outpatient setting, the economic development and health system maturity of the study setting may limit the direct generalizability of the results to rural or less-developed regions within China, or to other countries with different health insurance structures and reform trajectories.
Third, since it verifies the incidence of moral hazard attributable to the financing mechanism for outpatient pooled funds of Urban Employee Basic Medical Insurance, but how to provide strong protection against moral hazard still needs further research.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261441100 – Supplemental material for Expanding Outpatient Benefit Package Without Increasing Total Spending: Evidence From Outpatient Benefit Reform for Non-Chronic Disease Patients
Supplemental material, sj-docx-1-inq-10.1177_00469580261441100 for Expanding Outpatient Benefit Package Without Increasing Total Spending: Evidence From Outpatient Benefit Reform for Non-Chronic Disease Patients by Kefan Shi, Yuhao Wang, Tianyu Jing, Guojuan Ma, Wei Xu and Wenwen Du in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580261441100 – Supplemental material for Expanding Outpatient Benefit Package Without Increasing Total Spending: Evidence From Outpatient Benefit Reform for Non-Chronic Disease Patients
Supplemental material, sj-pdf-2-inq-10.1177_00469580261441100 for Expanding Outpatient Benefit Package Without Increasing Total Spending: Evidence From Outpatient Benefit Reform for Non-Chronic Disease Patients by Kefan Shi, Yuhao Wang, Tianyu Jing, Guojuan Ma, Wei Xu and Wenwen Du in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-xlsx-3-inq-10.1177_00469580261441100 – Supplemental material for Expanding Outpatient Benefit Package Without Increasing Total Spending: Evidence From Outpatient Benefit Reform for Non-Chronic Disease Patients
Supplemental material, sj-xlsx-3-inq-10.1177_00469580261441100 for Expanding Outpatient Benefit Package Without Increasing Total Spending: Evidence From Outpatient Benefit Reform for Non-Chronic Disease Patients by Kefan Shi, Yuhao Wang, Tianyu Jing, Guojuan Ma, Wei Xu and Wenwen Du in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-xlsx-4-inq-10.1177_00469580261441100 – Supplemental material for Expanding Outpatient Benefit Package Without Increasing Total Spending: Evidence From Outpatient Benefit Reform for Non-Chronic Disease Patients
Supplemental material, sj-xlsx-4-inq-10.1177_00469580261441100 for Expanding Outpatient Benefit Package Without Increasing Total Spending: Evidence From Outpatient Benefit Reform for Non-Chronic Disease Patients by Kefan Shi, Yuhao Wang, Tianyu Jing, Guojuan Ma, Wei Xu and Wenwen Du in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-xlsx-5-inq-10.1177_00469580261441100 – Supplemental material for Expanding Outpatient Benefit Package Without Increasing Total Spending: Evidence From Outpatient Benefit Reform for Non-Chronic Disease Patients
Supplemental material, sj-xlsx-5-inq-10.1177_00469580261441100 for Expanding Outpatient Benefit Package Without Increasing Total Spending: Evidence From Outpatient Benefit Reform for Non-Chronic Disease Patients by Kefan Shi, Yuhao Wang, Tianyu Jing, Guojuan Ma, Wei Xu and Wenwen Du in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors are grateful to the National Natural Science Foundation of China (Grant No. 72074220) and the Guangzhou Healthcare Security Administration for supporting the research. And then sincerely thanks to the whole research group in China Pharmaceutical University for collecting and organizing data.
Ethical Considerations
All methods in our study were carried out in accordance with the Declaration of Helsinki. This retrospective study utilized fully de-identified administrative claims data from the Guangzhou Healthcare Security Administration. As the research involved no direct contact with human participants and all data were anonymized prior to analysis, it was exempt from requiring formal ethical review by the institutional review board of China Pharmaceutical University. The study protocol and data use were formally approved by the Guangzhou Healthcare Security Administration on July 10, 2024. Access to and use of the data were governed by a strict data use agreement between China Pharmaceutical University and the data provider, which ensured compliance with data protection regulations and ethical standards for secondary data analysis.
Consent to Participate
The requirement for individual informed consent was waived for this study due to the anonymized nature of the data.
Author Contributions
K.S. and Y.W. performed statistical analysis of data together and made major contributions to writing the manuscript. K.S. and Y.W. contributed equally to the work, and therefore they share first authorship. T.J. and G.M. were responsible for the quality control of the study and assisted in writing the manuscript. W.X. and W.D. conceived the research ideas, collected and organized data regarding medical visits of sample population, provided funding and analytical framework, and offered critical supervision on the first draft and revision. W.X. and W.D. contributed equally to the work, and therefore sharing corresponding authorship. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for the study was provided by the general program of National Natural Science Foundation of China: Study on the influence of medical insurance management and payment policy of medical treatment beyond pooling regions on recurrent population’s health-seeking behavior, health outcome and medical expenditure (Grant No. 72074220).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding authors on reasonable request.*
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.