
Abstract
Total hip arthroplasty (THA) critically influences outcomes; however, a comprehensive mapping of the research landscape remains absent. We systematically characterized the knowledge structure, collaborative networks, and research priorities within the THA approach literature from 2000 to 2026. Multi-database bibliometric analysis integrated data from the Web of Science, PubMed, Embase, and Cochrane Library. Following deduplication, 4023 publications were analyzed using Bibliometrix, VOSviewer, and CiteSpace to map publication trends, collaboration networks, thematic evolution, and citation dynamics. Annual publications demonstrated sustained expansion (annual growth rate: 9.68% over the complete-year window 2000-2024), with marked acceleration after 2020 and peak production exceeding 300 publications during 2023 to 2024. The United States emerged as the primary hub (30.7% of publications), with European and East Asian centers forming secondary nodes. The Journal of Arthroplasty anchored volume (637 publications), while high-impact general journals (JBJS-Am, CORR) achieved the greatest citation efficiency (>60 citations per publication). Keyword clustering revealed well-differentiated themes (Q = 0.351, S = 0.706) centered on outcome surveillance, direct anterior approach evaluation, and positioning accuracy. Citation bursts documented a 3-phase evolution: minimally invasive descriptions (2003-2012), comparative benchmarking (2012-2020), and registry-based evidence (2018-2026). The field has matured from seeking universal approach superiority toward patient-, surgeon-, and system-specific selection paradigms. Priority directions include implementation science for learning curves, standardized patient-centered outcomes, health economic assessment, and approach-technology-pathway interaction studies. Geographic expansion beyond North American and European centers is essential for evaluating context-dependent effectiveness across diverse healthcare systems worldwide.
Keywords
Introduction
Total hip arthroplasty (THA) ranks among the most successful interventions in modern orthopedics, consistently delivering substantial pain relief and functional restoration in patients with end-stage hip disease. 1 With demographic aging and expanding clinical indications, THA utilization continues its upward trajectory; projections based on United States national data suggest that the demand for primary THA may increase by approximately 174% by 2030, underscoring the critical importance of optimizing surgical techniques and perioperative care to meet this growing burden. 1 Within this context, surgical approach selection has emerged as one of the most extensively debated topics in arthroplasty practice, as approach-related variations in anatomical exposure, soft tissue handling, and component implantation may translate into clinically meaningful differences in early recovery trajectories, complication profiles, and long-term implant survivorship.2,3
Contemporary THA practice encompasses several principal surgical approaches, including the posterior (posterolateral), direct lateral (Hardinge), anterolateral (Watson-Jones), and direct anterior approaches (DAA), each characterized by distinct anatomical planes, technical requirements, and associated risk–benefit profiles.2,3 Systematic reviews and meta-analyses indicate that approach selection can significantly influence key clinical outcomes, such as dislocation risk, abductor muscle function, gait recovery patterns, and various perioperative metrics, although the identification of a universally “optimal” approach remains elusive and appears highly dependent on surgeon experience, institutional resources, and patient-specific factors.2,3 The complexity of interpreting comparative evidence is further compounded by substantial heterogeneity in study designs, patient selection criteria, implant systems, perioperative protocols, and outcome measure definitions across the published literature.4,5
Among contemporary approaches, the DAA has garnered considerable attention owing to its purported muscle-sparing characteristics and potential advantages for early postoperative recovery.4,5 Multiple meta-analyses have reported favorable perioperative and short-term functional outcomes for DAA compared with posterior approaches, while demonstrating broadly comparable rates of major complications in many clinical settings.4,5 However, umbrella-level evidence synthesis suggests that while early benefits may be demonstrable, outcome differences frequently attenuate over time, and conclusions remain sensitive to study design quality and risk of bias assessments. 6 This evolving evidence base increasingly reflects a paradigmatic shift from the simplistic question of “which approach is superior” toward the more nuanced inquiry of “under what specific conditions, and in whose hands, can each approach deliver optimal outcomes.”
A crucial consideration in approach selection is the well-documented learning curve associated with the adoption of surgical techniques. Systematic reviews have identified substantial learning-curve effects for DAA implementation, with metrics of operative efficiency and complication rates demonstrating progressive improvement as surgeon experience accumulates. 6 Complementary registry-based analyses similarly document elevated revision risk during early surgeon adoption phases, with risk profiles normalizing only after adequate case volume accumulation, thereby emphasizing that approach comparisons must be interpreted in the context of surgeon proficiency and healthcare system-level factors. 7 These implementation challenges likely contribute to ongoing clinical controversies and have driven the rapid expansion of the published literature on surgical technique refinement, complication prevention, rehabilitation optimization, enhanced recovery protocols, and patient-reported outcome measurement.6,7
Given the substantial volume and thematic diversity of THA approach research, traditional narrative synthesis methodologies are increasingly inadequate for comprehensively capturing the global knowledge structure, international collaboration networks and temporal evolution of research priorities within this domain. Bibliometric analysis provides a systematic, transparent, and reproducible framework for mapping scientific landscapes, quantifying influential contributors and thematic clusters, and identifying citation “bursts” that signal shifting research attention patterns over time.8 -10 Specialized bibliometric tools, including VOSviewer and CiteSpace, enable the construction of collaboration networks, keyword co-occurrence mapping, co-citation analysis, and research hotspot detection, while the bibliometrix platform offers integrated R-based workflows for comprehensive science mapping and temporal trend analysis.9,10
Despite the proliferation of THA approach research and its clinical significance, no comprehensive bibliometric analysis has systematically characterized the global knowledge architecture, collaborative networks, and thematic evolution of this field using multi-database integration to date. Previous bibliometric studies in orthopedics have typically relied on single-database retrieval, which may introduce coverage bias and limit the comprehensiveness of the findings. 10 Furthermore, the rapid expansion of THA literature in recent years necessitates updated mapping to inform future research directions and identify emerging knowledge frontiers. 11
To address this knowledge gap, we conducted a comprehensive multi-database bibliometric and visualization study integrating data from the Web of Science Core Collection (WoSCC), PubMed, Embase, and the Cochrane Library to systematically characterize publication trends, international collaboration patterns, institutional contributions, author networks, journal dissemination structures, thematic evolution, and landmark references in research on surgical approaches for primary THA from 2000 to 2026. The findings are anticipated to provide evidence-based insights into the developmental trajectory and current research frontiers of this clinically important field, thereby informing future investigation priorities and facilitating more efficient knowledge translation into clinical practice.
Methods
Study Design and Multi-Database Integration Strategy
This bibliometric analysis was designed to provide comprehensive coverage of the global literature on surgical approaches in primary total hip arthroplasty (THA) through a systematic multi-database integration. The study workflow is shown in Figure 1. To minimize single-database coverage bias and maximize retrieval comprehensiveness, we conducted parallel searches across 4 complementary bibliographic databases: Web of Science Core Collection (WoSCC; specifically, Science Citation Index Expanded), PubMed (MEDLINE), Embase, and the Cochrane Library. A 25-year publication window (2000-2026) was selected to capture the modern era of THA approach evolution, encompassing the introduction and widespread adoption of contemporary techniques, including the direct anterior approach.

Multi-database integration workflow and study methodology. Flowchart illustrating the systematic multi-database bibliometric analysis workflow for surgical approach research in primary total hip arthroplasty (THA). The methodology encompasses parallel searching across four complementary databases (Web of Science Core Collection, PubMed, Embase, and Cochrane Library) covering the period 2000–2026, followed by data export, systematic deduplication using hierarchical matching algorithms prioritizing DOI and fuzzy title-author-year matching, and unified processing in R using the bibliometrix package (version 4.1.3). The integrated dataset (n = 4,023 unique publications after deduplication) underwent comprehensive bibliometric analysis using three complementary platforms: Bibliometrix for descriptive statistics and science mapping, VOSviewer (version 1.6.20) for collaboration network visualization, and CiteSpace (version 6.4. R1) for temporal knowledge structure analysis and citation-burst detection. This workflow demonstrates the methodological rigor of this study in minimizing single-database coverage bias while maximizing retrieval comprehensiveness and analytical depth.
The rationale for multi-database integration stems from the recognized variations in journal indexing scope, citation coverage, and metadata completeness across databases. WoSCC provides robust citation tracking and bibliometric-ready metadata but exhibits selective journal coverage. PubMed offers comprehensive biomedical literature indexing with controlled Medical Subject Headings (MeSH) vocabulary but lacks citation network data. Embase extends coverage to pharmacological and European clinical literature with Emtree thesaurus indexing. The Cochrane Library contains high-quality systematic reviews and controlled trials that may not be comprehensively indexed elsewhere. By integrating these complementary resources, we aimed to construct a more representative corpus of the global evidence landscape than that achievable through single-database retrieval.
This study was conducted and reported in accordance with the PRISMA 2020 guidelines for systematic searches (Supplemental Table S1) and the TITAN Guidelines (2025) for AI-assisted research reporting. 12
Search Strategy Development and Implementation
Search strategies were developed iteratively through pilot testing and structured to balance sensitivity (comprehensive retrieval) with specificity (minimizing irrelevant records). The core search architecture consisted of 3 Boolean-linked concept blocks: (1) THA procedure terms, (2) surgical approach descriptors, and (3) exclusion criteria for nontarget procedures.
For WoSCC, we implemented an advanced search using Topic field indexing (which encompasses title, abstract, author keywords, and Keywords Plus) with the following structure: THA-related terms (eg, “total hip arthroplasty,” “total hip replacement,” THA, THR) were combined with approach-specific terminology representing anatomical descriptions and eponymous techniques (eg, “direct anterior approach,” DAA, posterior, posterolateral, anterolateral, lateral, trans gluteal, Hardinge, Watson-Jones, Smith-Petersen, Hueter). To enhance the specificity for primary THA, NOT operators were applied to exclude revision arthroplasty, conversion procedures, hemiarthroplasty, and hip resurfacing. The complete WoSCC search string is provided in Supplemental Material S1, For PubMed, the search strategy was translated to combine free-text searching in the Title/Abstract fields with MeSH vocabulary, where appropriate. Embase searches similarly integrated free-text terms with the Emtree controlled vocabulary and employed field-specific tags to optimize precision. Cochrane Library searches were conducted using the Cochrane Search Manager interface with MeSH descriptors supplemented with keyword variants. Across all databases, conceptual equivalence was maintained (THA AND approach AND NOT exclusions) to ensure comparability while respecting the database-specific syntax and indexing conventions.
All searches were restricted to Articles and Reviews to focus on primary research reports and evidence synthesis, excluding editorials, letters, conference abstracts, and other non-peer-reviewed material. No language restrictions were applied during the initial retrieval to avoid excluding potentially relevant non-English literature, although subsequent analysis focused on records with English-language metadata.
Data Retrieval, Integration, and Deduplication
Records retrieved from each database were exported in plain-text bibliographic formats with maximal available metadata, including author names, affiliations, article titles, source titles, abstracts, keywords, publication year, digital object identifiers (DOI), and citation counts, where available. Export formats were standardized to facilitate downstream processing: WoSCC records were exported as tab-delimited plain text, PubMed records as MEDLINE format, Embase records as RIS format, and Cochrane records as the RIS format.
All exported files were imported into R (version 4.3.1) for unified data processing using the Bibliometrix package (version 4.1.3). The convert2df() function was used to parse database-specific formats into standardized bibliographic data frames. Individual database data frames were then merged using the mergeDbSources() function, which implements intelligent field alignment and handles database-specific metadata variation.
Deduplication was performed using a hierarchical matching algorithm that prioritizes high-confidence identifiers. Records sharing identical DOIs were merged into single entries, retaining the most complete metadata. For records lacking DOIs, duplicate detection employed fuzzy matching across combinations of the normalized title, first author surname, publication year, and source title. The normalization steps included case standardization, punctuation removal, and whitespace condensation to improve matching sensitivity. Author names were standardized to account for formatting inconsistencies (eg, “Smith, J.” vs “Smith J” vs “J. Smith”). Manual inspection of potential duplicates with intermediate matching scores was performed to adjudicate ambiguous cases.
Following deduplication, the final analytical dataset comprised 4023 unique publications (2766 articles and 1257 reviews), representing an integration of 1847 records from WoSCC, 1342 from PubMed, 1156 from Embase, and 89 from Cochrane Library (with substantial overlap indicating multi-database indexing of core literature). Quality control procedures included verification of metadata completeness, identification of missing critical fields (author, year, title), and validation of citation counts against source databases, where discrepancies were noted.
Bibliometric Analysis and Visualization
Bibliometric analysis and network visualization were conducted using an integrated 3-platform approach: R/bibliometrix for descriptive statistics and science mapping, VOSviewer (version 1.6.20) for collaboration network visualization, and CiteSpace (version 6.4. R1) for temporal knowledge structure analysis and burst detection purposes.
Descriptive Bibliometric Indicators
Using the Biblioshiny web interface of BiblioMetrix, we generated comprehensive descriptive statistics characterizing the dataset profile and temporal trends. Key indicators included: (1) annual scientific production and growth rate; (2) document type distribution; (3) source (journal) concentration and Bradford’s law analysis; (4) author productivity metrics and collaboration indices (co-authors per document, collaboration index, international collaboration percentage); (5) geographic distribution by country/region with publication counts and citation metrics; (6) institutional productivity rankings; and (7) field-weighted citation impact measures. These analyses provided a quantitative foundation for characterizing the field’s development trajectory and identifying high-output and high-impact contributors.
Collaboration Network Analysis
Collaboration structures were analyzed and visualized using VOSviewer, with networks constructed based on co-authorship relationships at 3 levels: country/region, institution, and individual author. For country collaboration networks, nodes represent countries (sized proportional to publication volume), edges represent co-authorship relationships (thickness proportional to collaboration frequency), and total link strength (TLS) quantifies the overall collaboration intensity for each country. Institutional and author collaboration networks were constructed using similar principles.
Network maps employed the Visualization of Similarities (VOS) layout algorithm, which positions nodes based on association strength to create interpretable clustering patterns. Modularity-based clustering was applied to identify distinct collaborative communities, with colors indicating cluster membership. For the temporal analysis of author networks, overlay visualization was employed, wherein node colors represent the average publication year, enabling the identification of established versus emerging research teams.
Minimum thresholds were applied to reduce network complexity and enhance interpretability: country networks included countries with ≥10 publications; institutional networks included institutions with ≥15 publications; and author networks included authors with ≥10 publications. These thresholds balance the network density against the retention of significant contributors.
Keyword Co-occurrence and Thematic Structure
Keyword co-occurrence networks were constructed to identify the thematic clusters and research hotspots. Author-provided keywords (DE) and Keywords Plus (ID) were combined after normalization (case standardization, plural-to-singular conversion, and synonym consolidation). Co-occurrence matrices were generated based on keyword pair frequencies across the corpus, and networks were constructed with nodes representing keywords and edges representing co-occurrence relationships.
Network analysis employed the Louvain algorithm for community detection, which identifies thematically coherent clusters by optimizing the network modularity. Cluster quality was assessed using modularity Q (higher values indicate stronger cluster differentiation; Q >0.3 is considered acceptable) and mean silhouette S (higher values indicate better within-cluster homogeneity; S >0.5 is considered good). Temporal trends within the keyword clusters were examined through overlay visualization, showing the average appearance year.
Citation Analysis and Burst Detection
CiteSpace was employed for co-citation analysis, timeline visualization, and citation burst detection to map the intellectual base and identify pivotal studies driving the field evolution. Co-citation networks were constructed, wherein nodes represent cited references and edges represent co-citation relationships (ie, 2 references cited together by a later publication).
Timeline visualization arranges co-citation clusters chronologically, enabling the tracking of thematic evolution over time. Each horizontal timeline represents a thematic cluster, with nodes positioned according to the first appearance year and the vertical position indicating cluster membership. This approach reveals how research foci have shifted over time.
Citation burst detection employs Kleinberg’s burst detection algorithm to identify references and keywords that experience unusually rapid citation increases during specific time windows. Burst strength quantifies the intensity of the citation surge, while burst begin/end years demarcate the period of elevated attention. Burst analysis identifies “turning point” studies that catalyzed research activity and marks emerging research fronts through keyword burst patterns.
The network parameters for CiteSpace analysis included time slicing (annual), node type (cited reference for co-citation analysis; keyword for burst analysis), selection criteria (top 50 most cited/occurred per slice), and link retention (cosine similarity ≥0.1). Cluster labeling employed the log-likelihood ratio (LLR) algorithm using citing article keywords to generate descriptive cluster labels.
Transparency and Reproducibility
This study adheres to the Transparency in Artificial Intelligence-Assisted Academic Research (TITAN) Guidelines (2025) for reporting AI-assisted research workflows. 12 AI-assisted tools were employed for literature screening, preliminary data organization, and manuscript drafting support. All critical methodological decisions, data processing steps, analytical parameter selections, and interpretation of results were conducted and verified by the research team. The complete search strategies, data processing scripts, and network analysis parameters are provided in the Supplemental Materials to enable the reproduction and verification of the findings.
Ethical Considerations
This study exclusively analyzed publicly available bibliographic metadata from indexed scientific publications. No human subjects, patient data, clinical interventions, or primary data collection were used in this study. In accordance with our institutional research ethics policies and international guidelines for bibliometric research, formal research ethics committee approval was not required for the secondary analysis of the published literature. All data handling and reporting procedures complied with the applicable data protection regulations and citation ethics principles.
Results
Dataset Characteristics and Publication Trends
The multi-database integration yielded 4023 unique publications spanning 2000 to 2026, distributed across 439 distinct source journals. To provide an unbiased growth estimate unaffected by incomplete calendar-year indexing, the primary dataset summary (Figure 2a) reports descriptive statistics for the complete-year window (2000-2024; 3733 documents across 417 sources), yielding an annual growth rate of 9.68%. The corpus comprised predominantly original research articles (n = 3264, 81.1%) and systematic reviews or meta-analyses (n = 383, 9.5%), indicating a robust primary literature base supplemented by mature evidence-synthesis outputs. The thematic richness of the field was reflected in 3660 Keywords Plus terms and 5034 author-provided keywords, providing substantial terminological diversity for downstream clustering and hotspot analysis.

Dataset characteristics and temporal publication trends. (A) Descriptive summary of the primary analytical dataset (2000–2024 complete-year window). Key indicators include annual growth rate (9.68%), source and author counts, collaboration indices, and citation metrics. (B) Temporal evolution of annual publication volume from 2000 through 2026, demonstrating sustained field expansion with distinct growth phases: gradual increase during 2000–2010, moderate acceleration through 2010–2020, and marked growth from approximately 2020 onward, achieving peak annual production exceeding 300 publications during 2023–2024. The apparent decline in 2026 represents incomplete calendar-year coverage and ongoing database indexing lag (typically 6–12 months), rather than diminished research activity. The temporal trajectory reflects convergent factors, including accumulated clinical experience with contemporary surgical approaches, maturation of registry infrastructure, and increased emphasis on enhanced recovery protocols intersecting with approach selection. Data points represent annual publication counts; the trend line indicates the overall growth trajectory.
Collaborative authorship patterns demonstrated high engagement, with a mean of 5.17 co-authors per document, and international collaboration accounting for 14.12% of total publications. The dataset encompassed contributions from 13 439 distinct authors from multiple countries and institutions. Citation metrics revealed an average of 24.76 citations per document, with a mean document age of 9.96 years, reflecting sustained scholarly attention to the field’s core literature.
Temporal publication trends (Figure 2b) demonstrate a consistent upward trajectory from the early 2000s to 2025. Annual output increased gradually during 2000 to 2010, accelerated moderately through 2010 to 2020, and exhibited marked growth from approximately 2020 onward, achieving peak annual production during 2023 to 2024 (n >300 articles per year). The apparent decline in 2026 reflects incomplete calendar-year coverage and ongoing database indexing processes rather than diminished research activity, consistent with the typical 6 to 12 month database incorporation lag for recent publications.
Geographic Distribution and International Collaboration Networks
The country-level productivity and collaboration patterns are presented in Table 1 and visualized in Figure 3. The United States emerged as the dominant contributor, accounting for 1233 publications (30.7% of total output) and 39 682 citations, and demonstrating the highest international collaboration intensity (total link strength [TLS] = 319). This pattern establishes the United States as the primary hub in the global research network for THA surgical approaches.
Geographic Distribution of Research Productivity and International Collaboration Patterns.

Note. The top 10 most productive countries/regions contributing to research on surgical approaches in primary total hip arthroplasty, ranked by publication volume. Metrics include total publication count (N Publications), total citation accumulation (Total Citations), citation density (Average Citations per Publication), and international collaboration intensity quantified through total link strength (TLS) derived from country-level co-authorship network analysis. TLS represents the cumulative strength of collaborative connections with other countries, with higher values indicating greater engagement in multinational research partnerships. Data derived from multi-database integration of Web of Science Core Collection, PubMed, Embase, and Cochrane Library covering publications from 2000 to 2026.

Geographic distribution and international collaboration network.
The People’s Republic of China ranked second in publication volume with 447 documents (11.1%) and exhibited substantial collaborative engagement (TLS = 208), indicating rapid research expansion coupled with extensive cross-border partnerships. Japan contributed 303 publications (7.5%) characterized by notably high citation impact (10 776 citations; 35.56 citations per publication) and strong network connectivity (TLS = 170), suggesting influential contributions despite moderate output volumes.
European countries collectively represented a substantial research presence, with Germany (353 publications), Italy (185 publications), France (156 publications), and Switzerland (145 publications) forming an interconnected cluster. However, Germany’s relatively limited international linkage (TLS = 41) compared to its publication volume suggests that research networks are concentrated within national or regional boundaries. In contrast, smaller European nations, including the Netherlands (134 publications, TLS = 126) and Switzerland (145 publications, TLS = 98), demonstrated disproportionately high collaborative intensity relative to output volume, consistent with participation in multinational research consortia.
The collaboration network visualization (Figure 3) depicts a hub-and-spoke topology, with the United States occupying the central position and maintaining dense connections with multiple international partners. Secondary hubs emerged in East Asia (China, Japan, and South Korea) and Western Europe (particularly the Netherlands, Switzerland, and Scandinavian countries), with visible regional subclusters reflecting geographic proximity and established institutional partnerships. Several peripheral nodes with limited international connectivity suggest emerging research communities or nationally focused programs that have not yet been integrated into multinational collaboration networks.
Institutional Contributions and Collaborative Architecture
The temporal evolution of institutional research foci is illustrated through timeline cluster analysis (Figure 4a), which reveals progressive thematic diversification from broad arthroplasty concepts toward approach-specific and complication-oriented investigations. Early period clusters centered on foundational terminology (replacement, follow-up, arthroplasty), whereas middle-period clusters increasingly emphasized technical specifications (direct lateral approach, acetabular component) and adverse outcome surveillance (failure, complications). Recent activity was concentrated within the direct anterior approach cluster, reflecting the contemporary research prioritization of comparative approach evaluation.

Temporal evolution of research themes.
Keyword burst analysis (Figure 4b) corroborated this temporal progression, with early bursts (2000-2010) dominated by general THA terminology (arthroplasty, follow-up, cement, low-friction arthroplasty). Mid-period bursts (2010-2015) featured minimally invasive surgery and mini-incision descriptors, coinciding with the widespread adoption of tissue-sparing techniques. The most recent burst phase (2015-2026) highlighted approach-specific terms (posterolateral and direct anterior approaches) alongside contemporary implant strategies (short stem) and revision-related concerns, indicating maturation toward outcome-driven comparative research.
Against this thematic backdrop, institutional productivity rankings (Table 2) reveal marked heterogeneity in output volume, citation impact, and collaborative engagement. The Hospital for Special Surgery led in publication count (114 documents) with robust citation accumulation (2212 citations) and a strong collaborative capacity (TLS = 68). Despite fewer publications (79 documents), the Mayo Clinic demonstrated exceptional citation efficiency (3332 citations; 42.18 citations per publication) and substantial network integration (TLS = 41), suggesting high-impact contributions with broad research community engagement.
Institutional Productivity Rankings and Collaborative Network Integration.
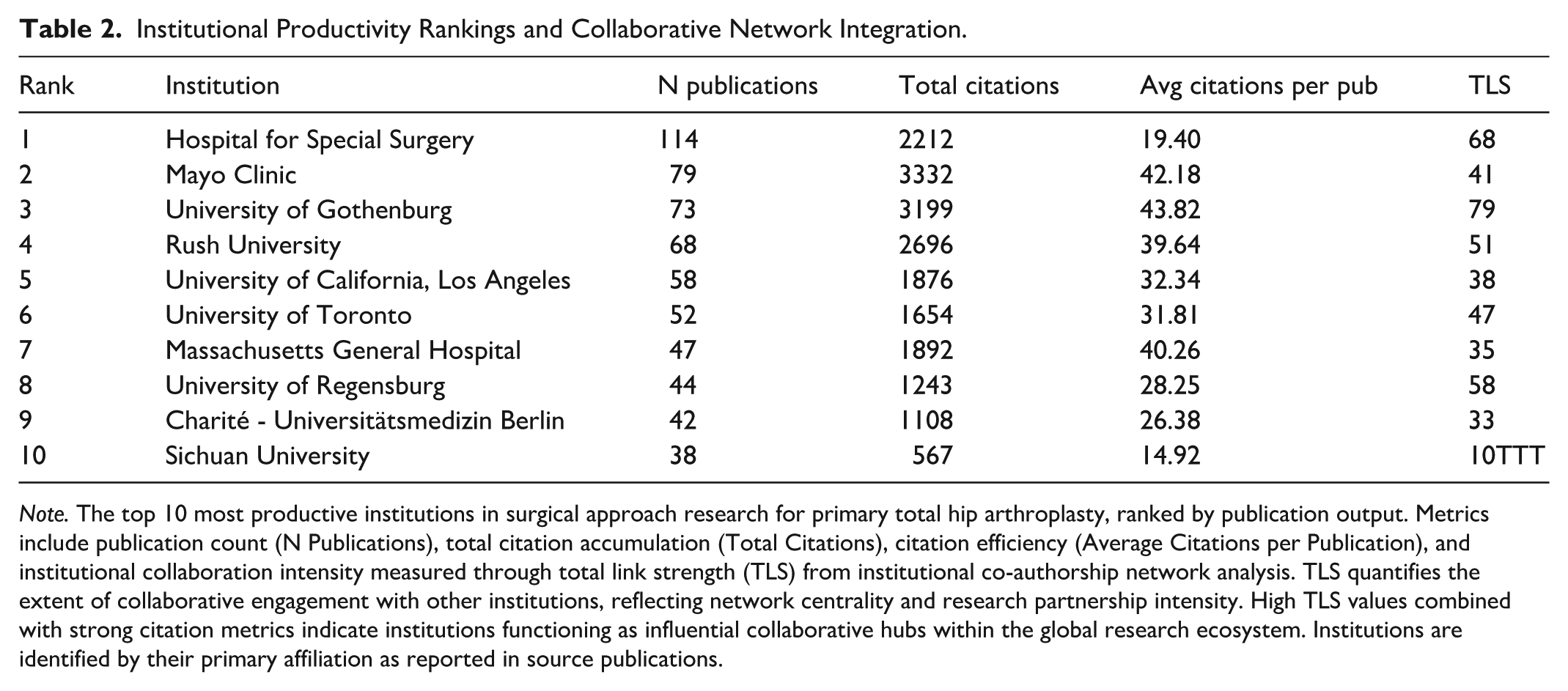
Note. The top 10 most productive institutions in surgical approach research for primary total hip arthroplasty, ranked by publication output. Metrics include publication count (N Publications), total citation accumulation (Total Citations), citation efficiency (Average Citations per Publication), and institutional collaboration intensity measured through total link strength (TLS) from institutional co-authorship network analysis. TLS quantifies the extent of collaborative engagement with other institutions, reflecting network centrality and research partnership intensity. High TLS values combined with strong citation metrics indicate institutions functioning as influential collaborative hubs within the global research ecosystem. Institutions are identified by their primary affiliation as reported in source publications.
European institutions exhibit particularly strong connectivity-to-impact ratios. The University of Gothenburg achieved the highest collaboration intensity among top-tier institutions (TLS = 79), coupled with superior average citation performance (43.82 citations per publication), consistent with participation in registry-based multicenter research networks. Rush University similarly combined above-average connectivity (TLS = 51) with strong citation metrics (39.64 citations per publication). In contrast, several high-output Asian institutions, including Sichuan University (38 documents, TLS = 10), demonstrated rapid productivity growth with comparatively limited international collaborative linkages at this developmental stage.
The institutional collaboration network (Figure 5) displays a densely interconnected core comprising North American and European high-output centers, surrounded by peripheral institutions with varying degrees of integration. This architecture suggests that the most extensively connected hubs play disproportionate roles in disseminating methodological approaches and shaping research priorities, particularly regarding contemporary, approach-specific comparative questions.

Institutional collaboration network and research architecture.
Author Productivity, Citation Impact, and Collaboration Networks
Author-level productivity and influence metrics are summarized in Table 3, with the collaboration structure and temporal activity patterns visualized in Figure 6. Beaulé, Paul E. ranked first in publication output with 33 documents, followed by Schwarzkopf, Ran (28 documents), and Parvizi, Javad (27 documents). The secondary tier of highly productive authors included Grifka, Joachim, and Perka, Carsten (both 26 documents), and Boettner, Friedrich, and Taunton, Michael J. (both 24 documents), indicating a concentration of sustained research activity within a limited number of established investigator teams.
Author Productivity, Citation Impact, and Collaborative Network Positioning.

Note. The top 20 most productive authors in surgical approach research for primary total hip arthroplasty, ranked by publication volume. Metrics characterize both individual productivity (N Publications) and research influence through citation-based indicators including total citations accumulated (Total Citations) and citation density (Average Citations per Publication). Author collaboration intensity is quantified through total link strength (TLS) derived from co-authorship network analysis, representing the cumulative strength of collaborative connections with other authors. High TLS values identify authors occupying central positions within collaborative networks who serve as connectors facilitating knowledge exchange and multicenter research productivity. The dissociation between publication volume and citation metrics across authors reflects heterogeneity in research impact beyond simple output quantity, likely influenced by study design, methodology, and conceptual contribution to the field.

Author collaboration network and temporal activity patterns.
Citation performance metrics reveal substantial dissociation between productivity and impact rankings. Kärrholm, Johan achieved the highest average citation density (1169 total citations; 53.14 citations per publication), followed by Parvizi, Javad (1213 citations; 44.93 citations per publication) and Taunton, Michael J. (774 citations; 32.25 citations per publication). Notably, Schwarzkopf, Ran—second in productivity—demonstrated a comparatively modest average citation performance (7.46 citations per publication), highlighting that research influence within this field extends beyond simple publication volume and likely reflects differences in study type, methodology, and adoption of key conceptual frameworks.
The collaborative network structure, quantified through total link strength (TLS), identified authors serving as connectors within the broader research community. Grifka, Joachim (TLS = 92) and Renkawitz, Tobias (TLS = 87) exhibited the strongest collaboration intensity, followed by Kärrholm, Johan (TLS = 68), and Taunton, Michael J. (TLS = 61). This pattern suggests that highly impactful authors frequently occupy structurally central network positions that facilitate multicenter productivity and accelerate the dissemination of approach-related evidence across institutional boundaries.
The overlay co-authorship visualization (Figure 6) delineates multiple densely connected author communities with temporal color gradients indicating research activity periods. Earlier-period activity (cooler colors) was concentrated within established European and Nordic collaborative groups, whereas recent-period activity (warmer colors) was clustered around approach-focused comparative research teams, consistent with the thematic evolution toward direct anterior approach evaluation and contemporary outcome benchmarking.
Journal Distribution and Citation Impact Patterns
Source journal analysis (Table 4) revealed concentrated dissemination within a core set of orthopedic and arthroplasty journals. The Journal of Arthroplasty dominated output volume with 637 publications (15.8% of total corpus), exhibited the strongest journal-level connectivity (TLS = 8000), and accumulated substantial citations (17 296 citations; 27.15 citations per publication), establishing it as the primary publication venue for approach-related THA research.
Journal Dissemination Patterns and Citation Impact Profiles.

Note. The top 10 most productive journals publishing research on surgical approaches in primary total hip arthroplasty, ranked by publication volume. Metrics include total publication count (N Publications), cumulative citation accumulation (Total Citations), citation efficiency (Average Citations per Publication), and journal-level collaboration strength (TLS) quantifying the extent of inter-journal citation relationships and knowledge network integration. The dual-tier journal ecosystem is evident, wherein 1 subspecialty journal (Journal of Arthroplasty) anchors publication volume and network connectivity, while high-impact general orthopedic journals (JBJS-Am, CORR) demonstrate superior citation efficiency despite lower publication counts, indicating their role as platforms for practice-shaping, high-impact clinical investigations. Citation efficiency disparities reflect differences in journal scope, peer review stringency, readership breadth, and the types of studies preferentially published in each venue.
However, citation impact analysis has demonstrated that publication volume and citation density are not synonymous. The Journal of Bone and Joint Surgery—American Volume, despite contributing only 114 publications (2.8%), achieved the highest average citation rate (63.73 citations per publication) with 7265 total citations, indicating its role as a preferred outlet for high-impact clinical research. Similarly, Clinical Orthopedics and Related Research demonstrated elevated citation efficiency (61.21 citations per publication) from 221 publications and 13 527 citations, suggesting that influential comparative studies and outcome analyses preferentially appear in high-impact general orthopedic journals rather than subspecialty venues.
The second tier of journals contributed moderate output with respectable citation metrics, including International Orthopedics (165 publications; 22.14 citations per publication), Orthopedics & Traumatology: Surgery & Research (121 publications; 19.36 citations per publication), and Archives of Orthopedic and Trauma Surgery (108 publications; 19.10 citations per publication). Open-access and clinically oriented journals, such as BMC Musculoskeletal Disorders (109 publications), expanded dissemination breadth but exhibited lower average citation performance (12.37 citations per publication), consistent with more heterogeneous content and broader audience targeting.
Collectively, these patterns indicate a dual-tier journal ecosystem: one high-volume subspecialty journal (Journal of Arthroplasty) anchoring the field’s publication infrastructure and citation network centrality, while prestigious general orthopedic journals (JBJS-Am, CORR) capture the highest-impact studies that establish practice-shaping evidence and methodological benchmarks.
Thematic Structure and Research Hotspots
Keyword co-occurrence analysis (Figure 7) generated a well-differentiated network comprising 769 keyword nodes connected by 6991 co-occurrence links (network density = 0.0237). Network quality metrics indicated an acceptable cluster structure (modularity Q = 0.351) with good internal consistency (mean silhouette S = 0.7057), supporting reliable thematic interpretation.

Thematic structure and research hotspots.
The network was resolved into multiple distinct thematic clusters representing the conceptual architecture of the field. Cluster #0 (follow-up) occupied a central position, reflecting the foundational role of longitudinal outcome surveillance, including survivorship, revision rates, complications, and functional recovery, as the primary framework for approach evaluation. Clusters #6 (total hip arthroplasty) and #7 (joint replacement) functioned as general terminological hubs connecting specialized subclusters, characteristic of mature surgical fields where technique-specific questions are ultimately adjudicated through standardized outcome metrics.
Approach-focused research emerged prominently in Cluster #1 (direct anterior approach), representing the most approach-specific thematic community. This cluster’s proximity to outcome-centered clusters (follow-up, complications) indicates that contemporary DAA discourse is predominantly outcome-driven rather than purely descriptive, emphasizing comparative recovery trajectories, complication profiles, component positioning accuracy, and learning-curve considerations.
Methodological and technical optimization themes appeared in Cluster #2 (accuracy), which encompassed component orientation, acetabular cup positioning, leg-length restoration, imaging guidance, navigation systems, and robotic assistance—all precision-related factors known to influence dislocation risk and functional outcomes. Cluster #8 (cementless THA) reflects the tight integration between approach selection and contemporary implant fixation strategies, mirroring real-world clinical decision-making, where surgical pathways and implant system choices co-evolve.
Indication-specific satellites included Cluster #4 (femoral neck fracture) and Cluster #5 (femoroacetabular impingement), demonstrating that approach research extends beyond elective primary osteoarthritis THA to encompass fracture management and complex hip morphology in younger patient populations. A minor cross-field signal (Cluster #3, total knee arthroplasty) likely reflects a shared arthroplasty methodology and terminology transfer rather than substantive topical overlap.
The overall network structure suggests a clear thematic hierarchy: general THA terminology and outcome surveillance form the knowledge base, approach-specific comparisons (particularly DAA) constitute a major contemporary research front, and accuracy optimization plus indication-driven subtopics represent key branching directions defining current and emerging investigative priorities.
Landmark References and Temporal Citation Dynamics
Citation burst detection identified the top 25 references experiencing unusually intense citation activity during specific time windows (Figure 8), revealing 3 distinct evolutionary phases characterizing the intellectual development of the field.
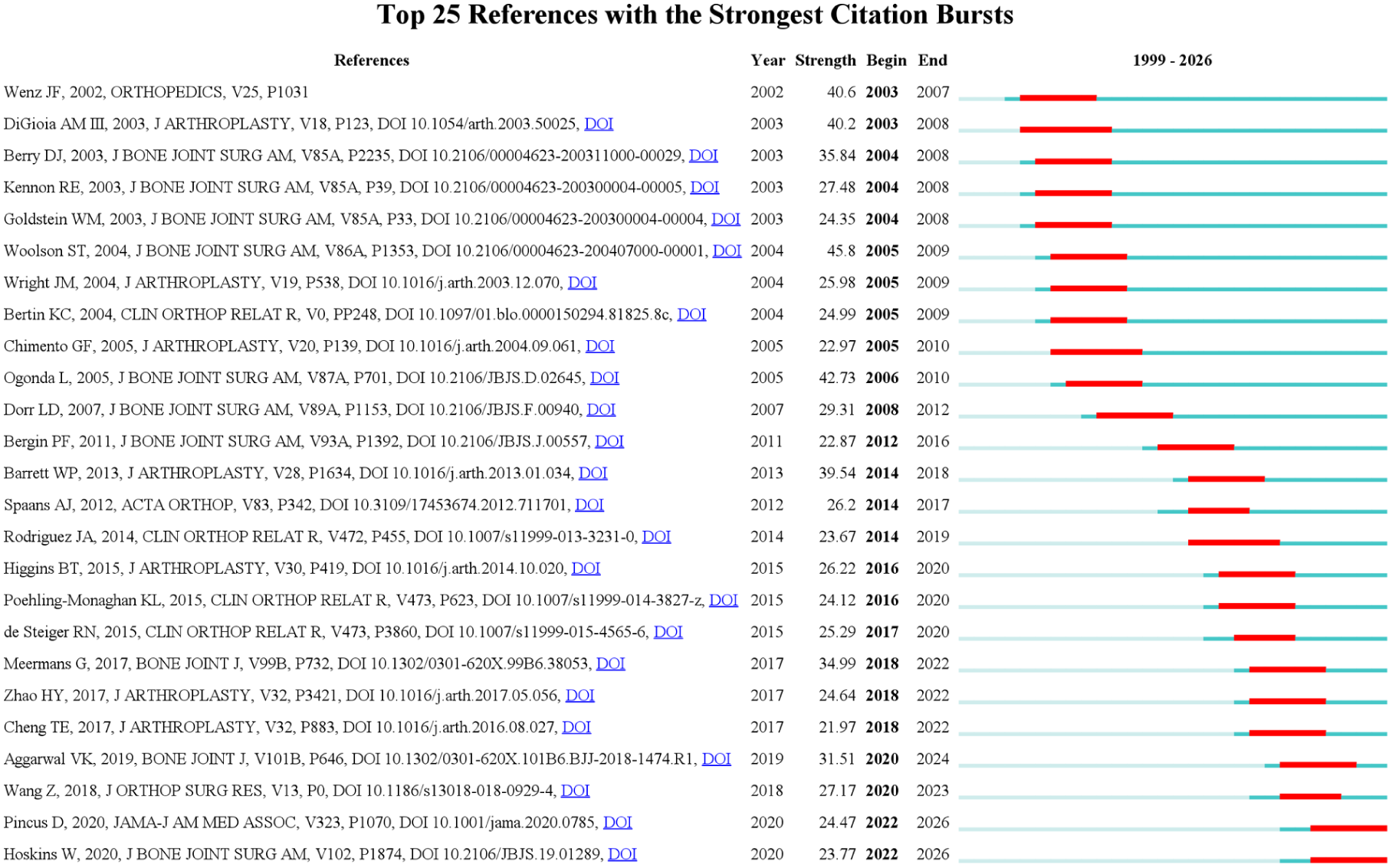
Landmark references and citation burst dynamics.
Early phase bursts (2003-2012) concentrated during 2003 to 2010 and were dominated by seminal papers published in JBJS-Am, Journal of Arthroplasty, and orthopedics, introducing and evaluating minimally invasive approaches and alternative surgical techniques. The earliest bursts were initiated as early as 2003 (Wenz et al. 13 , Hafez et al. 14 ) and extended through 2007 to 2008, capturing the rapid dissemination and debate surrounding less-invasive THA strategies. The strongest bursts during this period included Arsoy et al. 15 (burst strength = 45.8; 2005-2009) and Ogonda et al. 16 (burst strength = 42.73; 2006-2010), reflecting how powerfully early technique-innovation studies drove subsequent citation activity and shaped initial approach-comparison discourse.
Middle-phase bursts (2012-2020) exhibited a temporal shift toward comparative outcome evaluation and complication benchmarking, with multiple influential references demonstrating burst activity commencing around 2014 to 2017 and continuing through 2018 to 2020. Representative studies included Daher et al. 17 (burst strength = 39.54; 2014-2018), Rodriguez et al. 18 . (2014-2019), and a cluster of the mid-2010s publications with sustained burst periods extending to 2020 (Forlenza et al. 19 , Poehling-Monaghan et al. 20 , Campbell et al. 21 ). This pattern indicates maturation from technique novelty toward standardized outcome assessment, where approaches have been increasingly evaluated through reproducible functional endpoints, complication rates, and implant survivorship in generalizable patient cohorts.
Recent-phase bursts (2018-2026) anchored in the 2018 to 2026 window, with several references maintaining citation momentum through 2022 to 2026, signal continued high-intensity engagement with contemporary evidence. Pincus et al. 22 (2022-2026) and Hoskins et al 23 (2022-2026) represent the newest high-traction references, aligning with the recent emphasis on large-scale administrative datasets, registry analyses, perioperative safety metrics, and system-level outcomes. Strong bursts spanning 2020 to 2024 (including Gusho et al. 24 . indicate active evidence consolidation around modern practice patterns, real-world complication profiles, and patient-centered outcomes that are most relevant to clinical decision-making and health system value assessment.
Collectively, the burst trajectory documents field evolution from an early innovation-and-feasibility phase through mature outcomes-benchmarking toward a contemporary emphasis on large-scale, real-world evidence that can inform approach selection under actual clinical conditions rather than idealized research settings.
Discussion
This multi-database bibliometric analysis systematically mapped the global research landscape of surgical approaches in primary total hip arthroplasty across a 25-year period (2000-2026), integrating data from the WoSCC, PubMed, Embase, and Cochrane Library to minimize single-database coverage bias. Through a comprehensive analysis of 4023 publications using complementary bibliometric tools (Bibliometrix, VOSviewer, and CiteSpace), we characterized publication trajectories, international collaboration networks, institutional and author contributions, journal dissemination patterns, thematic evolution, and temporal citation dynamics. The synthesis presented in Figure 9 consolidates the key findings across dataset characteristics, temporal growth patterns, geographic collaboration hubs, institutional architecture, journal ecosystem structure, and staged thematic development. This integrated mapping provides evidence-based insights into knowledge production patterns, research priorities, and emerging frontiers in THA research.
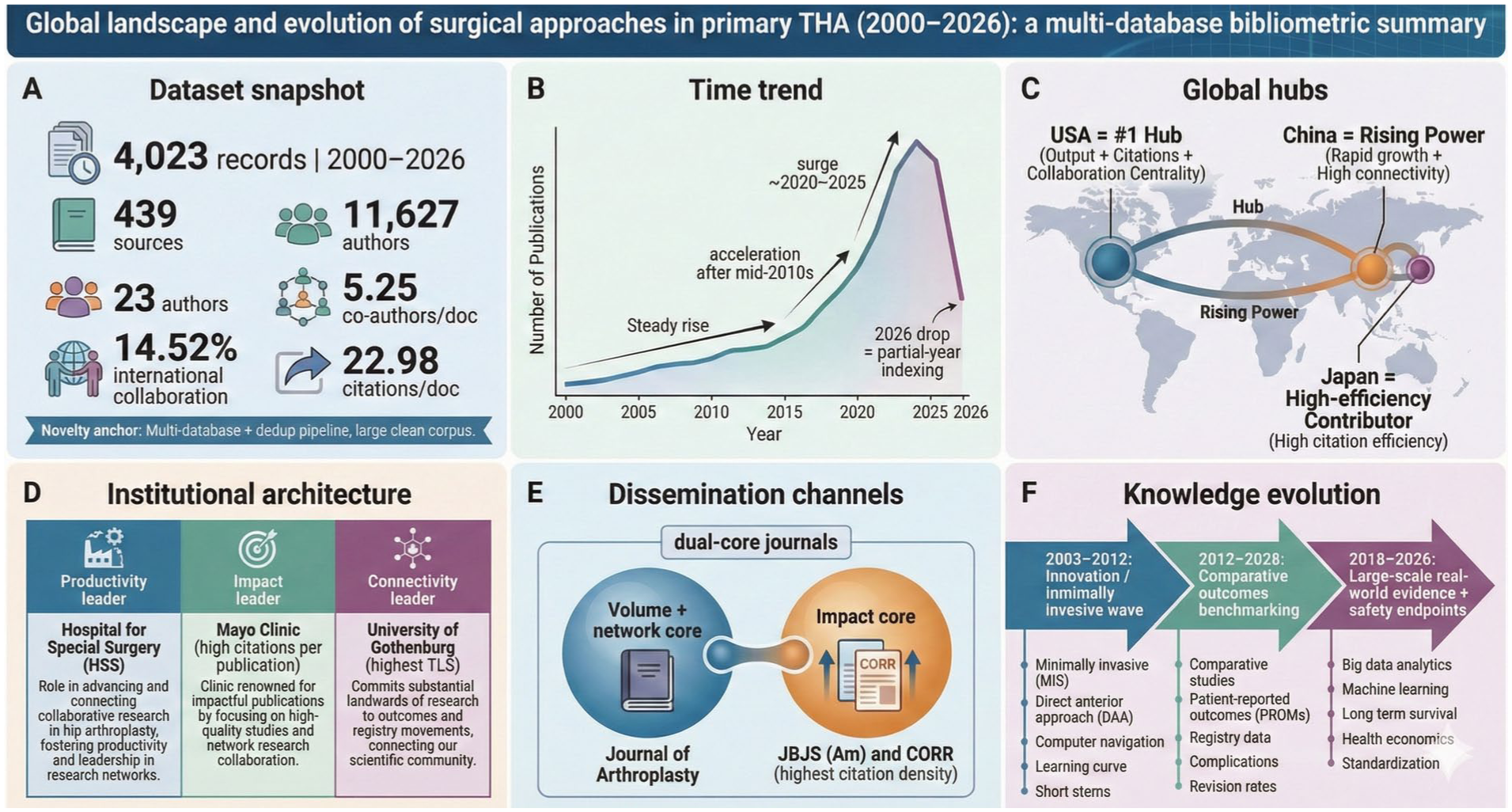
Integrated synthesis of knowledge production patterns.
Field Expansion and Temporal Dynamics: Interpreting Growth With Methodological Awareness
The observed publication trajectory demonstrates sustained expansion from the early 2000s, with pronounced acceleration after 2020, achieving peak annual production exceeding 300 publications during 2023 to 2024 (Figure 2b). Over the complete-year window (2000-2024), the field achieved an annual growth rate of 9.68% (Figure 2a), underscoring robust and accelerating research investment. At the macro level, this growth pattern parallels the well-documented global increase in THA utilization driven by demographic aging, expanding indications, and improved implant longevity. 12 The temporal inflection around 2020 likely reflects convergent factors, including accumulated clinical experience with the direct anterior approach enabling large-scale comparative studies, maturation of registry infrastructure facilitating real-world outcome assessment, and increased emphasis on enhanced recovery protocols that intersect directly with approach selection. 25
However, methodological awareness requires careful interpretation of apparent trends in the most recent period. The observed decline in 2026 output represents incomplete calendar-year indexing rather than genuine field contraction, consistent with the typical 6 to 12 month database incorporation lag for recent publications. 26 This artifact underscores a fundamental limitation of bibliometric temporal analysis: citation-based metrics are inherently age-dependent, and recent publications have not accumulated sufficient citation histories for valid impact assessments. Consequently, while publication volume provides real-time productivity indicators, citation-based influence measures require multi-year maturation periods before reaching interpretive stability. To mitigate such artifacts, the primary descriptive statistics in this study (Figure 2a) are reported for the complete-year window (2000-2024), ensuring that growth metrics are not distorted by differential indexing completeness in the most recent calendar year.
Collaborative Architecture and Knowledge Production Hubs: Implications for Evidence Quality and Generalizability
The documented network structure reveals a hub-dominated collaborative architecture, wherein a limited number of countries and institutions function as central connectors within the global research ecosystem (Figures 3 and 5). The United States’ position as the primary hub (30.7% of publications, TLS = 319) reflects well-established advantages in research infrastructure, funding mechanisms, and institutional capacity for large-scale arthroplasty research. 27 However, meaningful research contributions from smaller European nations with disproportionately high collaborative intensity (Netherlands, Switzerland) demonstrate that network centrality and research influence can be achieved through strategic participation in multinational consortia and registry-based research platforms, independent of absolute output volume. 28
From an evidence quality perspective, this collaborative architecture presents opportunities and concerns. Highly connected international networks theoretically enhance external validity through diverse patient populations, varied healthcare systems, and heterogeneous surgical practice patterns, which are critical for establishing generalizable conclusions about approach-related outcomes. 29 Registry-based collaborative research, particularly prominent among Scandinavian institutions with high connectivity-to-impact ratios, exemplifies this strength by enabling large-sample, real-world comparative effectiveness studies with prolonged follow-up that would be infeasible within single-institution frameworks. 30
Conversely, hub-dominated networks risk propagating methodological approaches, outcome prioritization, and interpretive frameworks that reflect the perspectives of central institutions while potentially marginalizing alternative conceptualizations or context-specific considerations relevant to peripheral communities. 31 The observed concentration of high-impact publications within established North American and Western European centers (Table 2) may contribute to geographic and socioeconomic homogeneity in study populations, limiting their applicability to healthcare systems with different resource constraints, patient demographics, or surgical training paradigms. This consideration is particularly important given the ongoing debates regarding the context-dependence of approach-related outcomes, where factors such as surgeon experience, institutional protocols, and available technology may modify comparative effectiveness relationships.32,33
The Direct Anterior Approach as Research Focal Point: Adoption Dynamics, Learning Curves, and Evidence Maturation
The prominent emergence of direct anterior approach-focused research (Cluster #1 in the keyword analysis, recent-period burst activity) represents a paradigmatic case study in surgical innovation diffusion and evidence development. The temporal evolution documented through citation burst analysis—from early period minimally invasive enthusiasm through middle-period comparative outcome evaluation to recent-period large-scale real-world assessment—recapitulates classical patterns of surgical innovation adoption, wherein initial technique-focused reports transition toward patient-centered outcome benchmarking as clinical experience accumulates and methodological rigor increases. 34
Multiple factors likely contribute to DAA’s sustained research prominence of DAA. First, the muscle-sparing anatomical rationale provides a compelling theoretical framework for predicting improved early recovery, reduced tissue trauma, and potentially favorable complication profiles. 35 Second, the technical distinctiveness of DAA (supine positioning, specialized instrumentation, and alternative component exposure sequences) creates clear comparative research opportunities versus traditional posterior and lateral approaches. Third, substantial learning curve effects documented for DAA implementation 36 generate practical clinical questions regarding optimal training pathways, case volume thresholds for proficiency, and patient selection criteria during adoption phases, which require evidence generation through systematic investigation.
Critically, the maturation from “which approach is better?” toward “under what conditions can each approach deliver optimal outcomes?” The (Introduction section) represents intellectual progress consistent with accumulating evidence that approach-related outcome differences are frequently context-dependent rather than universal. 37 Registry analyses have repeatedly demonstrated that surgeon and institutional experience substantially modify approach-associated complication rates and revision risks, particularly during early adoption periods. 38 This finding suggests that comparative effectiveness may be less determined by approach selection than by the interaction between approach choice, surgeon proficiency, institutional infrastructure, and patient-specific factors, a multivariate reality that simplistic approach superiority narratives inadequately capture.
Furthermore, the integration of approach comparisons with contemporary technology (navigation and robotics) and perioperative optimization (ERAS protocols) introduces additional complexity. 39 Enhanced recovery pathways can attenuate previously documented approach-related differences in hospital stay and early functional recovery, 40 whereas navigation systems may reduce approach-dependent variations in component positioning accuracy. 41 These developments suggest that the relevant clinical question is evolving from an isolated approach comparison toward optimization of the complete surgical pathway—encompassing approach selection, technological augmentation, and perioperative care integration—customized to individual patient characteristics and institutional capabilities.
Methodological Evolution and Evidence Hierarchy: From Case Series to Registry-Based Real-World Evidence
The temporal progression in landmark references (Figure 8) documents methodological maturation from early descriptive case series and single-center comparisons to large-scale registry analyses and systematic evidence syntheses. Early phase burst references (2003-2012) predominantly comprised technique descriptions, feasibility assessments, and initial comparative series—essential foundational literature establishing approach viability but limited in generalizability and long-term outcome assessment. 42 Middle-phase bursts (2012-2020) increasingly featured multicenter comparative studies, meta-analyses consolidating early evidence, and complication-focused investigations with longer follow-ups, reflecting field maturation toward standardized outcome reporting and evidence synthesis. 43
Recent-phase bursts (2018-2026) demonstrate continued evolution toward registry-based real-world evidence, examining large patient cohorts under actual clinical conditions rather than idealized research protocols. 44 This methodological progression aligns with broader evidence-based medicine trends, recognizing that while randomized controlled trials provide internal validity advantages, registry and administrative database analyses offer complementary strengths in external validity, sample size for rare outcome detection, and long-term survivorship assessment. 45 The prominence of registry-based institutions among high-impact contributors (Table 2) underscores how systematic outcome surveillance infrastructure enables the sustained production of practice-relevant evidence addressing real-world comparative effectiveness questions.
However, the methodological diversity in the literature introduces interpretive challenges. Heterogeneity in outcome measure definitions, follow-up duration, patient selection criteria, surgeon experience classification, and statistical adjustment strategies complicates evidence synthesis and may contribute to apparently contradictory conclusions across studies. 46 The documented concentration of high-citation studies in general orthopedic journals (JBJS-Am, CORR) rather than subspecialty venues (Table 4) may reflect the preferential publication of methodologically rigorous, adequately powered investigations with clear clinical implications—studies that are more likely to influence practice and generate sustained citations. Conversely, this pattern may also indicate publication bias, wherein smaller studies with null findings or approach-equivalence conclusions face greater publication barriers, potentially skewing the accessible evidence base toward an overestimation of approach-related outcome differences.
Notably, although the search strategy excluded studies primarily investigating revision procedures, the keyword burst of “revision total hip arthroplasty” (2021-2026) reflects the growing use of revision as a long-term outcome endpoint for evaluating primary THA approaches — particularly in registry-based survivorship analyses — rather than the inadvertent inclusion of revision-focused literature.
Thematic Integration: Accuracy, Technology, and the Precision Medicine Paradigm in Approach Selection
The prominence of accuracy-related themes (Cluster #2 encompassing component positioning, navigation, and robotics) reflects the growing recognition that optimal approach selection may be patient-specific rather than universally prescriptive. 47 Contemporary conceptualizations increasingly frame approach choice as 1 element within comprehensive surgical planning that considers patient anatomy (spinopelvic parameters, acetabular bone quality, femoral morphology), functional demands, comorbidity profiles, and available technological resources. 48 This paradigm shift aligns with broader precision medicine principles, wherein treatment selection is individualized based on patient characteristics predictive of differential treatment response, rather than applied uniformly across heterogeneous populations.
Navigation and robotic systems exemplify technological interventions that may modify approach-related outcome profiles by standardizing component positioning and reducing outlier placements. 49 If historical approach-related dislocation risk differences partially reflect differential precision in cup orientation achievable through different exposures, then technology enabling consistent target zone positioning regardless of approach could attenuate these differences. However, current evidence regarding technology-mediated outcome improvements remains mixed, with radiographic accuracy advantages not yet consistently translating to proportional improvements in patient-reported outcomes or revision rates. 50 This dissociation suggests that while precision optimization likely benefits specific high-risk patient subgroups (complex spinopelvic pathology, revision scenarios, and anatomic variants), population-level advantages may be modest when modern surgical techniques achieve acceptable accuracy across approaches in standard primary THA. 51
The integration of approach research with enhanced recovery protocols (cluster themes around early mobilization and reduced hospital stay) further illustrates the contemporary emphasis on systems-level optimization rather than isolated technical modification. 52 ERAS implementation can compress hospital stays and accelerate functional recovery across approaches, potentially neutralizing previously documented early recovery advantages attributed to specific approaches. 53 This finding reinforces that approach selection represents 1 component within multifactorial pathways determining patient outcomes, and optimization efforts targeting the complete perioperative experience may yield greater improvements than approach modification alone.
Publication and Citation Ecosystems: Understanding Journal Roles and Knowledge Dissemination Patterns
The documented dual-tier journal ecosystem, wherein 1 subspecialty journal (Journal of Arthroplasty) anchors publication volume while general orthopedic journals (JBJS-Am, CORR) capture the highest-impact studies (Table 4), reflects a common pattern in specialized surgical fields. 54 This structure serves complementary functions: subspecialty journals provide rapid dissemination platforms for incremental advances, technique refinements, and focused investigations valuable to specialist communities, while high-impact general journals function as gatekeepers for studies with broader implications, methodological exemplars, and practice-changing evidence requiring rigorous peer review and editorial scrutiny.10,55
From a knowledge translation perspective, this ecosystem structure has significant implications. High-impact general journal publications likely exert a disproportionate influence on practice patterns, guideline development, and surgical training curricula compared to subspecialty venue publications, despite the latter’s greater volume. 56 The concentration of influence among a limited number of publications risks oversimplifying nuanced evidence if highly cited studies are selectively referenced, while contradictory or null-finding publications receive less attention. This consideration underscores the importance of comprehensive evidence synthesis through systematic reviews and meta-analyses that systematically sample the complete evidence base rather than relying on citation-based prominence as a surrogate for evidential weight. 57
The relatively modest citation performance of open-access venues (BMC Musculoskeletal Disorders) despite their accessibility advantages suggests that citation accumulation remains primarily driven by perceived study quality, methodological rigor, and practice relevance, rather than access barriers per se. 58 However, open-access publications likely serve important dissemination functions for international audiences, resource-limited settings, and non-academic practitioners whose access to subscription journals may be constrained—populations potentially underrepresented in citation-based impact metrics but nonetheless constituting important evidence consumers.
Future Research Directions and Knowledge Gaps
Several priority directions have emerged from this bibliometric synthesis. First, implementation science research examining optimal training pathways, learning curve acceleration strategies, and institutional adoption frameworks for novel approaches represents a critical gap. 59 The documented importance of surgeon experience in modulating approach-related outcomes indicates that evidence regarding “how to implement” may be equally important as evidence regarding “which to implement,”; however, implementation research remains underrepresented relative to comparative effectiveness investigations.
Second, patient-centered outcome research employing validated instruments, extended follow-up, and adequately powered sample sizes for subgroup analysis represents an ongoing need. 60 While the recent emphasis on patient-reported outcome measures represents progress, heterogeneity in instrument selection and follow-up duration limits comparative interpretation across studies. Standardized outcome measure sets and minimum follow-up durations, potentially established through consensus processes, would enhance evidence synthesis and facilitate more robust comparative conclusions.
Third, health economic analyses examining cost-effectiveness, resource utilization, and value-based outcome assessments remain underrepresented in the identified literature. 61 As healthcare systems increasingly prioritize value optimization alongside clinical effectiveness, evidence regarding the economic implications of approach selection—considering operative time, complication costs, recovery pathway expenses, and long-term revision burden—becomes essential for informed policy and practice decision-making.
Fourth, the investigation of approach-technology-pathway interactions through factorial or adaptive trial designs could elucidate optimal combination strategies rather than evaluating isolated interventions.62,63 Given the multivariate reality of contemporary THA practice, studies examining how approach selection interacts with navigation use, ERAS implementation, and patient-specific factors would provide more actionable guidance than continued head-to-head approach comparisons under idealized conditions.
Finally, the expansion of research beyond traditional Western populations and healthcare systems would enhance generalizability and illuminate how resource constraints, training infrastructure, and patient demographics modify comparative effectiveness relationships. 64 The documented geographic concentration of research activity suggests potential limitations in its applicability to underrepresented settings and populations.
Limitations
This study has inherent limitations, which are characteristic of bibliometric research. First, the database coverage varies in terms of journal inclusion, indexing completeness, and metadata quality. 65 Despite multi-database integration to mitigate single-source bias, systematic gaps persist, particularly in non-English literature, regional journals, and gray literature excluded from major indexes. Second, citation-based metrics reflect research attention and academic influence but do not directly measure clinical validity, methodological quality, or practice impact. 66 Highly cited studies may be controversial or subsequently refuted, while methodologically rigorous null-finding studies may be under-cited despite their evidential value.
Third, the analyzed metadata reflect publication and indexing practices that evolve over time, potentially introducing temporal artifacts beyond those explicitly discussed. 67 Fourth, keyword-based thematic analysis depends on author terminology choices and indexing vocabulary, which may not fully capture conceptual nuances or emerging terminology that has not yet been standardized. 68 Fifth, collaborative network analysis cannot distinguish substantive intellectual contributions from honorary authorship, potentially overestimating the functional collaboration intensity.
Sixth, the partial-year 2026 data necessitate cautious interpretation of recent trends and preclude definitive conclusions about current research directions until indexing stabilizes. Seventh, bibliometric methods map the research landscape but cannot adjudicate clinical controversies or determine approach superiority—interpretations that require critical appraisal of primary evidence rather than citation pattern analysis. Finally, this analysis focused exclusively on primary THA approach research; the findings may not be generalizable to revision arthroplasty, other joint reconstructions, or broader orthopedic surgery domains.
Additionally, although no language restrictions were applied during the initial retrieval phase, the subsequent analysis focused on records with English-language metadata (titles, abstracts, and keywords), as required for keyword co-occurrence analysis and thematic clustering. This methodological constraint may underrepresent the true research output and thematic contributions of major international hubs—particularly China, Germany, Japan, and other nations with substantial domestic-language publication traditions—and should be considered when interpreting geographic productivity rankings and collaboration network structures.
Conclusion
The integrated synthesis consolidated in Figure 9—encompassing dataset characteristics, temporal growth dynamics, geographic collaboration hubs, institutional architecture, journal dissemination patterns, and staged thematic evolution—clarifies the origin of influential evidence and how research priorities have shifted over time. These patterns suggest that future progress depends critically on high-quality comparative designs with standardized outcome measures, registry-linked long-term follow-up, and explicit consideration of surgeon experience, perioperative optimization, and technology integration—contextual factors that likely determine whether approach-related advantages can be translated into consistent real-world benefits. For the clinical and research community, this mapping provides evidence-based guidance for understanding field development, identifying knowledge gaps, and directing future investigations toward questions with the greatest potential for practice improvement. Future bibliometric updates, as the field continues to evolve, will enable longitudinal tracking of whether these trends toward context-dependent, implementation-focused, and value-oriented research persist and ultimately translate into improved patient outcomes
Supplemental Material
sj-docx-1-inq-10.1177_00469580261439653 – Supplemental material for Research Trends and Knowledge Evolution of Surgical Approaches in Primary Total Hip Arthroplasty: A Bibliometric Analysis
Supplemental material, sj-docx-1-inq-10.1177_00469580261439653 for Research Trends and Knowledge Evolution of Surgical Approaches in Primary Total Hip Arthroplasty: A Bibliometric Analysis by Yang Liu, Chong Wang, Hao Zou, Chengguang Wang and Xu Peng in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We thank all of the research participants who volunteered their time to make this work possible.
Abbreviations
CORR clinical orthopedics and related research
DAA direct anterior approach
DE author-provided keywords (descriptive keywords)
DOI digital object identifier
ERAS enhanced recovery after surgery
ID keywords plus (indexing keywords)
JBJS-Am journal of bone and joint surgery - American volume
LLR log-likelihood ratio
MeSH medical subject headings
Q modularity (network quality metric)
RCT randomized controlled trial
S mean silhouette (network quality metric)
THA total hip arthroplasty
TITAN transparency in artificial intelligence-assisted academic research
TLS total link strength
VOS visualization of similarities
WoSCC web of science core collection
Ethical Considerations
This study did not require approval from the Ethics Committee of the People’s Hospital of Chongqing Hechuan as it involved analysis of published literature only.
Author Contributions
Conceptualization: XP and YL; data curation: YL and HZ; formal analysis: CW and CgW; methodology: CW and CgW; project administration: XP and CgW; supervision: XP; writing—original draft: YL; writing—review and editing: XP.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from Chongqing Municipal Hechuan District Research Project HCKJ-2025-055 and Chongqing Science and Health Joint Medical Research Project 2026MSXM127.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All relevant data are within the paper and its Supporting Information files.
Guarantor
XP, the corresponding author, serves as the guarantor of this work.
Provenance and Peer Review
Not commissioned, externally peer-reviewed.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.