
Abstract
Social determinants of health (SDoH) are key contributors to mental health disparities; however, the cumulative impact of multiple SDoH and the relative contribution of individual domains to anxiety remain unclear. Data were drawn from 3 NHANES cycles (2007-2012), including 11 547 adults aged ≥20 years. Anxiety was defined based on self-reported days of feeling worried, tense, or anxious during the past 30 days (≥7 days vs 0-6 days). Eight SDoH indicators were categorized according to the 5 domains of Healthy People 2030. Survey-weighted logistic regression estimated the associations between each SDoH and anxiety after adjustment for demographic, behavioral, and health covariates. A Weighted Quantile Sum (WQS) regression was further applied to assess the cumulative effect and the relative contribution of each SDoH factor. In fully adjusted models, unemployment (OR = 1.44, 95% CI: 1.17-1.76, P = .001) and food insecurity showed strong dose–response associations with anxiety: Marginal food security (OR = 1.38, 95% CI: 1.08-1.75, P = .010), Low food security (OR = 1.66, 95% CI: 1.30-2.13, P < .001), and Very low food security (OR = 1.97, 95% CI: 1.55-2.51, P < .001). The WQS model revealed a significant cumulative burden of social risk factors of health on anxiety (OR = 1.56, 95% CI: 1.22-2.00, P < .001), with the highest weights for food insecurity (0.377), housing instability (0.201), and marital status (0.198). These associations were consistent across sex, age, and racial/ethnic subgroups. Cumulative social determinants of health were significantly associated with anxiety among U.S. adults. Food insecurity, housing instability, marital status, and poverty-to-income ratio were the primary contributors. These findings emphasize the importance of addressing multiple co-occurring social disadvantages in mental health prevention efforts.
Keywords
Introduction
Anxiety disorders are among the most prevalent mental health conditions in the United States, affecting nearly 1 in 3 adults during their lifetime. 1 They contribute substantially to disability, impaired functioning, and poor quality of life, and are associated with an increased risk of comorbid physical diseases such as cardiovascular and metabolic disorders.2,3 Given their growing public health burden, identifying upstream, modifiable risk factors that contribute to anxiety is essential for developing effective prevention strategies.
A growing body of evidence highlights the importance of social determinants of health (SDoH)—the social, economic, and environmental conditions in which people live and work—as fundamental associated factors of mental health. 4 Adverse SDoH, including unemployment, 5 food insecurity, 6 housing instability, 7 lack of health insurance, and social isolation, have been independently associated with higher risks of anxiety or psychological distress. 8 These findings underscore that mental health disparities often reflect underlying social inequities rather than purely individual or biological vulnerabilities. Income is a central structural component within the SDoH framework and shapes access to material and psychosocial resources. 9 Lower income has been linked to anxiety and other mental health outcomes. 10 At the same time, income interacts with more proximal social risk factors, such as food insecurity and housing instability, which may more directly reflect day-to-day material hardship. Considering income alongside other social risk indicators may therefore provide a more comprehensive understanding of their joint associations with anxiety. 11
Nevertheless, most existing studies have focused on single SDoH indicators, neglecting the fact that social disadvantages frequently cluster and may have synergistic effects. Examining these factors separately may underestimate their combined influence and obscure which determinants contribute most strongly when considered together. 12 Mixture-based approaches such as Weighted Quantile Sum (WQS) regression provide an analytic framework to assess the overall burden of correlated exposures and to quantify the relative contribution of individual components. 13 Although widely applied in environmental epidemiology to assess cumulative effects of chemical mixtures, their use in studying multiple SDoH in relation to mental health outcomes remains limited.
Recent studies have begun to examine multi-domain SDoH and psychological outcomes. For instance, Xiao et al 14 used U.S. data to explore SDoH patterns and children’s mental health; Tanarsuwongkul et al 15 examined SDoH and anxiety using the All of Us Research Program; and Xu et al 16 investigated SDoH and mortality risk in the National Health and Nutrition Examination Survey (NHANES). However, to our knowledge, no prior study has used NHANES data to evaluate multiple SDoH indicators and their combined associations with anxiety among U.S. adults. Existing NHANES analyses have largely focused on physical or general health outcomes, leaving this important gap in understanding the social associated factors of adult anxiety.
Although prior studies have documented associations between social determinants of health and anxiety, less is known about the relative salience and joint burden of specific social risk factors within this framework. Therefore, this study addresses 2 primary research questions: (1) whether the co-occurring burden of multiple social risk factors is associated with anxiety beyond individual factors, and (2) which specific social risk factors contribute most strongly to this overall burden. By applying a mixture-based analytic approach, this study aims to advance understanding of how correlated social risks jointly shape anxiety risk.
Methods
Study Population
This cross-sectional study utilized data from the NHANES covering 3 continuous survey cycles from 2007 to 2012. NHANES employs a complex, multistage, probability sampling design to obtain a nationally representative sample of the noninstitutionalized U.S. population. A total of 30 359 participants were initially included across these cycles. After excluding individuals with missing information on anxiety status, key SDoH indicators, or relevant covariates, 11 547 adults (aged ≥20 years) remained in the final analytic sample, the detailed flow of participant selection is presented in Figure 1. All participants provided written informed consent, and the NHANES protocol was approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board, and public-use datasets are available on the official NHANES website: https://www.cdc.gov/nchs/nhanes/index.htm.

Flowchart illustrating the enrollment process of participants in US NHANES 2007-2012.
Determination of Anxiety and SDoH
Anxiety was evaluated based on participants’ self-reported responses to the NHANES questionnaire item: “During the past 30 days, for about how many days have you felt worried, tense, or anxious?” Following previous research, participants who reported feeling anxious for 7 to 30 days in the past month were classified as anxious, whereas those reporting 0 to 6 days were categorized as non-anxious. 17 In addition, the number of anxious days was treated as a continuous outcome variable to further examine whether higher exposure to adverse SDoH was associated with an increased number of anxious days.
Information on SDoH was obtained from the NHANES household interview component. The selection and categorization of variables were informed by prior national studies and corresponded to the 5 domains outlined in Healthy People 2030: economic stability, education access and quality, health care access and quality, neighborhood and built environment, and social and community context. Based on these domains, this study included 8 SDoH indicators: employment status, family poverty income ratio (PIR), food security, education level, health care access, insurance coverage, housing stability, and marital status. 18 Detailed coding procedures and classification criteria for these variables are described in Supplemental Material S1.
Covariates
Several covariates were selected based on prior literature and biological relevance. Demographic variables included age, sex, and race/ethnicity. Age was grouped into 3 categories: 20-34 years, 35-49 years, and ≥50 years. Race/ethnicity was classified as Mexican American, Other Hispanic, Non-Hispanic White, Non-Hispanic Black, or Other/multiracial. Lifestyle factors included body mass index (BMI), smoking, alcohol use, and sleep duration. BMI was calculated as weight (kg) divided by height squared (m2) and categorized as underweight (<18.5 kg/m2), normal weight (18.5-24.9 kg/m2), overweight (25.0-29.9 kg/m2), and obese (≥30.0 kg/m2). Smoking status was determined from participants’ lifetime cigarette use and classified as yes if they had smoked ≥ 100 cigarettes, and no otherwise. Alcohol consumption was categorized as yes for those who reported drinking alcoholic beverages at least 12 times in the past year, and no for those who drank less frequently. Sleep duration (hours per night) was self-reported. Health-related covariates included self-reported hypertension and diabetes status (yes/no). Depressive symptoms were measured using the 9-item Patient Health Questionnaire (PHQ-9), a validated instrument consistent with DSM-IV criteria. A PHQ-9 score ≥ 10 was used to indicate clinically significant depression.
Statistical Analysis
All analyses followed the analytic guidelines of NHANES and incorporated its complex, multistage probability sampling design. Data from 3 continuous cycles (2007-2012) were merged, and sampling weights were recalculated as WTMEC2YR/3 to represent the average U.S. population during this period.
Descriptive statistics were used to summarize participants’ sociodemographic, behavioral, and health characteristics by anxiety status. Continuous variables were expressed as weighted means (SD), and categorical variables as weighted frequencies (percentages). Between-group differences were tested using the design-based Kruskal–Wallis test for continuous variables and the Rao–Scott–adjusted chi-square test for categorical variables. Pairwise correlations among individual SDoH indicators were assessed using Spearman rank correlation coefficients.
Survey-weighted logistic regression models were used to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for the associations between each social determinant of health (SDoH) and anxiety. Model 1 was unadjusted; Model 2 was adjusted for the other 7 SDoH indicators; Model 3 was further adjusted for age, sex, race/ethnicity, BMI, and depressive symptoms. To further evaluate whether greater exposure to adverse SDoH was associated with a higher frequency of anxiety symptoms, survey-weighted linear regression models were conducted with the number of anxious days as a continuous dependent variable, based on the fully adjusted (Model 3) covariate set.
A Weighted Quantile Sum (WQS) regression was then performed to assess the joint effect of multiple SDoH and identify the most influential contributors, we conducted WQS analysis, adjusting for age, sex, race/ethnicity, BMI, smoking, alcohol use, hypertension, diabetes, depression, and sleep duration. The WQS index was constructed using SDoH deciles with a 40% training and 60% validation split and 100 bootstrap iterations. The final WQS model was based on Model 3 specifications.
Subgroup analyses were performed to explore potential heterogeneity across sex, age groups, and race/ethnicity. For each stratum, survey-weighted logistic regression models were re-estimated using the same covariate structure as in Model 3. Sensitivity analyses were conducted by additionally adjusting for smoking status, alcohol use, hypertension, diabetes, and sleep duration to examine the robustness of the results.
The reporting of this cross-sectional study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement.
All analyses were performed using R software (version 4.4.2; R Foundation for Statistical Computing, Vienna, Austria). Two-sided P values < .05 were considered statistically significant.
Results
Baseline Characteristics of Participants
A total of 11 547 adults from NHANES 2007-2012 were included in the analysis, among whom 27% reported anxiety (Table 1). The mean (SD) age of participants was 46.3 (16.3) years, and the overall mean BMI was 28.7 (6.6) kg/m2. Individuals with anxiety were generally younger (44.4 vs 47.0 years, P < .001) and more likely to be female (57% vs 46%, P < .001) than those without anxiety. Regarding socioeconomic indicators, participants with anxiety had a lower mean poverty income ratio (PIR; 2.76 vs 3.19, P < .001), were more frequently unemployed (29% vs 15%, P < .001), and less likely to have health insurance (58% vs 67%, P < .001). They were also more likely to experience food insecurity (P < .001) and housing instability (P < .001). Lower educational attainment and unmarried status were significantly more common among anxious participants (P < .001 for both). No significant difference was observed in health-care access between groups (P = .8). However, anxious participants showed higher rates of smoking (54% vs 47%, P < .001), hypertension (32% vs 29%, P = .038), and markedly higher prevalence of depression (25% vs 1.9%, P < .001). Diabetes prevalence and alcohol consumption did not differ significantly between groups. The mean number of anxious days in the past 30 days was 19 (9) among the anxious group and 1 (2) among the non-anxious group (P < .001). The results of the Spearman correlation analysis showed mild to moderate correlations among the 8 SDoH variables (Figure 2).
Survey-Weighted Characteristic Variables of the Study Participants Stratified by Anxiety, US NHANES 2007-2012 (N = 11 547).
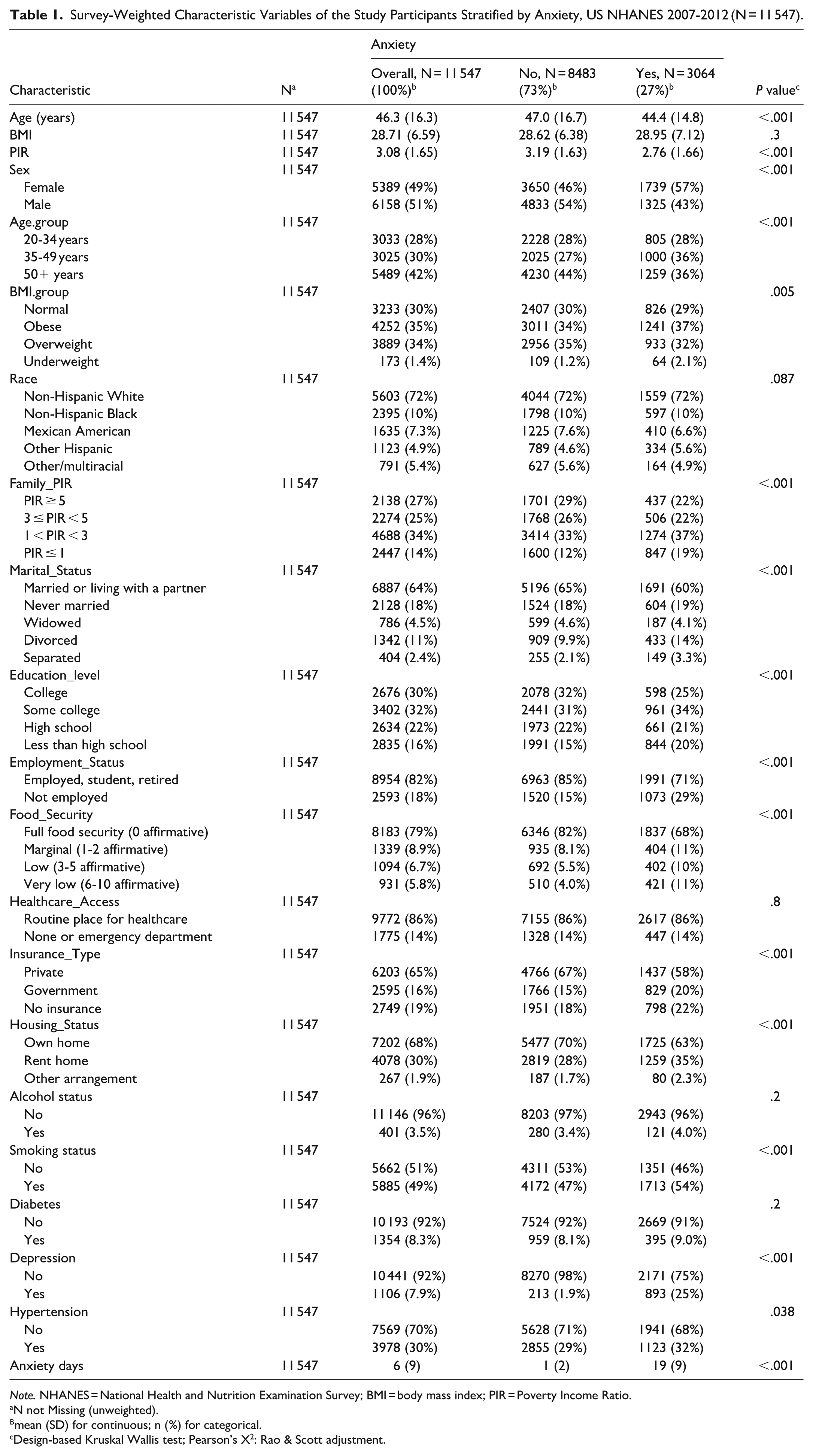
Note. NHANES = National Health and Nutrition Examination Survey; BMI = body mass index; PIR = Poverty Income Ratio.
N not Missing (unweighted).
mean (SD) for continuous; n (%) for categorical.
Design-based Kruskal Wallis test; Pearson’s X2: Rao & Scott adjustment.

Spearman correlations between 8 SDoH variables in US NHANES 2007-2012. Moderate Red to Dark Sea Green: Correlation coefficients (ρ) from +1 (strong positive) to −1 (strong negative); Numeric values show Spearman’s ρ (eg, 0.27 = weak positive correlation). Larger absolute values indicate stronger associations (eg, 0.46). The corresponding ρ is marked with an “×” if the P-value exceeds .05.
Associations Between Individual SDoH and Anxiety
Table 2 summarizes the associations between 8 SDoH indicators and anxiety among U.S. adults. In the fully adjusted logistic regression model (Model 3), several SDoH remained significantly associated with anxiety. Participants who were unemployed had higher odds of anxiety (OR = 1.44, 95% CI: 1.17-1.76, P = .001). Compared with those reporting full food security, the odds of anxiety increased progressively with food insecurity: marginal food security (OR = 1.38, 95% CI: 1.13-1.68, P = .003), low food security (OR = 1.66, 95% CI: 1.34-2.06, P < .001), and very low food security (OR = 1.97, 95% CI: 1.60-2.43, P < .001). Associations for marital status, insurance type, housing status, and health-care access were not statistically significant after full adjustment (all P > .05).
Association Between SDoH and Anxiety in Survey-Weighted Logistics Regression Models, US NHANES 2007-2012 (n = 11 547).

Note. For each of 8 SDoH variables: Model 1 was an unadjusted model. Model 2 was adjusted for other 7 SDoH variables. Model 3 was adjusted for sex, age, race/ethnicity, BMI, depression, and other 7 SDoH variables. The results show the adjusted Odds Ratio (OR), their 95% CIs, and P. Bold values indicate statistical significance (P < .05).
OR = odds ratio; CI = confidence interval; NHANES = National Health and Nutrition Examination Survey; PIR = poverty income ratio; SDoH = social determinants of health.
Conduct survey-weighted linear regression using Model 3, with the number of days of anxiety as a continuous variable. The results show the adjusted beta, their 95% CIs, and P. Bold values indicate statistical significance (P < .05).
When the number of anxious days was treated as a continuous outcome, similar patterns were observed in survey-weighted linear regression. Unemployment remained significantly associated with more anxious days (β = 1.40, 95% CI: 0.57-2.30, P = .002), and increasing levels of food insecurity were consistently related to longer anxiety duration (marginal food security: β = 1.7 [0.92-2.5], P < .001; low food security: β = 2.1 [1.2-3.0], P < .001; very low food security: β = 2.4 [1.4-3.4], P < .001).
Subgroup and Sensitivity Analyses
Age-stratified analyses are presented in Supplemental Table S2. Distinct age-specific patterns were observed for the associations between SDoH and anxiety. Among adults aged 20 to 34 years, low food security was significantly associated with higher odds of anxiety (OR = 1.62, 95% CI: 1.10-2.37, P = .016). In the 35 to 49-year group, both unemployment (OR = 1.53, 95% CI: 1.12-2.08, P = .010) and food insecurity demonstrated strong associations with anxiety. Compared with full food security, participants with low and very low food security had markedly higher odds of anxiety (OR = 1.92, 95% CI: 1.24-2.98, P = .005 and OR = 2.81, 95% CI: 1.73-4.56, P < .001, respectively). Among adults aged ≥50 years, unemployment (OR = 1.53, 95% CI: 1.11-2.11, P = .011) and increasing levels of food insecurity were significantly associated with anxiety, including marginal (OR = 1.78, 95% CI: 1.20-2.63, P = .006), low (OR = 1.50, 95% CI: 1.11-2.03, P = .011), and very low food security (OR = 2.25, 95% CI: 1.58-3.20, P < .001).
Detailed stratified analyses by sex and race/ethnicity are presented in Supplemental Table S3. Among men, unemployment (OR = 1.85, 95% CI: 1.39-2.47, P < .001) and very low food security (OR = 1.83, 95% CI: 1.34-2.51, P < .001) were significantly associated with higher odds of anxiety. Among women, food insecurity exhibited a clear dose–response pattern, beginning from marginal food insecurity (OR = 1.61, 95% CI: 1.20-2.15, P = .003) and strengthening at low (OR = 2.31, 95% CI: 1.67-3.19, P < .001) and very low levels (OR = 2.03, 95% CI: 1.46-2.83, P < .001).
Across racial and ethnic groups, both food insecurity and unemployment showed notable associations with anxiety. Among Non-Hispanic White adults, unemployment (OR = 1.43, 95% CI: 1.10-1.85, P = .009) and food insecurity at multiple levels—marginal (OR = 1.61, 95% CI: 1.20-2.16, P = .003), low (OR = 2.12, 95% CI: 1.53-2.94, P < .001), and very low (OR = 2.11, 95% CI: 1.56-2.84, P < .001)—were all significantly related to anxiety. Among Non-Hispanic Black participants, unemployment (OR = 1.71, 95% CI: 1.28-2.28, P < .001) and food insecurity (low: OR = 1.60, 95% CI: 1.08-2.37, P = .020; very low: OR = 1.91, 95% CI: 1.33-2.74, P = .001) were also strong associated factors. In Mexican Americans, very low food security was significantly associated with anxiety (OR = 2.17, 95% CI: 1.20-3.93, P = .013).
Sensitivity analyses incorporating additional covariates (smoking, alcohol status, diabetes mellitus, hypertension and sleep duration) yielded results consistent with the primary model (Supplemental Table S4). These findings confirm the robustness of our conclusions and suggest that the observed associations are unlikely to be driven by unmeasured confounding.
WQS Analyses
The WQS regression analysis (Table 3) showed a significant positive association between the overall mixture of adverse SDoH and anxiety among U.S. adults. Each unit increase in the WQS index was associated with a 56% higher odds of anxiety (OR = 1.56, 95% CI: 1.22-2.00, P < .001). As shown in Figure 3, the SDoH contributing most to the overall index were food insecurity (weight = 0.377), housing instability (weight = 0.201), marital status (weight = 0.198), and poverty income ratio (PIR; weight = 0.141). Detailed information on the individual weights of SDoH components is presented in Supplemental Table S5.
WQS Analysis Results of SDoH Variables With Anxiety, US NHANES 2007-2012.

Note. The model was adjusted for age, sex, BMI, race/ethnicity, smoking status, alcohol status, diabetes mellitus, hypertension, depression, and sleep duration. Results of adjusted OR, their 95% confidence intervals (95% CI), and P presented with bold values were statistically significant with P < .05 or P < .001.
Note. NHANES = National Health and Nutrition Examination Survey; SDoH = social determinants of health; WQS = weighted quantile sum; BMI = body mass index.

Weights of each SDoH variable in the WQS model regression indices, US NHANES 2007-2012.
Discussion
Main Findings
In this nationally representative study, we found that the cumulative burden of social risk factors of health was significantly associated with anxiety. In survey-weighted logistic regression models, unemployment and food insecurity were the strongest independent associated factors of anxiety, even after adjusting for multiple sociodemographic and health covariates. The odds of anxiety increased progressively with the severity of food insecurity, demonstrating a clear dose–response relationship.
The WQS regression further confirmed a significant cumulative effect of overall social disadvantage on anxiety. Each unit increase in the WQS index was associated with a 56% higher odds of anxiety. The most influential contributors to the overall SDoH mixture were food insecurity, housing instability, and marital status, underscoring the importance of material and social instability in shaping anxiety risk.
Interpretation of Subgroup Findings
The observed subgroup patterns suggest differential vulnerability to social risk factors across demographic groups. Women exhibited a clear dose–response relationship between food insecurity and anxiety, beginning at marginal food security, whereas men only showed significant associations at very low food security. This may reflect women’s greater responsibility for household food management or heightened psychological burden when facing resource constraints. 19 Age-stratified analyses revealed that unemployment was not significantly associated with anxiety among adults aged 20 to 34 years, possibly due to family financial support, transitional life stage, or greater optimism about future employment prospects. 20 In contrast, adults aged 35 to 49 years showed the strongest associations between both unemployment and food insecurity with anxiety, likely reflecting peak financial responsibilities and limited social safety nets during this life stage. 21 Among older adults (≥50 years), marginal food security was significantly associated with anxiety, suggesting that even minor food access concerns may trigger distress in this population. Racial/ethnic differences were also notable: Non-Hispanic White participants showed significant associations across all levels of food insecurity, while Non-Hispanic Black and Mexican American participants showed significant effects primarily at low or very low food security levels. This may reflect varying coping resources, social support networks, or culturally patterned responses to material hardship across groups. 22 These findings highlight the importance of targeted interventions that account for demographic-specific vulnerabilities.
Comparison With Previous Studies and Mechanisms
Previous research has consistently demonstrated that adverse social determinants of health (SDoH) are associated with increased anxiety risk. In our WQS model, food insecurity, housing instability, marital status, and PIR contributed most prominently to the overall index, suggesting that these domains may represent key pathways linking social disadvantage to anxiety.
Food insecurity has been repeatedly identified as a strong correlate of anxiety in population-based studies.23,24 Individuals experiencing food insecurity are more likely to report anxiety symptoms, a finding that is highly consistent with our observed dose–response relationship. Mechanistically, food insecurity may induce chronic psychological stress driven by uncertainty about meeting basic needs. Persistent concern over food access can activate prolonged stress responses and sustained emotional tension, 25 thereby increasing vulnerability to anxiety disorders. Its prominent weight in the WQS model underscores its role as a proximal and tangible manifestation of material hardship.
Housing instability also contributed substantially to anxiety risk in our analysis. Previous studies have shown that unstable housing conditions are associated with poorer mental health outcomes, including anxiety.26,27 Housing instability may function as an ongoing environmental stressor, generating insecurity, lack of control, and concerns about safety or displacement. Such chronic environmental uncertainty may perpetuate heightened vigilance and stress reactivity, thereby exacerbating anxiety symptoms.
Marital status emerged as another important contributor. Existing literature indicates that being unmarried, divorced, or widowed is associated with elevated anxiety risk compared with being married.28,29 Social relationships play a crucial protective role in buffering stress and promoting emotional regulation. The absence of close interpersonal support may increase social isolation and reduce resilience in the face of socioeconomic adversity. The relatively high weight assigned to marital status in our WQS model highlights the importance of relational and social support structures in mental health.
PIR, an upstream indicator of household income relative to the federal poverty threshold, also demonstrated a meaningful contribution to the WQS index. Lower income has consistently been associated with higher anxiety prevalence. 30 Income insufficiency may exert direct effects through chronic financial strain and indirect effects by increasing the likelihood of downstream adversities such as food insecurity and housing instability.31,32 Although its weight was not the highest, PIR likely represents a structural determinant that shapes exposure to multiple material hardships, consistent with the fundamental cause theory which posits that socioeconomic position influences health through multiple risk pathways. 33 Thus, its influence may be diffuse yet foundational within the broader system of socioeconomic disadvantage.
Importantly, most prior studies have examined these factors independently. By applying WQS regression, our study models SDoH as an interacting system of exposures and quantifies their joint contribution to anxiety risk in a nationally representative sample. These findings suggest that anxiety is not driven by a single social determinant but rather by the accumulated burden of material deprivation and social instability, potentially reflecting chronic stress accumulation consistent with the concept of allostatic load. 34 Addressing both upstream structural inequality and specific proximal hardships may therefore be essential for improving population mental health. 11
Implications for Clinical Practice and Future Research
Notably, the lack of correlation between employment and healthcare access in our data reflects the unique U.S. healthcare system, where insurance coverage is not exclusively tied to employment (eg, Medicare for retirees, Medicaid for eligible individuals). This decoupling suggests that interventions targeting employment alone may be insufficient to improve healthcare access or reduce anxiety at the population level.
The present findings highlight the substantial influence of social and economic instability on anxiety among U.S. adults, suggesting that assessment of SDoH should be incorporated into routine mental health care. 4 Clinicians and public health professionals could benefit from systematically screening for key social stressors—particularly food insecurity, unemployment, housing instability, and marital or social relationship status—when evaluating patients with anxiety symptoms. Identifying these underlying social risks may help tailor more comprehensive treatment plans that combine psychological care with social and economic support, such as connecting patients to food assistance programs, employment counseling, income support services, or community-based social support networks.
From a research perspective, our results emphasize the need for multidimensional approaches that consider the combined impact of multiple SDoH rather than assessing single factors in isolation. Future studies should apply longitudinal designs to clarify causal pathways linking social adversity and anxiety, and evaluate whether improvements in food access, stable housing, and supportive relationships can mitigate anxiety risk. Additionally, the WQS framework used here provides a valuable methodological approach for modeling the cumulative burden of correlated social exposures and could be extended to other mental health outcomes.
Overall, these findings suggest that addressing the root social causes of anxiety—through policies that promote income security, food security, stable employment, safe housing, and social connectedness—may be as critical as traditional clinical interventions in reducing the population burden of anxiety disorders.
Strengths and Limitations
This study has several notable strengths. First, it is based on a large, nationally representative sample of U.S. adults from NHANES, enhancing the generalizability of the findings to the general population. Second, the analysis incorporated a comprehensive set of SDoH, spanning economic, educational, healthcare, housing, and social domains, which allowed for a multidimensional assessment of social influences on anxiety. Third, the use of survey-weighted regression models ensured appropriate adjustment for NHANES’s complex sampling design, while the application of WQS regression provided an innovative approach to quantify the cumulative and relative contributions of multiple SDoH factors. Finally, multiple sensitivity and subgroup analyses confirmed the robustness and consistency of the observed associations across demographic groups.
Several limitations should also be acknowledged. First, the cross-sectional design precludes causal inference; temporal relationships between SDoH and anxiety cannot be established. Second, both SDoH and anxiety were self-reported, which may introduce recall bias and misclassification. Third, although extensive covariates were adjusted for, the possibility of residual confounding cannot be excluded. In particular, not all dimensions of SDoH were captured in the present analysis. Certain contextual factors—such as built environment characteristics (eg, neighborhood walkability or recreational infrastructure), social isolation, and experiences of discrimination—were not available or consistently measured in NHANES. These unmeasured domains may also influence anxiety risk and could partially account for the observed associations. Fourth, the measurement of anxiety was based on a single self-rated item rather than a structured diagnostic interview, which may not capture the full clinical spectrum of anxiety disorders. Lastly, because the data are cross-sectional, the estimated cumulative burden reflects co-occurring adverse social conditions measured at a single time point rather than accumulation over time or across the life course.
Conclusion
In conclusion, this study demonstrates that cumulative social determinants of health are significantly associated with anxiety among U.S. adults. Food insecurity, housing instability, marital status, and PIR emerged as key contributors in the WQS model, underscoring the importance of material and social conditions in shaping mental health. These findings highlight that anxiety is not attributable to a single social factor but reflects the combined burden of multiple disadvantages. Addressing upstream socioeconomic conditions alongside specific material hardships may be essential for improving population mental health.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261436354 – Supplemental material for Cumulative Social Determinants of Health Are Associated With Anxiety: A Weighted Quantile Sum Analysis
Supplemental material, sj-docx-1-inq-10.1177_00469580261436354 for Cumulative Social Determinants of Health Are Associated With Anxiety: A Weighted Quantile Sum Analysis by Bei Li, Peng Xia, Meidi Yang, Tingting Zhang and Haijing Liu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580261436354 – Supplemental material for Cumulative Social Determinants of Health Are Associated With Anxiety: A Weighted Quantile Sum Analysis
Supplemental material, sj-docx-2-inq-10.1177_00469580261436354 for Cumulative Social Determinants of Health Are Associated With Anxiety: A Weighted Quantile Sum Analysis by Bei Li, Peng Xia, Meidi Yang, Tingting Zhang and Haijing Liu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors would like to acknowledge the National Health and Nutrition Examination Survey (NHANES) for providing data.
Ethical Considerations
This study represents a secondary analysis of de-identified publicly available data. The original NHANES protocol was approved by the National Center for Health Statistics Research Ethics Review Board. No additional ethical approval was required for this secondary analysis.
Consent to Participate
All participants provided written informed consent.
Author contributions
Bei Li: Conceptualization; Visualization; Writing—original draft; Methodology. Peng Xia: Software; Investigation; Project administration. Meidi Yang: Data curation. Tingting Zhang: Formal analysis. Haijing Liu: Funding acquisition; Supervision; Writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was supported by the Yunnan Provincial Department of Science and Technology (NO. 202401AZ070001-018); Yunnan province innovation team of prevention and treatment for brain diseases with acupuncture and Tuina (NO. 202405AS350007). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.*
Supplemental Material
Supplemental material for this article is available online.